
P2DS: A Holistic Approach to Psychiatric Disease Detection in
Community Pharmacies
André Dias
1,2 a
, Tiago Dias
1,2 b
, Eva Maia
1,2 c
and Isabel Praça
1,2 d
1
School of Engineering, Polytechnic of Porto, (ISEP/IPP), Porto, Portugal
2
Research Group on Intelligent Engineering and Computing for Advanced Innovation and Development (GECAD),
Porto, Portugal
Keywords: Post-Traumatic Stress Disorder, Depression, Burnout, Smart Wearables, Emotion Recognition, Artificial
Intelligence.
Abstract: Health workers appear to have an increased risk of developing psychiatric diseases, namely Post-traumatic
stress disorder (PTSD), Depression and Burnout, due to the nature of their job. In recent years, several
approaches based on artificial intelligence have emerged, using facial expression, audio, text and
physiological features to detect depression, stress and burnout. However, most of these solutions have
limitations in their capacity to simultaneously detect multiple diseases, are not widely implemented in
healthcare settings, and, in some cases, lack explainability. To address this challenge, we propose Psychiatric
Disease Detection System (P2DS), a holistic rule-based system capable of detecting PTSD, Depression and
Burnout in community pharmacists, combining emotion recognition, physiological and performance-related
features. The set of rules developed to detect each disease is based on the most objective medical literature
available, making the system explainable and suitable for healthcare environments.
1 INTRODUCTION
The World Health Organization (WHO) defines
health workers as people whose work is destined to
improve health. Those include doctors, nurses,
pharmacists and technicians (World Health
Organization, 2022). There is increasing evidence
that health workers have an elevated risk of
developing psychiatric illnesses, mainly Depression
and Post-Traumatic Stress Disorder (PTSD), and
Burnout syndrome, in great part due to the multiple
risk factors present in their job (Hill et al., 2022; Razu
et al., 2021; World Health Organization, 2022). These
include increasing workload, long shifts, an
accelerated pace of work and lack of support (Søvold
et al., 2021). The presence of the aforementioned
diseases imposes serious consequences, namely
poorer patient care, increased work-related mistakes,
increased absenteeism and greater patient
a
https://orcid.org/0000-0001-5194-2784
b
https://orcid.org/0000-0002-1693-7872
c
https://orcid.org/0000-0002-8075-531X
d
https://orcid.org/0000-0002-2519-9859
dissatisfaction (Gregório et al., 2017; Samir AlKudsi
et al., 2022; Søvold et al., 2021).
In past years, researchers have developed multiple
systems to detect or predict psychiatric diseases.
These systems use physiological, audio and image
data, combined or separately, which is then run
through machine learning models to predict diseases
(Saganowski et al., 2023). Literature indicates that
these systems have revolved around pre-established
datasets and single disease detection. They have been
tested in patients, students, nurses, and corporate staff
(Chikersal et al., 2021; Eom et al., 2023; Francese &
Attanasio, 2022; Otsuka et al., 2023a; Yang et al.,
2020). Therefore, a gap in testing is noted in a
community pharmacy setting.
Hence, we propose Psychiatric Disease Detection
System (P2DS), a holistic system capable of detecting
and alerting for the presence PTSD, Major depressive
episode and Burnout syndrome. This can be achieved
through the detection of emotion and collection of
768
Dias, A., Dias, T., Maia, E. and Praça, I.
P2DS: A Holistic Approach to Psychiatric Disease Detection in Community Pharmacies.
DOI: 10.5220/0012568200003657
Paper published under CC license (CC BY-NC-ND 4.0)
In Proceedings of the 17th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2024) - Volume 2, pages 768-775
ISBN: 978-989-758-688-0; ISSN: 2184-4305
Proceedings Copyright © 2024 by SCITEPRESS – Science and Technology Publications, Lda.

physiological and performance information. All this
data is then correlated using a rule-based system,
grounded in the most objective medical literature,
leading to the detection of the most common
psychiatric diseases in pharmacists and the creation
of an alert for the need to seek medical care. We
expect that this system could help on early detection
of psychiatric diseases, preventing health issues for
community pharmacists and improving patient safety.
2 STATE OF THE ART
Health workers have a high prevalence of psychiatric
diseases, especially after the COVID-19 pandemic
(Braquehais & Vargas-Cáceres, 2023). According to
recent literature, 100% of health workers reported
Burnout and, regarding psychiatric diseases, 21,7%
reported PTSD, 16,1% Anxiety and 13,3%
Depression (Hill et al., 2022; Jakovljevic et al., 2021).
When focusing on pharmacists, these numbers can go
up to 50% for Anxiety and 44% for Depression, and
about 60% for Burnout syndrome (Dee et al., 2022;
Samir AlKudsi et al., 2022; Weichel et al., 2021).
Among the possible causes, the high community
pharmacists’ workload has been a major concern
(Gregório et al., 2017; Samir AlKudsi et al., 2022).
