
Predictive Modelling for Diabetes Mellitus with Respect to Basic Medical
History
Patrick Purta, Aryan Mishra, Vishal Reddy Vadde, Ruthvika Bojjala, Gopichand Jagarlamudi and
Bonaventure Chidube Molokwu
a
Department of Computer Science, College of Engineering and Computer Science, California State University,
Sacramento, U.S.A.
Keywords:
Diabetes Mellitus, SMOTE, SVM-SMOTE, SMOTE-ENN, Predictive Modeling, Risk Assessment, Clinical
Decision Support, Medical History.
Abstract:
In our work herein, we observed how three (3) common oversampling techniques - SMOTE, SMOTE-ENN,
and SVM-SMOTE - affect the performance of Machine Learning (ML) models applied towards predicting
diabetes risk with reference to the Pima-Indian (Akimel O’odham) Diabetes dataset. Our aim was to figure
out if using these methods to mitigate class imbalance, in a medical dataset, might cause the ML models to
overfit - in other words, they tend to do very well on the training data but lose fitness and accuracy on new data.
Our project began from a simple question: “Can oversampling fix class imbalances, with respect to a given
dataset, without hurting the model’s ability to generalize?” Previous studies have shown that oversampling can
help balance target-classes within a dataset, but these studies do not always address the risk of overfitting. To
answer this, we combined each oversampling technique via three (3) ensemble methods - Extra Trees, Gradi-
ent Boosting, and Random Forest - and compared their performances via cross-validation objective functions.
Our results reveal that, although each method improves the results or metrics on the training data, they tend to
under-perform slightly on unseen test or sample data. This suggests that while oversampling is a useful strat-
egy, it must be applied with caution to avoid overfitting. These insights are important for refining predictive
models, especially in healthcare contexts where reliable performance is critical.
1 INTRODUCTION
Working on this project has been like untangling a
knot in a routine we all know too well, balancing the
scales when it comes to data. In healthcare, especially
with something as crucial as diabetes diagnosis, hav-
ing a dataset where the positive cases are much fewer
than the negatives is common; and it often leaves our
models struggling to learn the right patterns. Imagine
trying to hear a soft whisper in a loud room; the less
frequent instances get drowned out.
We started exploring this issue because we noticed
something interesting with oversampling techniques
like Synthetic Minority Over-sampling Technique
(SMOTE), SMOTE-ENN (SMOTE + Edited Nearest
Neighbors), and SVM-SMOTE (Support Vector Ma-
chine SMOTE). These methods essentially “create”
more examples from the minority class so that every
voice in the dataset gets a chance to be heard. How-
ever, while these techniques boosted performance
a
https://orcid.org/0000-0003-4370-705X
during training, our models - built with Extra Trees,
Gradient Boosting, and Random Forest - sometimes
became too focused on the training data, showing
signs of overfitting when it came time to predict new
cases.
This raised a pressing question for our team: “Can
we use oversampling to balance the dataset without
inadvertently making the models overconfident with
reference to the training examples?” With the Pima-
Indian Diabetes dataset (Nnamoko and Korkontzelos,
2020) as our test case, we set out to find an answer
because, in healthcare, even the smallest error(s) can
yield big consequences. The goal is not just to record
high objective-function scores during training, but to
build tools that work reliably when it really counts.
To address this issue, we employed a thorough
hands-on approach. Individually, we applied each
oversampling technique separately to our training
data; thereafter, we carefully evaluated how different
ensemble models performed using a cross-validation
strategy. By comparing training and testing results,
Purta, P., Mishra, A., Vadde, V. R., Bojjala, R., Jagarlamudi, G. and Molokwu, B. C.
Predictive Modelling for Diabetes Mellitus with Respect to Basic Medical History.
DOI: 10.5220/0013692100003985
Paper published under CC license (CC BY-NC-ND 4.0)
In Proceedings of the 21st International Conference on Web Information Systems and Technologies (WEBIST 2025), pages 343-349
ISBN: 978-989-758-772-6; ISSN: 2184-3252
Proceedings Copyright © 2025 by SCITEPRESS – Science and Technology Publications, Lda.
343

we aimed at a better understanding of where our mod-
els were getting it right and where they were losing
their grip.
At its heart, our project is more than just statis-
tics - it is about making a realistic difference in how
we use technology in healthcare. By delving deeper
into the balance between correcting data imbalances
and avoiding overfitting, we do hope that our work
can guide the development of more robust as well as
trustworthy diagnostic tools that put patient-care first.
2 RELATED LITERATURE
In our effort to improve how machines predict dia-
betes, we dug into a lot of previous work to see how
others have handled similar challenges. This review
granted us insights into the past approaches and/or
methodologies.
