
Machine Learning Solutions for Heart Disease Diagnosis: Model
Choices and Factor Analysis
Hao Rui
a
Zhejiang University - University of Illinois Urbana-Champaign Institute, Zhejiang University, Jiaxing, Zhejiang, China
Keywords: Machine Learning, Model Training, Heart Disease Diagnosis.
Abstract: The prediction of heart disease diagnosis is of paramount importance since it is one of the leading causes of
death nowadays. Yet accurately identifying and monitoring the factors relative to heart diseases pose
significant challenges. Traditional visual survey methods are time-consuming, often hampered by the lack of
data exchange among hospitals and individual doctors, and may not provide real-time data crucial for effective
prevention strategies. Machine learning (ML) technologies have become increasingly potent instruments in
the diagnosis of diseases in recent years. In this project, several models were investigated. A complete set of
data gathered from Long Beach V, Cleveland, Hungary, and Switzerland was utilized. This data set, which
encompasses over 13 different factors that are relative to heart diseases, is meticulously preprocessed to ensure
data quality. The outcomes not only show how well machine learning techniques can anticipate heart
conditions, but they also open the door for the creation of edge computing and mobile applications. These
might be installed in far-off places, giving physicians and hospitals access to real-time data and enabling
timely treatment decisions. Thus, this study marks a substantial advancement in the use of cutting-edge
technologies for the identification of heart disease in real time.
1 INTRODUCTION
An estimated 17.9 million people die from heart
disease each year, making it one of the major causes
of mortality worldwide. Premature deaths can be
avoided by determining who is most at risk for heart
disease and making sure they get the right care
(World Health Organization, 2021). In less developed
countries the increasing population and the rising
number of heart disease patients are posing greater
challenges. Here, the effectiveness of screening
methods for patients exhibiting heart disease signs is
still up for debate because of the financial crisis and
restricted access to appropriate and equitable
healthcare facilities and equipment. Given this, many
academics and practitioners have found machine
learning-based heart disease detection (MLBHDD)
systems to be affordable and adaptable methods since
the introduction of machine learning (ML)
applications in the medical field (Ahsan & Siddique,
2022).
There are numerous risks to applying ML and
ML-based solutions since the behavior of the machine
a
https://orcid.org/0009-0000-4880-5519
during the process of feature drawing and final
prediction is still not clear, thus the credibility of its
outputs is still in doubt (Ahsan et al., 2021).
Imbalanced performance of ML also occurs when the
data is not equally collected, especially in some less
developed countries whose majority class has no
access to physical examination and medical
treatments. It is important to find a reliable data set
and use proper methods to ensure the credit of the
final diagnosis.
This research applied Random Forest, Naive
Bayes, Gradient Boosting, K- Nearest Neighbour
Classification (KNN), Logistic Regression and
Support Vector Machine (SVM). By comparing
different models and analyzing the final outcomes,
this research is dedicated to finding a suitable model
for heart disease diagnosis and looking for important
factors among the 14 attributes.
60
Rui, H.
Machine Learning Solutions for Heart Disease Diagnosis: Model Choices and Factor Analysis.
DOI: 10.5220/0013678100004670
Paper published under CC license (CC BY-NC-ND 4.0)
In Proceedings of the 2nd International Conference on Data Science and Engineering (ICDSE 2025), pages 60-66
ISBN: 978-989-758-765-8
Proceedings Copyright © 2025 by SCITEPRESS – Science and Technology Publications, Lda.

2 UNDERSTANDING THE DATA
SET
As mentioned earlier, the publicly available and well-
liked UCI heart disease data set is used in this study.
There are 76 attributes in all in the UCI heart disease
data collection.
However, the vast majority of previous research
has only used a maximum of 14 attributes. The UCI
heart disease data has been used to create a number of
datasets. The Cleveland data collection, which has 14
variables, has been primarily utilized by
computational intelligence researchers. The majority
of the data is in binary form, and computers can easily
identify features using this boolean expression. Five
class attributes in the data set indicate whether the
data set is healthy or one of four sick categories. Five
class attributes that correspond to either a healthy
state or one of the four sick types make up the data
set. Five class attributes, which stand for either a
healthy state or one of the four sick categories, make
up the data set. Each component is examined
separately in this study to ascertain its unique impact.
