
RehabVisual: Adapting and Testing the Visuomotor Skills Stimulation
Platform on Patients with Multiple Sclerosis
Margarida Henriques
1
, Maria Irene Mendes
3
, Ana Martins
3
, Carla Quint
˜
ao
1,2 a
and Cl
´
audia Quaresma
1,2 b
1
Physics Department, NOVA School of Science and Technology – FCT NOVA, Universidade Nova de Lisboa,
2829-516 Caparica, Portugal
2
LIBPhys-UNL, Physics Department, NOVA School of Science and Technology – FCT NOVA,
Universidade Nova de Lisboa, 2829-516 Caparica, Portugal
3
Neurology Department, Hospital Garcia de Orta, 2805-267 Almada, Portugal
Keywords:
Multiple Sclerosis, Visuomotor Skills, Eye Tracker.
Abstract:
Multiple Sclerosis (MS), the most prevalent immune-mediated inflammatory demyelinating disease affecting
the Central Nervous System (CNS), has an estimated global incidence of 2,8 million individuals. Although
its symptomatology is highly varied and unpredictable, depending on the lesions’ location in the CNS, visual
impairments are among the most common manifestations. However, conventional methods for assessing and
rehabilitating visuomotor competences are not sufficient to deliver objective assessments or personalized ther-
apies. The current study addresses this gap by adapting and testing the RehabVisual platform’s usability in
MS patients. RehabVisual, developed in previous studies, aims to objectively assess visuomotor skills through
an integrated low-cost eye tracking system, offering specific clinical intervention. Before clinical application,
a normative base was established using 50 healthy individuals for later comparison. The experimental group
comprised 25 MS patients with and without confirmed visuomotor alterations. The protocol involved viewing
three visual stimuli for later calculation of the mean Euclidean distance between the gaze and stimulus posi-
tions using the eye tracker, for further assessment of the patients’ performance in tracking the stimulus. The
findings confirmed diagnosed visual impairments, along with their quantification and storage for monitoring
and rehabilitation purposes, highlighting the platform’s potential as an auxiliary tool for healthcare profession-
als.
1 INTRODUCTION
Multiple Sclerosis (MS) is the most prevalent
immune-mediated inflammatory demyelinating dis-
ease affecting the Central Nervous System (CNS),
with an estimated incidence of 2,8 million individu-
als worldwide (Walton et al., 2020).
Patients suffering from this chronic pathology
may present a variety of symptoms depending on the
location of the CNS lesions, making it difficult to
predict the disease’s course. Visual impairments are
among the most common symptoms and are often the
first manifestation of the disease, significantly alter-
ing the patients’ quality of life. However, the evalua-
tion of these competencies is typically based on the
a
https://orcid.org/0000-0003-1015-4655
b
https://orcid.org/0000-0001-9978-261X
subjective observation of the physicians, since it is
usually performed by the naked eye, resulting in over-
looked impairments (Sheehy et al., 2018).
In this sense, it is clear that the clinical practice
would benefit from the inclusion of objective and ac-
curate methods to adequately monitor the oculomo-
tor function throughout the evolution of the pathol-
ogy to avoid neglecting possible pathological alter-
ations. Previous studies have included eye tracking
systems to achieve this outcome, namely a research
carried out in 2020 (Sheehy et al., 2020), which uti-
lized a retinal eye tracking system to objectively mea-
sure fixational microsaccades (small, rapid, and subtle
eye movements that occur during fixation on a station-
ary target) in MS patients. The results indicated that
these could serve as an effective measure of disability
in MS, with a higher frequency of fixational microsac-
164
Henriques, M., Mendes, M., Martins, A., Quintão, C. and Quaresma, C.
RehabVisual: Adapting and Testing the Visuomotor Skills Stimulation Platform on Patients with Multiple Sclerosis.
DOI: 10.5220/0012463700003657
Paper published under CC license (CC BY-NC-ND 4.0)
In Proceedings of the 17th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2024) - Volume 1, pages 164-171
ISBN: 978-989-758-688-0; ISSN: 2184-4305
Proceedings Copyright © 2024 by SCITEPRESS – Science and Technology Publications, Lda.
cades associated with greater neurological disability.
Additionally, these objective methods should also
aid in the rehabilitation area, allowing the creation of
rehabilitation plans tailored to the patients’ needs, en-
suring a higher quality of life and independence in
daily tasks.
RehabVisual is a visuomotor skills stimulation
web-based platform designed both to evaluate the
oculomotor behaviour and to develop personalized in-
tervention plans. It was originally developed in a part-
nership between students and professors of biomed-
ical engineering of NOVA School of Science and
Technology, and occupational therapists and physi-
cians from the Service of Physical Medicine and Re-
habilitation of the Hospital Dona Estef
ˆ
ania (Machado
et al., 2018) to improve the methodology used in
infants with developmental abnormalities. Subse-
quently, an eye tracking system was developed to in-
tegrate the platform and objectively quantify visual
impairments (Dias et al., 2020). Currently, the plat-
form has been adapted and tested in post-stroke pa-
tients (Ferreira et al., 2020) and the eye tracker has
been improved and validated (Fonseca, 2022).