2.1 Background of the Work
Researchers have long struggled with imbalanced
data, especially in healthcare, where the number
of positive cases (diabetes diagnosis) is often much
smaller than the negative cases. One of the earliest
breakthroughs came with the introduction of SMOTE
(Chawla et al., 2002), which set the stage for creat-
ing synthetic examples to balance the dataset. Since
then, numerous projects have applied these methods
- especially to datasets like the Pima-Indian-Indian
Diabetes dataset - to better understand how boosting
the minority class can help the overall model. How-
ever, these projects also revealed a common down-
side: while oversampling improves training results,
it sometimes leads the models to perform less effec-
tively when faced with new data.
2.2 Building a Strong Knowledge Base
A number of articles have reinforced the idea that
oversampling techniques such as SMOTE, SMOTE-
ENN, and SVM-SMOTE can help level the playing
field during model training - by providing more ex-
amples from the under-represented class. For exam-
ple, SVM-RBF: Support Vector Machine (SVM) with
Radial Basis Function (RBF), Decision Tree, Naive
Bayes, and RIPPER learning algorithms were cou-
pled with SMOTE to improve classification perfor-
mance on the Pima-Indian dataset. Studies that com-
pared these techniques have shown that although they
improve the class balance during training, they can
also make a model too “comfortable” with the train-
ing data, resulting in overfitting(Santos et al., 2018).
In other words, the model learns the training data so
well that it struggles to adapt when shown data it has
not seen before. Researchers (Poornima and R., 2024)
have also experimented with ensemble methods - e.g.
Extra-Trees, Random Forest(Olisah et al., 2022), Gra-
dient Boosting, etc. - highlighting both the benefits
and the challenges of combining these oversampling
techniques with robust classifiers(Zhang et al., 2024).
2.3 Theoretical Support and
Methodological Framework
What ties all these together is the well-known trade-
off between reducing bias and increasing variance.
Oversampling helps reduce bias by making sure the
model gets trained on sufficient examples of the mi-
nority class, but it can also lead to higher variance -
meaning that the model might not perform well on
unseen data. Several literature supports using cross-
validation as a way to tackle this problem. Cross-
validation (CV) helps check whether a model’s good
performance on the training data transcends to when
it encounters new data. Many studies (Santos et al.,
2018) have used this approach to ensure that the ben-
efits of oversampling are not lost due to overfitting.
This blend of theory and practical provides the frame-
work for our work herein - giving us guidance on how
to set up our experiments and interpret our results.
By examining the aforementioned past efforts and
work — early from the development of SMOTE to
recent studies on ensemble methods — we have built
a solid foundation for our work herein. Our review
of related literature not only highlights the strengths
and weaknesses of existing methods, but it also high-
lights areas where improvements can be made. Thus,
this background supports our goal towards striking
an ideal balance between fixing data imbalances and
keeping our models adaptable in real-world health-
care domains (Mooney, 2018; Lugat, 2021).
3 PROPOSED FRAMEWORK
AND METHODOLOGY
3.1 Formalism with Respect to the
Problem Statement
Given a medical dataset, D = (x
i
, y
i
), for i = 1 . . . n,
and with input features, x
i
∈ R
d
, and binary outcomes,
y
i
∈ {0, 1}, where class imbalance exists such that:
n
∑
i=1
y
i
<<
n
∑
i=1
(1 − y
i
)
WEBIST 2025 - 21st International Conference on Web Information Systems and Technologies
344
i.e. the number of diabetic cases, y
i
, is much
smaller than non-diabetic cases, 1 − y
i
; the goal is
to develop a robust classification function: f (x) :
R
d
→ {0, 1}, such that f (x) accurately predicts the
presence of diabetes (outcome = 1) using ensemble
classifiers, while reducing the effects of class im-
balance via oversampling techniques. This leads to
the following optimization objective: Minimize over
f ∈ F : L( f (x), y)
subject to the training set being
balanced via an oversampling method, O, where O ∈
{SMOTE, SMOTE-ENN, SVM-SMOTE}.
3.2 Methodology Overview
1. Data Preparation: We began by cleaning the
dataset — replacing zero-values in medically crit-
ical fields (like glucose level, blood pressure,
BMI, etc.) with NaN-values, and then imputing the
missing values using the KNN-Imputer method.
This helps ensure the model is not biased via in-
valid misleading inputs.
2. Train-Test Split: The dataset was split into train-
ing and testing sets using stratified sampling in a
bid to preserve the proportion of diabetic and non-
diabetic cases in both sets.
