
Hospital Readmission Risk Prediction Using Ensemble Learning
Mangalgouri P Kademani
a
, Yuvaraj P Rathod
b
, Shruti Nagave
c
, Omkar Harlapur
d
,
Uday Kulkarni
e
and Shashank Hegde
School of Computer Science & Engg, KLE Technological University, Hubballi, India
Keywords:
Ensemble Learning, Multilayer Perceptron, XG-Boost, Catboost, Healthcare.
Abstract:
The study focuses on features that affect of hospital readmission’s and explores how advanced machine learn-
ing algorithms can predict the chances of hospital readmission’s. Readmissions are caused by early patient
discharge, improper discharge planning, and lack of treatment, which lead to de-creased health outcomes, and
higher costs. In this study, the patient data is used from the CMS Hospital Readmissions Reduction Program
to create prediction models for hospital readmission risk. which includes over 18774 records and 12 columns
from 2019 to 2022. The machine learning models, such as MLP, XGBoost, CatBoost, and ensemble, were used
to improve the prediction’s. Where MLP achieved the accuracy of 82.69%, and XGBoost and CatBoost out-
performed MLP with scores of 85.43% and 86.50%. The accuracy of 87.08% is achieved by ensemble model,
which combined the output of all base model’s prediction outputs. Performance matrices which includes
precision, recall, F1-score were evaluated in addition to accuracy, the ensemble model obtained precision of
87.48%, recall of 87.08% , and F1-score of 86.38%. The outcomes show the result of the ensemble approach
in resolving the complex issue of hospital readmission prediction.
1 INTRODUCTION
Our topic of discussion focuses on the prediction of
hospital readmissions, a critical task in healthcare
care aimed at improving patient outcomes and re-
ducing costs. The complexity of health care data,
including missing values, discrepancies, and the in-
teraction of several readmission-causing factors(Zhou
et al., 2023), makes it difficult to effectively estimate
patient readmission risk despite continuous attempts
to reduce readmission. We can improve the accu-
racy and robustness of the prediction by using ma-
chine learning techniques(Rizinde et al., 2024). In
this various machine learning models and methods
are investigated that might handle a range of health-
care datasets. Gradient boosting and deep learning are
two types of machine learning models that are popu-
lar because of their exceptional results. In order to
predict hospital readmission’s, researchers have also
looked into deep learning(Lopez et al., 2023) and
a
https://orcid.org/0009-0000-3214-5042
b
https://orcid.org/0009-0004-2635-9975
c
https://orcid.org/0009-0005-5928-8242
d
https://orcid.org/0009-0006-6302-7093
e
https://orcid.org/0000-0003-0109-9957
Gradient boosting techniques (Slezak et al., 2021;
Kalusivalingam et al., 2012). Such as ensemble learn-
ing approach, which combines the Multilayer Percep-
tron (MLP) (Teo et al., 2023; Ti’jay Goudjerkan, ),
XGBoost (Chen et al., 2023; Hidayaturrohman and
Hanada, 2024), and CatBoost (Safaei et al., 2022;
Quan and Gopukumar, 2023) models, which can do
the better readmission prediction.