2.1 Psychiatric Diseases and Burnout
Anxiety disorders are a large group of psychiatric
diseases. According to the Diagnostic and Statistical
Manual of Mental Disorders (DSM-V), examples of
Anxiety disorders are Generalized Anxiety Disorder,
Panic Disorder and Phobias (American Psychiatric
Association, 2013). Clinically, Anxiety can be
experienced through psychological and physical
symptoms. Psychological symptoms include fearful
anticipation, which is the sensation of fear before a
specific (phobia) or non-specific (generalized) event,
worrying thoughts, irritability, restlessness and poor
concentration. Physical symptoms can range from
palpitations (tachycardia) or tachypnea to increased
urinary frequency and mydriasis. Sleep disturbances,
namely initial insomnia, are also common. It is
defined by a Wake After Sleep Onset (WASO) or
Sleep Onset Latency (SOL) superior or equal to 30
minutes, at least three nights per week (Craske et al.,
2017; Harrison et al., 2017; Lichstein et al., 2003).
According to DSM-V, PTSD is allocated to the stress-
related disorders group. To diagnose this condition, a
preceding traumatic event (witnessed or experienced)
is necessary. In response to the causative trauma, the
patient develops intrusive ideas (for example, re-
experiencing the traumatic event or having
flashbacks), leading to the avoidance of triggering
stimuli, which are usually related to the traumatic
event. Negative alterations in cognition and mood are
present, for example amnesia, self-negative beliefs
(guilt), and a negative emotional state (that includes
fear or anger). Other symptoms that may be present
are Anxiety-related, namely poor concentration,
insomnia, and irritability. To establish a diagnosis,
these symptoms must be present for over one month
and cause functional impairment (American
Psychiatric Association, 2013; Sareen, 2023).
Depressive disorders are characterised by
depressed mood and lack of willingness and joy in
activities that were once enjoyable (Harrison et al.,
2017). Sadness is typically associated with Depression.
However, for a depressive episode to occur, sadness
must be present every day, for the most part of the day
and lasting a minimum of two weeks. Other symptoms
that help establishing the diagnosis are insomnia, early
awakenings, fatigue, diminished efficiency, loss of
weight (at least 5% body weight in 1 month) and
anorexia. There are also feelings of worthlessness and
guilt, which are usually excessive or inappropriate. In
milder or atypical forms of the disease, symptoms that
overlap with Anxiety disorders can occur, for example,
irritability and hypersomnia (American Psychiatric
Association, 2013; Bains & Abdijadid, 2023; Harrison
et al., 2017).
Burnout syndrome is a response to chronic work
stress and can be defined by emotional exhaustion,
depersonalization and lack of personal achievement.
Emotional exhaustion typically manifests with
tiredness and fatigue, leading to increased difficulty
adapting to the work environment, as the person stops
having the necessary emotional energy to cope with
work. Depersonalization is described as a detachment
or indifference towards co-workers, sometimes
leading to negative attitudes due to increased
irritability. At last, people experiencing lack of
personal achievement typically refer a feeling of
worthlessness, of not being good enough or feeling
that they are underperforming at work. Furthermore,
burnout syndrome can be contagious. This
phenomenon is called emotional contagion and is
particularly common in health settings. It can be
detected if other coworkers start experiencing the
same symptoms and emotions (Edú‐valsania et al.,
2022; Nápoles, 2022). A person with burnout
syndrome expresses typical emotions that,
accordingly to Otsuka et. al, are increased surprise
and sadness, and decreased happiness, for more than
one month. However, the authors only highlight the
P2DS: A Holistic Approach to Psychiatric Disease Detection in Community Pharmacies
769

role of decreased happiness as a predictive factor for
burnout syndrome (Otsuka et al., 2023b).
There are numerous consequences to the
aforementioned diseases. In the case of Depression
and Anxiety, examples include an increased risk for
coronary artery disease (Ayers & de Visser, 2021).
Depression alone increases the risk of type 2 Diabetes
Mellitus and Parkinson disease and ultimately, if
untreated, can lead to death by suicide (American
Psychiatric Association, 2013; Ayers & de Visser,
2021). Furthermore, there is an increased risk for
substance abuse and social isolation, leading to
functional decline. In terms of work-related
consequences, PTSD, Depression and Burnout lead to
increased absenteeism, work-related mistakes and
diminished productivity (American Psychiatric
Association, 2013; Craske et al., 2017; Edú‐valsania
et al., 2022; Lerner et al., 2010; Vignoli et al., 2017).
In conclusion, there is a growing urgency to address
the emotional, physical and mental exhaustion of
health workers (Mollica & Fricchione, 2021).
2.2 Related Work
In the field of psychiatric condition detection,
multiple approaches have surfaced for the detection
of Depression and stress, using facial expression,
speech, and physiological data as the main features
analysed (Saganowski et al., 2023).