3. Oversampling the Minority Class: We tested three
(3) widely-used oversampling techniques: SMOTE:
Generates synthetic samples for the minority class
based on k-nearest neighbors. SMOTE-ENN: Com-
bines SMOTE with Edited Nearest Neighbors to
also clean noisy samples. SVM-SMOTE (Demidova
and Klyueva, 2017): A variant of SMOTE that uses
an SVM to better define the border of the minority
class.
4. Feature Scaling and Standardization: After impu-
tation, we applied a Quantile Transformer to stan-
dardize the data and reduce skewness. This step
is crucial before training, especially when using
models that are sensitive to large-scale data val-
ues.
5. Model Training: For each oversampling tech-
nique, we trained three (3) models — Random
Forest, Extra Trees, and Gradient Boosting — on
the resampled training data.
6. Model Evaluation: Finally, we evaluated each
model using multiple metrics such as Accuracy,
Precision, Recall, F1-score, AUC (Area Under the
Curve), and MCC (Matthews Correlation Coeffi-
cient). This helped us understand not just how ac-
curate the models were, but how well they handled
both classes (Kaliappan et al., 2024).
3.3 Formal Algorithm
The formal algorithm for the Oversampling and
Model-Training Pipeline begins with the input of a
dataset, D, an oversampler, O, and a classifier, C,
with the aim of producing a trained model, M, as
the output. Initially, the dataset, D, is split into fea-
tures, X, and labels, y. Any missing values in the
features are handled via a KNN-Imputer. Subse-
quently, the features, X, are standardized via a Quan-
tile Transformer to ensure a uniformly scaled distri-
bution. The dataset is then further divided into Train-
ing and Testing sets: X_train, X_test, y_train,
y_test. The oversampler, O, is applied to the
Training data to generate: X_train_oversampled
and Y_train_oversampled. After oversampling, the
classifier, C, is trained on the oversampled Training
data. Finally, the trained model, M, is returned.
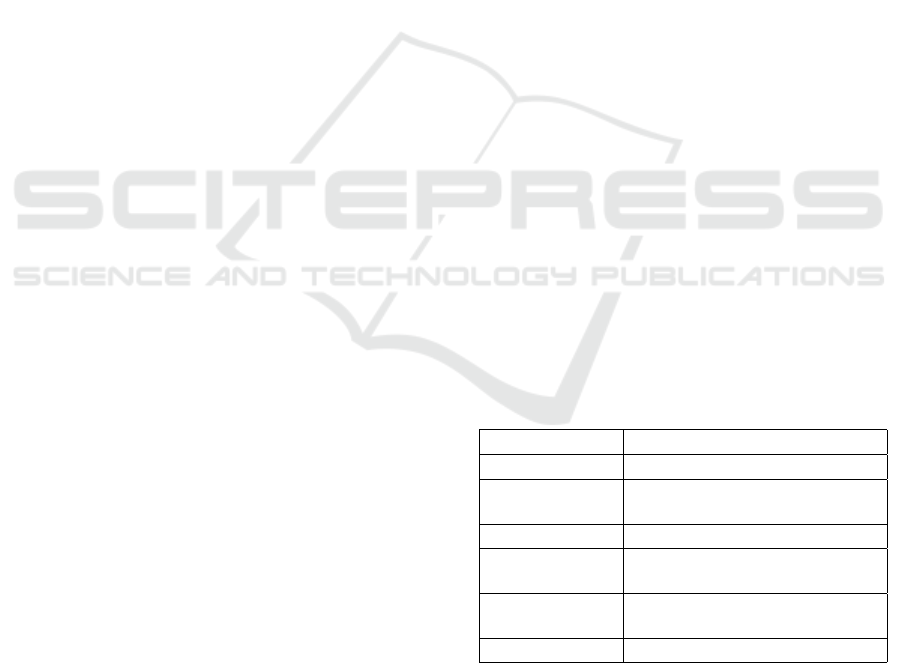
4 PROPOSED SYSTEM
ARCHITECTURE AND SETUP
The framework of our proposed system is illustrated
via Figure 1; while Table 1 represents the descrip-
tion of our benchmark dataset. Table 2 showcases
a handful of the hyperparameter configurations for
our experimental setup. Table 3 highlights the ob-
jective functions (or performance metrics) employed
herein to evaluate how well each benchmark model
performed - especially in terms of identifying diabetic
patients (the minority class). Table 4 lists the baseline
models we have employed toward benchmarking and
comparative analyses.
Table 1: Description of Dataset.
