
Architectural Design for Enhancing Remote Patient Monitoring in
Heart Failure: A Case Study of the RETENTION Project
Ourania Manta
1a
, Nikolaos Vasileiou
1b
, Olympia Giannakopoulou
1c
, Konstantinos Bromis
1
,
Ioannis Kouris
1
, Maria Haritou
1d
, Lefteris Koumakis
2
, George Spanoudakis
2
, Irina E. Nicolae
3e
,
C. Septimiu Nechifor
3f
, Miltiadis Kokkonidis
4
, Michalis Vakalelis
4
, Yorgos Goletsis
5
,
Maria Roumpi
5
, Dimitrios I. Fotiadis
5
, Heraklis Galanis
6
, Panagiotis Dimitrakopoulos
6
,
George K. Matsopoulos
1g
and Dimitrios D. Koutsouris
1h
1
Biomedical Engineering Laboratory, Institute of Communication and Computer Systems,
National Technical University of Athens, 15773 Athens, Greece
2
Sphynx Technology Solutions AG, 6300 Zug, Switzerland
3
Configuration Technologies, Data Analytics and Artificial Intelligence, Siemens Technology, 500097, Brașov, Romania
4
AEGIS IT Research GmbH, 38106 Braunschweig, Germany
5
Biomedical Research Institute, FORTH, University of Ioannina, Ioannina, Greece
6
Datamed SA, Athens, 15124, Greece
{rmanta, nvasileiou, ogiannakopoulou, konbromis, ikouris, mhari,}@biomed.ntua.gr,
{mkokkonidis, mvakalelis}@aegisresearch.eu, goletsis@uoi.gr, mroumpi89@gmail.com, dimitris.fotiadis30@gmail.com,
{hgalanis, pdimitrakopoulos}@datamed.gr, {gmatsopoulos, dkoutsou}@biomed.ntua.gr
Keywords: Clinical Site Backend, Data Analysis, Global Insights Cloud, Heart Failure, Integration, Machine Learning,
Patient Edge, Personalised Interventions, Retention Platform, Testing.
Abstract: This paper introduces the RETENTION Platform, an integrated healthcare data management system
meticulously crafted to support personalised interventions, thereby enhancing outcomes for heart failure (HF)
patients. Comprising three fundamental components—the Global Insights Cloud (GIC), the Clinical Site
Backend (CSB), and Patient Edge (PE)—the platform coordinates a sophisticated array of functions. The GIC
facilitates data analysis and machine learning model training, while the CSB enables daily patient check-ups,
data gathering, and intervention application. The Patient Edge enables continuous monitoring and feedback
collection from patients. The system is deployed using virtual machines (VMs) and Docker containers on a
cloud-based infrastructure. Integration and testing procedures are outlined to safeguard system functionality.
This paper provides a comprehensive overview of the RETENTION Platform's architecture and highlights its
potential for improving healthcare delivery through personalised interventions.
1 INTRODUCTION
Chronic diseases are long-lasting conditions that
require ongoing medical attention and may limit daily
activities (Bernell & Howard, 2016). Heart failure
a
https://orcid.org/0000-0003-2071-1144
b
https://orcid.org/0009-0009-5486-6508
c
https://orcid.org/0000-0003-4473-2070
d
https://orcid.org/0000-0003-1136-8209
e
https://orcid.org/0000-0002-9346-8467
f
https://orcid.org/0000-0001-5727-6081
g
https://orcid.org/0000-0002-2600-9914
h
https://orcid.org/0000-0003-1205-9918
(HF) is a prevalent chronic disease and a significant
global health burden (Smith et al., 2012). HF is
characterised by symptoms and signs resulting from
cardiac abnormalities, leading to reduced cardiac
output and elevated intracardiac pressures. Despite
advancements in prevention, diagnosis, and
708
Manta, O., Vasileiou, N., Giannakopoulou, O., Bromis, K., Kouris, I., Haritou, M., Koumakis, L., Spanoudakis, G., Nicolae, I., Nechifor, C., Kokkonidis, M., Vakalelis, M., Goletsis, Y., Roumpi,
M., Fotiadis, D., Galanis, H., Dimitrakopoulos, P., Matsopoulos, G. and Koutsouris, D.
Architectural Design for Enhancing Remote Patient Monitoring in Heart Failure: A Case Study of the RETENTION Project.
DOI: 10.5220/0012458500003657
Paper published under CC license (CC BY-NC-ND 4.0)
In Proceedings of the 17th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2024) - Volume 2, pages 708-715
ISBN: 978-989-758-688-0; ISSN: 2184-4305
Proceedings Copyright © 2024 by SCITEPRESS – Science and Technology Publications, Lda.

