
Treatment Methods for Anterior Cruciate Ligament (ACL) Injuries
Xiangqian Ling
Shanghai YKPAO School, Shanghai, China
Keywords: Anterior Cruciate Ligament (ACL) Injury, Rehabilitation, Digital Therapy.
Abstract: Anterior cruciate ligament (ACL) injury is prevalent in sports players and physically active people and causes
significant morbidity and functional impairment. In this review, the epidemiology, methods of diagnosis,
methods of treatment, and rehabilitation regimens of ACL injury are addressed in a systematic manner.
Particular emphasis is placed on the advantages and disadvantages of current surgical procedures, including
arthroscopic reconstruction, and emerging non-surgical interventions, including digital therapy. In addition,
the diagnostic contribution of MRI and physical examination is sharply evaluated. The findings emphasize
the importance of personalized rehabilitation programs and use of emerging technologies to improve patient
outcomes.
1 INTRODUCTION
One of the significant ligaments found in the human
body is the anterior cruciate ligament, particularly for
the stability of the knee joint. It has a crucial function
of preventing the sliding forward of the tibia against
the femur and helps prevent rotational instability.
Damaging the ligament will result in serious
impairment, particularly for athletes or physically
active patients. Sports ACL injuries are commonly
associated with jumping, pivoting, or most abrupt
stops that participate in sporting events, which are
soccer, basketball, skiing, and football. Over the last
few years, the rate of ACL injuries has been rising,
mostly due to increased involvement in sports and
physical activity across various age groups. The
effects of injuries are not only physical but also result
in prolonged periods of inactivity, loss of function,
emotional distress, and expense of medical treatment
and rehabilitation. The effects of injuries are not only
physical but also result in prolonged periods of
inactivity, loss of function, emotional distress, and
expense of medical treatment and rehabilitation. The
individual and social impacts of ACL injury have
promoted a rapid rate of research and innovation on
their prevention, diagnosis, treatment, and
rehabilitation (Anderson & Wu, 2020). This article is
a review of the management and practice of ACL
injury. There is a detailed review of the epidemiology
of ACL injury with the usual risk factors and
demographics involved. Diagnostic modalities in
terms of physical examination tests and imaging are
discussed. Following diagnosis, different treatment
options are weighed whether surgical or not. The
paper also deals with the process of rehabilitation,
with the modern digital methods employed in
rehabilitating patients to recover from an ACL injury
being given much importance. Injuries to the ACL
happen in a diverse population but predominantly in
athletes. The global prevalence has been increasing
steadily, at least partially due to higher levels of
sporting participation, particularly in youth and
females. Evidence shows that female sportsmen are at
greater risk of developing ACL injuries compared to
their male counterparts. This has been attributed to
anatomical variations such as a broader pelvis,
hormonal effects, and neuromuscular control
differences.
Table 1. ACL Injury Incidence by Population Group.
Population Group Incidence Rate (Pe
r
100,100)
General Population 68.6
Male Athletes 85.0
Female Athletes 120.0
Adolescents 130.0
As table 1 shows, adolescents have a higher
incidence rate compared to adults, which indicates
that age is also a factor. Adolescents and young adults
engaging in sports with high intensities are most
commonly involved (Anderson & Wu 2020).
However, ACL injuries are not limited to athletes.
448
Ling, X.
Treatment Methods for Anterior Cruciate Ligament (ACL) Injuries.
DOI: 10.5220/0014495100004933
Paper published under CC license (CC BY-NC-ND 4.0)
In Proceedings of the 1st International Conference on Biomedical Engineering and Food Science (BEFS 2025), pages 448-452
ISBN: 978-989-758-789-4
Proceedings Copyright © 2026 by SCITEPRESS – Science and Technology Publications, Lda.

They can occur in non-athletes due to falls, car
accidents, or sudden missteps that overexert the knee
joint. Besides, as table 1 shows, gender also plays a
role in incidence rate.
Figure 1 rising trends of ACL injuries in youth athletes
(2010–2024).
Biomechanically, ACL injuries are typically
caused by non-contact mechanisms. These include
sudden deceleration, poor landing mechanics, and
unexpected alterations of direction (Polhill, 1982).
These movements place the knee joint under
excessive stress, especially when there is poor
muscular control or quadriceps-hamstring imbalance.
Individuals with weak core stability or impaired
proprioception are also more susceptible. Untreated
ACL injuries have severe long-term effects. Besides
the initial instability and pain, there is also a high
likelihood of secondary cartilage or meniscus injury.
Such damage can ultimately lead to chronic
instability and osteoarthritis that occur prematurely.
(Filbay & Grindem 2019). This underscores the
importance of early and proper diagnosis followed by
effective intervention (O’Connor, 2020).