Ensemble Learning (Mahajan and Ghani, 2019;
Turgeman and May, 2016) is an effective machine
learning technique that strengthens accuracy and con-
sistency by combining the predictions of several mod-
els. This approach involves training several models
and aggregating their outputs to address a real-world
such as predicting hospital readmission’s, where ac-
curate risk analysis is essential for patient care and re-
source allocation, this process involves training multi-
ple models and combining their outputs, to efficiently
process and analyze patient data. MLP takes care of
the non-linear relationships. XGBoost and CatBoost
are also great models for structured data especially
because they can handle categorical features distantly
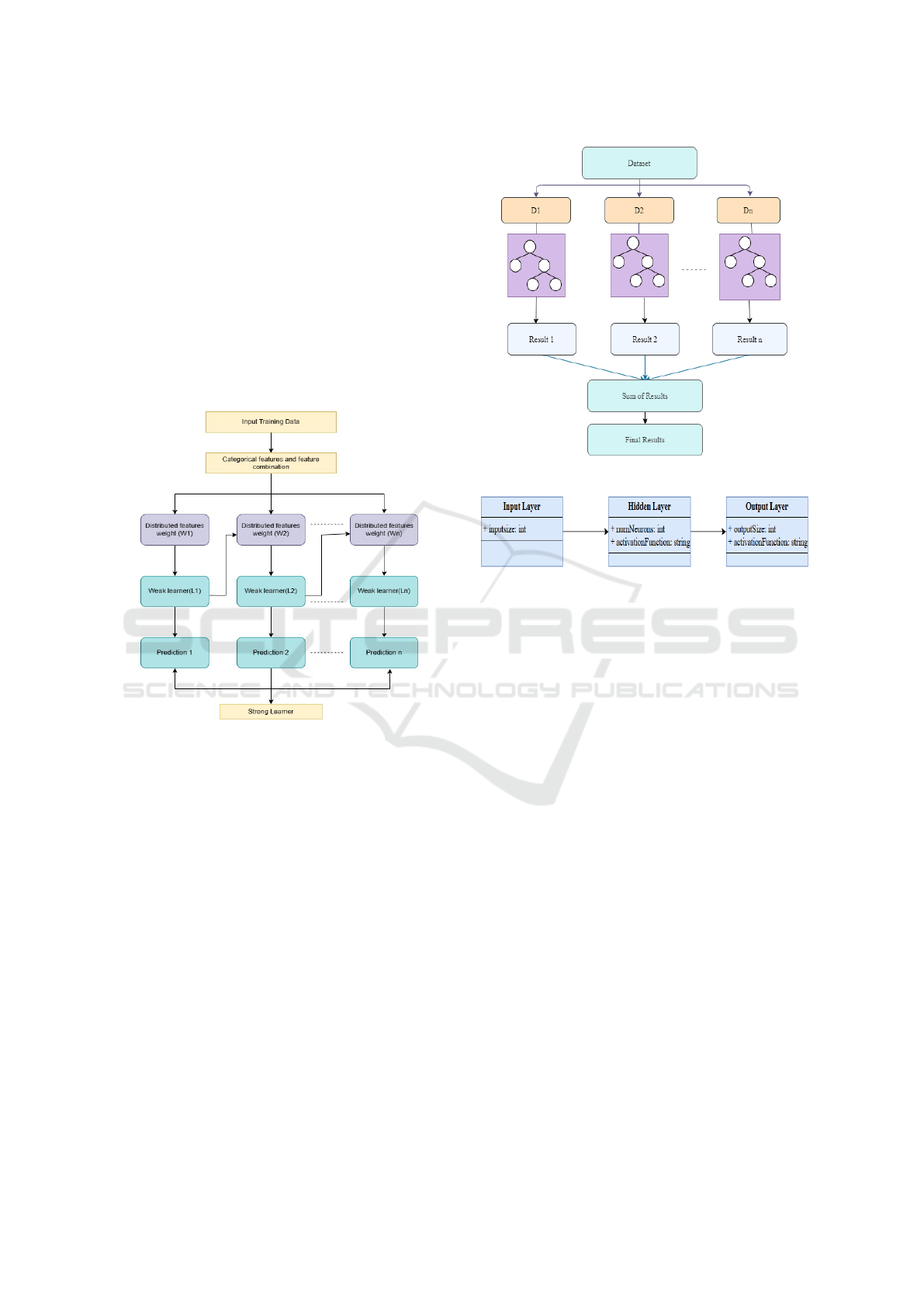
better than other models. The Figure 1 explains a
pipeline that begins with data collection, moves on
to pre-processing and feature extraction, and ends
with encoding for machine learning-based readmis-
820
Kademani, M. P., Rathod, Y. P., Nagave, S., Harlapur, O., Kulkarni, U. and Hegde, S.
Hospital Readmission Risk Prediction Using Ensemble Learning.
DOI: 10.5220/0013603200004664
Paper published under CC license (CC BY-NC-ND 4.0)
In Proceedings of the 3rd International Conference on Futuristic Technology (INCOFT 2025) - Volume 2, pages 820-826
ISBN: 978-989-758-763-4
Proceedings Copyright © 2025 by SCITEPRESS – Science and Technology Publications, Lda.

Figure 1: Pipeline of proposed methodology
sion prediction in hospitals. The set is divided into
train and test. Various models, such as MLP, XG-
Boost, and Catboost, are trained. The accuracy of
these models is then verified using their respective
results on the test set. Finally, the system uses an
ensemble learning technique, which combines the re-
sults of multiple models to improve the prediction of
hospital readmission.
