
Android App for Symptomatic Monitoring of Cervical Dystonia:
Design and Usability Study
Roland Stenger
1,∗ a
, Rica Schulze
1,∗
, Sebastian L
¨
ons
2
, Tobias B
¨
aumer
2
and Sebastian Fudickar
1 b
1
MOVE Junior Research Group, Institute of Medical Informatics, University of L
¨
ubeck, 23562 L
¨
ubeck, Germany
2
Institute for Systems Motor Science, CBBM, University of L
¨
ubeck, 23562 L
¨
ubeck, Germany
Keywords:
Smartphone App, Cervical Dystonia, Telemedicine, Asynchronous Video Recording.
Abstract:
Movement disorders are characterized by paucity or excess of movement. Access to specialists is difficult for
patients living in rural areas, making regular visits for symptom monitoring inconvenient. Asynchronous video
recording represents a telemedicine approach with temporal freedom but holds the challenge that clinicians
and patients can’t interact with each other and thus can’t correct errors, which can lead to a decrease in data
quality. This article presents an android application (Move2Screen) that aims to enable asynchronous therapy
monitoring and addresses the problem of missing interaction by an implemented video protocol for guided
recording to capture visible symptoms in the example of cervical dystonia. The videos can be accessed by
clinicians subsequent to an automated upload. A user study of the app was conducted, indicating a strong
interest and acceptance rate with a high willingness to use the app. Furthermore, the app can be used to
record a standardized data set, which allows a large number of patients to be reached without great effort by
clinicians and also provides the possibility of a semi-automated video-based analysis of current symptoms and
the longitudinal symptom progression.
1 INTRODUCTION
Movement disorders are a group of neurological
disorders, that present with involuntary movements.
They are caused by a variety of diseases, such as
Parkinson disease, Tourette syndrome, Huntington’s
disease, or dystonia. A distinction is made between
hypokinetic and hyperkinetic movement disorders.
Hypokinetic movement disorders such as Parkinson’s
disease are associated with a paucity of movement,
whereas hyperkinetic movement disorders such as
dystonia are marked by an excess of movement.
This article presents an app for therapy monitoring
through the example of cervical dystonia (the most
common form of dystonia). Dystonia is characterized
by abnormal, sustained muscle contractions that re-
sult in twisting or contorting of one or multiple joints.
It can manifest in different body areas, such as the
neck (cervical dystonia), eyelids (blepharospasm) or
the larynx (spasmodic dysphonia as a type of focal
a
https://orcid.org/0000-0002-7590-7286
b
https://orcid.org/0000-0002-3553-5131
∗
Authors contributed equally
dystonia). Dystonia can be classified into focal, seg-
mental, with tremor or generalized forms. For exam-
ple, “writer’s cramp” is focal hand dystonia, while
segmental dystonia involves two or more continu-
ous body regions. Generalized or multifocal dystonia
impacts multiple body parts simultaneously (Gerpen,
2013).
Cervical dystonia is usually diagnosed and treated
by specialists. However, access can be difficult and
costly, due to the limited number of movement dis-
order specialists, movement limitations, underserved
areas, and long travel distances (Ben-Pazi et al.,
2018)(Srinivasan et al., 2020). However, it is impor-
tant to monitor the progress of therapy regularly, as
the severity of cervical dystonia may change over time
and/or as a result of therapy. Cervical dystonia is of-
ten treated with botulinum toxin injections, where it
is common to receive such injections approximately
every 12 to 16 weeks (Ospina Medical, 2023). Con-
tinuous monitoring has potential benefits because the
effects of the injection vary from patient to patient and
side effects that may be caused by high doses can be
detected and corrected on an individual basis.
Telemedicine interventions such as (synchronous)
Stenger, R., Schulze, R., Löns, S., Bäumer, T. and Fudickar, S.
Android App for Symptomatic Monitoring of Cervical Dystonia: Design and Usability Study.
DOI: 10.5220/0012465300003657
Paper published under CC license (CC BY-NC-ND 4.0)
In Proceedings of the 17th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2024) - Volume 2, pages 201-207
ISBN: 978-989-758-688-0; ISSN: 2184-4305
Proceedings Copyright © 2024 by SCITEPRESS – Science and Technology Publications, Lda.