2 DIAGNOSIS
The diagnostic work-up of ACL injuries begins with
a comprehensive clinical examination. Clinicians
make a working diagnosis by a blend of patient
history, physical examination tests, and imaging
studies. In table 2, it presents the ideas of different
methods and their clinical effectiveness, which can be
linked to physical examination for diagnosis.
Physical examination plays a very important role in
the diagnosis (Anderson & Wu 2020). The lachman
test is usually considered the most sensitive test of
ACL damage (lee 2018). To perform the lachman
test, place the knee in a reduced amount of flexion and
apply an anterior force to the tibia. More anterior
translation of the tibia than the opposite knee is a
positive test. Another useful test is the anterior drawer
test, which also checks for anterior displacement of
the tibia. (Filbay, Grindem 2019). Pivot-shift test,
though technically more challenging, is an ACL
injury-specific and evaluates rotational instability.
However, physical tests are not perfect. Swelling,
pain, or muscle guarding can influence the validity of
a test (Zhou, H,2019).
Therefore, imaging techniques have an important
supporting role to play. Magnetic resonance imaging
(MRI) is the gold standard for visualization of the
ACL and associated structures (Johnson 1965). MRI
can detect sensitive inspection of the integrity of the
ligament, as well as detection of other concomitant
injuries to menisci or cartilage. MRI is reliable,
though costly, and not yet widely available to all
practices (Smith, 2020). Other imaging modalities
include ultrasound and x-ray. X-rays, though they
don't directly visualize the ACL, are useful in ruling
out fracture or avulsion injury. Ultrasound is not so
commonly utilized but can provide dynamic
evaluation of ligamentous structures when performed
by skilled operators (Patel 2018).
Table 2. Diagnostic methods and their clinical
effectiveness.
Method Sensitivity (%) Specificity
(
%
)
Lachman Test 85-95 85-95
Anterior Drawer
Test
70-90 70-90
Pivot-Shift Test 60-80 90-98
MRI 86-95 80-95
3 TREATMENT MODALITIES
The treatment of ACL injuries depends on several
factors, including the degree of injury, the level of
activity of the patient, age, and personal goals.
Treatment can be broadly classified into surgical and
non-surgical interventions (Davis 2017).
Operative repair is generally recommended for
those with complete ACL tears who are willing to
regain high level physical function (Johnson 1965).
Arthroscopic ACL reconstruction is the most
common type of surgery in which the compromised
ligament is replaced by a graft. Either autografts
Treatment Methods for Anterior Cruciate Ligament (ACL) Injuries
449
(tissue harvested from the patient) or allografts (donor
tissue) can be utilized as grafts (Wang, H,2019).
Table 3. Comparison of autograft vs. Allograft in ACL
reconstruction.
Feature Auto
g
raft Allo
g
raft
Source Patient’s Own
Issue
Donor Issue
Healin
g
S
p
ee
d
Faste
r
Slowe
r
Risk Of Rejection None Low To
Moderate
Donor Site
Morbidit
y
Present None
Reo
p
eration Ris
k
Lowe
r
Sli
g
htl
y
Hi
g
he
r
Figure 2. ACL reconstruction outcomes by graft type (1-
year follow-up).
Autografts Are Typically Harvested from The
Quadriceps Tendon, Hamstring Tendons, Or Patellar
Tendon. Each Graft Is Associated with Both
Advantages and Disadvantages. (A. Todor 2024).
Patellar Tendon Grafts Are Robust and Provide Good
Fixation but Are Associated with Anterior Knee Pain.
Hamstring Grafts Are Less Invasive to Harvest but
May Result in Slightly Weaker Early Fixation.
As figure 2 shown, allografts obviate donor site
morbidity and reduce operating time but may have an
increased likelihood of graft loss and delayed
incorporation (Kumar & Singh 2016) in figure 2, it
shows the process of ACL reconstruction by graft
type, graft choice is based on patient concerns,
surgeon preference, and specific functional demand
(Davis 2017). Another consideration in surgical
technique is whether to use single-bundle or double-
bundle reconstruction. (Filbay, Grindem 2019). The
single-bundle technique reconstructs the
anteromedial bundle of the ACL, while the double-
bundle technique attempts to more closely replicate
the native anatomy by reconstructing both the
anteromedial and posterolateral bundles (Mitchell
2021). While the double-bundle technique might
offer improved rotational stability, it is technically
more demanding and time-consuming. Non-surgical
treatment may be applied to patients with partial tears
of the ACL or those with minimal functional demands
(Robinson 2019). Treatment is typically physical
therapy that makes the supporting musculature
stronger, increases proprioception, and enhances
neuromuscular control. Brsing can impart external
support for the knee for physical activity though its
long-term efficacy is questioned. Modification of
activity to avert the causative factor tends to reduce
recurrence. (a. Todor 2024). For most patients,
conservatively, including those not partaking in the
pivoting sporting activities, satisfying results may
occur. More recent therapies such as biological
injections are also being explored. Platelet-rich
plasma (prp) and stem cell therapy are trying to
enhance healing by delivering growth factors to the
location of injury. (Chen, 2021) although early
reports are promising, larger clinical trials need to be
done to establish their efficacy and safety (Jappelli, R
1997).