The paper is divided into 5 sections listed below:
With an overview of Several methods for group learn-
ing, such as the functions MLP, XGBoost, and Cat-
Boost, Section 2 describes the algorithms for machine
learning that are currently available for hospital read-
mission prediction. The process of preparing patient
data, training models, and combining their predictions
using ensemble methods like voting or weighted av-
eraging to produce the final result is covered in Sec-
tion 3. The experimental results are presented in Sec-
tion 4, which compares a performance of ensemble
model with individual models on important metircs
such as F1-score, recall, and accuracy. Section 5 gives
additional details regarding the results implications
and future approaches for developing strong ensem-
ble learning techniques to improve hospital readmis-
sion prediction are also included in this.
2 BACKGROUND STUDY
Predicting hospital readmissions is a crucial field
of healthcare analysis that has been deeply researched
through different methods of machine learning. Be-
cause to their basic analysis and implementation, tra-
ditional models such as logistic regression(Leonard
et al., 2022) have been used frequently. When there is
a clear correlation between the input factors (such as
age, clinical history, etc.) and the output (readmission
risk), the linear model known as logistic regression
performs well. However, traditional models may find
it difficult to represent the complex and non-linear in-
teractions between variables seen in healthcare data.
For instance, non-linear relationships that are difficult
for linear models to accurately represent may develop
from interactions between different medical disorders
and treatments. As a result, these models frequently
lack predictive ability when dealing with the complex
of healthcare datasets.
In the area of hospital readmission prediction, ef-
fective tree-based algorithms like XGBoost (Hiday-
aturrohman and Hanada, 2024; Chen et al., 2023) and
CatBoost (Safaei et al., 2022; Quan and Gopukumar,
2023) have come up. To efficiently manage structured
data with missing values and complex feature interac-
tions, XGBoost applies gradient boosting. With its or-
dered boosting technique, CatBoost improves at cate-
gorical features without the need for any preprocess-
ing. While these models have shown promise, their
complexity in computation is frequently a challenge
in situations with limited resources or in applications
in real time.
Deep learning approaches, such as Recurrent Neu-
ral Network(RNN) (Chopra et al., 2017) and MLP
(Ti’jay Goudjerkan, ; Teo et al., 2023) , offer accu-
rate techniques for handling big and complex datasets.
The patient data’s cyclic patterns and non-linear re-
lationships can be captured by such models. How-
ever, many factors preventing their broader clinical
use include high computational costs, significant pre-
processing needs, and limited comprehension.
The strengths of many models have demonstrated
that ensemble learning techniques (Mienye and Sun,
2022; Yu and Xie, 2019) can significantly increase
predictive performance. In order to increase stabil-
ity and decrease variation, techniques such as vot-
ing, stacking, and bagging combine predictions from
various models. However, studies have shown that
ensembles frequently perform better than individual
models when managing the complexity of healthcare
datasets. A number of current ensemble approaches
may not be efficient, because they do not have enough
variance among base models.
To predict hospital readmissions, other machine
learning techniques such as Naive Bayes (Rao and
Battula, 2019), Random Forests (Bleich et al., 2021;
Kalusivalingam et al., 2012), and Support Vector Ma-
chine(SVM) (Wang and Paschalidis, 2019) have also
been used. These methods work well for use with
smaller datasets or for specific applications, however
they are unlikely to deal with the huge quantities of
complex healthcare data.
Although the previously discussed research are
helpful, there are circumstances where they fall short
in terms of generalization, data handling, and model
interpretability. It is challenging to deal with limited,
imbalanced datasets and categorical features. Neural
networks and other high-accuracy models frequently
Hospital Readmission Risk Prediction Using Ensemble Learning
821
lack transparency when making medical decisions.
This study uses a new ensemble approach com-
bines CatBoost, XGBoost, and MLP to overcome
the issues. The strengths of each model are as fol-
lows: The first model is CatBoost, it performs well at
handling categorical data, this method of use several
weak learners to make predictions is represented by
the CatBoost architecture in Figure 2. The first step
involves processing the input training data and assign-
ing weights (W1, W2, to Wn). After that, each weak
learner (L1, L2, to Ln) uses the scattered features to
produce a prediction. All of the predictions outcomes
are saved and integrated to create the final output pre-
diction.
Figure 2: CatBoost Architecture Diagram.