Property Description
Name Pima-Indian Diabetes Dataset
Source
UCI Machine Learning Repository
/ Kaggle
Instances 768
Features
8 input features + 1 binary output
(Outcome)
Target Variable
Outcome (1 = diabetic, 0 = non-
diabetic)
Missing Values Handled using KNN-Imputer
5 EXPERIMENT AND RESULTS
We used the Pima-Indian diabetes dataset, a widely
recognized dataset in medical and healthcare re-
Predictive Modelling for Diabetes Mellitus with Respect to Basic Medical History
345
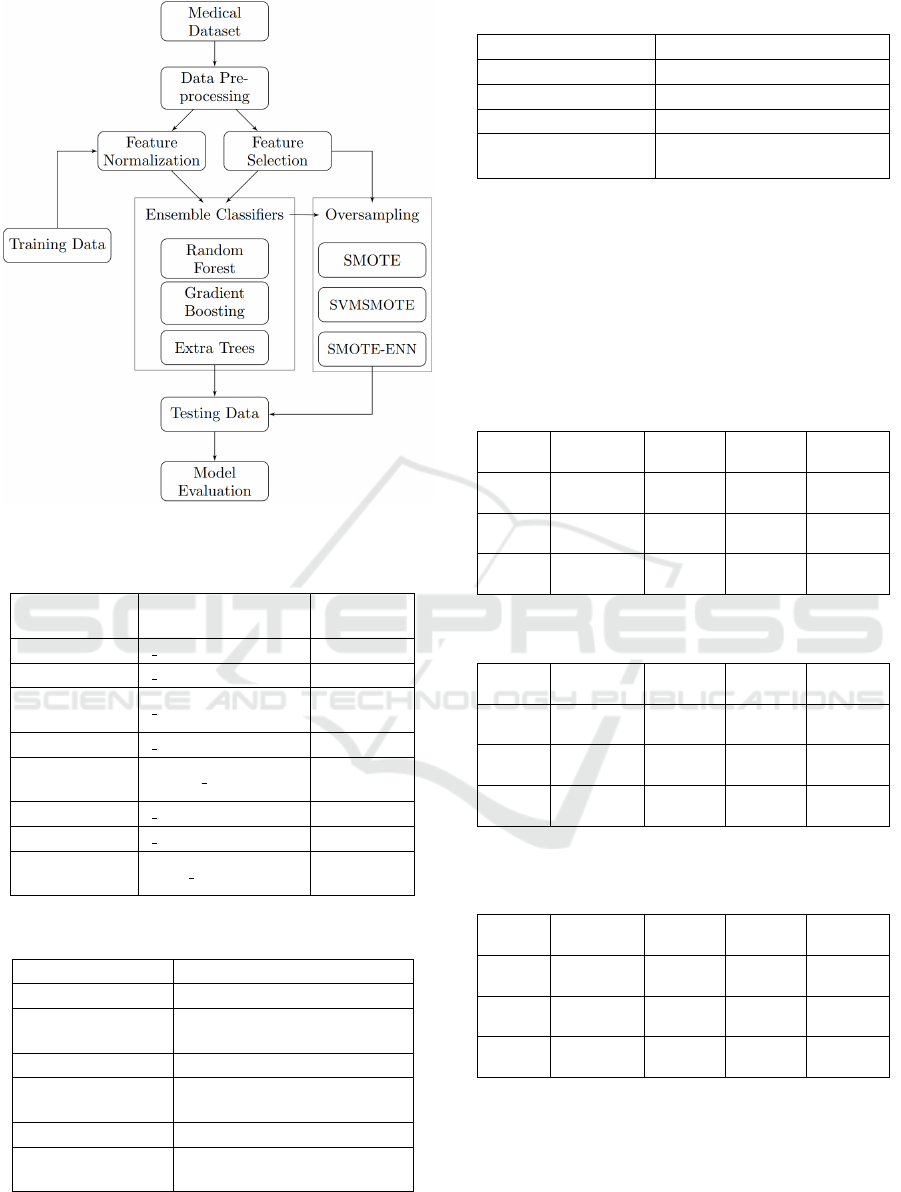
Figure 1: Architectural overview of our proposed system.
Table 2: Hyperparameters Configuration/Setting.
Component Parameter
Value(s)
Tested
SMOTE k neighbors 5
SVMSMOTE k neighbors 5
Random For-
est
n estimators 100
Extra Trees n estimators 100
Gradient Boost-
ing
learning rate 0.1
n estimators 100
KNNImputer n neighbors 5
Quantile Trans-
former
output distribution ‘normal’
Table 3: Objective Functions (Performance Metrics).
Metric Purpose
Accuracy Measures overall correctness
Precision
Ratio of True Positives to pre-
dicted Positives
Recall Sensitivity to positive cases
F1-score
Harmonic mean of Precision and
Recall
ROC-AUC Area under ROC curve
MCC
Balanced measure for imbal-
anced datasets
search, to thoroughly test the effectiveness of three (3)
robust ML algorithms: Random Forest, Extra Trees,
Table 4: Baseline Models for Comparison.