The present paper aims to describe the adaptations
made to the RehabVisual platform for its application
on individuals diagnosed with MS, along with a com-
parison between the patients and a control group of
individuals without associated pathology. The entire
process was undertaken in collaboration with the Hos-
pital Garcia de Orta (HGO), both the platform’s alter-
ations and the clinical application.
2 MATERIALS AND METHODS
The current chapter addresses the instruments used
and expanded in this work, the RehabVisual platform
and its integrated eye tracking system, in Section 2.1,
along with the data acquisition methodology in Sec-
tion 2.2.
2.1 Instruments
2.1.1 RehabVisual Platform
RehabVisual was designed using different program-
ming languages, such as HTML, PHP, JS, CSS to
create the web application, and SQL to create the
database (Machado et al., 2018). Also, it allows four
different profiles with distinct permissions within the
platform: administrator, physician/technician, occu-
pational therapist and caregiver.
The platform has two sections: assessment and
intervention. The first one consists of a database to
record all the relevant clinical information of the pa-
tient, namely their clinical record and ophthalmologi-
cal, behavioral, neuropsychological and functional as-
sessments, facilitating a long-term monitoring. The
intervention program presents a variety of protocols
with different stimuli according to the visuomotor
skills status, allowing the selection of a more adequate
set of stimuli for a specific patient.
The current study focused on the confirmation and
monitoring of diagnosed visual alterations, namely in
the functional assessment of MS patients, so the inter-
vention program was not altered nor approached.
Regarding the specificities of the studied pathol-
ogy, it was added a new database entry for the neu-
ropsychology assessment, typically carried out in MS
patients to evaluate their executive system. Also, the
functional assessment was altered to include the ex-
perimental protocol employed in the current study, ex-
plained in Section 2.2.2.
2.1.2 Eye Tracking System
The eye tracking system was created using Matlab
software and operates offline, only requiring prior
recording of the participant’s face during stimulus
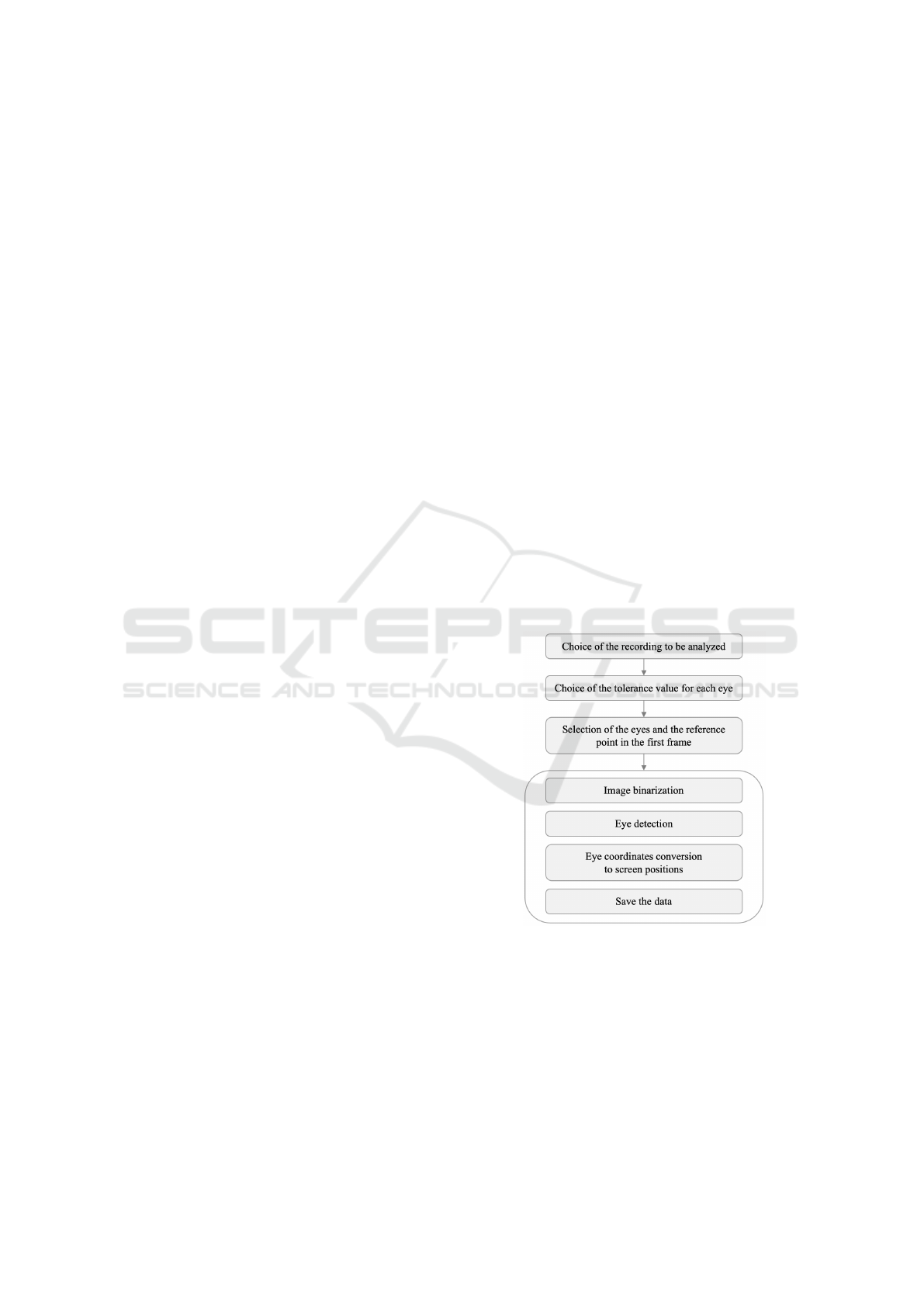
observation. Figure 1 summarizes the eye tracker’s
semi-automated workflow.