The Second Model used is XGBoost, in which it
structures data and feature relations. In XGBoost the
dataset is processed by dividing it into several subsets
(D1, D2, to Dn) using the provided XGBoost archi-
tecture in Figure 3. Individual decision trees (shown
by the circles) are then applied to each subset, pro-
ducing results that belong to those subsets (Result 1,
Result 2, to Result n). The combined final predic-
tion is produced by adding the individual outcomes
from each tree.
And the third model is MLP, it captures nonlin-
ear relationships. The Figure 4 shows the architecture
of MLP which includes several stages, comprising an
input layer, an output layer, and one or more layers
that are hidden. Every layer is completely linked to
every other layer, and the weight of each link varies
throughout training. In the ensemble learning (Ma-
hajan and Ghani, 2019; Turgeman and May, 2016),
weighted averaging is used to improve comprehen-
sion, accuracy, and strength. This work provides an
Figure 3: XGBoost Architecture Diagram.
Figure 4: MLP Architecture Diagram.
efficient and scalable solution to various healthcare
scenarios by improving the ability to generalize and
clinical use of hospital readmission prediction mod-
els through testing this approach on a difficult, large
dataset.
3 PROPOSED METHODOLOGY
The proposed methodology includes combining
each model’s predictions to create the ensemble’s
final output. Accuracy, precision, recall, and F1-score
are performance metrics that are used to evaluate the
ensemble model towards individual models.
3.1 Methods and Techniques
The proposed research improve the predicted accu-
racy and reliability of various machine learning mod-
els by combining their abilities. These are the models
that were utilized are: MLP, XGBoost, CatBoost. In
order to combine the predictions of all three models,
the ensemble model uses weighted averaging to com-
bine their results.
MLP: The feedforward neural network known as
the Multilayer Perceptron is ideal for capturing non-
linear interactions.
INCOFT 2025 - International Conference on Futuristic Technology
822

Input layer: Takes Scaled feature vector.
Hidden layer: The equation 1 uses the ReLU activa-
tion function to represent the output h
j
of the j-th neu-
ron in a neural network. In addition to adding a bias
b
j
, it calculates the weighted sum of inputs x
i
with ap-
propriate weights w
i j
. The output is set to 0 if the sum
is negative, and passes the sum unchanged otherwise.
h
j
= max
0,
n
∑
i=1
w
i j
x
i
+ b
j
!
(1)
Output layer: The equation 2 represents the sig-
moid function. In this case, z represents the linear
combination of input features, it is usually written as
z = w
T
X + b, where w are weights and b is the bias.
The output, compressed by the sigmoid function, lies
between 0 and 1, representing the probability of the
positive group (y = 1).
P(y = 1 | X) =
1
1 + e
−z
(2)
XGBoost: It is a very powerful gradient boosting al-
gorithm that works well with feature-level interaction
and structured data. The objective function is given
by equation 3. The first term
∑
n
i=1
ℓ(y
i
, ˆy
i
),is the loss
function that calculates the difference between the
predictions ( ˆy
i
) and true labels (y
i
). The second term
∑
M
m=1
Ω(T
m
), add a regularization feature that reduces
the complexity of M trees (T
m
), supporting simpler
models and minimizing overfitting.
L =
n
∑
i=1
ℓ(y
i
, ˆy
i
) +
M
∑
m=1
Ω(T
m
) (3)
Tree Weight Update: The weights are adjusted by
equation 4. The numerator
∑
g
i
collects the gradi-
ents, and the denominator
∑
h
i
indicates the curvature,
providing stability during optimization. This formula
minimizes the total loss by modifying the leaf’s con-
tribution to the prediction in the best possible way.
w
m
= −
n
∑
i=1
h
i
+ λ
n
∑
i=1
g
i
(4)
CatBoost: It is Not really designed for a lot of pre-
processing previously, but optimized for categorical
features. Where equation 5 shows the weighted to-
tal of the outputs from multiple base learners T
m
(x),
where α
m
are each model’s weights, as well as the fi-
nal prediction f (x). Here, M is the total number of
base models, and the prediction from the m-th model
is shown by T
m
(x).
f (x) =
M
∑
m=1
α
m
T
m
(x) (5)
Ensemble Learning: To leverage the individual mod-
els, predictions are combined using weighted averag-
ing by equation 6. Where the weights given to each
model are represented by w
i
. The predictions of each
specific model, Model
i
(x), are combined to create the
result of the ensemble.
