
A Hybrid SARIMAX-SVR Model for Drug Demand Prediction
Rithagia Palelleng
a
and Novy N. R. A. Mokobombang
b
Department of Informatics, Faculty of Engineering, Universitas Hasanuddin, Gowa, South Sulawesi, Indonesia
Keywords: Forecasting, SARIMAX, SVR, Hybrid Model, Machine Learning.
Abstract: Accurate prediction of drug demand is a critical challenge in Indonesia’s National Health Insurance (JKN)
system, where misestimation can lead to two major problems: overstock, resulting in financial inefficiency,
and stockouts, which directly disrupt patient therapy. Traditional time-series models such as ARIMA and
SARIMA are often insufficient to capture nonlinear fluctuations and complex seasonal patterns in drug
demand. To address this issue, this study proposes a hybrid prediction model that integrates the Seasonal
Autoregressive Integrated Moving Average with Exogenous Variables (SARIMAX) and Support Vector
Regression (SVR). The SARIMAX component captures linear trends and seasonality by incorporating
external factors such as patient volume and e-catalog procurement status, while the SVR component corrects
nonlinear residual patterns. The dataset consisted of daily drug consumption records, patient visits, and
procurement data from the Dr. Tadjuddin Chalid Makassar Hospital. The Experimental results demonstrate
that the hybrid SARIMAX–SVR model reduces the Root Mean Square Error (RMSE) by approximately 44%
compared to standalone SARIMAX, across different drug demand categories. This approach provides a more
adaptive, accurate, and computationally efficient forecasting framework to support decision-making in
pharmaceutical supply chain management under the JKN scheme.
1 INTRODUCTION
The availability of the right amount and time of
medicine is a vital element in maintaining the quality
of health services, especially in the National Health
Insurance (JKN) system, which covers the majority
of the Indonesian population. Inaccuracies in
planning drug needs can lead to two main problems:
overstock, which causes cost inefficiencies, or
stockouts, which have a direct impact on the
continuity of patient therapy. In practice, this
challenge is increasingly complex because the
dynamics of drug demand are influenced by various
factors such as seasonal disease trends, fluctuations
in the number of patient visits, and limitations in e-
catalog-based procurement systems.
In article (Satibi et al., 2020), the drug supply
chain management system in the JKN era still faced
problems in ensuring the availability of drugs on an
ongoing basis. This is exacerbated by the lack of
utilization of data-based predictive approaches in the
demand planning process. Traditional time series
methods such as ARIMA or SARIMA are often used
a
https://orcid.org/0009-0003-5389-4634
b
https://orcid.org/0000-0001-5706-939X
for demand forecasting but tend to be limited in
handling non-linear patterns and instability that are
common in drug demand data.
To accommodate such complexity, the Seasonal
Autoregressive Integrated Moving Average with
Exogenous Variables (SARIMAX) model offers
advantages in modeling both trend and seasonality
while allowing the inclusion of exogenous variables
such as patient numbers and e-catalog status (Alharbi
& Csala, 2022). However, despite these strengths,
SARIMAX remains limited in capturing nonlinear
variability and sudden spikes in demand.
Recent studies have increasingly adopted hybrid
time-series models that integrate statistical and
machine learning techniques for healthcare
forecasting. For instance, Zhao and Zhang (2023)
proposed a SARIMA–ETS–SVR hybrid for
influenza incidence prediction, achieving up to 18%
accuracy improvement. Similarly, Benitez et al.
(2023) combined SARIMAX and LSTM for solar
energy prediction, showing that hybrid architectures
can effectively capture both linear and nonlinear
temporal structures. In the pharmaceutical domain,
(Alzami et al., 2024) employed SARIMAX with
Palelleng, R. and Mokobombang, N. N. R. A.
A Hybrid SARIMAX-SVR Model for Drug Demand Prediction.
DOI: 10.5220/0014272400004928
Paper published under CC license (CC BY-NC-ND 4.0)
In Proceedings of the 1st International Conference on Research and Innovations in Information and Engineering Technology (RITECH 2025), pages 209-216
ISBN: 978-989-758-784-9
Proceedings Copyright © 2025 by SCITEPRESS – Science and Technology Publications, Lda.
209

exogenous weather factors to forecast food and
beverage demand, while (Alsaber et al., 2024)
demonstrated the potential of SVR in predicting
biologic therapy response among rheumatoid arthritis
patients.
Building on these findings, the present study
extends hybrid SARIMAX–SVR modeling into the
context of hospital drug demand forecasting—an area
rarely explored in Indonesia—by integrating patient
volume and e-catalog procurement data as exogenous
factors.
Based on these problems, this study proposed a
hybrid SARIMAX-SVR model approach to improve
the accuracy of predicting drug needs in the JKN
system. The data used were daily drug supply data
from the Central General Hospital (RSUP) Dr.