Concerning PTSD, multiple works have emerged
for stress detection. Grupta et. al developed a system
based in the Wearable Stress and Affect Detection
(WESAD) dataset, containing real-world data from
corporate employees. Physiological data (ECG,
temperature, respiratory rate, electrodermal activity
and electromyogram) was collected through smart
bands, allowing the identification of employees with
abnormal levels of stress (Gupta et al., 2022). A
similar approach has been used on real-word
healthcare data, in an experimental fashion. Eom et.
al used a dataset containing over 1000 hours of
physiological data captured by an Empatica E4 band,
used by hospital nurses during the COVID-19
pandemic. The nurses were also instructed to answer
a stress-related survey to help validating the acquired
data, which was then processed in a multimodal
Convolutional Neural Network (CNN) model to
predict stress. Although real-world data was used, the
model was not implemented on the field (Eom et al.,
2023). Muñoz and Iglesias tried a different approach,
using text. They used the datasets Dreaddit, Natural
Stress Emotion and TensiStrenght, which contain text
data from Reddit, real world interviews and Twitter,
respectively. Data was processed in a lexicon-based
framework for the detection of stress (Muñoz &
Iglesias, 2022). Keystroke analysis has also been used
to this end by Bakkialakshmi and Sudalaimuthu. The
authors collected typing data with the help of 200
volunteers which was posteriorly run through a
Dynamic Cat-Boost algorithm to detect stress. (G.L.
Bajaj Institute of Technology & Management, 2022).
Rodrigues and Correia combined physiology and
image features of 28 healthy volunteers of an
insurance company. They collected heart rate and eye
closure from users and validated data with stress-
related questionnaires, serving as input for training
machine learning models capable of predicting stress
(Rodrigues & Correia, 2023). Singh et. al collected
video and audio data from students using cameras and
smartphone microphones, which was then run though
machine learning models to detect stress (Singh et al.,
2022). Lastly, Dogan and Akbulut combined
physiological, audio and visual data from the
WorkStress3D dataset for stress detection, by
analysing facial expressions, physiological and audio
data (Dogan & Akbulut, 2023). Although stress
relates to PTSD, to the best of the author’s
knowledge, there are no systems for PTSD detection.
Concerning Depression, Francese et. al used a
system that combined speech and facial recognition
to increase the accuracy of the Beck Depression
Inventory II (BDI-II) questionnaire, a screening tool
for Depression. The combination between facial
expression, speech and the answers provided in BDI-
II impressed both clinicians and patients, who
highlighted it as helpful in decision making (Francese
& Attanasio, 2022). Yoon et al. explored the dataset
D-Vlog, consisting of 160 hours of Youtube Vlog
video. Speech and facial expressions were extracted,
processed and combined for the detection of
depression (Yoon et al., 2022). Anshul et. al tried a
different approach, using text, image and account
details from Twitter users. The collected data was
used to train three different machine learning models
to identify Depression (Anshul et al., 2023). Yang et.
al used a similar methodology, retrieving Facebook
data (text and account details) from the dataset
“myPersonality” and Thorstad and Wolff used online
text from Reddit to predict user Depression (Thorstad
& Wolff, 2019; Yang et al., 2020). Park and Moon
collected speech and text data from the DAIC-WOZ
Dataset, which were processed separately and then
fused by a multimodal fusion model to recognise
Depression (Park & Moon, 2022). Chikersal et al
used data from smartphones and fitness trackers to
identify Depression on campus students. The
collected data included number of calls, GPS
location, phone usage, steps, sleep and behaviour.
HEALTHINF 2024 - 17th International Conference on Health Informatics
770
Comparatively to similar works, this had the most
participants and variety of devices and data sources
(Chikersal et al., 2021).
Regarding Burnout, to the best of the authors
knowledge, there are no detection systems that
comprise wearables, facial expression, or audio.
Despite this, Otsuka et. al studied the relation
between emotions and Burnout by detecting the facial
expression of the participants. They used a “Face
Recognition and Attendance App” for facial
recognition and the questionnaire BAT-J (Japanese
version of the Burnout Assessment Scale) for Burnout
screening (Otsuka et al., 2023a).
Table 1 encompasses the various approaches
previously described. Notably, only the study by Eom
et al. uses data from health workers, although the
system was not tested in a healthcare setting. In
contrast, Francese et al.'s work on Depression took
place on a healthcare setting but targeted patients. No
studies were found for the detection of a combination
of diseases.
3 PSYCHIATRIC DISEASES
DETECTION SYSTEM
The analysis of medical literature related to the three
psychiatric diseases under analysis, PTSD, Major
Depressive Episode and Burnout Syndrome,
permitted the identification of the key characteristics
present on each condition. We have aggregated these
into three different domains: (i) human emotion, (ii)
physiological signs and (iii) performance metrics.
Considering the holistic setting in which these
diseases can be predicted, we propose P2DS, a
psychiatric diseases detection system composed of
three alert-generation modules, one for each domain,
and a rule-based inference engine capable of
correlating the alerts generated via classification
rules. Figure 1 describes a general overview of P2DS.