EnsemblePrediction =
n
∑
i=1
w
i
· Model
i
(x) (6)
Model Evaluation: In this, performance of models are
evalued using a variety of metrics, including accuracy,
precision, recall, and F1-score. The performance of
an ensemble model is compared to that of an individ-
ual model in order to identify improvements through
the combination of multiple models.
The Ensemble Learning Workflow for hospital pa-
tient readmission prediction is described in Algorithm
1. To improve prediction accuracy, CatBoost, XG-
Boost, and MLP are used in the suggested ensem-
ble learning technique. First, numerical features are
scaled for consistency, missing values are handled,
and categorical features are encoded. After that, the
dataset is used to train each model separately. Predic-
tions are produced for the test data following training.
Higher weights are given to models that perform bet-
ter after each model’s performance is assessed using
the F1-score. Individual model outputs are weighted
and added together to determine the final ensemble
prediction. This method ensures a predictive model
that is more reliable and accurate.
4 RESULTS
The results displays performance evaluation for
different machine learning models created using hos-
pital readmission risk. The performance comparison
of an ensemble model, XGBoost, CatBoost, and MLP
is shown using accuracy, precision, recall, and F1-
score. AUC values and ROC curves are also used to
assess predictions. The experiments were carried out
on Google Colab, for effective computing and reliable
model training for high predictive performance.
4.1 Dataset Description
The Hospital Readmission dataset which is used
for this study is based on CMS Hospital Readmission
Reduction Program (Kahn III et al., 2023) which in-
cludes over 18774 records and 12 columns from 2019
to 2022. And among other metrics, the data taken
along the predicted readmission rate, expected read-
mission rate, and excess readmission ratio’s values. In
this dataset both Categorical and numerical columns
Hospital Readmission Risk Prediction Using Ensemble Learning
823

are included in the dataset. scalable modeling was
made possible by encoding categorical classifications
and normalizing the numerical features for scale con-
sistency. As the result, the dataset serves as a funda-
mental source for traing and testing ML models aimed
to forecast the possibility that more patients will re-
quire readmission.
4.2 Data Preprocessing
Cleaning the data begins with handling missing
values. The absence of data in a record, whether
intentional or not, is referred to as missing values.
Data inconsistencies alter algorithm performance and
Put in danger data integrity. Therefore, addressing
issues like bias in data becomes the second cleansing
stage. The last stage of feature optimization, which
in this case mainly comprises lowering the number of
unique values for categorical variables, is carried out
after the data has been cleaned for missing values and
other causes of bias. The various feature engineering
(Bahrami, ) steps feature creation, feature encoding,
outlier removal, feature selection are used. In fact,
while certain feature engineering processes depend
on the data and business knowledge, others such
as variable encoding, take into account what future
algorithms need to be used.
The proposed work demonstrates the training and
testing of ML models, that are MLP, XGBoost,
CatBoost for predicting the risk of readmission for
patients. To accurately assess model performance,
the dataset is separated into training and testing.
While the training set (80%) was utilized to train
the models, the testing set (20%) was reserved for
validation. In order to categorize readmission’s
according to the Excess Readmission Ratio threshold
( >1 for excess readmission’s), these are evaluated
using preprocessed data. several input features which
includes encoded category data and pre-processed
patient data, are used to get the expected result.
The MLP model is trained using regularization, early
stopping, and a single hidden layer to avoid over-
fitting. 400 estimators, a learning rate of 0.01 and
regularization to lower model complexity are used to
train XGBoost. CatBoost contains 400 estimators,
regularization, and a learning rate of 0.01 and was
intended for categorical data. In an ensemble tech-
nique, the predictions produced by each model are
merged with those from the training and test sets. To
increase overall prediction accuracy and generaliza-
tion, the weighted ensemble approach was used to in-
crease the predictive accuracy of the hospital readmis-
sion risk prediction model. With weights of 0.2, 0.35,
and 0.35, respectively, the predictions of three mod-
els MLP, XGBoost, and CatBoost were combined to
make use of each model’s strengths.