Figure 1: Eye tracking system operation summary.
The system needs a manual input of the video to
be analysed, the tolerance value for each eye, and the
position of the eyes and a reference point. These tol-
erance values are the input argument for the image
segmentation technique used in the image binariza-
tion process (performed with the Matlab command
grayconnected()). After the abovementioned steps
that require user interaction, the system automatically
analyses the whole video, processing every frame.
RehabVisual: Adapting and Testing the Visuomotor Skills Stimulation Platform on Patients with Multiple Sclerosis
165

The eye detection is obtained by the
imfindcircles() function, which finds black
circles with a radius ranging from 80% to 120% of
the first found circle’s radius. The image coordinates
of both irises and the reference point are saved in
matrices and converted into screen positions in pixels
following a calibration.
With the pixel coordinates of the subject’s gaze
and of the stimulus, it is possible to correlate these to
metrics and calculate the distance between them. The
program automatically presents the mean Euclidean
distance between the gaze and the stimulus positions
for the chosen video and respective stimulus, which
is a metric that showed a promising result in the val-
idation of this system (Fonseca, 2022). Additionally,
it also generates graphs depicting the overlay of the
stimulus positions with the gaze’s direction of each
eye (both in pixels) as a function of the video frame
number. These graphs are separated between vertical
and horizontal directions and can be used to assess a
subject’s performance in following the visual stimu-
lus presented.
2.2 Data Acquisition
Data acquisition was carried out in two separate sam-
ples, forming a control group and an experimental
group. The Ethics Committees of the HGO and the
NOVA School of Science and Technology reviewed
the present protocol and allowed its execution in their
facilities, for the construction of the experimental and
control groups, respectively.
Section 2.2.1 presents a characterization of both
groups. The experimental protocol is detailed in Sec-
tion 2.2.2.
2.2.1 Samples Characterization
Control Group. Two inclusion criteria were de-
fined for the selection of the control group: minimum
age of 18 years old and absence of known pathol-
ogy that could affect ocular movements in any way.
Additionally, all subjects were asked to remove their
glasses to prevent interference with the detection of
the eyes by the eye tracker. Nonetheless, it was en-
sured that the stimulus recognition was not affected
in order to allow an accurate stimulus tracking by the
participant.
Data collection was carried out in a sample of 50
volunteers, among whom 38 (76%) were female and
12 (24%) were male. Ages ranged from 19 to 63 years
old (mean 30,3 ± 13,3 years), while the female pop-
ulation presented a mean value of 32,7 years of age
with a standard deviation of 14,4 years and the male
cohort presented a mean value of 22,5 years of age
with a standard deviation of 1,6.
Additionally, all participants willingly agreed to
collaborate in the study, providing their free consent
before initializing any experiment.
Multiple Sclerosis Group. Regarding the experi-
mental group, the inclusion criteria defined were hav-
ing a diagnostic of MS and not having a relapse
in more than six months. Similarly to the control
group, the participants were asked to remove their
glasses due to the same reasons explained earlier. The
study population involved 25 participants, 18 females
(72%) and 7 males (28%). Ages ranged from 19 to
63 years old (mean 41,8 ± 11,7 years), with a mean
value of 41,2 years of age for the female cohort and
a standard deviation of 11,5 years, whereas the male
population had a mean value of 43,3 years of age and
a standard deviation of 12,9 years.
It was also taken into consideration the MS sub-
type of each patient and whether they had a diagnosis
of internuclear ophthalmoplegia, optic neuropathy, or
executive alterations, which are common symptoms
related to MS and may affect the patient’s perfor-
mance in following a visual stimulus. The most com-
mon subtype presented was Relapsing-remitting Mul-
tiple Sclerosis, accounting for 22 (88%) of the partic-
ipants, while the other 3 (12%) were diagnosed with
Secondary Progressive Multiple Sclerosis. Regarding
the neurological symptoms, 9 patients (36%) had al-
ready been diagnosed with internuclear ophthalmo-
plegia, 9 patients (36%) with optic neuropathy, and
12 (48%) with executive alterations.