Model Description
Logistic Regression Simple linear classifier
Naive Bayes Probabilistic classifier
Decision Tree Base model for tree ensembles
Dummy Classifier
Majority class predictor (base-
line)
and Gradient Boosting. Each of these algorithms was
carefully selected based on their known strengths in
handling classification tasks, especially with medical
datasets. To ensure our models effectively manage
data imbalance — a common issue in medical diag-
nosis — we employed multiple sampling techniques
(SMOTE, SVM-SMOTE, and SMOTE-ENN) as well
as “No Sampling” technique.
Table 5: Accuracy scores (Train/Test).
Model
No Sam-
pling
SMOTE
SVM-
SMOTE
SMOTE-
ENN
Random
Forest
0.759/
0.721
0.819/
0.766
0.814/
0.753
0.961/
0.721
Extra
Trees
0.756/
0.714
0.823/
0.734
0.833/
0.734
0.960/
0.727
Grad-
Boost
0.754/
0.760
0.785/
0.740
0.788/
0.760
0.941/
0.766
Table 6: F1-scores (Train/Test).
Model
No Sam-
pling
SMOTE
SVM-
SMOTE
SMOTE-
ENN
Random
Forest
0.755/
0.716
0.820/
0.750
0.804/
0.726
0.961/
0.726
Extra
Trees
0.748/
0.710
0.822/
0.735
0.833/
0.736
0.960/
0.733
Grad-
Boost
0.752/
0.754
0.785/
0.745
0.787/
0.764
0.941/
0.771
Table 7: Matthews Correlation Coefficient, MCC, scores
(Train/Test).
Model
No Sam-
pling
SMOTE
SVM-
SMOTE
SMOTE-
ENN
Random
Forest
0.456/
0.420
0.631/
0.457
0.606/
0.490
0.893/
0.427
Extra
Trees
0.452/
0.420
0.639/
0.462
0.644/
0.401
0.926/
0.463
Grad-
Boost
0.467/
0.455
0.571/
0.390
0.583/
0.468
0.886/
0.508
6 DISCUSSION
Table 8 showcases the experiment results with re-
spect to our Extra-Trees model, and Table 9 represents
the experiment results with respect to our Gradient-
WEBIST 2025 - 21st International Conference on Web Information Systems and Technologies
346
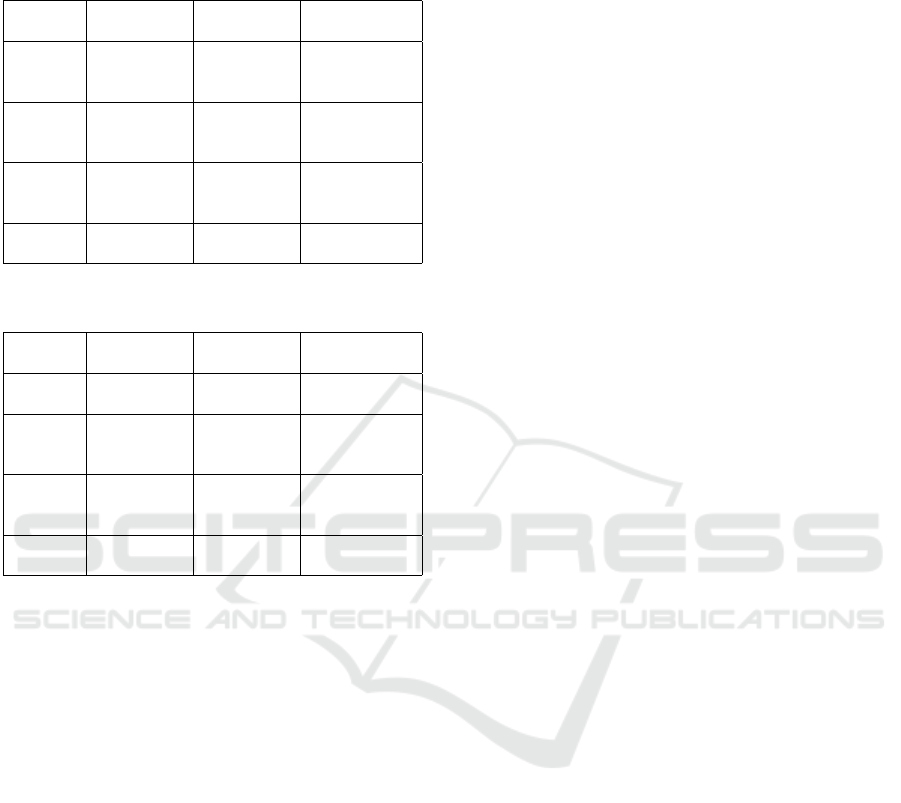
Boosting model.