[1] Training data (X
train
,y
train
), Testing data
(X
test
,y
test
) Final predictions P
ensemble
and
evaluation metrics
Preprocessing: if categorical features exist
then
E
end
ncode them else
S
end
kip encoding if missing values exist then
H
end
andle them else
C
end
ontinue Scale numerical features as needed
Train Base Models: for each
m ∈ {CatBoost, XGBoost, MLP} do
end
m is XGBoost Tune hyperparameters else
U
end
se defaults Train m on (X
train
,y
train
)
Generate Predictions: for each
m ∈ {CatBoost, XGBoost, MLP} do
C
end
ompute P
m
= m.predict(X
test
)
Define Weights: if XGBoost performs best
then
A
end
ssign higher w
2
MLP performs best Assign
higher w
1
else
A
end
ssign equal weights
Compute Ensemble:
P
ensemble
← w
1
· P
MLP
+ w
2
· P
XGB
+ w
3
· P
Cat
Evaluate and Return: if F1-score ≥ 0.8
then
P
end
roceed to deployment else
R
end
etrain models return P
ensemble
and metrics
Algorithm 1: Ensemble Learning Workflow
INCOFT 2025 - International Conference on Futuristic Technology
824
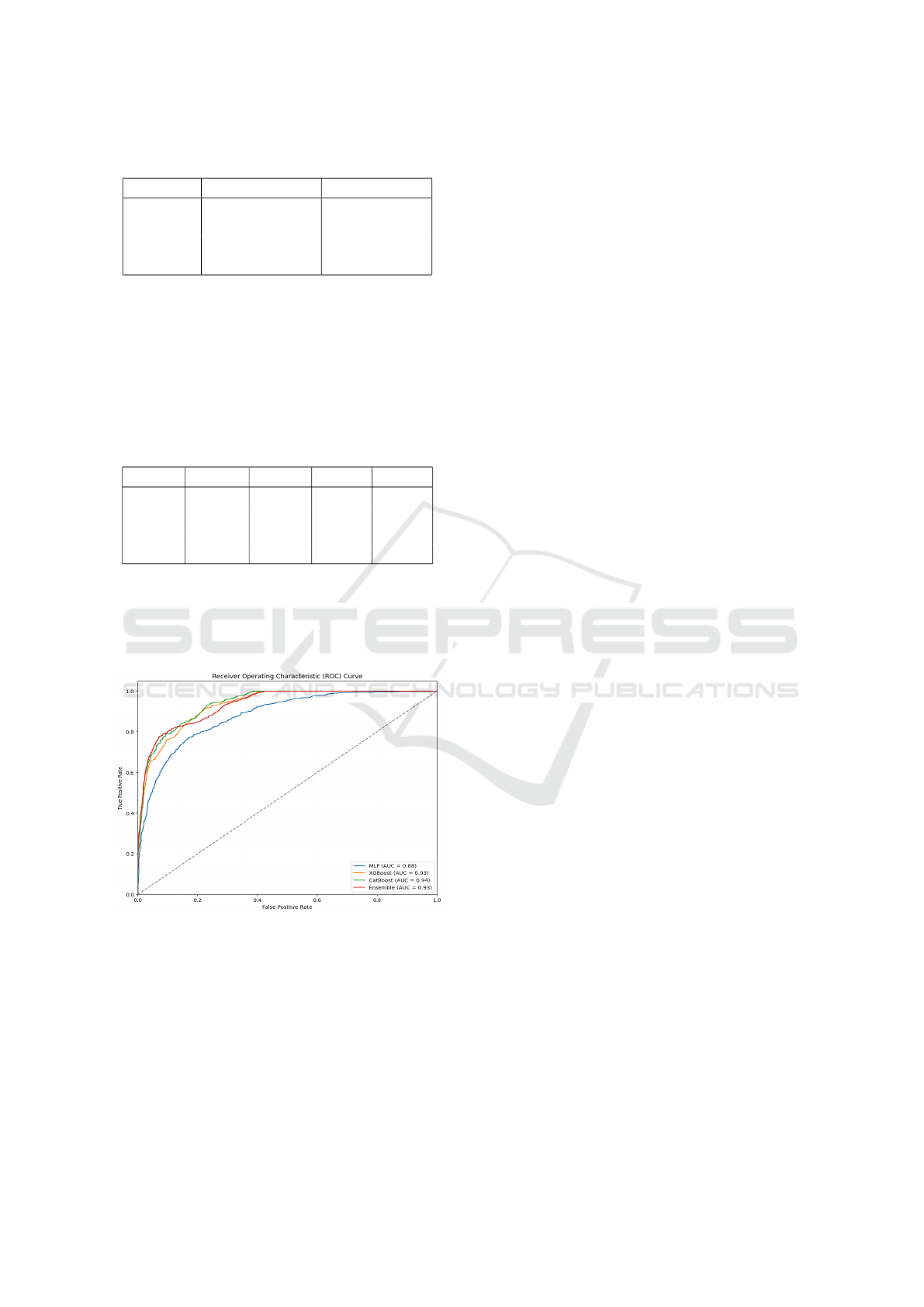
Table 1: Comparison of model accuracy for Hospital Read-
mission Prediction
Model Train Accuracy Test Accuracy
MLP 83.32% 82.69%
XGBoost 85.55% 84.43%
CatBoost 86.71% 86.60%
Ensemble 87.14% 87.08%
The output is the result of integrating the predic-
tions of individual models and an ensemble model.