With 0 denoting no disease and 1 denoting disease,
the classifier used in the studies is essentially binary.
Five datasets were produced as a result. The
following symbols are used to refer to the generated
datasets: Sick1, Sick2, Sick3, and Sick4,
correspondingly, with H-0 standing for healthy.
Table 1 shows some important example attributes in
this study.
Table 1: Explanation of Partial Attributes
Name
Description
Age
age (numeric)
Sex
male, female (nominal)
Chest pain type
(CP)
4 chest pain types
Trestbps
resting blood pressure, mm/Hg
Chol
Serum cholesterol, mg/dekadaliter
Fbs
Whether the blood sugar levels after fasting exceed 120 mg/dl: (0 = False; 1 = True)
Restecg
Three different kinds of values. Normal (norm), aberrant (abn): exhibiting ventricular hypertrophy
(hyp) or abnormal ST-T waves.
Thalach
highest heart rate reached
Exang
whether angina brought on by exercise has occurred: 0 indicates no, whereas 1 indicates yes.
Oldpeak
Exercise-induced ST depression compared to rest
Slope
the ST segment's slope at maximal exertion. Three different value types: downsloping, flat, and
upsloping
Ca
number of main fluoroscopy-colored vessels (0–3)
Thal
heart issue (reversible, fixed, or normal)
The class
attributes
either cardiac illness or healthy.
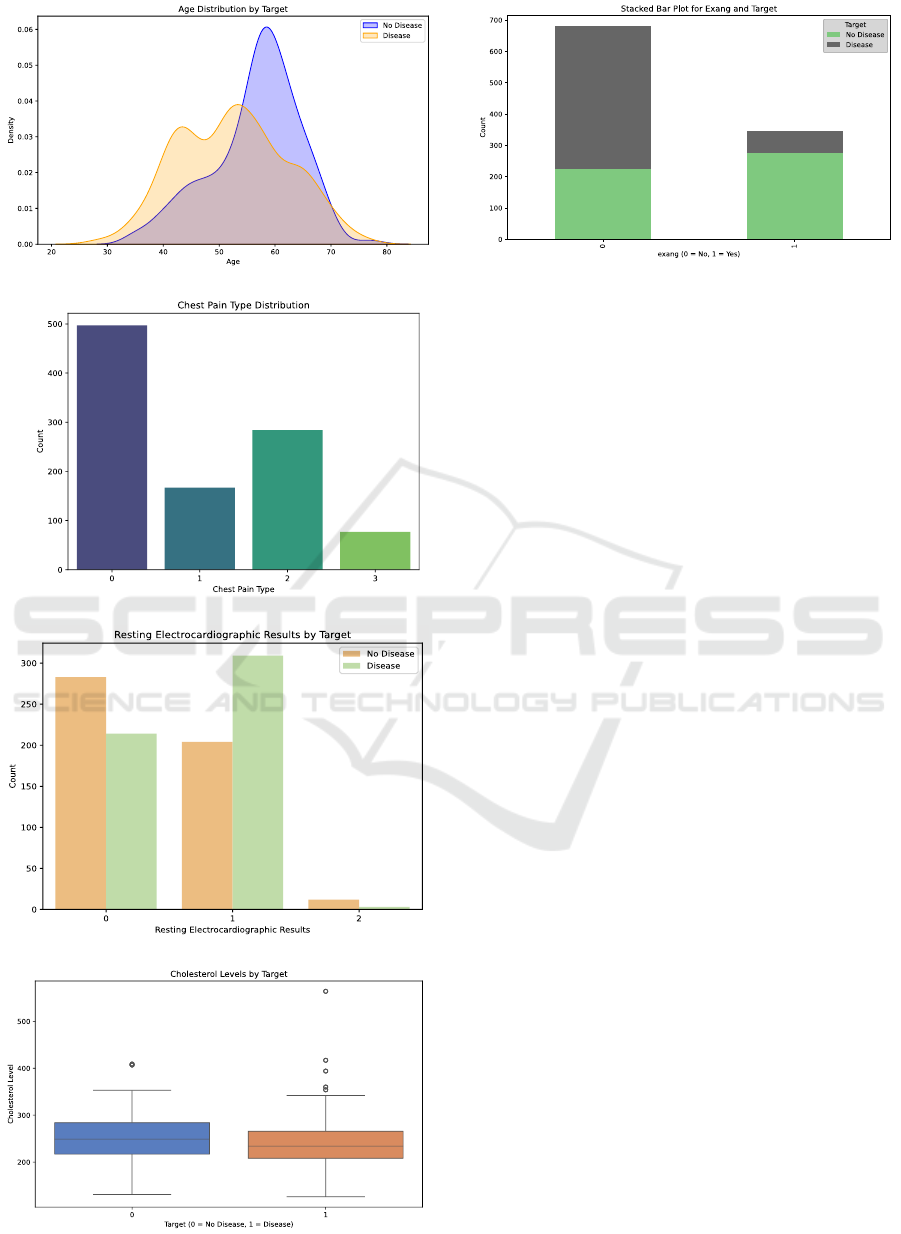
Figure 1(a) displays a distribution for age and
heart disease frequencies. The frequencies of the age
groups 50 - 60 years old and 60 - 70 years old are
relatively high, showing a pattern similar to a normal
distribution.
There are four forms of chest pain. From a
medical perspective, (i) is defined as substernal
discomfort brought on by emotional or physical stress
(Jones et al., 2020). A patient with typical angina has
a high risk of coronary artery blockages since their
past medical history exhibits the typical symptoms. (ii)