treatment, HF remains a leading cause of disability
and premature death worldwide (The Global
Cardiovascular Disease Pandemic, Current Status and
Future Projections, 2015). It affects a substantial
portion of the population, with estimates suggesting
around 15 million Europeans and 5.8 million
Americans suffer from HF (Braunschweig et al.,
2011). The prevalence of HF is particularly high
among older individuals, reaching over 10% in those
over 70 years of age (Ponikowski et al., 2016). HF is
associated with a poor five-year survival rate
compared to other conditions like myocardial
infarction and certain cancers (Ponikowski et al.,
2016). Co-morbidities, including various diseases
and mental disorders, often accompany HF,
influencing its management and treatment
(Ponikowski et al., 2016), (Calmette & Clauser,
2018),(Reiss et al., 2018). The economic burden of
HF is substantial, with significant healthcare costs
attributed to hospitalisations and the growing elderly
population (Ayyadurai et al., 2019).
Efforts have been made to predict and prevent HF
decompensation episodes, improve medical therapy,
and introduce new devices to reduce hospitalisations
(Ayyadurai et al., 2019). Remote monitoring, such as
e-health applications, has shown promise in the
follow-up management of HF patients (Rosen et al.,
2017),(Black et al., 2014),(Koehler et al., 2018).
Technological advancements enable the collection of
patient data, including vital signs, routine ECGs, and
advanced monitoring parameters, which can aid in
disease management (Bashi et al., 2017). Evidence-
based therapies, devices, and disease management
programmes have demonstrated improved outcomes
for HF patients (Braunschweig et al., 2011).
However, despite these advancements, some
patients progress to an advanced stage of HF,
requiring mechanical support devices or heart
transplants (Calmette & Clauser, 2018),(Reiss et al.,
2018). Remote monitoring of device parameters and
patient data can help identify complications and the
need for hospital evaluation (Calmette & Clauser,
2018). Heart transplant recipients often require
multiple outpatient visits for monitoring and rejection
assessment.
In light of these challenges, the RETENTION
project aims to implement daily remote monitoring
for HF patients. The goal is to collect various clinical,
behavioural, and real-world data. The project will
analyse this data using novel data analytics and
artificial intelligence (AI) to enhance clinical
management, minimise hospitalisations, and improve
1
https://optn.transplant.hrsa.gov/data/
patient outcomes. It will also evaluate the potential of
remote monitoring, data analysis models, and clinical
interventions. This assessment will consider different
health policy perspectives, addressing patient safety,
quality of care, and the growing healthcare demand
among the ageing population with complex
conditions (Calmette & Clauser, 2018),(Reiss et al.,
2018).
2 ADVANCING HEART FAILURE
MONITORING
RETENTION strives to elevate remote patient
monitoring for heart failure by enhancing current
state-of-the-art technology across multiple
dimensions. Through advancements in these areas, it
seeks to enhance the quality of life, clinical
management, and remote monitoring of patients with
heart failure. In summary, the key contributions of
RETENTION can be outlined as follows:
2.1 Artificial Intelligence in Heart
Failure Management
Building a personalised decision support system that
can make diagnosis, prognosis, and therapy more
effective and reliable for HF patients is a complex
challenge (Mielczarek, 2016). AI techniques, such as
Bayesian networks, machine learning (ML) methods,
and supervised learning algorithms like artificial
neural networks (ANN), decision trees (DT), genetic
algorithms (GA), and Support Vector Machines
(SVM), have been utilised to develop risk
assessments and mortality predictions (Weiss et al.,
2012) using relevant medical data sources
12
. The
application of ML algorithms to individual patient
data allows for more accurate predictions and the
elimination of noisy and irrelevant features.
Furthermore, the ethical dimension of AI usage in
healthcare, as addressed in the new EU framework for
trustworthy AI, emphasises the need for lawful,
ethical, and robust decision-making processes
(Khodadadi et al., 2019). RETENTION will address
these requirements by conforming to GDPR, ensuring
privacy management, providing insights into data
analytics, and continuously evaluating security
standards and machine learning model reliability
factors.
2
https://statistics.eurotransplant.org/
Architectural Design for Enhancing Remote Patient Monitoring in Heart Failure: A Case Study of the RETENTION Project
709

2.2 Explanation and Verification in
Machine Learning
Machine learning methods, including deep learning,
have been utilised to analyse large amounts of data in
HF research (Sung et al., 2019). Interpretability and
explainability of ML models have become crucial in
validating and understanding the decisions made by
the models (Quaglini et al., 2015). Techniques for
interpreting and understanding the learned models
have been developed to shed light on complex
machine learning models (Bryan & Heagerty, 2016).
RETENTION will investigate model-agnostic
methods for interpreting ML models to enhance the
interpretability and explainability of the system.
2.3 Wearables, Smart Homes and
Internet of Things Devices in
Healthcare
Smart homes and Internet of Things (IoT) devices
have the potential to transform traditional healthcare
systems into more efficient and personalised
environments (Linkous et al., 2019). These
technologies can collect health data, provide real-time
self-monitoring and enable remote interventions by
healthcare providers. Wearable sensors, implantable
devices, and smart information platforms can
continuously monitor physiological indicators of
heart failure patients, improving comfort and
combining data from various sources (Akmandor &
Jha, 2017),(Crema et al., 2015),(Tripoliti et al., 2019).