201

videoconferencing, which are already being increas-
ingly used (Ben-Pazi et al., 2018), may be able to
address these problems. It was found by (Hassan
et al., 2018) that 50% of Movement Disorder Soci-
ety members, mostly physicians, from 83 countries
around the world already use and plan to continue us-
ing telemedicine interventions such as videoconfer-
encing and video education in the context of move-
ment disorders. In addition, (Ben-Pazi et al., 2018)
has shown that Parkinson’s patients are satisfied with
a video consultation or even prefer it to a face-to-
face consultation. A study of telemedicine visits for
dystonia came to the same conclusions (Fraint et al.,
2020). Another study used web-based videoconfer-
encing to administer the MoCA test to subjects with
Parkinson’s and Huntington’s disease and concluded
that administration was feasible with only minor tech-
nically related problems (Abdolahi et al., 2014).
While (Ben-Pazi et al., 2018) sees synchronous
videoconferencing as an improvement, (Srinivasan
et al., 2020) points out that asynchronous methods
can overcome the problems of poor internet connec-
tions, low resolution, and possible time management
problems due to the need for scheduling. In addition,
asynchronous methods are suitable for a longer-term
exchange, because patient and doctor do not have to
make an appointment every time and are more flexible
in their time management.
However, telemedicine via asynchronous videos
also holds challenges. Information gain is not as good
with asynchronous video because clinician and pa-
tient can not interact. (Srinivasan et al., 2020) sees
the problem that, some features in dystonic disorders
can only be detected through task-specific and in site-
specific situations. Furthermore, the article empha-
sizes that the quality of telemedicine analysis may de-
pend on the correct camera angle and good lighting.
This article presents the Move2Screen app, which
aims to overcome such problems in the example of
cervical dystonia. The app allows patients to record
guided videos at home. In these videos, they per-
form specific movements following a protocol, de-
signed to enhance the detection and assessment of
dystonia-specific symptoms. Guided positioning in
front of the camera and movement instructions are
displayed through an avatar, who imitates the desired
movements. The application is asynchronous, so the
patient can record videos at any time, overcoming the
need for a face-to-face appointment. The integrating
of a video protocol that guides the patient through the
recording process, is intended to overcome the chal-
lenges that arise from the lack of interaction in asyn-
chronous recordings. The video protocol ensures that
patients perform standardized movements so that the
clinician can identify and assess symptoms and com-
pare multiple videos at the same time stamps. In ad-
dition, the app allows patients to complete a question-
naire about their general well-being. This should pro-
vide the clinician with information about the patient’s
condition and the effect of the therapy.
Following, the app is introduced in detail. First, in
Section 2.1 the requirements of the app are discussed.
Then, the framework of the app is presented in Sec-
tion 2.2. While the app is still a research prototype,
we present the results of a first user study in Section 3.
2 MATERIAL AND METHODS
2.1 Requirements of the App
Having previously discussed the advantages and dis-
advantages of telemedicine methods, we now want to
discuss the requirements for the app. Given the user
group that is to use the app and the sensitivity of the
data, we identify two particularly important require-
ments that the app must fulfill.
Ease of Use: As an asynchronous method, user-
friendliness is particularly important from the user’s
point of view, as it is not possible to respond quickly
and individually to problems and ambiguities when
using the app. Smartphone use is increasing in all
age groups. Cervical dystonia often starts between
30 and 50 years of age, whereas dystonia in cranial
regions first appears in the fifth or sixth decade of
life (Martino et al., 2012). Especially for this reason,
it is important to make the app as simple and intu-
itive as possible, so that users who have little knowl-
edge of smartphones can utilize the app without any
problems. Through the user experience study, we are
able to evaluate the simplicity of the app, which is dis-
cussed in section 3. Another related aspect regarding
ease of use is satisfaction, which is also addressed in
the usability study. According to (Liew et al., 2019)
is this based on their study the most important aspect
of health and wellness mobile apps.
Data Protection/Privacy: Person-identifying video
recordings can be considered very sensitive data, es-
pecially when the aim is to record a visible disease.