Chest pain that doesn't match the definition of typical
or classic chest pain is referred to as atypical
(Cleveland Clinic, 2023). (iii) The stabbing or knife-
like, protracted, dull, or uncomfortable condition that
can persist for brief or extended periods of time is
known as non-angina pain (Constant, 1990). ( ⅳ )
Asymptomatic pain does not manifest any signs of
illness or disease and may not be the source of or a
sign of a disease. The distribution of chest pain types
is as follows in Figure 1(b).
The rest distribution is as Figure 1(c) with three
resting electrocardiographic results 0, 1 and 2,
representing 3 different ranges. Cholesterol level can
be classified into two categories according to a target
value and can be inferred in Figure 1(d), while Exang
can be inferred in Figure 1(e).
Machine Learning Solutions for Heart Disease Diagnosis: Model Choices and Factor Analysis
61
(a)
(b)
(c)
(d)
(e)
Figure 1: Analysis of the important attributes. (a) is the Age
distribution by target, (b) is the Chest Pain type distribution,
(c) is the Resting Electrocardiographic results by target, (d)
is the Cholesterol Levels by target, (e) is the stacked bar
plot for Exang and Target. (Photo/Picture credit: Original).
3 MACHINE LEARNING IN
HEALTHCARE
Machine learning is a growing topic in recent
healthcare, which analyzes vast volumes of medical
data using algorithms. In the medical field, machine
learning algorithms are essential. Their pattern-
recognition capabilities in large datasets are well-
suited for genomics and proteomics applications.
They aid significantly in illness diagnosis and
detection, enabling better treatment decisions. As
medical data grows, the role of machine learning will
expand, promising more personalized and efficient
healthcare (Shailaja et al., 2018).