Tadjuddin Chalid Makassar for the last two years,
complemented by data on the number of patient visits
and e-catalog procurement status as exogenous
variables. The main objectives of this study were to
(1) develop a SARIMAX-SVR-based drug demand
prediction model, (2) evaluate the performance of the
model compared to conventional approaches, and (3)
provide a decision support system that can be
implemented in data-based pharmaceutical logistics
planning at the national health service scale.
2 RESEARCH METHOD
This study proposed a drug demand prediction
approach based on a hybrid SARIMAX-SVR model.
The methodology consisted of three main stages:
SARIMAX model building, SVR model training
based on SARIMAX residuals, and prediction
performance evaluation using the Root Mean
Squared Error (RMSE) metric. The SARIMAX
model was chosen to capture the seasonal and linear
components of drug demand by incorporating
external factors, such as patient volume and
procurement policy. However, because SARIMAX
may fail to explain nonlinear dynamics and sudden
spikes in demand, Support Vector Regression (SVR)
with a Radial Basis Function (RBF) kernel was
applied to model the residual errors. The RBF kernel
was selected for its proven ability to capture
complex, non-linear relationships without excessive
overfitting, while maintaining computational
efficiency, making the SARIMAX–SVR hybrid
model both accurate and practical for hospital-level
forecasting systems. The dataset used includes daily
inventory data of more than 100 types of drugs at Dr.
Tadjuddin Chalid Hospital Makassar for three years
(2023-2024), as well as data on the number of patient
visits and e-catalog procurement status as exogenous
variables.
2.1 SARIMAX Model
Box and Jenkins (Pankratz.A, 2019) proposed the
ARIMA model, a series forecasting method. The
basic idea of the ARIMA model is to consider the
observational dataset over time as a random set and
use a mathematical model to approximate this
sequence.
Recent studies have proposed various hybrid
forecasting approaches that integrate SARIMAX
with deep learning or ensemble-based machine
learning methods such as LSTM and XGBoost to
address the limitations of linear time-series models.
A study by (Benitez et al., 2023) applied a hybrid
SARIMAX–LSTM model to solar irradiance
forecasting in the Philippines. The study found that
although the hybrid model outperformed standalone
SARIMAX or LSTM in certain regions, it did not
consistently produce superior results across all
datasets. The performance was highly dependent on
the data characteristics, and the model required
substantial computational resources and tuning
efforts. In another study (Lee et al., n.d.),
SARIMAX–LSTM and SARIMAX–SVR were used
for electric load forecasting. Their findings showed
that SARIMAX–LSTM performed well in capturing
peak demands, whereas SARIMAX–SVR achieved
better overall accuracy and stability in multivariate
settings.
In recent epidemiological research(Man et al.,
2023), a SARIMA–XGBoost hybrid model was used
to predict daily incidence of hand, foot, and mouth
disease (HFMD) in Xinjiang, China. The study
followed a two-stage modeling process: first, fitting
a SARIMA model, followed by residual correction
using XGBoost with optimized hyperparameters,
such as max depth and learning rate, via
GridSearchCV. The hybrid model achieved a
significantly lower RMSE of 112.51, compared to
147.51 (SARIMA alone), 152.75 (XGBoost alone),
129.43 (LSTM), and 167.01 (SVR), demonstrating
its superiority and improved R² by up to 25% over
base models.
The SARIMAX model is a form of SARIMA that
includes independent (exogenous) variables. The
SARIMAX model is denoted as (𝑝, 𝑑, 𝑞)(𝑃, 𝐷,
𝑄)𝑆(𝑋), where 𝑋 represents the exogenous variables.
These independent variables in the SARIMAX model
can be modeled using a multiple linear regression
equation. The general form of the SARIMAX model
(𝑝,𝑑,𝑞)(𝑃,𝐷,𝑄)
(𝑋) represents the linear
relationship between drug demand and its past
RITECH 2025 - The International Conference on Research and Innovations in Information and Engineering Technology
210

observations, seasonal components, and external
factors. This relationship can be expressed as follows
[8]:
𝑌
= 𝑐 +
∑
𝜑
𝑌
+
∑
𝜃
𝜀
+
∑
𝛷
𝑌
·
+
∑
𝛩
𝜀
·
+ 𝛽
+ 𝛽
𝑉
,
+
𝛽
𝑉
,
+ ⋯ + 𝛽
,
+ 𝜀
(1)
Where:
𝑌𝑡 = drug demand at time t
C = constant
p,d,q = orders of the non-seasonal ARIMA
components (autoregressive,
differencing, moving average)
P,D,Q,s = orders of the seasonal ARIMA
components (seasonal AR, seasonal
differencing, seasonal MA, and
seasonal period)
Φi = autoregressive coefficients
Θj = moving average coefficients
Φk,Θl = seasonal autoregressive and moving
average coefficients
Vj,t = exogenous variable jjj at time ttt
(e.g., number of patients, e-catalog
status, weekday dummy)
𝛽0, 𝛽1,..,𝛽m = regression coefficients of the dummy
variables
ε
t
= residual (white noise)
In this formulation, 𝑌
denotes the drug demand at
time 𝑡, while the terms 𝜙
, 𝜃
, Φ
, and Θ
represent
the autoregressive (AR) and moving average (MA)
coefficients for both non-seasonal and seasonal
components. Exogenous variables 𝑉
,
— such as
patient volume or e-catalog status — are included
with regression coefficients 𝛽
,𝛽
,…,𝛽
. The
residual term 𝜀
captures random disturbances or
unexplained variation. This formulation allows the
SARIMAX model to incorporate both temporal
dynamics and external influences in predicting
hospital drug demand
In this research, the SARIMAX model was fitted
using the Auto-ARIMA procedure, which
automatically selects the optimal (p,d,q)(P,D,Q)s
parameters based on information criteria (AIC/BIC),
while simultaneously including the exogenous
variables. This ensures that both the temporal
dynamics (trend, seasonality, autoregressive and
moving average components) and the external
influences are captured in the model.