To prevent discomfort that might come from uncer-
tainty about how the data is processed and its location,
it is important to maintain transparency. Regarding
the importance of data security, (McGraw and Mandl,
2021) emphasizes that depending on health-related
data is used can yield positive or negative effects for
both individuals and entire populations. Unauthorized
HEALTHINF 2024 - 17th International Conference on Health Informatics
202
access could lead to embarrassment and discrimina-
tion. Furthermore, the article mentions transparency
as an important point to encourage people to pro-
vide personal medical data. Before each upload to
a server for clinicians to view, users should always
know which data has been uploaded and retain full
control over the uploading process. We expect that the
app will be more widely accepted if users can delete
the data as quickly and easily as possible if they wish
to do so and the data is taken with care. Therefore,
we encrypt all data before it is uploaded. The data is
stored on a password-protected server that can only
be accessed by medical professionals or those who
have the login password and private key to decrypt
the data. The study showed that the respondents were
least likely to agree with the statement that they don’t
mind using the app in social settings compared to all
other responses. This emphasizes our point about the
importance of data security.
2.2 The Framework of the App
In the following, the features of the app are intro-
duced.
General Aspects: The framework is developed with
Android Studio and is designed for smartphones with
Android 8.0 or higher. It uses standardized functional
graphical units and will be familiar to Android users,
which increases intuitive usage.
Login: On the first start, the user logs in with a QR
code, which encodes an individual user ID. The ID is
then later used to pseudonymize the data.
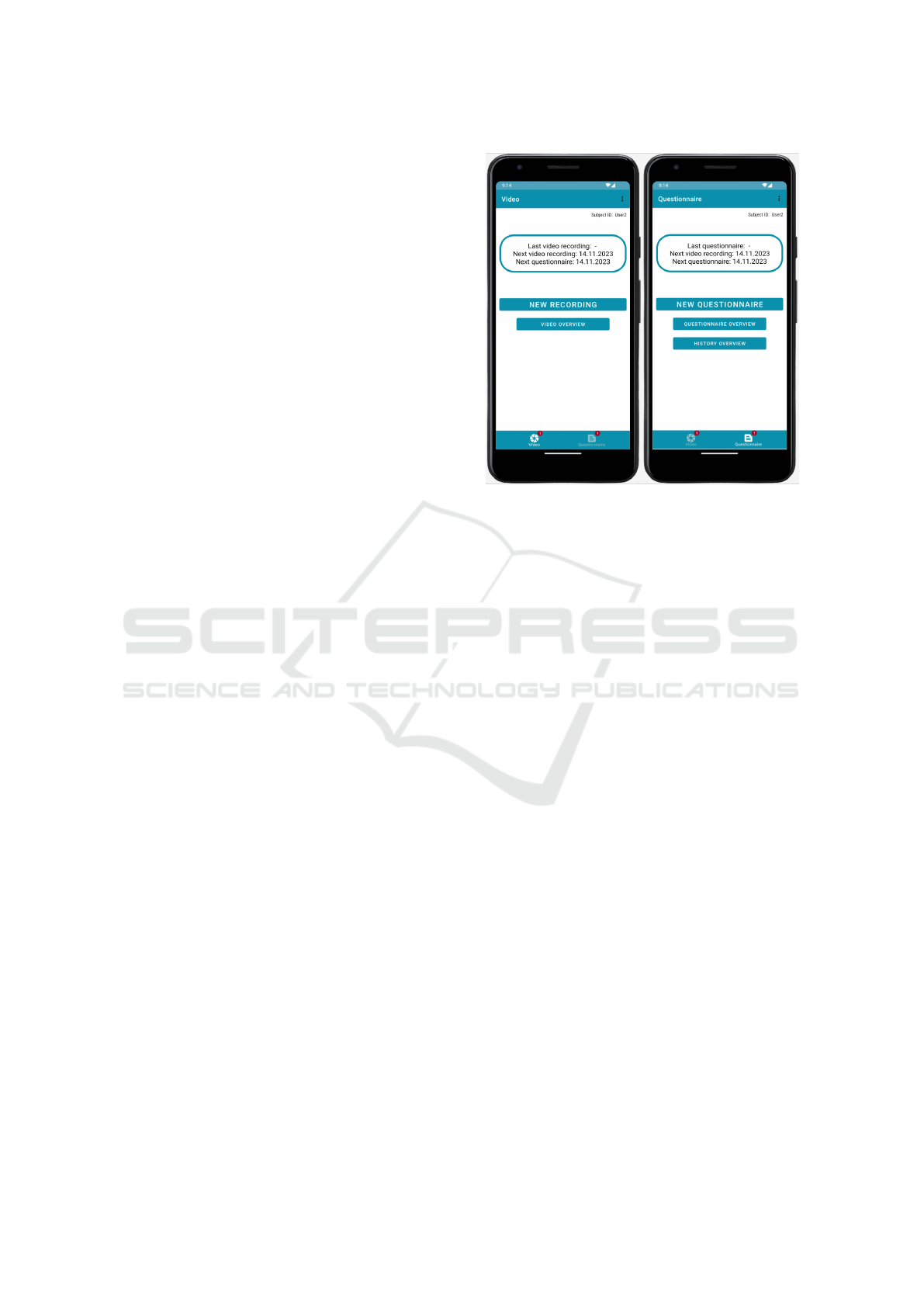
Main Page: The app implements a bottom naviga-
tion with two tiles, one for video recording, and the
other one for the questionnaire, as shown in Figure 1.