4 REHABILITATION AND
DIGITAL THERAPY
Table 4. Phased postoperative rehabilitation timeline.
Phase Duration Focus
Phase I 0-2 Weeks Pain Control,
ROM Recover
y
Phase II 2-6 Weeks Muscle
Strength,
Wei
g
ht Bea
r
Phase III 6-12 Weeks Balance
Phase IV 3-6 Months Functional
Training
Phase V 6+ Months Return To S
p
ort
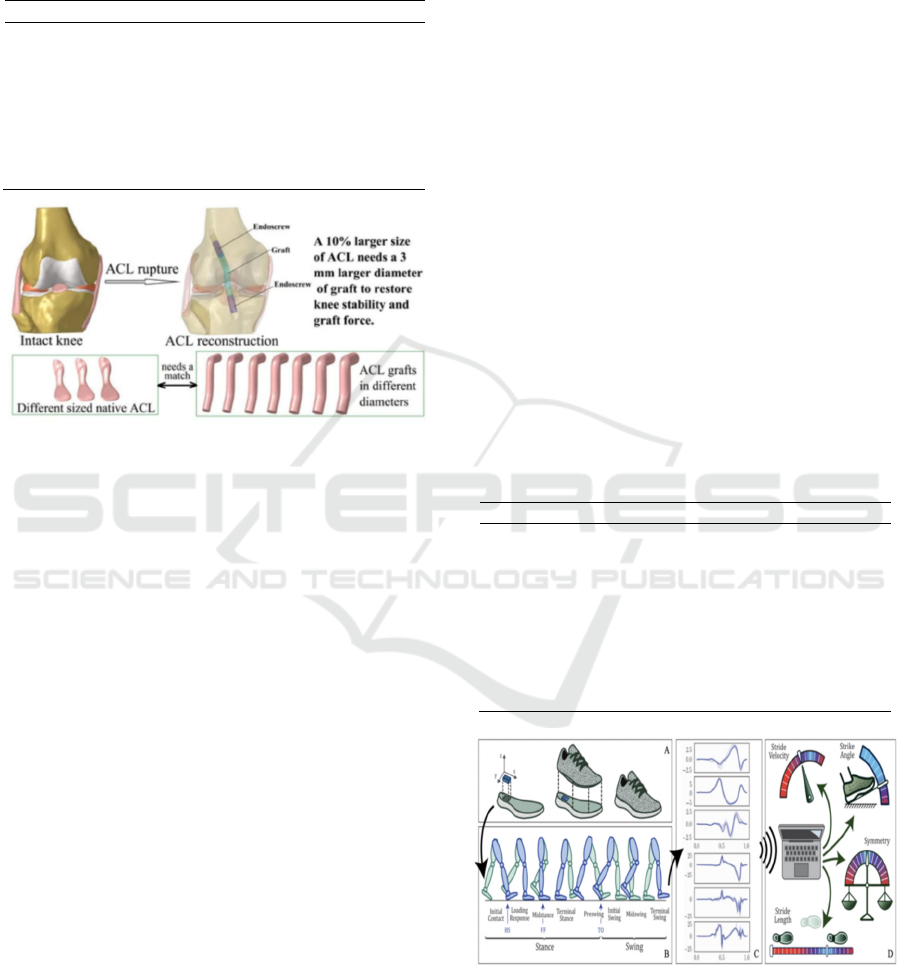
Figure 3. wearable sensors and gait symmetry tracking
during rehab.
Rehabilitation is the cornerstone of effective
management of ACL injury. Regardless of whether
the treatment is surgical or non-surgical, formal
BEFS 2025 - International Conference on Biomedical Engineering and Food Science
450

rehabilitation is essential for return of function,
prevention of re-injury, and return to activity. As
table 4 shows, rehabilitation postoperatively typically
follows a staged approach. Pain management,
reduction of swelling, and restoration of range of
motion passively are the focus of the initial phase.
Strengthening exercises, especially of the quadriceps
and hamstrings, become important as healing
progresses. Training in balance and proprioception is
established to further enhance joint stability. The
advanced stages of rehabilitation involve sport-
specific training, agility drills, and endurance.
Return-to-sport standards usually consist of adequate
strength and flexibility, passing of functional tests,
and mental readiness. (A. Todor 2024). The entire
rehabilitation process could take six months to one
year based on individual progress and severity of
injury (Brown, 2020) digital health technologies are
transforming rehabilitation. Wearable sensors,
mobile apps, and tele-rehabilitation platforms are
being used more and more in recovery programs.