Table 8: Extra-Trees model (Train/Test).
Sampling
Method
Accuracy
(Train/Test)
F1-score
(Train/Test)
Interpretation
No Sam-
pling
0.756/ 0.714 0.748/ 0.710
Minor over-
fitting, ∼5%
variance
SMOTE 0.823/ 0.734 0.822/ 0.735
Better scores
but overfitting
by 7-10%
SVM-
SMOTE
0.833/ 0.734 0.833/ 0.736
Better scores
but overfitting
by 7-10%
SMOTE-
ENN
0.960/ 0.727 0.960/ 0.733
Major overfit-
ting, up to 25%
Table 9: Gradient-Boosting model (Train/Test).
Sampling
Method
Accuracy
(Train/Test)
F1-score
(Train/Test)
Interpretation
No Sam-
pling
0.754/ 0.760 0.752/ 0.754
No overfitting,
∼1% variance
SMOTE 0.785/ 0.740 0.785/ 0.745
Minor over-
fitting, 1-5%
variance
SVM-
SMOTE
0.788/ 0.760 0.787/ 0.764
Minor over-
fitting, 1-5%
variance
SMOTE-
ENN
0.941/ 0.766 0.941/ 0.771
Major overfit-
ting, up to 20%
6.1 Performance Analysis
The experimental results reveal that the performance
of the ensemble classifiers — Random Forest, Ex-
tra Trees, and Gradient Boosting — varied signifi-
cantly depending on the oversampling technique ap-
plied. Random Forest consistently achieved the high-
est training scores across all oversampling methods,
with training Accuracy reaching as high as 0.961 and
training F1-score also at 0.961 when using SMOTE-
ENN. However, these impressive training metrics did
not carry over to the Test set, where the corresponding
Accuracy and F1-score dropped to 0.721 and 0.726,
respectively. This large disparity suggests significant
overfitting, where the model learns the Training data
too closely and fails to generalize well to new, un-
seen data. A similar pattern was observed in the
Extra-Trees classifier, where training Accuracy and
F1-score under SMOTE-ENN were both 0.960, but
Test set values fell to 0.727 and 0.733, respectively.
This reinforces the conclusion that aggressive over-
sampling techniques like SMOTE-ENN can lead to
overly optimistic training performance while compro-
mising real-world applicability.
In contrast, Gradient Boosting demonstrated a
more balanced performance between the training and
testing phases. The differences between the train-
ing and test metrics were much narrower, espe-
cially with SMOTE and SVM-SMOTE. For example,
when paired with SVM-SMOTE, Gradient Boosting
achieved a training Accuracy of 0.788 and a test Ac-
curacy of 0.760, with F1-scores of 0.787 and 0.764,
respectively. This indicates only a minor degree of
overfitting, suggesting that Gradient Boosting may be
better at generalizing from the Training data while
still benefiting from oversampling. These findings
are further supported by the Matthews Correlation
Coefficient (MCC) score, which reflects the quality
of binary classifications in imbalanced datasets. Al-
though, Random Forest and Extra-Trees yielded very
high MCC values on the Training data (up to 0.926);
their test MCC scores were notably lower. In con-
trast, Gradient Boosting with SMOTE-ENN achieved
the highest test MCC at 0.508, indicating a stronger
ability to maintain balanced performance across both
classes.
6.2 Interpretation of Results
The primary performance indicators used to evaluate
the models were Accuracy, F1-score, and Matthews
Correlation Coefficient (MCC); which together pro-
vide a multidimensional view of the classification
quality. Accuracy captures the overall correctness of
the model, while F1-score accounts for the trade-off
between Precision and Recall, making it particularly
useful in imbalanced medical datasets. MCC offers
a single summary metric that reflects the balance of
both True and False Positives as well as negatives
- making it especially relevant when the dataset is
skewed.
While training Accuracy for all models frequently
exceeded 90%, such high values were not replicated
on the Test set where most accuracy values hovered
between 71% and 76%. This discrepancy underscores
the presence of overfitting, particularly in models like
Random Forest and Extra Trees when trained with
SMOTE-ENN. F1-scores on the Test set ranged be-
tween 0.71 and 0.77, with Gradient Boosting paired
with SMOTE-ENN yielding the highest test F1-score
of 0.771. This suggests that the combination allowed
for the most effective balance between detecting true
diabetic cases and avoiding False Positives. Mean-
while, the MCC results offered a more nuanced in-
terpretation of model balance. Gradient Boosting
with SMOTE-ENN once again led with a test MCC
of 0.508, indicating strong classification consistency.