Both pages have a main button, which starts the video
recording process or the questionnaire. A bordered
window shows the date of the last data recording and
the date of the next planned recording. For fine-scale
data collection, we consider weekly collection as a
good compromise between adequacy and collection
frequency.
In order to give the user the knowledge of which
data is already recorded and if it is uploaded (con-
sidering the data protection requirement mentioned
above), the app provides on both pages, the video
recording- and questionnaire- page navigation to-
wards a history page, which list all video recordings
or questionnaires respectively. The user can delete the
data and see which data is already uploaded. If it is
already uploaded, only the local file will be deleted to
save storage space. On the same history page, the user
Figure 1: Screenshots of the main pages of the app. The
video recording page is on the left side and the question-
naire page is on the right.
is able to watch the recorded videos or all given an-
swers to the questionnaires. Both pages are directly
accessible through the main page, as visible in Fig-
ure 1 through the buttons video overview and history
overview.
Video Recording and Questionnaire: When click-
ing on the button “neue Aufnahme” (new recording),
the user is guided through a preparation page, which
can be seen in Figure 2. This includes instructions
about positioning, background, and volume control
and gives the option to look through all the follow-
ing instructions within the video protocol or watch
an example recording of such video protocol. This
feature is optional since the instructions are spoken
out by the app and tests on subjects have shown a
good intuitive understanding. As the instructions are
adapted to typical movements for assessment of the
specified disease, the patient might be familiar with
them. The second preparation page shows the cam-
era view and the user sees him/herself. A human sil-
houette is drawn as an overlay to the camera view of
the user to show the correct positioning. The user
is instructed to position the camera so that the head
and shoulders are clearly visible, as cervical dystonia
affects the muscles in the head and neck. The user
can then start the recording by clicking on a button
at the bottom of the page. The recording is stopped
automatically after the last instruction. Directly after
the protocol finishes, the user can decide if the video
should be uploaded or deleted.
Android App for Symptomatic Monitoring of Cervical Dystonia: Design and Usability Study
203

Menu Button: The menu button on the main page
provides access to the privacy policy, instructions for
use, and information about the app in general and its
goals. The privacy policy has to be accepted with the
first login to the app and contains information on how
the data is handled as well as contact information of
the responsible data protection office of the Univer-
sity of L
¨
ubeck.
Tutorial Video
Figure 2: The two preparation pages before the guided
video recording, which contain confirmation buttons for
some necessary preparations a test button for the volume
on the first page, and a camera view for positioning on the
second page.
To help with questions about using or understanding
the app, we have created a tutorial video for each as-
pect of the app. These points explain both the oper-
ation and the purpose/idea of the app. The following
individual topics are covered by tutorial videos and
can be accessed via the menu under the Instructions
for use tab.