It is important to note that the formulation above
is consistent with previous SARIMAX-based
forecasting studies. For instance (Alharbi & Csala,
2022)(Alzami et al., 2024)applied a SARIMAX
model with exogenous weather variables in food and
beverage demand forecasting, and [MDPI, 2022]
used a similar SARIMAX formulation to forecast
container throughput at the Port of Singapore. Both
studies explicitly adopted the same mathematical
structure, combining ARIMA components with
seasonal adjustments and exogenous regressors, thus
validating the methodological basis of the present
research
The Seasonal Autoregressive Integrated Moving
Average with Exogenous Variables (SARIMAX)
model was used to capture the linear components of
drug demand patterns, including trends and
seasonality. The model also integrates exogenous
variables, namely, the number of patients and
ecatalog status, which are assumed to have an
influence on drug demand. The SARIMAX model is
trained on the training data and produces an initial
predicted value along with the residual (the difference
between the prediction and actual realization).
2.2 SVR Model (Support Vector
Regression)
To address nonlinear patterns that cannot be fully
explained by SARIMAX, the residuals from the
SARIMAX model were remodeled using the Support
Vector Regression (SVR) method. SVR constructs a
regression function in a high-dimensional feature
space by mapping the input data through a kernel
function, enabling the model to capture complex
relationships To capture the nonlinear relationships
left unexplained by SARIMAX, the residuals are
modeled using the Support Vector Regression (SVR)
function. The general regression form of SVR is
defined as follows (Zhao & Zhang, 2023):
𝑓
(
𝑥
)
=
∑(
𝛼
− 𝛼
∗
)
𝐾
(
𝑥
,𝑥
)
+ 𝑏 (2)
where:
• m = number of support vectors
• α
i
and α
i
*
= Lagrange multipliers obtained from
the optimization problem,
• K (x
i
,x) = kernel function that measures the
similarity between support vectors x
i
dan x,
• b = bias term.
In this equation, 𝑚 represents the number of
support vectors, while 𝛼
and 𝛼
∗
are Lagrange
multipliers obtained through optimization. The kernel
function 𝐾
(
𝑥
,𝑥
)
measures the similarity between the
input vectors, and 𝑏 denotes the bias term. This
formulation allows SVR to construct a regression
A Hybrid SARIMAX-SVR Model for Drug Demand Prediction
211

surface that best fits the residual patterns from
SARIMAX, minimizing prediction error within a
defined margin.
The performance of SVR largely depends on the
choice of kernel function, which transforms the input
space into a higher-dimensional feature space to
capture nonlinear relationships. The general
definition of the kernel function is given by Equation
(3) (Zhao & Zhang, 2023)(Alsaber et al., 2024):
𝐾𝑥
,𝑥
= 𝜑
(
𝑥
)
,𝜑𝑥
(3)
Where
g
j
are basis functions representing the feature
mapping ϕ(x).
Among the various kernel functions, this study
employed the Radial Basis Function (RBF) kernel,
expressed as:
𝐾𝑥
,𝑥
=exp
−𝛾 𝑥
− 𝑥
(4)
In this equation, 𝐾𝑥
,𝑥
represents the kernel
value, which measures the similarity between two
input vectors. The parameter 𝛾controls the influence
of individual data points — a larger 𝛾produces a more
localized kernel, making the model more sensitive to
sudden changes or spikes in drug demand. The term
∥𝑥
−𝑥
∥
denotes the squared Euclidean distance
between the two vectors. This function therefore
expresses an exponential similarity: when two inputs
are very close, the kernel value approaches 1; as the
distance increases, the kernel value rapidly decays
toward 0.