The performance matrics includes accuracy, preci-
sion, recall, and F1-score are calculated for every
model. Table 1 show the comparison accuracy of train
and test of each model and Table 2 shows the perfor-
mance metrics of every model.
Table 2: Model Performance Metrics for Hospital Readmis-
sion Prediction
Model Accuracy Precision Recall F1-score
MLP 0.826897 0.822383 0.826897 0.821813
XGBoost 0.854328 0.859647 0.854328 0.844663
CatBoost 0.866045 0.869467 0.866045 0.858756
Ensemble 0.870839 0.874830 0.870839 0.863865
As shown in above Table 2, the Ensemble has
strong metrics on all performance, as Ensemble
model combines the predictions of each individual al-
gorithm, it has highest test accuracy of 87.08%.
Figure 5: ROC Curve graph of Models.
The ROC curve in Figure 5 analysis performed to
compare the performance of 4 models in prediction
of hospital readmission.With AUC value of 0.93 for
XGBoost and Ensemble, and 0.94 for CatBoost is a
best individual model in this case, outperforming XG-
Boost, a comparison of the AUC values shows that
the Ensemble model, XGBoost, CatBoost all have ex-
cellent predictive ability in identifying readmitted pa-
tients. While the MLP model achieved a moderate
AUC value of 0.88 but not as effective as other mod-
els.
5 CONCLUSION AND FUTURE
WORK
The study aimed to identify the optimal approach
for predicting hospital readmissions using machine
learning models. MLP, XGBoost, and CatBoost were
used to train models predicting readmission risk
based on the dataset features. XGBoost and CatBoost
outperformed MLP, with AUC scores of 0.93 and
0.94, while MLP with an AUC of 0.88. The ensemble
model, combining all three algorithms, achieved
an accuracy of 87.08%. These results demonstrate
that these algorithms can accurately predict hospital
readmissions. The study provides a foundation for
possible future developments in hospital readmission
prediction. Future work could focus on hyperparame-
ter tuning, advanced ensemble methods like stacking,
and incorporating additional data, such as medication
history, and treatment information, to further improve
performance.
REFERENCES
Bahrami, P. Using Ensemble Deep Learning and Feature
Engineering Approaches to Classify Hospital Read-
mitted Heart Disease Patients. PhD thesis, Toronto
Metropolitan University.
Bleich, J., Cole, B., Kapelner, A., Baillie, C. A., Gupta, R.,
Hanish, A., Calgua, E., Umscheid, C. A., and Berk,
R. (2021). Using random forests with asymmetric
costs to predict hospital readmissions. medRxiv, pages
2021–03.
Chen, R., Zhang, S., Li, J., Guo, D., Zhang, W., Wang, X.,
Tian, D., Qu, Z., and Wang, X. (2023). A study on
predicting the length of hospital stay for chinese pa-
tients with ischemic stroke based on the xgboost algo-
rithm. BMC medical informatics and decision making,
23(1):49.
Chopra, C., Sinha, S., Jaroli, S., Shukla, A., and Mahesh-
wari, S. (2017). Recurrent neural networks with non-
sequential data to predict hospital readmission of di-
abetic patients. In proceedings of the 2017 Inter-
national Conference on Computational Biology and
Bioinformatics, pages 18–23.
Hidayaturrohman, Q. A. and Hanada, E. (2024). Impact
of data pre-processing techniques on xgboost model
performance for predicting all-cause readmission and
mortality among patients with heart failure. BioMed-
Informatics, 4(4):2201–2212.