• Idea of the app
• Start page
• Menu
• Questionnaire
• Video recording
2.3 User Experience Study
A user experience study was conducted with a total of
10 participants, five of whom had symptoms of cer-
vical dystonia. The remaining five participants had
no symptoms. The purpose of the study was to test
the acceptance and usefulness of the app. In the first
part of the study, the participants were asked to navi-
gate through the app and then,find out how to record
a video. After navigating to the video recording page,
the participants were asked to record a video accord-
ing to the implemented protocol as second part of
the study. Participants were then asked to fill out a
questionnaire about the app. The questionnaire con-
sists of an adapted version of the German mHealth
App Usability Questionnaire (G-MAUQ) (Zhou et al.,
2019)(Kopka et al., 2023), general questions about
the age, gender, and experience with smartphones,
and several free text questions aiming for the subjec-
tive impression. The questionnaire is appended. The
last two question of the G-MAUQ where discarded,
as 3 to 4 of the diseased subjects gave an answer at
all to these questions. Each item of a total of re-
maining 16 items of the G-MAUQ was evaluated on
a 7-point scale, ranging from 1 (strongly disagree) to
7 (strongly agree). The Q-MAUQ covers three sub-
scales: ease of use (5 items), interface and satisfac-
tion (7 items) and usefulness (4 items) which will be
evaluated separately.
3 STUDY RESULTS
In this section, the results of the user study are pre-
sented. In Figure 3 the answers to the G-MAUQ are
shown. The answers are sorted into the three groups
ease of use (E), interface and satisfaction (I) and use-
fulness (U). The answers are given in a range be-
tween 1 and 7, where 1 means strongly disagree and
7 strongly agree. In 75% of cases, the answers given
were 6 or 7 (agree or strongly agree), showing a high
acceptance of the app. The average value over all par-
ticipants and question groups are listed in Table 1.
Table 1: Average values of the answers to the G-MAUQ.
Group Subjects Avg. (Std) Min/Max
E
Diseased 6.27 (±1.01) 4/7
Healthy 5.64 (±0.79) 3/7
I
Diseased 6.09 (±1.16) 3/7
Healthy 5.89 (±0.92) 3/7
U
Diseased 5.7 (±1.0) 4/7
Healthy 5.95 (±0.59) 5/7
The answers to question 9 (Q9: I feel comfort-
able using this app in social settings) stand out here,
as an average value of 4.8 (±1.6) was given. This
result emphasizes that video recording of oneself, es-
pecially with the aim of recording symptoms, is an in-
HEALTHINF 2024 - 17th International Conference on Health Informatics
204
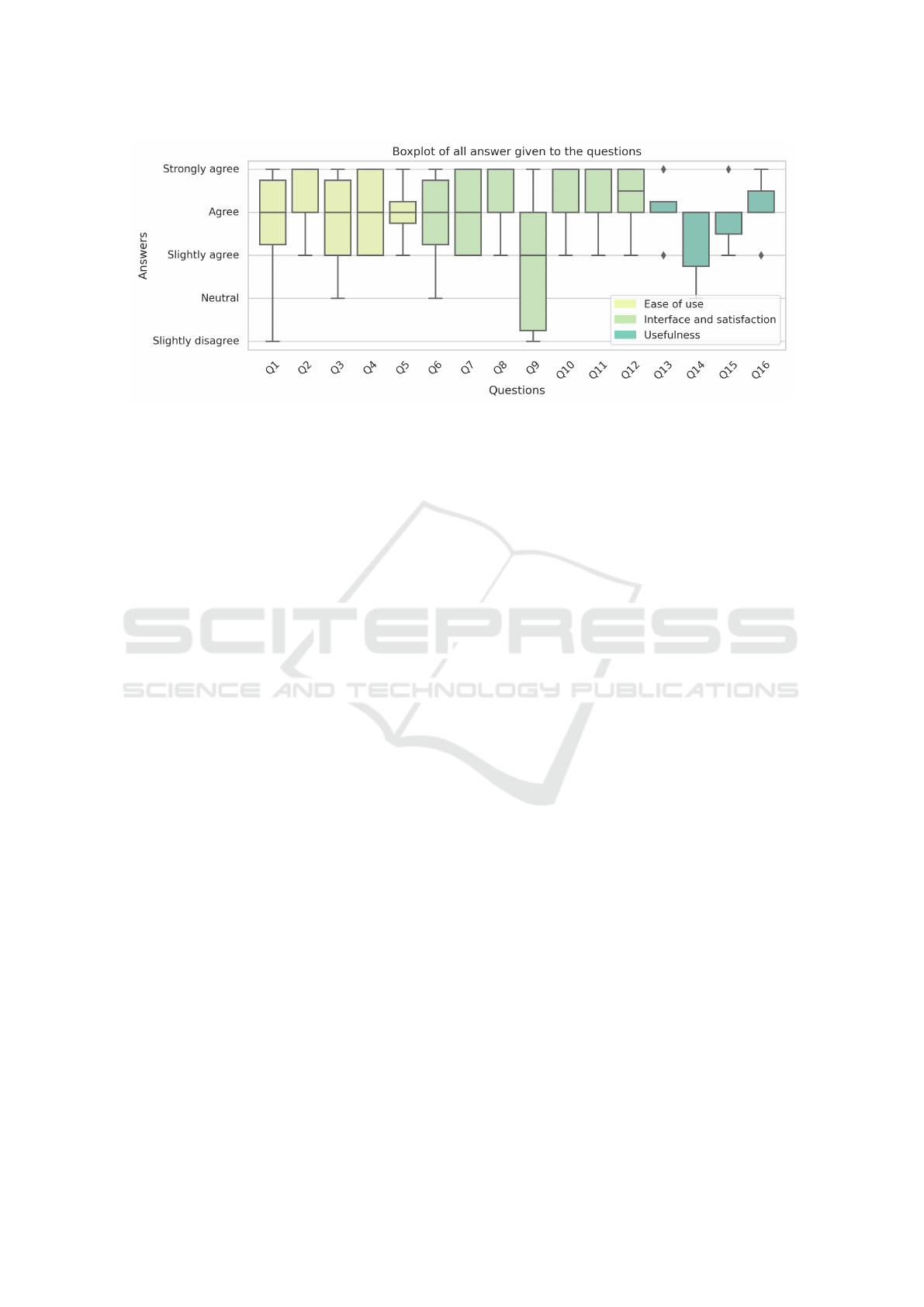
Figure 3: Boxplot of the answers to the G-MAUQ, sorted into the three groups ease of use, interface and usefulness.
timate matter. Question 14 (Q14: The app improved