In this architecture, the modules defined as Emotion
Recognizer, Physiology Monitor and Performance
Collector are constant observers of the pharmacists’
emotions, physiological signs and performance
metrics in the context of the pharmacy, outputting a
great amount of data in real-time. The correlation
Table 1. Detection of Stress, Depression and Burnout Approaches Summary.
Author and year Psychiatric condition Field-tested Features
(Francese & Attanasio, 2022) Depression (aid only) Yes Speech + Facial recognition
(Yoon et al., 2022) Depression No Speech + Facial recognition
(Anshul et al., 2023) Depression No
Text + Online image + Account
details
(Yang et al., 2020) Depression No Text + Account details
(Thorstad & Wolff, 2019) Depression No Text
(Park & Moon, 2022) Depression No Speech + Text
(Chikersal et al., 2021) Depression Yes
Physiologic signs + GPS location
+ calls numbe
r
(Gupta et al., 2022) Stress No Physiologic signs
(Eom et al., 2023) Stress No Physiologic signs + Questionnaire
(Muñoz & Iglesias, 2022) Stress No Text
(G.L. Bajaj Institute of Technology
& Mana
g
ement, 2022)
Stress Yes Typing patterns
(Rodrigues & Correia, 2023) Stress Yes
Physiologic signs + Eye closure +
Questionnaire
(Singh et al., 2022) Stress No Speech + Facial recognition
(Dogan & Akbulut, 2023) Stress No
Physiologic signs + Speech +
Facial reco
g
nition
(Otsuka et al., 2023a) Burnout Yes Facial recognition + Questionnaire
P2DS: A Holistic Approach to Psychiatric Disease Detection in Community Pharmacies
771
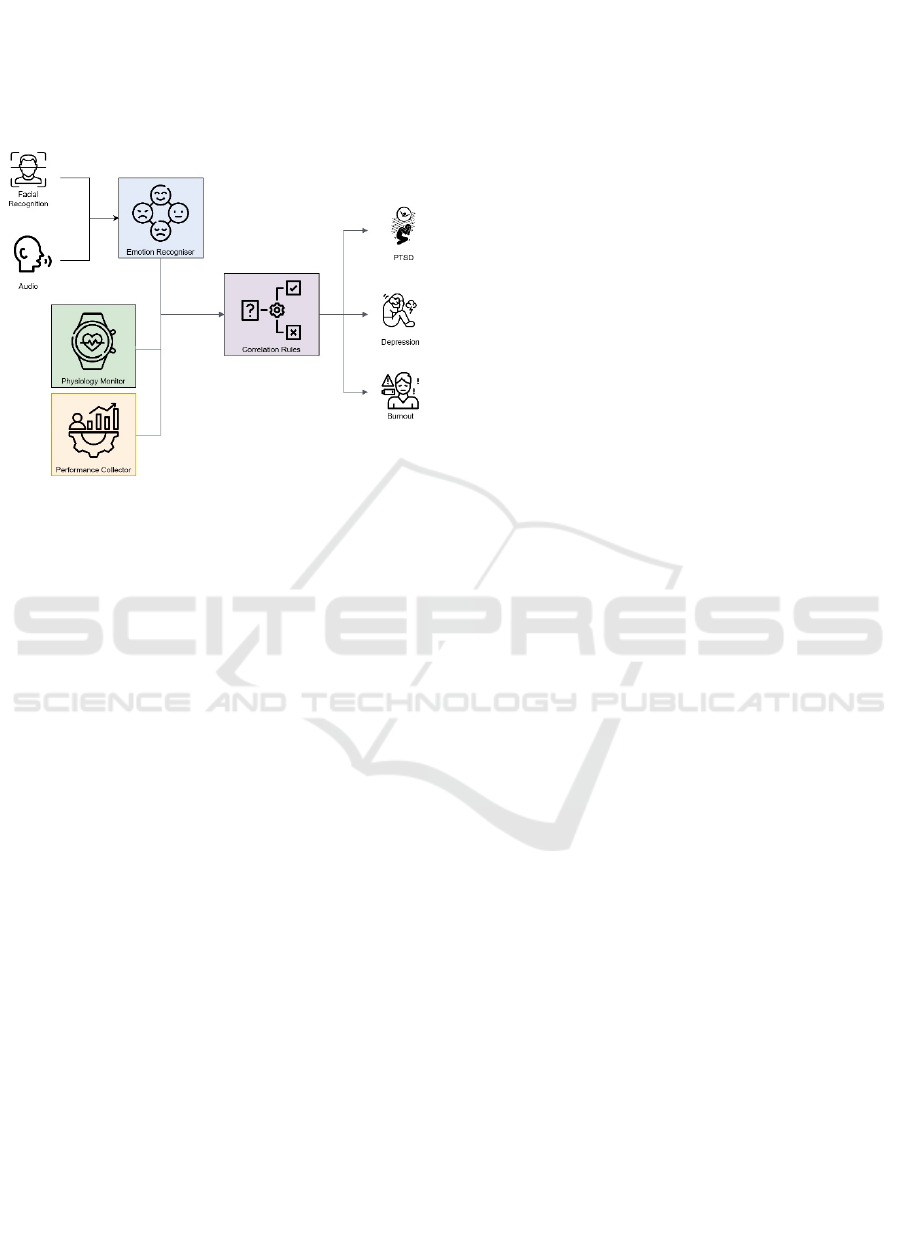
engine ingests this information and processes it using
the classification rules defined in its knowledge base
to predict the presence of psychiatric diseases, raising
alerts for the need to seek medical attention. The
following subsections describe in greater detail the
intricacies and characteristics of each subsystem.