Random Forest with SVM-SMOTE also performed
Predictive Modelling for Diabetes Mellitus with Respect to Basic Medical History
347

welll with a test MCC of 0.490.
These results suggest that while oversampling
methods can enhance model performance by mitigat-
ing class imbalance, they must be applied with cau-
tion to avoid overfitting. Among the classifiers tested,
Gradient Boosting demonstrated the most robust and
reliable generalization, especially when combined
with SMOTE-ENN or SVM-SMOTE. These combi-
nations improved the model’s ability to identify dia-
betic cases effectively without significantly compro-
mising performance on the majority class, which is
essential in high-stake medical prediction tasks.
6.3 Implications, Benefits, and
Contribution to Humanity
The results from this work and project have several
important real-world implications, viz:
(a) Early and accurate detection of diabetes: Our
models can help identify positive diabetes cases
earlier, thereby enabling timely interventions that
can prevent serious complications, improve pa-
tient outcomes, and significantly reduce health-
care costs.
(b) Deployment in real-world scenarios: Credits to
the robust performance after advanced prepro-
cessing (especially SVM-SMOTE and SMOTE-
ENN). This enabled the models to be confidently
deployed in critical fields such as healthcare or
finance, where imbalanced data is common and
high-stake decisions are made.
(c) Broader applicability: The techniques and work-
flow we demonstrated herein, combining strong
ensemble models with smart preprocessing tech-
niques, can be applied to other imbalanced prob-
lems like cancer detection, fraud detection, or pre-
dicting rare diseases.
7 CONCLUSIONS AND FUTURE
7.1 Limitations
Despite the promising outcomes herein, our research
has several limitations. Primarily, our evaluation was
limited to the Pima-Indian dataset which predom-
inantly includes data from women of (Indigenous)
Pima-Indian heritage; thus potentially restricting the
model’s applicability to broader populations and gen-
ders. Additionally, advanced Deep Learning archi-
tectures and a wider range of preprocessing methods
were not explored.
7.2 Summary of Model
Our developed models are effective analytical tools
capable of ingesting and processing medical and clin-
ical data. The model is capable of taking tabular nu-
meric data as input, where each row is an instance of a
patient’s medical profile and each column represents
features such as pregnancy count, glucose levels, in-
sulin levels, etc. In the initial phase of data trans-
formation, missing and/or invalid values were identi-
fied in the dataset with respect to features like Glu-
cose level, BloodPressure, SkinThickness, Insulin,
and BMI. These features contained invalid zero en-
tries, which were later transformed into NaN-values,
and imputed using KNN-Imputer to maintain data in-
tegrity.
Preprocessing stage consists of several steps to
prepare the data for modeling. Firstly, we tack-
led missing values by filling them up, then we used
EDA (Exploratory Data Analysis): using histograms
to show that the distribution of features has been cor-
rected, and confirming there are no more zero-entries.
Feature selection is done with the help of SelectKBest
and ANOVA F-test (f classif), so that we can choose
the most relevant features which correlate with the tar-
get for our model. The dataset is then cross-validated
with train test split.
Data oversampling is performed using SMOTE,
SVMSMOTE, or SMOTE-ENN, depending on which
sampling method the user chooses to include in the
model. The Testing data should not have any knowl-
edge of the Training data. Our oversampling methods
create synthetic data points via interpolation between
two (2) original data points with respect to a given
dataset. If the Test set includes these synthetic data
points, then it has some knowledge of the Training
data, and this may cause bias in the resultant model’s
learning (Zhang et al., 2024). Therefore, oversam-
pling is performed only on the Training data. Sub-
sequently, the features are standardized using Quan-
tileTransformer with a normal-distribution output to
reduce skewness and ensure that the model sees uni-
formly distributed input features.
Upon completion of preprocessing, model train-
ing is done robustly with the help of k-fold cross
validation so that the performance of the model can
be evaluated effectively. To properly evaluate the
model’s generalization capability, key performance
metrics such as Accuracy and F1-score are calculated
for both Training data and Testing data which we
have explained in detail in the previous section. The
model yields its results with respect to standard ob-
jective functions/metrics for classification tasks. The
primary output is whether a patient is diabetic or not
WEBIST 2025 - 21st International Conference on Web Information Systems and Technologies
348

diabetic. This research is not just limited to only med-
ical data, it can be adapted to any type of numeric data
requiring a classification task.