my access to health care services.) was answered with
an average value of 5.4 (±0.9), and in two cases the
question was left unanswered. We assume that such
matter comes due to the fact, that the app was tested
in the setting of the study, which was not intended
to present a finished medical product, but merely to
serve as a test phase, without any advantages for the
diseased test subjects. For questions 11 to 16, at least
two and at maximum three times, an answer was not
given.
Additional to the G-MAUQ question, several text
questions were asked as well (see appendix questions
22-26) and a discussion was held on the general im-
pression of the app. Individual uncertainties regarding
operation were expressed. The steps to counter these
ambiguities are listed below, to name a few:
• The bottom navigation was colored to make it
more visible.
• Text was added under the back-arrow, to make it
more clear that it is a back button.
• One prerequisite was that the test subjects remove
their glasses in order to collect the data more uni-
formly. This requirement was discarded due to a
comment from a subject
• Within the video protocol, it was not clear in
which direction the subject should rotate as part
of the tasks. This was changed by adding a clearer
vocal instruction.
• The silhouette that is used to show the correct po-
sitioning of the camera was not in a realistic shape
of a human. This was changed to a more realistic
shape (visible in Figure 2)
4 DISCUSSION
This paper presents asynchronous therapy monitoring
app for cervical dystonia in order to create standard-
ized videos that may help clinicians to derive a quali-
tative severity score. The app is designed for the mon-
itor the progression of cervical dystonia, but it could
be adapted to other movement disorders. First results
from patients with cervical dystonia and a healthy
control group indicate a high interest in the app based
on the good results of the G-MAUQ. Good results in
the qualitative user study groups Ease of use and In-
terface and satisfaction of the G-MAUQ, which both
scored with a rating of over 6 (agree) of the dis-
eased participants, underline the user-friendliness of
the app. The question group Usefulness scored with
a rating of 5.7 (agree) of the diseased participants,
which is slightly below the global average of 5.94
(±0.96) and several questions in this group were not
answered by each subject, so the data base on which
this result is based is smaller than for the other ques-
tion group. We hypothesize that this result was in-
fluenced by the context of the study. The app was
evaluated during a test phase, not as a complete med-
ical product. Consequently, this trial phase did not
provide any direct benefit to the participants suffer-
ing from dystonia, which could then influence the per-
ceived usability.