Figure 1: General overview of P2DS.
3.1 Emotion Recogniser
Emotion is a broad term that includes our affect,
mood, and impulses. It is generally divided into three
separate components: a cognitive one, relative to how
our interpretation of a situation modulates emotion; a
physiological one, related to the physiologic changes
in response to emotions; and lastly a behavioural one,
which includes our facial expressions (Ayers & de
Visser, 2021). Technological progress has allowed
the identification of human emotions through these
components, with most recent approaches using
Machine Learning (Cai et al., 2023; Pan et al., 2023).
The Emotion Recognizer is intended to perform
emotion classification using Machine Learning
models and relying on image and audio data, as these
would be the expected means of communication
utilized in a pharmacy. These classifiers could be
trained effectively utilizing pre-existing datasets,
providing that they follow Paul Ekman’s model of
basic emotions, a standard, cross-cultural, recognized
model defining 6 universal emotions: sadness,
happiness, disgust, anger, surprise and fear, plus
neutral (Ayers & de Visser, 2021).
Regarding the data to train these classification
models, there is a wide range of datasets for emotion
detection, which have been collected in natural and
induced environments. However, literature shows
that models trained with data captured in a controlled
environment tend to be less applicable in a real
context with real conditions (Aguilera et al., 2023).
Since this module constitutes multimodality, a
dataset like MELD or RECOLA would be fit for
training the model (Poria et al., n.d.; Ringeval et al.,
2013). Nonetheless, the importance of unimodal
datasets, such as IFEED, cannot be overlooked, as
these could provide valuable data to increase the
model’s performance and generalizability (T. Dias et
al., 2023).
3.2 Physiology Monitor
The popularity of wearable health devices has
increased in the recent years, as reflected by an
increasing market value over the years, with more
units sold (D. Dias & Cunha, 2018; Escobar-Linero et
al., 2023; Lu et al., 2020). These devices allow for the
continuous monitorization of a person’s vital signs,
providing a stream of real-time data. They have the
advantage of being non-obtrusive and are readily
accessible. As so, similarly to other studies cited
above, the Physiology Monitor uses wearable health
devices, such as smartwatches, for collecting sleep
data (SOL, WASO and awakening time), cardiac and
respiratory rate, tremor (via electromyogram) and
sweating (via electrodermal activity).
Weight changes can be monitored by establishing
the initial weight and subsequently conducting
monthly re-evaluations. The use of a Bluetooth scale
obviates the necessity for manual weight input.
Afterwards, weight variation would be the difference
between the previous and the current weight,
subsequently turned into a percentage.
3.3 Performance Collector
Psychiatric diseases imply the existence of functional
impairment, which may manifest by loss of perfor-
mance (Telles-Correia et al., 2018). To measure this,
we propose the Performance Collector, an information
system designed to gather data from the software
systems of pharmacies concerning the productivity,
work-related errors, and absenteeism of pharmacists.
The standard values for these parameters should be
based on the pharmacy’s estimates, as different
pharmacies have different numbers of employees, sales
volumes and working hours (Gregório et al., 2017).
Values that are significantly different to those defined
could pose a red flag for all conditions.
3.4 Correlation Engine
The Correlation Engine is a rule-based inference
engine that leverages expert knowledge in the form of
classification rules to perform inference. This module
HEALTHINF 2024 - 17th International Conference on Health Informatics
772
aggregates evidence from all three subsystems,
leveraging rules to analyse the data and infer alert-
raising conclusions. These rules include objective
emotions, signs and other information related to each
psychiatric disease.
We propose two sets of medical literature-based
rules, complementary to this system, which are
subdivided into main and adjuvant. The main rules
include information regarding emotion. The adjuvant
rules allow for a more fine-grained detection of each
disease and comprise physiological and performance
information. Since these are grounded on medical
literature, our system achieves a greater degree of
explainability in comparison to existing alternatives.
In PTSD, we defined persistent fear (for over 1
month) as a necessary condition. The adjuvant
conditions are tachycardia, tachypnea, increased
sweating, tremor, insomnia, increased absenteeism,
work-related mistakes, diminished productivity, and
irritability. As irritability is nonspecific, we considered
it an adjuvant condition rather than a main one.
For Major depressive episode, daily sadness, for
the most part of the day and during at least two weeks
is a main condition. The adjuvants are insomnia (as
defined earlier), early awakenings (compared to the
normal personal awakening time), weight loss
superior to 5% of total body weight in one month,
increased absenteeism, work-related mistakes and
diminished productivity. To cover for atypical
Depression symptoms, hypersomnia (defined by
delayed awakening when compared to normal) and
irritability are also adjuvant conditions.