The SVR model used default hyperparameters (C
= 1.0, ε = 0.1, γ = ' scale') to maintain computational
efficiency and focus on evaluating the hybrid model.
Notably, benchmarks across multiple datasets have
found default hyperparameter settings to perform
non-inferiorly compared to tuned values, supporting
the validity of this pragmatic approach. The RBF
kernel was chosen because of its flexibility and
robustness in modeling nonlinear, fluctuating drug
demand data
2.3 Evaluation Model
A performance evaluation was performed using the
Root Mean Squared Error (RMSE) metric to measure
the average deviation between the predicted and
actual values. The RMSE is used because it is
sensitive to outliers and can reflect the overall
prediction error. To evaluate prediction accuracy, this
study employs the Root Mean Squared Error (RMSE)
metric, which measures the average magnitude of
prediction errors. It is defined as follows (Zhao &
Zhang, 2022):
𝑅𝑀𝑆𝐸 = √((1/𝑛) ∑_(𝑡 = 1)^𝑛(𝑦
− ŷ
)^2 ) (5)
Where:
𝑦
= actual demand at time 𝑡,
𝑦
= predicted demand at time 𝑡,
𝑛= number of observations.
In this formula, 𝑛 denotes the number of
observations, 𝑦
is the actual value, and 𝑦
is the
predicted value. Lower RMSE values indicate better
model performance. Because RMSE penalizes large
deviations more strongly, it is particularly suitable for
assessing drug demand forecasts where occasional
spikes can greatly influence hospital inventory
decisions.
RMSE was selected because of its sensitivity to
large deviations, making it appropriate for evaluating
the forecasting accuracy of hospital demand data. The
models were evaluated under two scenarios: a single
SARIMAX model and a hybrid SARIMAX-SVR
model (combined SARIMAX prediction and SVR
correction based on residual data). Comparisons were
made for all drug types and averaged by drug therapy
category to determine the consistency of the model
performance.
In terms of computational cost, the SARIMAX
model required around 2.1 seconds per drug using
stats models, while the SVR correction stage added
4.6 seconds per drug with GridSearchCV. Overall,
the hybrid SARIMAX–SVR model completed
training and prediction in less than seven seconds per
drug, making it feasible for batch forecasting in
hospital systems. Compared to models like
SARIMAX–LSTM, which may take over 20 seconds
per drug, SARIMAX–SVR offers a more efficient
and scalable solution.
3 RESULT AND DISCUSSION
Experiments were conducted on daily drug demand
data from Dr. Tadjuddin Chalid Hospital Makassar
for the period of 2023-2024. The dataset included
more than 100 types of drugs. The first step is data
preprocessing (data cleaning, differencing, and
normalization), followed by extracting demand
pattern features and seasonal features. Demand
patterns were classified into the following categories:
a.The smooth Demand has a normal pattern, b.Erratic
Demand is a need with a high quantity of variation, c.
Intermittent Demand is a need with high variation in
the interval between two needs, but has low variation
in quantity needs., d. Lumpy Demand is a need with
high variation in the interval of two needs and
RITECH 2025 - The International Conference on Research and Innovations in Information and Engineering Technology
212
quantity Classification of demand patterns can be
done using 2 classification coefficients, namely the
average demand interval (𝑝) and the square of the
coefficient of variation 𝐶𝑉2. The separation point of
each coefficient is p = 1.32 and 𝐶𝑉2= 0.49.
Extraction results from existing datasets: Smooth
Demand, 90 drugs; intermittent demand, 2 drugs;
erratic demand, 13 drugs; and Lumpy Demand, 6
drugs.