The results of the study show the interest in the
app and the amount of participants (10 individuals
where 5 are diseased and 5 healthy) is sufficient in our
estimation, as the comments did not differ much from
each other except for some minor navigation difficul-
ties and a saturation of findings was reached¡ (Sauro
and Lewis, 2012). However, not all subjects gave an
answer to all questions, which shrinks the cohort on
some questions. The short duration of the usability
Android App for Symptomatic Monitoring of Cervical Dystonia: Design and Usability Study
205

study does not encompass the engagement and effi-
cacy when the app is used for a long period and from
home.
5 CONCLUCION
Our initial short-term usability study with a sample
size of 10 participants showed promising results in
terms of user acceptance and willingness to use the
app. However, we acknowledge the limited duration
of the individual subject tests of the app which can-
not replace a study lasting several weeks. Although
initial responses regarding usability are encouraging,
further research is needed to investigate the clinical
efficacy of the application. We aim to conduct a more
comprehensive study with a larger and more diverse
cohort to test the reliability and acceptance of the
application for independent use over a 12-week pe-
riod. This longer period will allow us to determine the
level of acceptance of the app more clearly, as it re-
quires more initiative to use independently. Subjects
must invest time on a weekly basis without receiv-
ing immediate feedback. Regarding these aspects, we
expect that some questions of the G-MAUQ will be
more meaningful in the context of the planned study.
Furthermore, the quality of the uploaded videos will
also be evaluated for their medical usefulness. The
app’s fundamental purpose is to document the pro-
gression of symptoms over several weeks. The videos
recorded in the planned study provide a data set that
allows for comparison of the same time stamps be-
tween videos of the same person over a period of
multiple weeks, enabling an accurate assessment of
symptom progression. The implemented video pro-
tocol ensures fixed time points at which the same
movement is performed. This standardized evaluation
would not be possible without such a video protocol
as it is implemented in the app
ACKNOWLEDGMENTS
The author thank all participants of the user study
for their time and effort. We acknowledge financial
support by the German Federal Ministry of Education
and Research (01ZZ2007).
REFERENCES
Abdolahi, A., Bull, M. T., Darwin, K. C., Venkatara-
man, V., Grana, M. J., Dorsey, E. R., and Biglan,
K. M. (2014). A feasibility study of conducting the
montreal cognitive assessment remotely in individuals
with movement disorders. Health Informatics Jour-
nal, 22(2):304–311.
Ben-Pazi, H., , Browne, P., Chan, P., Cubo, E., Guttman, M.,
Hassan, A., Hatcher-Martin, J., Mari, Z., Moukheiber,
E., Okubadejo, N. U., and Shalash, A. (2018). The
promise of telemedicine for movement disorders: an
interdisciplinary approach. Current Neurology and
Neuroscience Reports, 18(5).
Fraint, A., Stebbins, G. T., Pal, G., and Comella, C. L.
(2020). Reliability, feasibility and satisfaction of
telemedicine evaluations for cervical dystonia. Jour-
nal of Telemedicine and Telecare, 26(9):560–567.
Gerpen, J. A. V. (2013). Marsden's book of movement dis-
orders. Neurology, 80(24):2278–2278.
Hassan, A., Dorsey, E. R., Goetz, C. G., Bloem, B. R.,
Guttman, M., Tanner, C. M., Mari, Z., Pantelyat, A.,
Galifianakis, N. B., Bajwa, J. A., Gatto, E. M., and
Cubo, E. (2018). Telemedicine use for movement dis-
orders: A global survey. Telemedicine and e-Health,
24(12):979–992.