3.1 Explanation of Algorithms Used for
Diagnosis
Random forest, K-Nearest Neighbors (KNN),
Logistic Regression, Naive Bayes, Gradient Boosting
and Support Vector Machine (SVM) are evaluated for
heart disease diagnosis. Random forest is one
ensemble learning approach that exemplifies an
information mining methodology. It employs
multiple classifiers that work in tandem to identify the
class label for a new, unlabeled instance within a data
set (Parmar et al., 2019). A majority vote among the
individual decision trees determines the final forecast
for classification. Every tree makes a class prediction,
and the random forest predicts the class with the most
votes. Compared to a single decision tree, random
forests have the advantage of being able to handle
high-dimensional data well, being reasonably
ICDSE 2025 - The International Conference on Data Science and Engineering
62

resistant to overfitting, and being able to identify
intricate non-linear correlations in the data.
KNN is a learning algorithm that is instance-based.
When a new sample is provided, the KNN algorithm
locates the K samples in the training dataset that are
the most comparable (closest in distance) and then
uses the classes of these K neighbors to forecast the
new sample's class. Manhattan distance, Euclidean
distance, and other methods are typically used to
measure the distances between samples. It is
extensively utilized in domains including
recommendation systems, text categorization, and
image recognition. It is quite flexible with regard to
data distribution and does not require a training
procedure. One of its drawbacks is its high
computational complexity, which rises sharply with
data volume. Additionally, it is susceptible to local
noise in the data, and the model's performance may
be impacted by the K value selection.
Logistic regression is a linear model for
classification issues. It represents the likelihood that
a sample belongs to a particular class by mapping the
outcomes of linear regression to probability values
between 0 and 1. The likelihood function is
maximized in the model to estimate parameters, and
gradient descent is a popular solution technique. The
model can effectively handle linearly separable data
and is straightforward, interpretable, and
computationally efficient. Its restrictions on data
distribution, which typically call for feature
independence, are its drawbacks. Its capacity to fit
complex non-linear data is restricted, and it can only
handle linear relationships.
The Bayes theorem and the feature conditional
independence assumption form the foundation of the
Naive Bayes classification technique. It computes the
posterior probability of each class given the features
and makes the assumption that each feature is
independent given the class. The prediction outcome
is chosen from the class with the highest posterior
probability. This model is insensitive to missing
values, works well on small-scale data, and trains
quickly. The drawback is that the feature conditional
independence assumption is highly sensitive to the
input data's representation form and is frequently
challenging to meet in practice, which could
compromise the model's accuracy.
Based on the concept of ensemble learning,
gradient boosting trains a number of weak learners
iteratively before combining them to create a strong
learner. The approach gradually improves the
performance of the model by modifying the training
of the subsequent weak learner based on the gradient
of the current model's loss function in each iteration.
Numerous data kinds, including categorical and
numerical data, can be handled by it. It performs well
in generalization and has a strong fit for intricate non-
linear relationships. However, it is time-consuming to
train, prone to overfitting, and very sensitive to
hyperparameter selection, necessitating adjustment.
SVM maximizes the margin between the two
classes of samples by identifying the best hyperplane
to divide them. A kernel function is used to translate
the data to a high-dimensional space in order to make
it linearly separable in the high-dimensional space
while dealing with non-linear situations. SVM
performs well in handling both linear and non-linear
issues, has strong generalization ability, and
successfully prevents overfitting when working with
small sample data. The drawbacks include a lengthy
training period and considerable computational
complexity, particularly when working with huge
amounts of data. It also necessitates specific tuning
abilities and is highly sensitive to the kernel functions
and parameter choices.
4 MODEL TRAINING AND
COMPARISON
The six algorithms are properly applied in the process
of training and show different performances. To
evaluate the functionality of each algorithm, accuracy
and F1-score are calculated in Equation (1), and
Equation (2), using True Positive (TP), True Negative
(TN), False Positive (FP), False Negative (FN), with
P refers to precision and R refers to recall.