Kahn III, C. N., Rhodes, K., Pal, S., McBride, T. J., May, D.,
DaVanzo, J. E., and Dobson, A. (2023). Cms hospital
value-based programs: Refinements are needed to re-
duce health disparities and improve outcomes: Study
Hospital Readmission Risk Prediction Using Ensemble Learning
825

examines cms hospital value-based programs’ effec-
tiveness in addressing health disparities and outcomes.
Health Affairs, 42(7):928–936.
Kalusivalingam, A. K., Sharma, A., Patel, N., and Singh, V.
(2012). Enhancing hospital readmission rate predic-
tions using random forest and gradient boosting algo-
rithms. International Journal of AI and ML, 1(2).
Leonard, G., South, C., Balentine, C., Porembka, M., Man-
sour, J., Wang, S., Yopp, A., Polanco, P., Zeh, H.,
and Augustine, M. (2022). Machine learning im-
proves prediction over logistic regression on resected
colon cancer patients. Journal of Surgical Research,
275:181–193.
Lopez, K., Li, H., Lipkin-Moore, Z., Kay, S., Rajeevan,
H., Davis, J. L., Wilson, F. P., Rochester, C. L., and
Gomez, J. L. (2023). Deep learning prediction of hos-
pital readmissions for asthma and copd. Respiratory
Research, 24(1):311.
Mahajan, S. M. and Ghani, R. (2019). Using ensemble ma-
chine learning methods for predicting risk of readmis-
sion for heart failure. In MEDINFO 2019: Health and
Wellbeing e-Networks for All, pages 243–247. IOS
Press.
Mienye, I. D. and Sun, Y. (2022). A survey of ensem-
ble learning: Concepts, algorithms, applications, and
prospects. IEEE Access, 10:99129–99149.
Quan, X. and Gopukumar, D. (2023). Use of claims data to
predict the inpatient length of stay among us stroke pa-
tients. Informatics in Medicine Unlocked, 42:101337.
Rao, T. S. S. and Battula, B. P. (2019). A frame work
for hospital readmission based on deep learning ap-
proach and naive bayes classification model. Rev.
d’Intelligence Artif., 33(1):67–74.
Rizinde, T., Ngaruye, I., and Cahill, N. (2024). Machine
learning algorithms for predicting hospital readmis-
sion and mortality rates in patients with heart failure.
African Journal of Applied Research, 10(1):316–338.
Safaei, N., Safaei, B., Seyedekrami, S., Talafidaryani, M.,
Masoud, A., Wang, S., Li, Q., and Moqri, M. (2022).
E-catboost: An efficient machine learning framework
for predicting icu mortality using the eicu collabora-
tive research database. Plos one, 17(5):e0262895.
Slezak, J., Butler, L., and Akbilgic, O. (2021). The role
of frailty index in predicting readmission risk follow-
ing total joint replacement using light gradient boost-
ing machines. Informatics in Medicine Unlocked,
25:100657.
Teo, K., Yong, C. W., Chuah, J. H., Hum, Y. C., Tee,
Y. K., Xia, K., and Lai, K. W. (2023). Current
trends in readmission prediction: an overview of ap-
proaches. Arabian journal for science and engineer-
ing, 48(8):11117–11134.
Ti’jay Goudjerkan, M. J. Predicting 30-day hospital read-
mission for diabetes patients using multilayer percep-
tron.
Turgeman, L. and May, J. H. (2016). A mixed-ensemble
model for hospital readmission. Artificial intelligence
in medicine, 72:72–82.
Wang, T. and Paschalidis, I. C. (2019). Prescriptive cluster-
dependent support vector machines with an applica-
tion to reducing hospital readmissions. In 2019 18th
European Control Conference (ECC), pages 1182–
1187. IEEE.
Yu, K. and Xie, X. (2019). Predicting hospital readmis-
sion: a joint ensemble-learning model. IEEE journal
of biomedical and health informatics, 24(2):447–456.
Zhou, H., Ngune, I., Albrecht, M. A., and Della, P. R.
(2023). Risk factors associated with 30-day un-
planned hospital readmission for patients with mental
illness. International Journal of Mental Health Nurs-
ing, 32(1):30–53.
INCOFT 2025 - International Conference on Futuristic Technology
826