For Burnout syndrome the main condition is
decreased happiness for more than one month, based
on the work of Otsuka et.al (Otsuka et al., 2023a).
Adjuvant conditions are increased absenteeism,
work-related mistakes, diminished productivity,
irritability and emotional contagion.
To increase accuracy, we propose the application
of standardized score-based questionnaires, namely
Primary Care PTSD Screening questionnaire (PC-
PTSD-5) for PTSD, Patient Health Questionnaire-9
(PHQ-9) for Depression and Burnout Assessment
Tool (BAT) for Burnout. (Bains & Abdijadid, 2023;
Edú‐valsania et al., 2022; Sareen, 2023; Sinval et al.,
2022). Table 2 summarizes all these rules.
4 CONCLUSIONS
This article presents a novel solution for the detection
of the most common psychiatric diseases in healthcare
workers, particularly community pharmacists.
Comparatively to other existing systems, our proposal
detects three different conditions: PTSD, Major
depressive episode and Burnout syndrome, which, to
the best of the authors knowledge, has not been done.
In addition, we designed this system to be as holistic as
possible, respecting objective medical literature
available, and combining image, audio, physiological
and performance data. In comparison to other works
that also combine multiple modalities, ours is
explainable, as each correlation can be explained by the
classification rules defined. In addition to the field of
psychiatric disease detection, we also define, design
and architect a system purposefully built to be
implemented in the context of community pharmacies.
Data collection in this setting is as non-obtrusive as
possible, requiring only the use of a wristband,
monthly weight determinations and image and audio
capturing. Furthermore, this work contributes to the
knowledge of psychiatric disease detection, by
analysing several sources of available medical
literature, using the most objective criteria possible to
design the rules.
Table 2: Correlation Rules for each disease.
Conditions PTSD Ma
j
or De
p
ressive E
p
isode Burnout S
y
ndrome
Main condition
Increase in fear for more
than one month
Daily sadness for at least two weeks
Decreased happiness for
more than one month
Adjuvant
conditions
Tachycardia
Weight loss superior to 5% in one
month
Emotional contagion
Tachypnea Early awakenings
Increased sweatin
g
Insomnia Increased tremo
r
Insomnia
Increased absenteeis
m
Decreased productivit
y
Increased wor
k
-related mistakes
Irritabilit
y
Questionnaire PC-PTSD-5 PHQ-9 BAT
P2DS: A Holistic Approach to Psychiatric Disease Detection in Community Pharmacies
773

ACKNOWLEDGEMENTS
This work has received funding from the project
ForPharmacy (P2020-COMPETE-FEDER number
070053). This work has also received funding from
projects UIDB/00760/2020 and UIDP/00760/2020.
REFERENCES
Aguilera, A., Mellado, D., & Rojas, F. (2023). An
Assessment of In-the-Wild Datasets for Multimodal
Emotion Recognition. Sensors, 23(11).
American Psychiatric Association. (2013). Diagnostic and
statistical manual of mental disorders (5th ed.).
Anshul, A., Pranav, G. S., Rehman, M. Z. U., & Kumar, N.
(2023). A Multimodal Framework for Depression
Detection During COVID-19 via Harvesting Social
Media. IEEE Transactions on Computational Social
Systems.
Ayers, S., & de Visser, R. (2021). Psychology for Medicine
& Healthcare (3rd Edition) (Sage Publishing).
Bains, N., & Abdijadid, S. (2023, April 10). Major
Depressive Disorder. StatPeals.
https://www.ncbi.nlm.nih.gov/books/NBK559078/
Braquehais, M. D., & Vargas-Cáceres, S. (2023).
Psychiatric Issues Among Health Professionals. In
Medical Clinics of North America (Vol. 107, Issue 1,
pp. 131–142). W.B. Saunders.
Cai, Y., Li, X., & Li, J. (2023). Emotion Recognition Using
Different Sensors, Emotion Models, Methods and
Datasets: A Comprehensive Review. In Sensors (Vol.
23, Issue 5). MDPI.
Chikersal, P., Doryab, A., Tumminia, M., Villalba, D. K.,
Dutcher, J. M., Liu, X., Cohen, S., Creswell, K. G.,
Mankoff, J., David Creswell, J., Goel, M., & Dey, A.
K. (2021). Detecting depression and predicting its onset
using longitudinal symptoms captured by passive
sensing: A machine learning approach with robust
feature selection. ACM Transactions on Computer-
Human Interaction, 28(1).
Craske, M. G., Stein, M. B., Eley, T. C., Milad, M. R.,
Holmes, A., Rapee, R. M., & Wittchen, H. U. (2017).
Anxiety disorders. Nature Reviews Disease Primers, 3.
Dee, J., Dhuhaibawi, N., & Hayden, J. C. (2022). A
systematic review and pooled prevalence of burnout in
pharmacists. In International Journal of Clinical
Pharmacy. Springer Science and Business Media
Deutschland GmbH.