𝐴𝑐𝑐𝑢𝑟𝑎𝑐𝑦 =
TP + TN
TP + TN + FP + FN
(
1
)
𝐹1 =
2PR
P + R
(
2
)
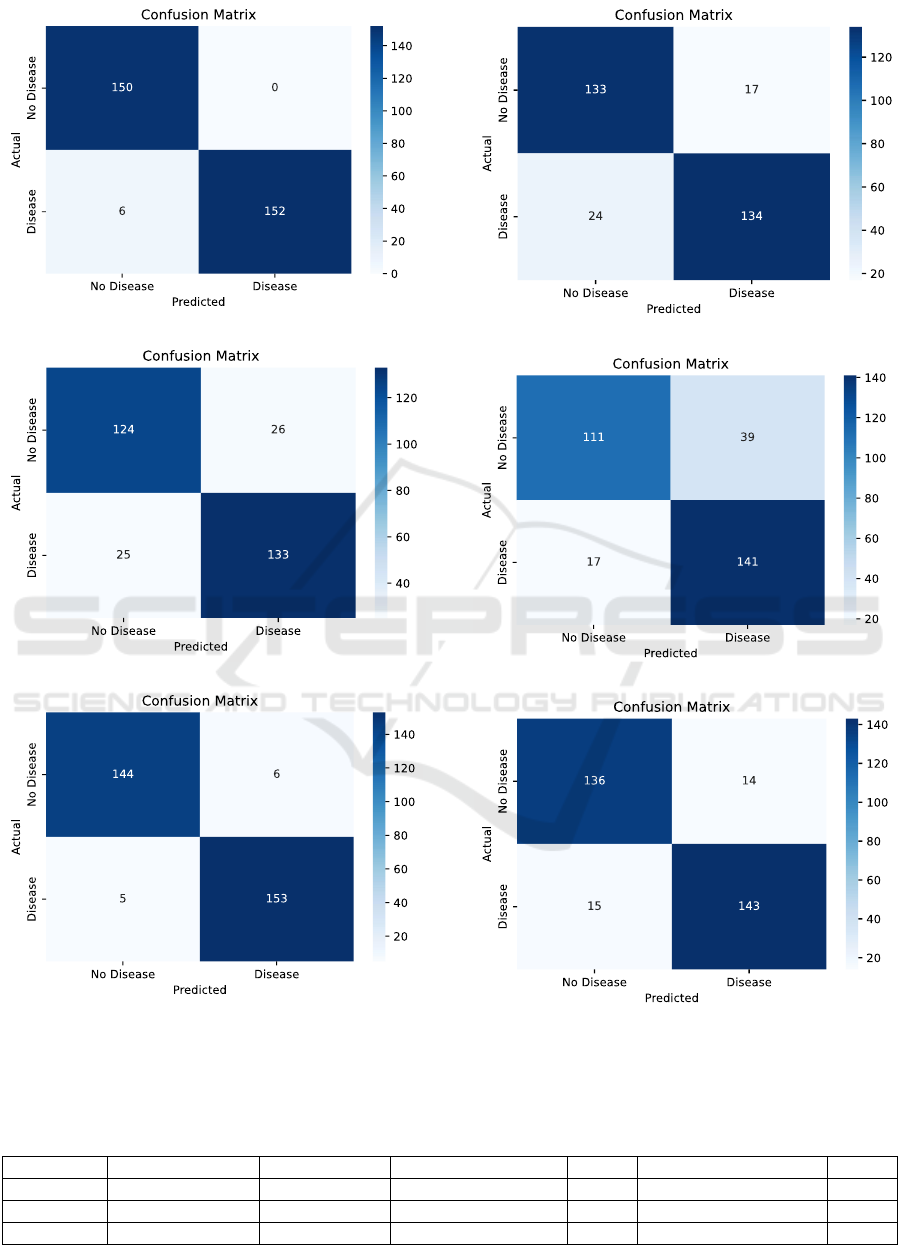
A key tool for assessing the effectiveness of
diagnostic tests, particularly in binary classification
settings, is the ROC curve (Srinivasan & Mishra,
2024), which is also used to compare various models.
A greater area under the curve typically indicates
higher performance. Figure 2 shows the inferred
confusion matrix reports, each of which represents an
algorithm. Table 2 lists the F1 Scores and Accuracy.