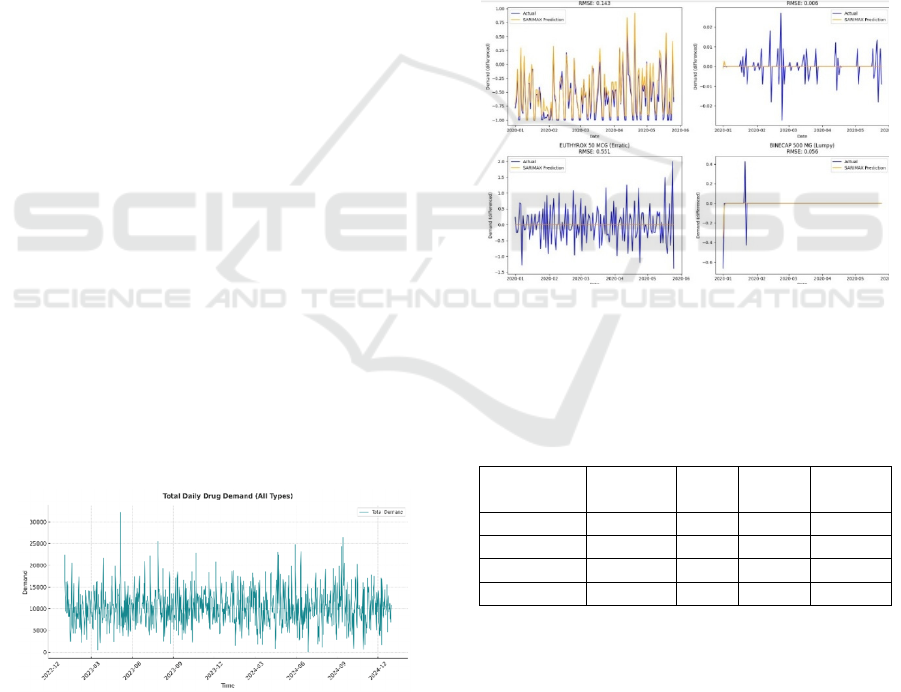
3.1 SARIMAX Model
We performed SARIMAX modeling on the drug data
using Python on Google Collab. Figure 1. shows drug
usage data from Dr. Tadjuddin Chalid Hospital
Makassar from 2023 to 2025. A general upward trend
is observed from 2023 to 2024. This indicates that the
need for drugs tends to increase over time. Although
there are fluctuations, the increase in total demand is
more consistent in 2024 than in the early 2023. The
demand pattern fluctuated sharply on a periodic basis
(rising and falling sharply every few days). This is
most likely due to weekly or monthly ordering
behavior, as well as healthcare activity (e.g., spikes at
the beginning of the working week). The amplitude
of the fluctuations was quite large, indicating high
volatility in drug demand. Some extreme
spikes/outliers (> 30,000) were observed, particularly
in early and mid-2023. For SARIMAX modeling,
AutoArima was used to automatically select the best
parameters for the SARIMAX model based on
historical data. Autoarima used a grid search
approach to try various combinations of parameters
(P, D, Q) and (P,D,Q,m) to find a model with the
smallest Akaike Information Criterion (AIC) or
Bayesian Information Criterion (BIC) values. The
smaller the AIC/BIC ratio, the better the model
explains the data without overfitting.
Figure 1: The Original Time Series.
Based on Figure 2., the sarimax model works quite
well for drugs in the smooth category. The demand is
quite regular, and fluctuations are small, and the
Sarimax predictions are quite accurate, following the
actual pattern well, and RMSE: 0.143 is quite low,
indicating a good prediction. However, for the other
three categories, the SARIMAX model does not work
sufficiently well. Intermittedly, many values are zero
or very small, with random spikes. The graph is
almost always flat (straight line at zero) and the model
fails to capture small and sporadic spikes in demand.
RMSE: 0.006 appears low, but this can be misleading,
as the model only estimates the mean of zero. For
large and irregular Erratic Fluctuations, SARIMAX
Prediction: Unable to keep up with sharp spikes and
dips; RMSE: 0.551–the highest among all, indicating
poor prediction performance. On Lumpy, almost
always zero, with occasional large spikes. SARIMAX
Prediction: Straight line close to zero cannot capture
occasional demands. The RMSE of 0.056 is low, but
the model clearly does not capture surge dynamics.
Figure 2: SARIMAX Model based on Drug Category.
The following are the results of the RMSE
evaluation of the SARIMAX model based on the drug
category.
Table 1: RMSE Evaluation SARIMAX Model.
Demand
Type
Amount of
drug
Min
RMSE
Max
RMSE
Avg
RSME
Smooth 90 0.000 1.037 0.240
Intermittent 2 0.006 0.047 0.026
Erratic 13 0.078 0.735 0.477
Lumpy 6 0.000 0.611 0.180
Based on Table 1., the Smooth Demand with a
total of 90 types of drugs, with an average RMSE of
0.240, is quite low for a statistical model. This
indicates that SARIMAX is suitable for stable
demand and exhibits a clear seasonal pattern or trend.
In the Intermittent Demand category for the two
drugs, the Average RMSE of 0.026 was very low.
However, the number of drugs was too small (n = 2);
therefore, this result is not representative. For the
A Hybrid SARIMAX-SVR Model for Drug Demand Prediction
213
Erratic Demand with 13 drugs, the highest RMSE was
0.735, and the average RMSE was 0.477, which was
the worst compared to the others. This shows that it is
very difficult to handle erratic patterns because
fluctuations cannot be captured using a
linear/seasonal approach. This supports the need for
hybrid or nonlinear models such as SVR. The average
RMSE was 0.180, which is quite good. However, the
range of RMSE is very wide (0.000–0.611), which
means that some cases can be predicted well (perhaps
due to seasonal patterns), but others fail, perhaps due
to sparsity/volatility. SARIMAX has an inconsistent
performance for this type of demand.