Dias, D., & Cunha, J. P. S. (2018). Wearable health
devices—vital sign monitoring, systems and
technologies. In Sensors (Switzerland) (Vol. 18, Issue
8). MDPI AG.
Dias, T., Vitorino, J., Oliveira, J., Oliveira, N., Maia, E., &
Praça, I. (2023). IFEED: Interactive Facial Expression
and Emotion Detection Dataset. Zenodo.
Dogan, G., & Akbulut, F. P. (2023). Multi-modal fusion
learning through biosignal, audio, and visual content for
detection of mental stress. Neural Computing and
Applications, 35(34), 24435–24454.
Edú‐valsania, S., Laguía, A., & Moriano, J. A. (2022).
Burnout: A Review of Theory and Measurement. In
International Journal of Environmental Research and
Public Health (Vol. 19, Issue 3). MDPI.
Eom, S., Eom, S., & Washington, P. (2023). SIM-CNN:
Self-Supervised Individualized Multimodal Learning
for Stress Prediction on Nurses Using Biosignals.
Escobar-Linero, E., Muñoz-Saavedra, L., Luna-Perejón, F.,
Sevillano, J. L., & Domínguez-Morales, M. (2023).
Wearable Health Devices for Diagnosis Support:
Evolution and Future Tendencies. In Sensors (Vol. 23,
Issue 3). MDPI.
Francese, R., & Attanasio, P. (2022). Emotion detection for
supporting depression screening. Multimedia Tools and
Application.
G.L. Bajaj Institute of Technology & Management. (2022).
2022 International Conference on Computational
Intelligence and Sustainable Engineering Solutions
(CISES) 20-21 May 2022.
Gregório, J., Cavaco, A. M., & Lapão, L. V. (2017). How
to best manage time interaction with patients?
Community pharmacist workload and service provision
analysis. Research in Social and Administrative
Pharmacy, 13(1), 133–147.
Gupta, A., Raut, A., Yadav, R., Kumar, M., & Chaurasiya,
V. K. (2022). A Hybrid Approach based Stress
Monitoring System for Office Environment using IoT.
INDICON 2022 - 2022 IEEE 19th India Council
International Conference.
Harrison, P., Cowen, P., Burns, T., & Fazel, M. (2017).
Shorter Oxford Textbook of Psychiatry. Shorter Oxford
Textbook of Psychiatry.
Hill, J. E., Harris, C., Danielle L., C., Boland, P., Doherty,
A. J., Benedetto, V., Gita, B. E., & Clegg, A. J. (2022).
The prevalence of mental health conditions in
healthcare workers during and after a pandemic:
Systematic review and meta-analysis. In Journal of
Advanced Nursing (Vol. 78, Issue 6, pp. 1551–1573).
John Wiley and Sons Inc.
Jakovljevic, B., Stojanovic, K., Turnic, T. N., &
Jakovljevic, V. L. (2021). Burnout of physicians,
pharmacists and nurses in the course of the covid-19
pandemic: A serbian cross-sectional questionnaire
study. International Journal of Environmental
Research and Public Health, 18(16).
Lerner, D., Adler, D. A., Rogers, W. H., Chang, H.,
Lapitsky, L., McLaughlin, T., & Reed, J. (2010). Work
Performance of Employees With Depression: The
Impact of Work Stressors. American Journal of Health
Promotion : AJHP, 24(3), 205.
Lichstein, K. L., Durrence, H. H., Taylor, D. J., Bush, A. J.,
& Riedel, B. W. (2003). Quantitative criteria for
insomnia. Behaviour Research and Therapy, 41(4),
427–445.
Lu, L., Zhang, J., Xie, Y., Gao, F., Xu, S., Wu, X., & Ye,
Z. (2020). Wearable health devices in health care:
Narrative systematic review. In JMIR mHealth and
uHealth (Vol. 8, Issue 11). JMIR Publications Inc.
HEALTHINF 2024 - 17th International Conference on Health Informatics
774

Mollica, R. F., & Fricchione, G. L. (2021). Mental and
physical exhaustion of health-care practitioners. In The
Lancet (Vol. 398, Issue 10318, pp. 2243–2244).
Elsevier B.V.
Muñoz, S., & Iglesias, C. A. (2022). A text classification
approach to detect psychological stress combining a
lexicon-based feature framework with distributional
representations. Information Processing &
Management, 59(5), 103011.
Nápoles, J. (2022). Burnout: A Review of the Literature.
Update: Applications of Research in Music Education,
40(2), 19–26.
Otsuka, Y., Sagisaka, Y., Nakamura, J., Hara, K., Okada,
M., Takeuchi, Y., Tsuchiya, M., & Monden, Y.
(2023a). Happiness Detected by the Emotion Cognition
System Is Associated with Burnout in an Information
Technology Products and Services Trading Company.
International Journal of Environmental Research and
Public Health, 20(3).