Figure 3 shows the ROC curve.
Machine Learning Solutions for Heart Disease Diagnosis: Model Choices and Factor Analysis
63
(a)
(b)
(c)
(d)
(e)
(f)
Figure 2: Confusion matrix for each model. (a) is the Random Forest confusion matrix, (b) is the Naive Bayes confusion
matrix, (c) is the Gradient Boosting confusion matrix, (d) is the KNN confusion matrix, (e) is the Logistic Regression
confusion matrix, (f) is the SVM confusion matrix. (Photo/Picture credit: Original).
Table 2: F1 score and accuracy.
Random Forest
Naive Bayes
Gradient Boosting
KNN
Logistic Regression
SVM
F1 for 0
0.98
0.83
0.96
0.87
0.80
0.90
F1 for 1
0.98
0.84
0.97
0.87
0.83
0.91
Accuracy
0.98
0.83
0.96
0.87
0.82
0.91
ICDSE 2025 - The International Conference on Data Science and Engineering
64
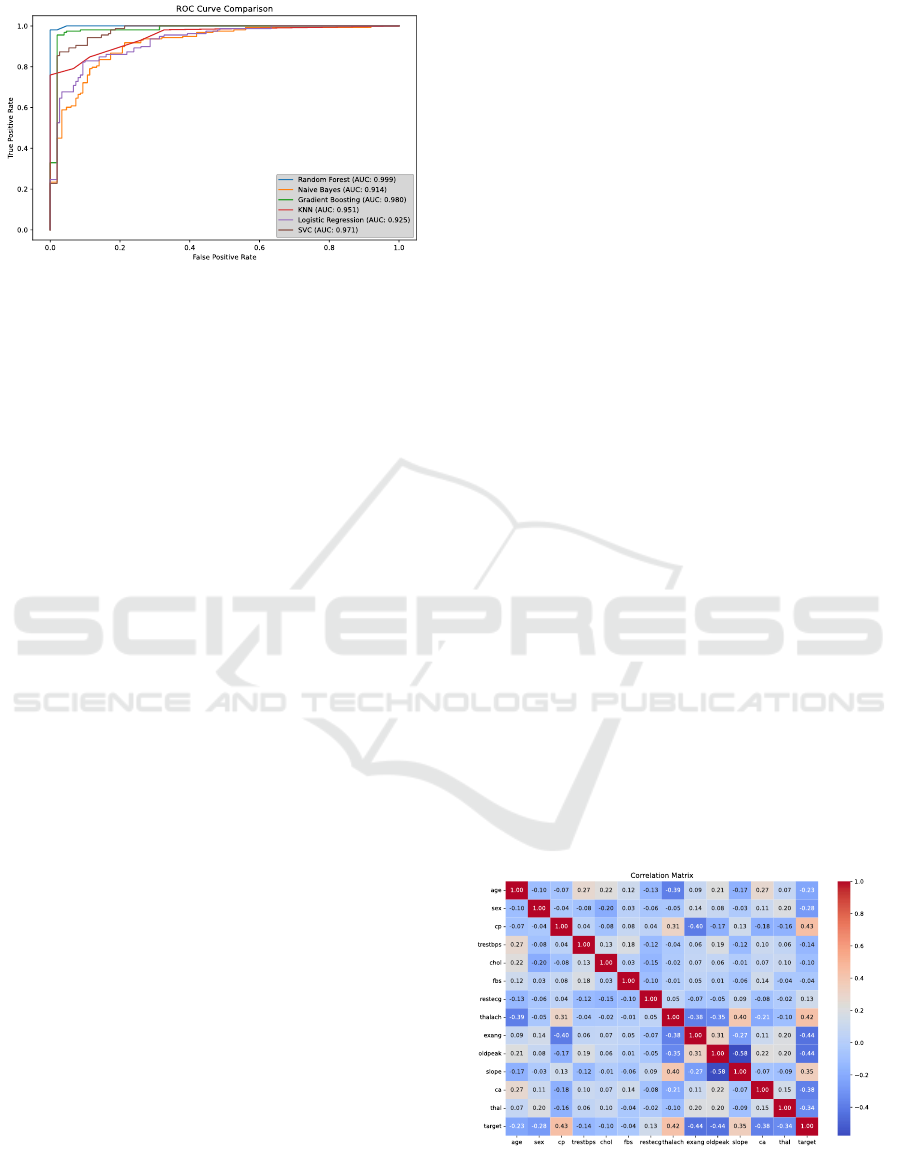
Figure 3: ROC curve for each model. (Photo/Picture credit:
Original).