Before initializing the experimental protocol, all
participants were fully informed about the aim of the
study and its procedures, and all provided free in-
formed consent.
2.2.2 Experimental Protocol
All participants from both groups were asked to visu-
alize three videos containing different visual stimuli
with increasing complexity, while resting their head
on a support, and an external camera recorded their
face. The subjects were instructed to follow the stim-
ulus solely with their eyes, keeping their head immo-
bile throughout the entire videos. The recording of the
participants’ face must include a clear image of their
eyes, uncovered and aligned with the screen. Fur-
thermore, the lighting conditions should be favorable,
minimizing reflections or shadows on the subjects’
ocular surfaces, and this video should be recorded at
approximately 30 frames per second, since recording
at a lower frame rate could result in the loss of rele-
vant movement information. Lastly, it is essential that
BIODEVICES 2024 - 17th International Conference on Biomedical Electronics and Devices
166

their head is rest and immobile, ensuring that the only
present movements are the eyes’.
Experimental Setup. The experimental setup is
shown in Figure 2 (on the left) and is constituted by
a laptop, a head-immobilizer, an external webcam,
and an external screen. The laptop was used to con-
trol the RehabVisual platform, while the extra moni-
tor was employed to reduce the visual clutter for the
subject, displaying only the visual stimuli intended to
be shown. Accordingly, an extra camera was neces-
sary to record the participant’s face while they visual-
ized the videos. The support, Figure 2 (on the right),
was used to immobilize the head, as the subject was
instructed to rest their chin and forehead during the
acquisition.
Figure 2: Experimental setup (on the left) and head rest (on
the right).
The monitor and the camera were positioned at
approximately 20 cm in height to align with the eye
level, and at a distance of approximately 60 cm from
the subject, allowing a comfortable viewing of the
stimuli in the participant’s field of view.
The camera used was a Logitech C920 HD PRO
Webcam, which offers a 78º field of view and a
recording resolution of 1920x1080 pixels (full HD)
at 30 frames per second, while the display (22”) pre-
sented a resolution of 1680x1050 pixels at 60 Hz. The
laptop utilized to control the stimuli, as well as record
and process the webcam data was an Acer Aspire E15.
Stimuli. Three different stimuli were elaborated in
collaboration with the Neurology Service of the HGO
and were shown during the experimental protocol.
The stimulus itself was the same, comprised by a
black circle with a red center (Figure 3, on the left),
differing only in the trajectory followed. Addition-
ally, all three videos started with a calibration se-
quence of 15 seconds, equivalent to 450 frames, cre-
ating a correspondence between the maximum and
minimum amplitude of the eyes and the screen edges.
Considering the scheme represented in Figure 3 (on
the right), the calibration procedure followed the se-
quence B-D-H-F, after an initial fixed position for 3 s
at the first location and with a fixation on each of the
marked locations of 1 s.
Figure 3: Stimulus (on the left) and possible locations of the
stimuli’s paths (on the right).
The first video has a duration of 28 s, in which
the stimulus moves to location E, where it remains
stationary for 10 s until the end, following the cali-
bration abovementioned. This stimulus was chosen to
ascertain the presence of nystagmus, by investigating
the capability of maintaining a steady gaze at a fixed
point.
The second video aimed to assess if the subject
could achieve a smooth pursuit of the stimulus, which
could translate into the presence (or absence) of sac-
cadic intrusions. Accordingly, in this 40 s video, the
stimulus describes the path E-B-H-E-D-F after the
calibration, comprising vertical and horizontal move-
ments with 1 s fixations at each marked location.
Lastly, the third video comprehends a trajectory
along the screen corners, as well as an intermittent
movement at the end, resulting in a duration of 1
minute and 40 seconds, in order to assess the subject’s
visual filed and visual perception. The initial contin-
uous movement corresponds to the path E-B-H-I-A-
G-C with a fixation of 1 s in each location following
the calibration. Subsequently, the stimulus fades and
reappears in another area, where it remains stationary
for 3 s, describing the unpredictable sequence E-A-I-
D-F-B-G-C-H.
3 RESULTS AND DISCUSSION
3.1 Control Group
After applying the experimental protocol to the con-
trol group, the mean Euclidean distance between the
stimulus and the gaze positions was calculated for the
first two videos and for each subject in order to es-
tablish a reference value for further comparison with
the experimental group. The third video was analysed
separately. Table 1 summarizes the results obtained.