7.3 Future Work
Future research efforts will substantially broaden the
scope of our investigation. We plan to incorporate
more diverse and extensive datasets, encompassing
varied populations to enhance the generalizability and
robustness of the predictive models herein. Addition-
ally, further exploration into advanced Deep Learn-
ing methods such as Convolutional Neural Networks
(CNNs), Recurrent Neural Networks (RNNs), and hy-
brid Deep Learning models is anticipated. These so-
phisticated architectures could uncover deeper pat-
terns within complex medical data, potentially of-
fering substantial improvements in predictive perfor-
mance. Moreover, detailed preprocessing techniques
including advanced feature engineering, dimensional-
ity reduction techniques such as Principal Component
Analysis (PCA) and t-distributed Stochastic Neighbor
Embedding (t-SNE), will be rigorously examined to
optimize the feature set for enhanced predictive Ac-
curacy scores.
Addressing the interpretability of these models
will also be an essential aspect of our future work,
aiming to produce models that are not only accurate
but also easily interpretable by healthcare profession-
als. In addition to technical advancements, we intend
to deploy our model on accessible and user-friendly
platforms, such as interactive web applications or mo-
bile apps. This approach aims to facilitate real-time
diabetes risk assessment tools for healthcare profes-
sionals and patients alike, promoting proactive health
management.
Collaborations with clinical institutions and
healthcare providers will also be pursued to validate
our model further through extensive real-world clini-
cal trials and implementations, ensuring practical rel-
evance and efficiency in varied clinical domains.
ACKNOWLEDGMENT
The authors would like to thank the Department
of Computer Science at California State University,
Sacramento, for providing the necessary resources
and guidance throughout the course of this project.
We also extend our gratitude to the faculty members
and mentors who offered valuable insights and sup-
port during the research and experimentation phases.
Special thanks to the creators and managers of the
Pima-Indian Diabetes Dataset for making the dataset
publicly available, which served as a critical foun-
dation for our study. Finally, we would like to ac-
knowledge the contributions of all team members
whose dedication, collaboration, and shared problem-
solving efforts were instrumental in the successful
completion of this project.
REFERENCES
Chawla, N. V., Bowyer, K. W., Hall, L. O., and Kegelmeyer,
W. P. (2002). Smote: Synthetic minority over-
sampling technique. Journal of Artificial Intelligence
Research, 16:321–357.
Demidova, L. and Klyueva, I. (2017). Svm classification:
Optimization with the smote algorithm for the class
imbalance problem. In 2017 6th Mediterranean Con-
ference on Embedded Computing (MECO), pages 1–4.
Kaliappan, J., Kumar, I. J. S., Sundaravelan, S., Anesh,
T., Rithik, R. R., Singh, Y., Vera-Garcia, D. V.,
Himeur, Y., Mansoor, W., Atalla, S., and Srinivasan,
K. (2024). Analyzing classification and feature selec-
tion strategies for diabetes prediction across diverse
diabetes datasets. Frontiers in Artificial Intelligence,
7:1421751.
Lugat, V. (2021). Pima indians diabetes - eda and prediction
(0.906). https://www.kaggle.com/code/vincentlugat/
pima-indians-diabetes-eda-prediction-0-906. Ac-
cessed: 2025-05-18.
Mooney, P. T. (2018). Predict diabetes
from medical records. https://www.
kaggle.com/code/paultimothymooney/
predict-diabetes-from-medical-records. Accessed:
2025-05-18.
Nnamoko, N. and Korkontzelos, I. (2020). Efficient
treatment of outliers and class imbalance for dia-
betes prediction. Artificial intelligence in medicine,
104:101815.
Olisah, C. C., Smith, L. N., and Smith, M. L. (2022).
Diabetes mellitus prediction and diagnosis from a
data preprocessing and machine learning perspec-
tive. Computer methods and programs in biomedicine,
220:106773.
Poornima, V. and R., R. (2024). A hybrid model for predic-
tion of diabetes using machine learning classification
algorithms and random projection. Wirel. Pers. Com-
mun., 139:1437–1449.
Santos, M. S., Soares, J. P., Abreu, P. H., Ara
´
ujo, H., and
Santos, J. A. M. (2018). Cross-validation for imbal-
anced datasets: Avoiding overoptimistic and overfit-
ting approaches [research frontier]. IEEE Computa-
tional Intelligence Magazine, 13:59–76.
Zhang, Z., Ahmed, K. A., Hasan, M. R., Gedeon, T., and
Hossain, M. Z. (2024). A deep learning approach to
diabetes diagnosis. In Asian Conference on Intelli-
gent Information and Database Systems, pages 87–99.
Springer.
Predictive Modelling for Diabetes Mellitus with Respect to Basic Medical History
349