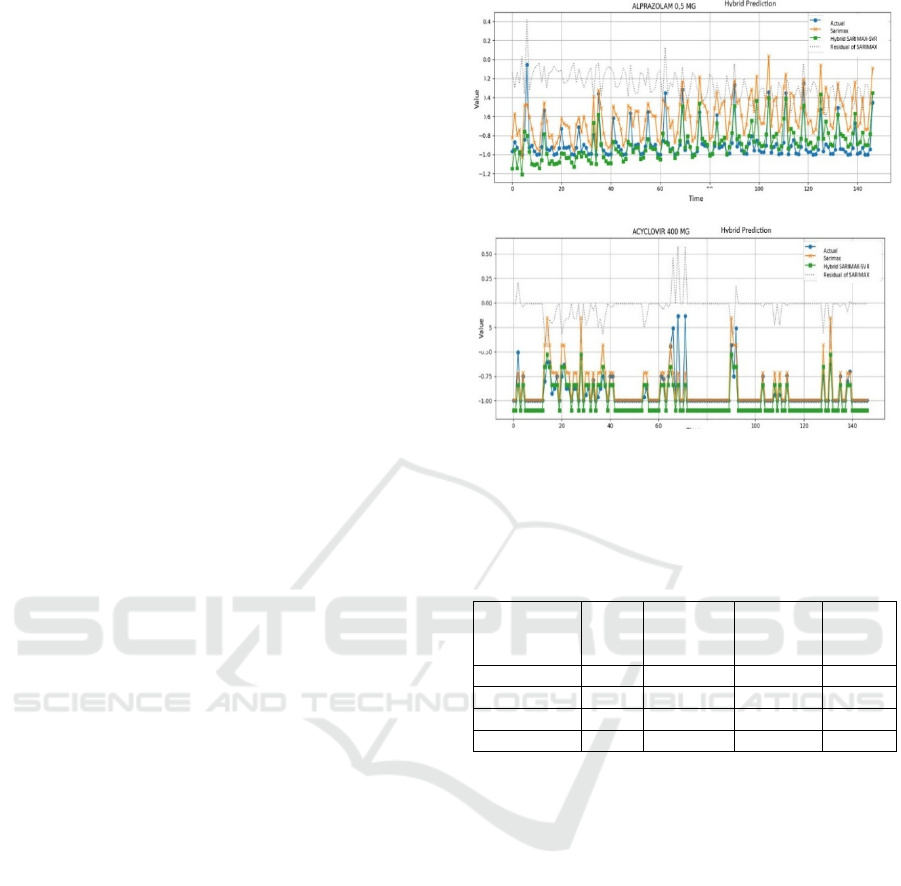
3.2 Hybrid Model with SVR
The SVR model uses residual data from the
SARIMAX model to identify nonlinear patterns. In
Figure 3a. SARIMAX predictions appear volatile and
tend to overreact to short-term fluctuations. The
model often overestimates values, particularly when
the actual demand is stable or low, and fails to capture
the long-term stability observed in the data. The
residuals display a repetitive pattern, indicating that
the model does not fully capture the underlying
dynamics and that additional nonlinear information
remains unexplained. By contrast, the hybrid
SARIMAX–SVR model produces predictions that
are consistently closer to the actual values, more
stable against minor noise, and less prone to extreme
deviations. The ability of the hybrid to maintain
consistency when the actual data tends to be low and
stable is a major advantage.
Likewise, in Figure 3b, SARIMAX is able to
follow certain spikes but performs poorly in periods
with zero demand or sudden fluctuations, leading to
large deviations from the actual values. Again, the
residuals reveal structured patterns, suggesting
incomplete modeling of the series. The hybrid model
demonstrates improved flexibility by reducing errors
at both spikes and low-value regions, producing
predictions that are generally more aligned with the
observed demand. The following are the RMSE
evaluation results for the hybrid model (SVR
correction based on residual data):
(a)
(b)
Figure 3: Comparison of SARIMAX vs Hybrid
SARIMAX-SVR predictions for selected drug: (a)
Alprazolam 0.5 mg), (b) Acyclovir 400 mg.
Table 2: RMSE Evaluation SARIMAX and SVR Model
Hybrid.
Demand Type
Amount
of drug
Avg RMSE
SARIMAX
Avg RMSE
SVR
Avg
RMSE
Hybri
d
Smooth 90 0.239957 0.115559 0.115559
Intermittent 2 0.026251 0.050815 0.050815
Erratic 13 0.476634 0.368423 0.368423
Lum
py
6 0.179767 0.166393 0.166393
Based on Table 2., for Smooth Demand (90
drugs), the average RMSE dropped to 0.115 from
0.240 in SARIMAX. A decrease of more than 50%
shows that the hybrid model improved the prediction
accuracy for stable patterns. Min RMSE = 0,
indicating that some predictions are precise.
Intermittent Demand (2 drugs), RMSE decreased to
0.0508 from 0.026 in SARIMAX, but the amount of
data is so small that even small fluctuations can have
a significant effect. Max RMSE is still low (<0.1),
meaning the prediction is still accurate in general.