RehabVisual: Adapting and Testing the Visuomotor Skills Stimulation Platform on Patients with Multiple Sclerosis
167
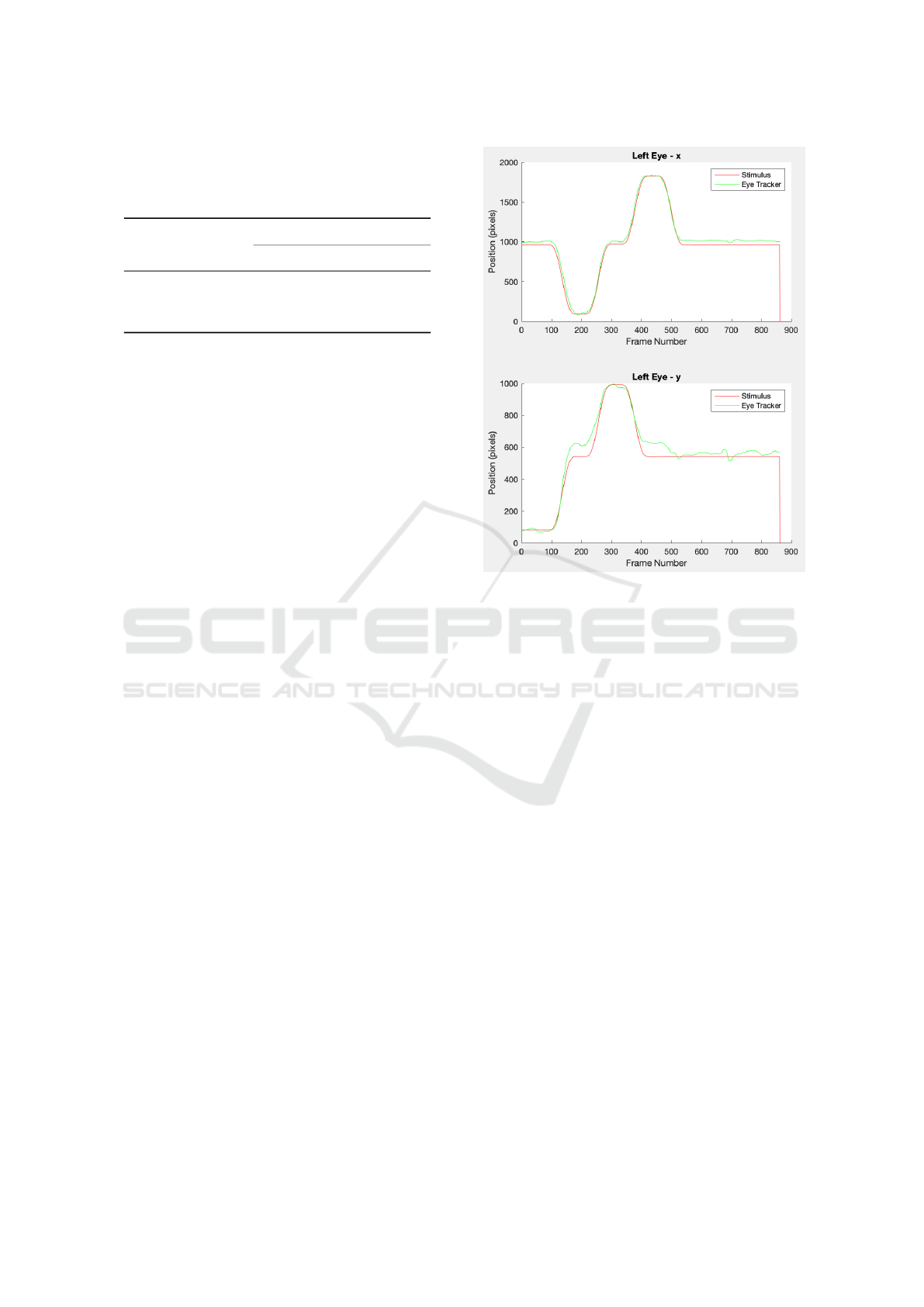
Table 1: Descriptive statistics of the mean Euclidean dis-
tance between the stimulus and the gaze positions (in pix-
els) for the first two videos and for both eyes of the control
group.
Mean Euclidean
distances (pixels)
1
st
Video 2
nd
Video
Right Left Right Left
Maximum 125 119 137 149
Minimun 49 44 53 61
Mean 84 89 109 116
As it was expected, in general the obtained val-
ues are greater for the second video. This result may
be related to the participants’ performance, as well
as to the eye detecting system. A longer video de-
mands a longer attention span and can lead to visual
fatigue, therefore resulting in a more imprecise track-
ing. On the other hand, a longer time interval implies
a higher chance of situations where the eye is not cor-
rectly detected, namely due to blinking or momentary
changes in brightness, and a higher chance of the sub-
ject moving their head. Moreover, an initial impre-
cise calibration results in more inaccurate values in a
longer video, thus leading to higher mean Euclidean
distances.
Following the same methodology of the study that
validated the eye tracking system (Fonseca, 2022), it
was established a threshold value for each stimulus
according to the approximate maximum value. There-
fore, mean Euclidean distances above 130 pixels and
150 pixels, for the first and second stimulus respec-
tively, were indicators of difficulties in tracking the
stimulus. The three figures below depict the graphs
generated by the eye tracking system for the three
stimuli of one healthy participant’s left eye.