Compared to other models, the Random Forest
classifier and Gradient Boosting performed better.
With the highest accuracy of 0.98, the Random Forest
classifier is closely followed by the Gradient
Boosting classifier, which has an accuracy of 0.96.
This suggests that in comparison to the other
classifiers, Random Forest and Gradient Boosting do
better overall at accurately classifying instances in
this data set. Random Forest has the highest precision
(0.96 & 1.00), whereas Gradient Boosting comes in
second (0.97 & 0.96). Gradient Boosting has a recall
of 0.96 and 0.97, both much higher than other models,
whereas Random Forest has a perfect recall of 1.00
for class 0 and 0.96 for class 1. With the greatest f1-
scores of 0.98 & 0.98 and 0.96 & 0.97, respectively,
Random Forest and Gradient Boosting demonstrate a
good trade-off between recall and precision. Figure 3
shows the ROC curves. Based on the Area Under
ROC Curve (AUC) values, the Random Forest model
performs the best, followed by Gradient Boosting and
SVM. In contrast, Naive Bayes, KNN, and Logistic
Regression are all above 0.900, indicating fairly high
functionalities, but they are all relatively weaker.
Random Forest or Gradient Boosting would be the
best options if overall high accuracy and strong
performance in both classes are the primary
objectives. These classifiers appear to be capable of
producing precise predictions and effectively
capturing the patterns in the data. Regarding feature
selection, Random Forest and Gradient Boosting
produced encouraging results when paired with the
computerized feature selection process (CFS) and the
medical knowledge-based motivated feature selection
process (MFS) (Nahar et al., 2013). This suggests that
it can improve its discriminatory power by efficiently
leveraging the improved feature sets.
Additionally, SVM does fairly well, with an
accuracy of 0.91. If Random Forest or Gradient
Boosting has too high of a computational cost, this
can be an acceptable substitute.
KNN performs mediocrely, with an accuracy of
0.87. It might work well with data sets when the local
similarity assumption is valid, but in this instance, the
best-performing classifiers exceed it.
The accuracy of Naive Bayes and Logistic
Regression is comparatively lower. The feature
independence assumed by Naive Bayes might not
hold true for this set of data. The intricacy of the
decision boundary in the data may be a limitation of
logistic regression. Despite its poorer performance,
logistic regression may still be taken into
consideration if interpretability and simplicity are
important since it can shed light on the link between
the target variable and the features.
5 RESULTS AND
INTERPRETATION
Using the six different methods of training, a
correlation matrix can be established in Figure 4. The
diagonal elements are all 1, indicating that each
variable is perfectly correlated with itself.
The correlation values are represented in the
matrix by a color gradient. A positive correlation is
shown in red and a negative correlation in blue.
Positive correlations imply that when one variable
rises, the other one tends to rise as well. When one
variable rises, the other one tends to fall, according to
negative correlations. For instance, there is a
somewhat negative association (-0.07) between age
and cp. Conversely, there is a moderately positive
connection (r = 0.22) between chol and trestbps.
Figure 4: Correlation Matrix. (Photo/Picture credit:
Original).
Machine Learning Solutions for Heart Disease Diagnosis: Model Choices and Factor Analysis
65

Table 3: significant correlations.
trestbps and chol
exang and oldpeak
age and exang
thalach and exang
0.22
0.40
-0.39
-0.38
Some significant correlations were included in
this correlation matrix and are shown in Table 3.