Kopka, M., Slagman, A., Schorr, C., Krampe, H., Al-
tendorf, M. B., Balzer, F., Bolanaki, M., Kuschick,
D., M
¨
ockel, M., Napierala, H., Scatturin, L., Schmidt,
K., Thissen, A., and Schmieding, M. (2023). Ger-
man mHealth app usability questionnaire (g-MAUQ):
Translation and validation study. Center for Open Sci-
ence.
Liew, M. S., Zhang, J., See, J., and Ong, Y. L. (2019).
Usability challenges for health and wellness mobile
apps: Mixed-methods study among mhealth experts
and consumers. JMIR MHealth UHealth, 7(1).
Martino, D., Berardelli, A., Abbruzzese, G., Bentivoglio,
A. R., Esposito, M., Fabbrini, G., Guidubaldi, A.,
Girlanda, P., Liguori, R., Marinelli, L., Morgante,
F., Santoro, L., and Defazio, G. (2012). Age at on-
set and symptom spread in primary adult-onset ble-
pharospasm and cervical dystonia: Age and spread in
primary adult-onset dystonia. Movement Disorders,
27(11):1447–1450.
McGraw, D. and Mandl, K. D. (2021). Privacy protections
to encourage use of health-relevant digital data in a
learning health system. npj Digital Medicine, 4(1).
Ospina Medical (2023). Conquering cervical dystonia:
The power of intramuscular botox injections. [2023,
April 19] https://ospinamedical.com/orthopedic-
blog/conquering-cervical-dystonia-the-power-of-
intramuscular-botox-injections.
Sauro, J. and Lewis, J. R. (2012). Chapter 2 - quantifying
user research. In Sauro, J. and Lewis, J. R., editors,
Quantifying the User Experience, pages 9–18. Mor-
gan Kaufmann, Boston.
Srinivasan, R., Ben-Pazi, H., Dekker, M., Cubo, E.,
Bloem, B., Moukheiber, E., Gonzalez-Santos, J., and
Guttman, M. (2020). Telemedicine for hyperkinetic
movement disorders. Tremor and Other Hyperkinetic
Movements, 10(0).
Zhou, L., Bao, J., Setiawan, I. M. A., Saptono, A., and
Parmanto, B. (2019). The mHealth app usability
questionnaire (MAUQ): Development and validation
study. JMIR mHealth and uHealth, 7(4):e11500.
HEALTHINF 2024 - 17th International Conference on Health Informatics
206

APPENDIX
Questionaire
The questionaire consists of the G-MAUQ and addi-
tional questions which are listed below. The MAUQ
question which we use for our study were translated
into German and validated by (Kopka et al., 2023).
Ease of Use (MAUQ)
Q1. The app was easy to use.
Q2. It was easy for me to learn to use the app.
Q3. The navigation was consistent when moving
between screens.
Q4. The interface of the app allowed me to use all the
functions (such as entering information, responding
to reminders, viewing information) offered by the
app.
Q5. Whenever I made a mistake using the app, I
could recover easily and quickly.
Interface and Satisfaction (MAUQ)
Q6. I like the interface of the app.
Q7. The information in the app was well organized,
so I could easily find the information I needed.
Q8. The app adequately acknowledged and provided
information to let me know the progress of my action.
Q9. I feel comfortable using this app in social
settings.
Q10. The amount of time involved in using this app
has been fitting for me.
Q11. I would use this app again.
Q12. Overall, I am satisfied with this app.
Usefulness (MAUQ)
Q13. The app would be useful for my health and
well-being.
Q14. The app improved my access to health care
services.
Q15. The app helped me manage my health effec-
tively.
Q16. This app has all the functions and capabilities I
expect it to have.
General Questions
Q17. Age
Q18. Gender
Q19. Do you have any experience with smartphones?
(on a scale 1-5)
Q20. How often do you use your smartphone? (less
than 1x per week, multiple times per week, daily)
Q21. What do you use your smartphone for? (phone
calls, chat/social media, gaming, streaming, internet
research, organization)
Free Text Questions
Q22. For which functions unexpected errors have
occurred?
Q23. What about the app did you not understand or
find it too complicated?
Q24. Which functions did you miss?
Q25. Which functions do you find superfluous?
Q26. Do you have any further comments or sugges-
tions for improving the app?
Android App for Symptomatic Monitoring of Cervical Dystonia: Design and Usability Study
207