Figure 4 shows the graphs representing the move-
ments of the first stimulus (red) and the left eye
(green) tracking it. The graphs are separated in the
two directions, horizontal (top) and vertical (bottom),
and both measure screen positions in pixels as a func-
tion of the video’s frame number. As the stimulus
remains static at the end of the video, there is a hori-
zontal line in both graphs representing the unchanged
coordinates.
Accordingly, Figure 5 depicts the graphs repre-
senting the movements of the second stimulus (red)
and the left eye (green) following it, for the horizon-
tal (top) and vertical (bottom) directions. During the
vertical movements, the graph corresponding to the
movement in the x axis shows a horizontal line, as
the stimulus does not change its x coordinate. On the
other hand, during the horizontal movements, there is
no change in the y coordinate of the stimulus, hence
the horizontal line in the graph that corresponds to the
Figure 4: Coordinates in pixels of the first stimulus (red)
and the gaze (green) as a function of the frame number for
the left eye.
movements in the vertical direction.
Lastly, the graphs in Figure 6 detail the movement
of the third stimulus (red) and of the left eye (green)
tracking it. In this case, the stimulus fades and ap-
pears in another location to produce an intermittent
movement, which is evident by the abrupt changes
in both graphs representing each direction, horizon-
tal (top) and vertical (bottom).
Analysing the generated graphs, and taking into
consideration that the graphs for the right eye are
identical, the curves representing the participant’s
gaze are noisier than the curves representing the stim-
ulus. Yet, all the transitions and fixations are correctly
identified. Another outcome is that the y coordinate
estimation of the eye movement seems less accurate
than the horizontal coordinate, for the three stimuli.
Said discrepancy might be caused by differences in
eyelid opening during vertical movements, which do
not occur during horizontal ones.
3.2 Multiple Sclerosis Group
In accordance with the previous subsection, Table 2
represents the results obtained for the experimental
group of MS patients.
Upon initial examination, we can confirm that, on
average, the values are higher for this group of indi-
BIODEVICES 2024 - 17th International Conference on Biomedical Electronics and Devices
168

Figure 5: Coordinates in pixels of the second stimulus (red)
and the gaze (green) as a function of the frame number for
the left eye.
Figure 6: Coordinates in pixels of the third stimulus (red)
and the gaze (green) as a function of the frame number for
the left eye.
viduals than for the group constituted by healthy indi-
viduals, which was undoubtedly expected since this
Table 2: Descriptive statistics of the mean Euclidean dis-
tance between the stimulus and the gaze positions (in pixels)
for the first two videos and for both eyes of the experimental
group.
Mean Euclidean
distances (pixels)
1
st
Video 2
nd
Video
Right Left Right Left
Maximum 336 346 367 457
Minimun 58 48 81 72
Mean 113 128 159 171
sample includes patients with diagnosed visual im-
pairments. Furthermore, during the acquisition, some
patients were unable to keep their head still and track
the stimulus only with eye movements, resulting in a
relatively mobile reference point and, consequently,
in disparate results. This limitation may be linked to
the presence of executive impairments, which can af-
fect, for example, the ability to maintain focus and
follow instructions.
As mentioned above, the first stimulus was used
to assess the presence of nystagmus. However, it was
not possible to draw any conclusions regarding this
visual alteration. This could be due to a low accuracy
of the eye tracker or a low incidence or intensity of
nystagmus in the patients studied. On the other hand,
it was possible to confirm the presence of abnormal
eye movements in some cases, confirming the diag-
nostic of visuomotor alterations, which can be seen in
the following figures.
Figure 7 represents the right eye movements of pa-
tient 15 while visualizing the first stimulus. This pa-
tient is a female diagnosed with Relapsing-remitting
Multiple Sclerosis and executive alterations. The
mean Euclidean distances between the stimulus and
the gaze positions were 159 ± 96 pixels for the right
eye and 134 ± 113 pixels for the left eye.
As this patient has no diagnosed visual alterations,
it was expected that the graphs would show a smooth
pursuit of the stimulus. Yet, by the presence of several
peaks, it is clear that the patient was not able to fol-
low the stimulus’s continuous movement. Also, in the
highlighted area, it is possible to see a higher slope in
the green line, suggesting that the patient anticipated
the movement and had to adjust their gaze.