They offer real-time feedback, monitor patient
progress, and increase engagement. As figure 3
shows, wearable sensors can monitor movement
patterns, detect departures from standard
biomechanics, and alert clinicians to intervene.
(Filbay, Grindem 2019). Cellular apps give patients
exercise routines, reminders, and tracking. Patients
also notify their therapists, making it more convenient
and personalized. Gamification and virtual reality are
emerging as new methods of increasing patient
motivation and compliance. These interventions
make rehabilitation interactive and fun, which is also
essential for young patients. Secondly, data obtained
from virtual sites can be employed to calibrate
treatment strategies, predict recovery pathways, and
identify risk patients with poor outcomes (Brown
2020). This evidence-based approach maximizes
evidence-based practice and enhances the provision
of care (A. Todor 2024).
5 CONCLUSIONS
Injuries of the ACL are a significant concern in sports
medicine and orthopedics. They affect a wide
population of people and have profound effects on
quality of life, mobility, and joint health in the long
term. Accurate diagnosis, tailored treatment planning,
and close rehabilitation are paramount to optimal
outcome. Surgical reconstruction remains the gold
standard in active patients with full thickness ACL
injuries, and non-operative treatment is applied to
selected patients who are of low demand. The
treatment would have to be tailored according to the
nature of injury, patient needs, and likelihood of
complications versus benefits. Rehabilitation is a key
factor in recovery, and the incorporation of digital
technologies opens up new directions for enhancing
its effectiveness. The future of research may include
developing new advanced biological therapies,
enhanced personalization of rehabilitation regimens,
and digital tool extension applications. Last, a
multidisciplinary approach coupled with surgical
competence, physiotherapy, and technological
innovation is the most likely to yield a successful
future for those who suffer ACL injury. A continuous
collaboration of clinicians, researchers, and patients
will promote advances and improve results in the care
of ACL injuries.
REFERENCES
Anderson, R.J. & Wu, Q. 2020. Graft selection in ACL
surgery: a systematic review. Orthopedic Reviews
45(1): 65-72.
Brown, T.M. Et Al. 2020. Comparative outcomes of ACL
reconstruction techniques. Knee Surgery Journal 22(1):
34-47.
Chen, Y. & Zhang, L. 2021. Role of prp in ACL healing: a
meta-analysis. Sports Medicine Review 29(3): 145-
158.
Davis, K. 2017. ACL injury trends in youth athletes.
Pediatric Sports Health 8(2): 90-98.
Filbay, Stephanie R., and Hege Grindem. “Evidence-Based
Recommendations for the Management of Anterior
Cruciate Ligament (ACL) Rupture.” Best Practice &
Research Clinical Rheumatology, vol. 33, no. 1, 2019,
pp. 33–47.2019.01.018.
Jappelli, R. & Marconi, N. 1997. Recommendations and
prejudices in the realm of foundation engineering in
italy: a historical review. In carlo viggiani (ed.),
geotechnical engineering for the preservation of
monuments and historical sites; Proc. Intern. Symp.,
Napoli, 3-4 October 1996. Rotterdam: Balkema.
Johnson, H.L. 1965. Artistic development in autistic
children. Child Development 65(1): 13-16.
Kumar, N. & Singh, D. 2016. Biomechanical analysis of
ACL injury. International Journal of Sports Medicine
17(6): 331-338.
Lee, M.H. Et Al. 2018. Neuromuscular training for ACL
injury prevention. Journal Of Sports Science 36(4):
401-412.
Mitchell, G. 2021. The future of digital rehab in ACL
recovery. Ehealth Reports 9(3): 77-88.
O’Connor, P. & Malik, T. 2020. Comparison of autograft
types in ACLR. Surgical Trends 33(2): 98-106.
Treatment Methods for Anterior Cruciate Ligament (ACL) Injuries
451

Patel, R. 2018. Digital therapy in post-ACL recovery.
Health Tech Innovations 10(4): 78-85.
Polhill, R.M. 1982. Crotalaria in africa and madagascar.
Rotterdam : Balkema.
Robinson, A.P. Et Al. 2019. Wearable technology in
orthopedic rehabilitation. Med Tech Frontier 11(2):
120-128.
Smith, J.R. & Johnson, L.K. 2020. Advances in ACL
reconstruction. New York: Springer.
Wang, H. Et Al. 2019. MRI Accuracy in Diagnosing ACL
Tears. Journal Of Orthopedic Research 37(2): 45-52.
Zhou, H. Et Al. 2017. Psychological Readiness and Return
to Sport Post-ACL Surgery. Clinical Orthopedic
Research 26(5): 213-220.
BEFS 2025 - International Conference on Biomedical Engineering and Food Science
452