Trestbps is associated with higher chol and the same
as exang and oldpeak. Thalach and age are associated
with a lower likelihood of exang.
The feature cp has the highest importance value,
close to 0.25, while features like ca and thal also have
relatively high importance values, around 0.15. On
the other hand, features such as fbs, restecg, sex, and
exang have rather low importance values, with fbs,
nearly 0. Features with very low importance values
like fbs might be considered for removal if the goal is
to streamline the model.
6 CONCLUSIONS
Early diagnosis of heart disease plays a crucial role in
saving lives. Recognizing the significance of data
mining in facilitating heart disease diagnosis is of
utmost importance. This paper has elaborated on the
comparison of various classifiers for detecting heart
disease. It was noted that the Random Forest and
Gradient Boosting have emerged as a potentially
effective classification algorithm in this domain,
especially when total accuracy is regarded as the
performance metric. The results can also help in
feature selection, where less important features can be
removed to simplify the model without significantly
sacrificing accuracy. It also allows medical
practitioners to focus on the crucial aspects during
patient evaluations, potentially leading to earlier and
more accurate diagnoses.
There is an urgent need for further researches and
applications in this field to harness its full benefits
and continuously enhance the quality of healthcare,
ensuring more lives are saved and better health
outcomes are achieved.
REFERENCES
Ahsan, M. M., & Siddique, Z. 2022. Machine learning-
based heart disease diagnosis: A systematic literature
review. Artificial Intelligence in Medicine, 128, 102289.
Ahsan, M. M., Nazim, R., Siddique, Z., & Huebner, P. 2021.
Detection of COVID-19 patients from CT scan and
chest X-ray data using modified MobileNetV2 and
LIME. In Healthcare (Vol. 9, No. 9, p. 1099). MDPI.
Cleveland Clinic. 2023. Atypical chest pain. Retrieved from
https://my.clevelandclinic.org/health/symptoms/24935
-atypical-chest-pain
Constant, J. 1990. The diagnosis of nonanginal chest pain.
The Keio Journal of Medicine, 39(3), 187-192.
Jones, E., Johnson, B. D., Shaw, L. J., Bakir, M., Wei, J.,
Mehta, P. K., ... & Merz, C. N. B. 2020. Not typical
angina and mortality in women with obstructive
coronary artery disease: Results from the Women’s
Ischemic Syndrome Evaluation study (WISE). IJC
Heart & Vasculature, 27, 100502.
Nahar, J., Imam, T., Tickle, K. S., & Chen, Y. P. P. 2013.
Computational intelligence for heart disease diagnosis:
A medical knowledge driven approach. Expert Systems
with Applications, 40(1), 96-104.
Parmar, A., Katariya, R., & Patel, V. 2019. A review on
random forest: An ensemble classifier. In International
conference on intelligent data communication
technologies and internet of things (ICICI) 2018 (pp.
758-763). Springer International Publishing.
Shailaja, K., Seetharamulu, B., & Jabbar, M. A. 2018.
Machine learning in healthcare: A review. In 2018
Second international conference on electronics,
communication and aerospace technology (ICECA) (pp.
910-914). IEEE.
Stiglic, G., Kocbek, P., Fijacko, N., Zitnik, M., Verbert, K.,
& Cilar, L. 2020. Interpretability of machine learning-
based prediction models in healthcare. Wiley
Interdisciplinary Reviews-Data Mining and Knowledge
Discovery, 10(5).
Srinivasan, A., & Mishra, A. 2024. Receiver Operating
Characteristic (ROC) Curve Analysis for Diagnostic
Studies. In R for Basic Biostatistics in Medical
Research (pp. 253-258). Springer, Singapore.
World Health Organization. 2021. Cardiovascular disease.
Retrieved from https://www.who.int/health-
topics/cardiovascular-diseases#tab=tab_1
ICDSE 2025 - The International Conference on Data Science and Engineering
66