Erratic Demand (13 drugs), the average RMSE
dropped from 0.477 to 0.360, showing significant
improvement. However, the RMSE value was still
quite high, indicating that erratic patterns remained
difficult to predict. The hybrid model is helpful but
not optimal, and there may be a need for a more
adaptive model. Lumpy Demand (six drugs), the
average RMSE dropped from 0.180 to 0.166, a small
but statistically significant improvement. Max RMSE
RITECH 2025 - The International Conference on Research and Innovations in Information and Engineering Technology
214

dropped slightly from 0.611 to 0.503, hybrid model
more stable at extremes.
Compared to other hybrid models such as
SARIMAX–LSTM or SARIMA–XGBoost reported
in previous studies [5–7], the SARIMAX–SVR offers
shorter training times (<7s per drug) with competitive
accuracy (44% RMSE reduction), making it more
practical for hospital forecasting systems.
Table 3: RMSE Comparison of SARIMAX and Hybrid
SARIMAX -SVR.
Drug Name RMSE
SARIMAX
RMSE
Hybri
d
Improvement
Thyrozo 5
MG
1.000000 0.000000 1.000000
INH 100
MG
1.005824 0.104220 0.901604
Depakote
ER 250 MG
0.984608 0.116687 0.867922
The comparison of RMSE for SARIMAX and
Hybrid SARIMAX - SVR for several drugs is as
shown in Table 3. Based on the Table 3, these three
drugs showed a drastic performance improvement of
> 86%–100%. This is a strong indicator that
SARIMAX residuals contain hidden patterns can be
modelled by SVR. The hybrid model (SARIMAX +
SVR) consistently outperforms SARIMAX,
especially for: Drugs with irregular demand patterns
and those that may exhibit lumpy or erratic
characteristics. [
3.3 Comparative Context
The hybrid SARIMAX–SVR model demonstrated
superior performance compared to the single
SARIMAX model, achieving an average RMSE
reduction of approximately 44% across different drug
demand categories. This improvement aligns with the
results of Zhao and Zhang (2023), who reported a
38% error reduction in hybrid influenza forecasts, and
Man et al. (2023), whose SARIMA–XGBoost model
reduced RMSE by over 25% in epidemiological
prediction.
Compared with deep-learning-based hybrids such
as SARIMAX–LSTM (Benitez et al., 2023) or
SARIMA–XGBoost (Man et al., 2023), the proposed
SARIMAX–SVR model offers competitive accuracy
while maintaining computational efficiency—
training and prediction completed in under seven
seconds per drug. This advantage is particularly
relevant in hospital environments, where rapid and
scalable forecasting is essential.
Moreover, the integration of SVR effectively
corrected nonlinear residuals, stabilizing predictions
in erratic and lumpy demand categories. These
findings are consistent with Liu and Han (2023) and
Li and Zhao (2024), who emphasized the importance
of residual-based learning in improving hybrid time-
series robustness. Thus, the SARIMAX–SVR model
not only refines prediction accuracy but also offers
practical feasibility for routine pharmaceutical
demand management.
4 CONCLUSIONS
This study proposes a drug demand prediction
approach based on the SARIMAX–SVR hybrid
model to improve the accuracy of drug demand
forecasting in JKN services. Based on the evaluation
of drug supply data from Dr. Tadjuddin Chalid
Makassar Hospital, the hybrid model demonstrated
superior predictive performance compared to the
single approach, with an average RMSE reduction of
approximately 44% across various drug demand
categories.The SARIMAX model is effective in
capturing linear and seasonal patterns, whereas SVR
can correct nonlinear and fluctuating prediction
errors. The integration of the two enables a more
adaptive, accurate, and suitable prediction system to
support informed decision making in hospital
pharmacy logistics management. This study was
limited to data from a single hospital; future research
should expand to multiple hospitals across different
regions of Indonesia to improve generalizability
within the JKN system
ACKNOWLEDGEMENTS
The authors would like to thank Dr. Tadjuddin Chalid
Makassar Hospital, for providing access to the drug
datasets essential to this research.(Fan et al., 2022),(A
et al., 2025)(Aravazhi, 2021)
REFERENCES
A, S., Christo, M. S., & Elizabeth, J. V. (2025). A hybrid
approach to time series forecasting: Integrating
ARIMA and prophet for improved accuracy. Results in
Engineering, 27(June), 105703.
https://doi.org/10.1016/j.rineng.2025.105703
Alharbi, F. R., & Csala, D. (2022). A Seasonal
Autoregressive Integrated Moving Average with
Exogenous Factors (SARIMAX) Forecasting Model-
Based Time Series Approach. Inventions, 7(4).
https://doi.org/10.3390/inventions7040094
A Hybrid SARIMAX-SVR Model for Drug Demand Prediction
215

Alsaber, A. R., Al-Herz, A., Alawadhi, B., Doush, I. A.,
Setiya, P., AL-Sultan, A. T., Saleh, K., Al-Awadhi, A.,
Hasan, E., Al-Kandari, W., Mokaddem, K., Ghanem,
A. A., Attia, Y., Hussain, M., AlHadhood, N., Ali, Y.,
Tarakmeh, H., Aldabie, G., AlKadi, A., & Alhajeri, H.