Regarding the second stimulus, its aim was to
evaluate the participants’ ability to track continuous
motion. Although the first video had already provided
some information about these movements, it was pos-
sible to observe visuomotor alterations with this video
as well, as expected. Patient 5 had already been di-
agnosed with internuclear ophthalmoplegia and ex-
ecutive alterations, so the presence of abnormal eye
movements were predicted. The graphs generated by
RehabVisual: Adapting and Testing the Visuomotor Skills Stimulation Platform on Patients with Multiple Sclerosis
169
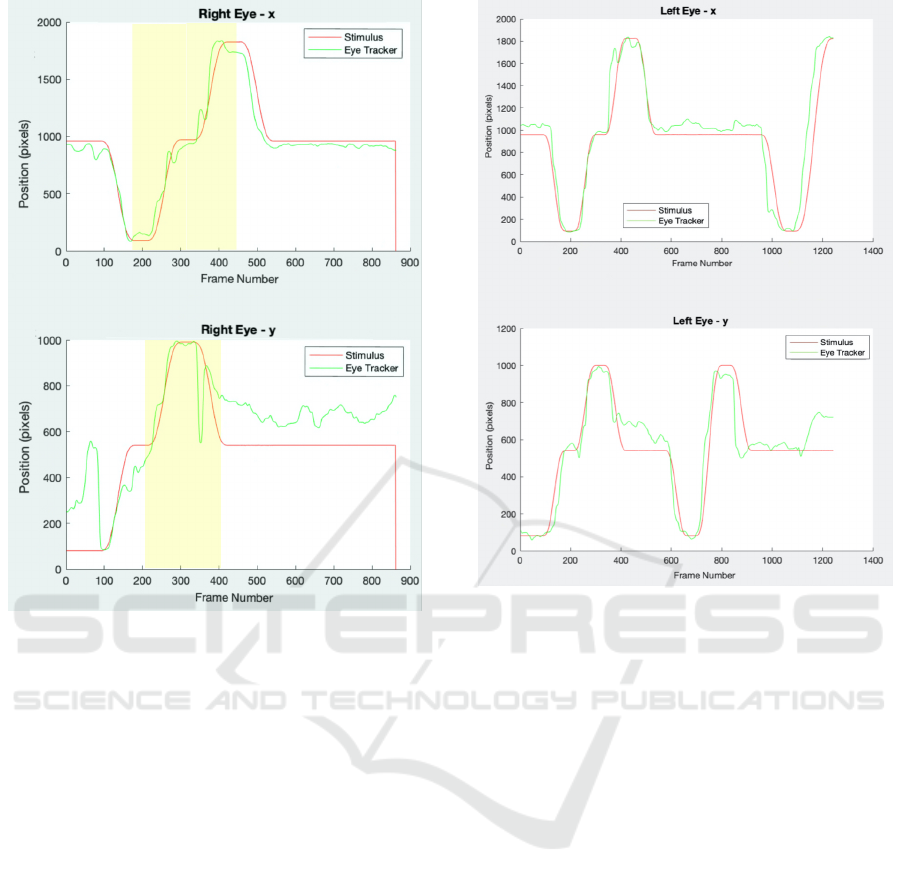
Figure 7: Coordinates in pixels of the first stimulus (red)
and the right eye’s gaze (green) of patient 15 as a function
of the frame number, with the x positions on the top and the
y positions on the bottom.
the eye tracking system corresponding to the visual-
ization of the second video by patient 5 are presented
in Figure 8. In this case, the mean Euclidean distances
between the stimulus and the left eye’s gaze positions
were 153 ± 161 pixels for the right eye and 157 ± 144
pixels for the left eye.
As can be observed, there is a peak at approxi-
mately frame 380, leading to a steeper slope of the
graph line representing the gaze position (green) com-
pared to the slope of the line representing the stim-
ulus position (red). Similarly to the first case, this
indicates that the patient anticipated the movement,
resulting in a discontinuous motion and having to
later adjust the gaze to properly follow the stimu-
lus’s movement. The same phenomenon occurs at
approximately frame 980, during a horizontal move-
ment from the middle of the screen to the left.
The third stimulus aimed to assess the patients’
field of vision, as well as their visual attention. In MS,
the visual field may be affected due to the inflamma-
tion of the optic nerve (optic neuritis). However, at
the time of the acquisition, none of the patients was in
this situation, and as a result none of them exhibited a
Figure 8: Coordinates in pixels of the second stimulus (red)
and the left eye’s gaze (green) of patient 5 as a function of
the frame number, with the x positions on the top and the y
positions on the bottom.
loss of the visual field. Therefore, no new results were
anticipated when compared to the outcomes obtained
with the two previous stimuli. This hypothesis was
corroborated, as the patients did not encounter diffi-
culties that had not already been identified with the
initial videos, nor did they experience difficulties in
locating the stimulus during intermittent movement.
However, it is important to integrate a stimulus to as-
sess these competences in future studies as well, as
they are usually affected in individuals with MS.
4 CONCLUSIONS AND FUTURE
WORK
The main objective of the present study was to expand
and adapt the RehabVisual platform to MS and test its
usability on patients diagnosed with this pathology,
following its adaptation and expansion for this popu-
lation as a continuation of previous work.
To achieve this goal, the experimental proto-
col was performed in 50 healthy volunteers (control
group) to establish normative values for further com-
parison and 25 MS patients from the HGO (exper-
BIODEVICES 2024 - 17th International Conference on Biomedical Electronics and Devices
170

imental group). Subsequently, the mean Euclidean
distances between the gaze and the stimulus positions
were calculated and it was evident that the values, in
general, were higher for the experimental group, as it
was expected.