Otsuka, Y., Sagisaka, Y., Nakamura, J., Hara, K., Okada,
M., Takeuchi, Y., Tsuchiya, M., & Monden, Y.
(2023b). Happiness Detected by the Emotion Cognition
System Is Associated with Burnout in an Information
Technology Products and Services Trading Company.
International Journal of Environmental Research and
Public Health, 20(3).
Pan, B., Hirota, K., Jia, Z., & Dai, Y. (2023). A review of
multimodal emotion recognition from datasets,
preprocessing, features, and fusion methods.
Neurocomputing, 561, 126866.
Park, J., & Moon, N. (2022). Design and Implementation of
Attention Depression Detection Model Based on
Multimodal Analysis. Sustainability (Switzerland),
14(6).
Poria, S., Hazarika, D., Majumder, N., Naik, G., Cambria,
E., & Mihalcea, R. (n.d.). MELD: A Multimodal Multi-
Party Dataset for Emotion Recognition in
Conversations.
Razu, S. R., Yasmin, T., Arif, T. B., Islam, M. S., Islam, S.
M. S., Gesesew, H. A., & Ward, P. (2021). Challenges
Faced by Healthcare Professionals During the COVID-
19 Pandemic: A Qualitative Inquiry From Bangladesh.
Frontiers in Public Health, 9, 1024.
Ringeval, F., Sonderegger, A., Sauer, J., & Lalanne, D.
(2013). Introducing the RECOLA multimodal corpus of
remote collaborative and affective interactions. 2013
10th IEEE International Conference and Workshops on
Automatic Face and Gesture Recognition, FG 2013.
Rodrigues, F., & Correia, H. (2023). Semi-supervised and
ensemble learning to predict work-related stress.
Journal of Intelligent Information Systems.
Saganowski, S., Perz, B., Polak, A. G., & Kazienko, P.
(2023). Emotion Recognition for Everyday Life Using
Physiological Signals From Wearables: A Systematic
Literature Review. In IEEE Transactions on Affective
Computing (Vol. 14, Issue 3, pp. 1876–1897). Institute
of Electrical and Electronics Engineers Inc.
Samir AlKudsi, Z., Hany Kamel, N., El-Awaisi, A., Shraim,
M., & Saffouh El Hajj, M. (2022). Mental health,
burnout and resilience in community pharmacists
during the COVID-19 pandemic: A cross-sectional
study. Saudi Pharmaceutical Journal, 30(7), 1009–
1017.
Sareen, J. (2023). Posttraumatic stress disorder in adults:
Epidemiology, pathophysiology, clinical features,
assessment, and diagnosis. In UpToDate, Post TW,
Wolters Kluwer.
Singh, M., Bharti, S., Kaur, H., Arora, V., Saini, M., Kaur,
M., & Singh, J. (2022). A Facial and Vocal Expression
Based Comprehensive Framework for Real-Time
Student Stress Monitoring in an IoT-Fog-Cloud
Environment. IEEE Access, 10, 63177–63188.
Sinval, J., Vazquez, A. C. S., Hutz, C. S., Schaufeli, W. B.,
& Silva, S. (2022). Burnout Assessment Tool (BAT):
Validity Evidence from Brazil and Portugal.
International Journal of Environmental Research and
Public Health, 19(3).
Søvold, L. E., Naslund, J. A., Kousoulis, A. A., Saxena, S.,
Qoronfleh, M. W., Grobler, C., & Münter, L. (2021).
Prioritizing the Mental Health and Well-Being of
Healthcare Workers: An Urgent Global Public Health
Priority. Frontiers in Public Health, 9, 679397.
Telles-Correia, D., Saraiva, S., & Gonçalves, J. (2018).
Mental disorder-The need for an accurate definition.
Frontiers in Psychiatry, 9(MAR).
Thorstad, R., & Wolff, P. (2019). Predicting future mental
illness from social media: A big-data approach.
Behavior Research Methods, 51(4), 1586–1600.
Vignoli, M., Muschalla, B., & Mariani, M. G. (2017).
Workplace Phobic Anxiety as a Mental Health
Phenomenon in the Job Demands-Resources Model.
BioMed Research International, 2017.
Weichel, C., Lee, J. S., & Lee, J. Y. (2021). Burnout among
Hospital Pharmacists: Prevalence, Self-Awareness, and
Preventive Programs in Pharmacy School Curricula.
Canadian Journal of Hospital Pharmacy, 74(4), 309–
316.
World Health Organization. (2022). Occupational health:
health workers.
Yang, X., McEwen, R., Ong, L. R., & Zihayat, M. (2020).
A big data analytics framework for detecting user-level
depression from social networks. International Journal
of Information Management, 54.
Yoon, J., Kang, C., Kim, S., & Han, J. (2022). D-vlog:
Multimodal Vlog Dataset for Depression Detection.
https://sites.google.com/view/jeewoo-yoon/dataset
P2DS: A Holistic Approach to Psychiatric Disease Detection in Community Pharmacies
775