(2024). Machine learning-based remission prediction in
rheumatoid arthritis patients treated with biologic
disease-modifying anti-rheumatic drugs: findings from
the Kuwait rheumatic disease registry. Frontiers in Big
Data, 7. https://doi.org/10.3389/fdata.2024.1406365
Alzami, F., Salam, A., Rizqa, I., Irawan, C., Andono, P. N.,
Aqmala, D., & Sartika, M. (2024). Demand Prediction
for Food and Beverage SMEs Using SARIMAX and
Weather Data. Ingenierie Des Systemes d’Information,
29(1), 293–300. https://doi.org/10.18280/isi.290129
Aravazhi, A. (2021). Hybrid Machine Learning Models for
Forecasting Surgical Case Volumes at a Hospital. AI
(Switzerland), 2(4), 512–526.
https://doi.org/10.3390/ai2040032
Ashtar, D., Mohammadi Ziabari, S. S., & Alsahag, A. M.
M. (2025). Hybrid Forecasting for Sustainable
Electricity Demand in The Netherlands Using
SARIMAX, SARIMAX-LSTM, and Sequence-to-
Sequence Deep Learning Models. Sustainability
(Switzerland), 17(16).
https://doi.org/10.3390/su17167192
Benitez, I. B., Ibañez, J. A., Lumabad, C. I. I. I. D., Cañete,
J. M., & Principe, J. A. (2023). Day-Ahead Hourly
Solar Photovoltaic Output Forecasting Using
SARIMAX, Long Short-Term Memory, and Extreme
Gradient Boosting: Case of the Philippines.
Energies_MDPI, 16.
https://doi.org/10.3390/en16237823
Fan, B., Peng, J., Guo, H., Gu, H., Xu, K., & Wu, T. (2022).
Accurate Forecasting of Emergency Department
Arrivals With Internet Search Index and Machine
Learning Models: Model Development and
Performance Evaluation. JMIR Medical Informatics,
10(7), 1–17. https://doi.org/10.2196/34504
Lee, J., Cho, Y., Lee, J., & Ph, D. (n.d.). National - scale
electricity peak load forecasting : Traditional , machine
learning , or hybrid model ? National - scale electricity
peak load forecasting : Traditional , machine learning
, or hybrid model ? 1–42.
Man, H., Huang, H., Qin, Z., & Li, Z. (2023). Analysis of a
SARIMA-XGBoost model for hand, foot, and mouth
disease in Xinjiang, China. Epidemiology and Infection,
151. https://doi.org/10.1017/S0950268823001905
Pankratz.A. (2019). Forecasting with Unvariate Box-
Jenkins Model Concept and Cases. In John Wily &
Sons,Inc. Indiana (Vol. 11, Issue 1).
http://scioteca.caf.com/bitstream/handle/123456789/10
91/RED2017-Eng-
8ene.pdf?sequence=12&isAllowed=y%0Ahttp://dx.do
i.org/10.1016/j.regsciurbeco.2008.06.005%0Ahttps://
www.researchgate.net/publication/305320484_SISTE
M_PEMBETUNGAN_TERPUSAT_STRATEGI_ME
LESTARI
Satibi, S., Copalcanty, F. A., Tuko, E., & Sawatiandari, L.
G. (2020). Pharmaceutical suply chain management in
supporting drugs avaibility in the jkn era in indonesia.
International Journal of Scientific and Technology
Research, 9(4), 3034–3038.
Teja, M. D., & Rayalu, G. M. (2025). Hybrid time series
and machine learning models for forecasting
cardiovascular mortality in India: an age specific
analysis. BMC Public Health, 25(1).
https://doi.org/10.1186/s12889-025-23318-7
Yulianti, R., Amanda, N. T., Notodiputro, K. A., Angraini,
Y., & Mualifah, L. N. A. (2025). Comparison of Sarima
and Sarimax Methods for Forecasting Harvested Dry
Grain Prices in Indonesia. Barekeng, 19(1), 319–330.
https://doi.org/10.30598/barekengvol19iss1pp319-330
Zhao, D., & Zhang, R. (2023). A new hybrid model
SARIMA-ETS-SVR for seasonal influenza incidence
prediction in mainland China. Journal of Infection in
Developing Countries, 17(11), 1581–1590.
https://doi.org/10.3855/jidc.18037
RITECH 2025 - The International Conference on Research and Innovations in Information and Engineering Technology
216