The results obtained show that it is possible to
record and save a quantification of the visual impair-
ments, as the eye tracking system was able to con-
firm diagnosed visual alterations. This platform en-
ables an easier monitoring of the disease’s progress,
along with a possible auxiliary tool for the rehabili-
tation planning. In this sense, it is evident that MS
patients may benefit from the use of the RehabVisual
platform.
Although the results obtained are promising, there
are some limitations that were encountered and
should be addressed in future studies. Regarding the
eye tracking system itself, there were some errors
demonstrated in the eye detection, leading to inac-
curate values, thus the system’s general performance
should continue to be improved. Additionally, the
computational time needed to process the data was
greater than desired, taking approximately 5 minutes
to process a video of 29 seconds (with around 600
frames). On another note, the metric used for assess-
ment (mean Euclidean distance between the stimulus
and the gaze positions) was not always a good indica-
tor of difficulties in tracking the stimulus, since it is a
mean value. In this regard, analysing Euclidean dis-
tances in specific positions should be interesting and
could bring satisfactory results.
Also regarding future work, it is important to con-
duct a usability test in order to evaluate the platform’s
performance in the hands of healthcare professionals,
as well as to assess areas for improvement. Addition-
ally, as the present work did not focus on the reha-
bilitation area, it would be interesting to use the plat-
form to choose individualized rehabilitation programs
in future studies and test its results and relevance.
The present study offers a summary of the
methodologies and results obtained, intending to
highlight the potential of the RehabVisual platform,
as mentioned earlier. Furthermore, RehabVisual al-
lows for systematic and standardized monitoring of
patients with visuomotor impairments over time. Ad-
ditionally, it facilitates the identification the interven-
tion methodologies’ impact, allowing necessary adap-
tations to address the specific needs of each patient
when required.
ACKNOWLEDGEMENTS
Research was supported by Fundac¸
˜
ao para a
Ci
ˆ
encia e a Tecnologia through research Grants
UIDB/FIS/04559/2020 and UIDP/FIS/04559/2020
(LIBPhys).
REFERENCES
Dias, P., Ferreira, A., Vig
´
ario, R., Quaresma, C., and
Quint
˜
ao, C. (2020). Rehabvisual: Implementation of
a low cost eye tracker without pre-calibration. In Pro-
ceedings of the 13th International Joint Conference
on Biomedical Engineering Systems and Technolo-
gies (BIOSTEC 2020) - BIODEVICES, pages 235–
241. SciTePress.
Ferreira, A., Santos, P., Dias, P., Alves, A., Carmo, B., Vil-
hena, F., Costa, S., Quaresma, C., and Quint
˜
ao, C.
(2020). Rehabvisual: Application on subjects with
stroke. IFIP Advances in Information and Communi-
cation Technology, 577:355–365.
Fonseca, P. (2022). Validac¸
˜
ao da plataforma rehabvisual:
Ferramenta para estimulac¸
˜
ao das compet
ˆ
encias visuo-
motoras - aplicac¸
˜
ao a doentes com avc. Master’s the-
sis, NOVA School of Science and Technology.
Machado, R., Ferreira, A., Quint
˜
ao, C., and Quaresma, C.
(2018). Rehabvisual: Development of an applica-
tion to stimulate visuomotor skills. In Proceedings of
the 11th International Joint Conference on Biomedi-
cal Engineering Systems and Technologies (BIOSTEC
2018) - BIODEVICES, pages 173–178. SciTePress.
Sheehy, C. K., Beaudry-Richard, A., Bensinger, E., Theis,
J., and Green, A. J. (2018). Methods to assess ocular
motor dysfunction in multiple sclerosis. Journal of
Neuro-Ophthalmology, 38:488–493.
Sheehy, C. K., Bensinger, E. S., Romeo, A., Rani, L.,
Stepien-Bernabe, N., Shi, B., Helft, Z., Putnam, N.,
Cordano, C., Gelfand, J. M., Bove, R., Stevenson,
S. B., and Green, A. J. (2020). Fixational microsac-
cades: A quantitative and objective measure of dis-
ability in multiple sclerosis. Multiple Sclerosis Jour-
nal, 26(3):343–353.
Walton, C., King, R., Rechtman, L., Kaye, W., Leray, E.,
Marrie, R. A., Robertson, N., Rocca, N. L., Uitdehaag,
B., van der Mei, I., Wallin, M., Helme, A., Napier,
C. A., Rijke, N., and Baneke, P. (2020). Rising preva-
lence of multiple sclerosis worldwide: Insights from
the atlas of ms. Multiple Sclerosis Journal, 26:1816–
1821.
RehabVisual: Adapting and Testing the Visuomotor Skills Stimulation Platform on Patients with Multiple Sclerosis
171