RETENTION will leverage a wide gamut of inputs
from smart medical devices used daily by patients at
home, wearable devices, Patient Reported Outcome
Measures electronic questionnaires, and real-time
sensor measurements, coupled with state-of-the-art
ML models offering personalised predictions, to
provide a ground-breaking yet practical and patient-
friendly IT-enhanced patient monitoring framework
that aims to help doctors improve patient outcomes
and minimise emergency room visits and
hospitalisations, contributing to the effective and
efficient management of HF patients.
2.4 Big Data Management and
Analytics
Big data analytics (BDA) platforms have evolved to
address the challenges of complex correlations of
heterogeneous, open, public, and private big data in a
cost-effective, safe, and user-friendly manner
(Assunção et al., 2015). RETENTION will adopt a
model-driven approach to designing and
implementing big data infrastructures, aiming for
modularity, reusability, and automation.
Interpretability and explainability of data analytics
will be crucial in validating the results and ensuring
evidence-based interventions (Sparks et al., n.d.),(Du
et al., 2018).
2.5 Personalised Human-Computer
Interactions
Human-Computer Interaction (HCI) plays a vital role
in delivering digital technologies to the healthcare
sector (Blandford, 2019). User needs and usability
factors, such as health literacy, age-related
conditions, and the visualisation of complex health
data, need to be considered in the design of user
interfaces (Patel et al., 2015),(Groenvold et al., 2006).
RETENTION will adopt a user-centric approach,
involve users in the iterative design process, and
develop adaptive visualisations and interfaces for
healthcare practitioners and patients.
2.6 Security, Privacy, and Trust in
Healthcare and IoT Systems
IoT applications in healthcare face security and
privacy challenges, including mutual authentication,
encryption, and data integrity (Salah & Khan, 2017).
Cryptographic techniques, such as privacy-
preserving encryption and differential privacy, have
been proposed to preserve data confidentiality. Proper
identity and authorisation management, along with
access control policies, are essential for protecting
user privacy (Hassija et al., 2019), (Li et al., 2018).
RETENTION will combine novel and standardised
technologies to provide lightweight and usable
mechanisms for authentication, authorisation, privacy
preservation, and secure communications.
Continuous security and privacy assurance will be
ensured through monitoring and evaluation tools (Li
et al., 2018).
3 ARCHITECTURAL DESIGN OF
THE RETENTION PLATFORM
3.1 RETENTION Project Overview
The architectural design of the RETENTION project
follows a comprehensive approach aimed at
enhancing remote patient monitoring in heart failure.
To summarise, the primary objective of the
HEALTHINF 2024 - 17th International Conference on Health Informatics
710
RETENTION initiative is to develop and implement
a groundbreaking platform that facilitates advanced
clinical monitoring and interventions with the aim of
enhancing the management of patients suffering from
chronic HF. This entails reducing mortality and
hospitalisation rates while concurrently improving
their overall quality of life, safety, and well-being.
The RETENTION platform will effectively aid
clinical decision-making and provide evidence-based
personalised interventions for HF patients by
employing the following methods:
Continuously monitoring and aggregating an
extensive range of medical, clinical,
physiological, behavioural, psychosocial,
and real-world data pertinent to HF patients;
Utilising cutting-edge model-driven big data
analytics, statistical analysis, artificial
intelligence, and machine learning
techniques to analyse these data;
Identifying patterns in the progression of HF
and evaluating the patients' quality of life
through a thorough examination of the
collected data;
Thoroughly cross-referencing and validating
these findings against existing clinical
literature; and
Fostering transparent, comprehensible, and
verifiable decision-making capabilities that
leverage the evidence generated by the
underlying data analysis, thereby bolstering
clinical studies targeting HF and other
cardiovascular diseases.
The RETENTION approach and its platform will
be validated through a clinical study involving 450
HF patients recruited by six different hospitals in four
different EU countries, within which there is some
diversity in the management of such patients.
3.2 RETENTION Conceptual and
System Architecture
The purpose of the system architecture activities was
to define a coherent, comprehensive solution to the
RETENTION platform based on principles, concepts,
and properties that are related and functional to each
other in a logical way. In this section, a detailed
description of the architecture of the RETENTION
system is provided, outlining the conceptual model
and descriptions of the main components that
constitute it. The RETENTION platform is
architected with privacy considerations in mind and
avoids unnecessary concentration of patients’
personal data on, say, a cloud infrastructure beyond
the patient’s or hospital's control. But at the same
time, it allows ML model training across the data
collected from multiple hospitals’ patients. It does so
through a carefully designed architecture that pays
particular attention to privacy protection while
allowing direct access to the medically relevant
patient data collected from the clinical sites, as
enhanced through RETENTION’s enhanced patient
monitoring outside the hospital. It is expected that the
RETENTION Platform will attain a level of human-
machine interaction of the highest standards to enable
user-friendly interactions for handling the complexity
of workflows and their outputs, coping with the
output of complex models, the verification of those
via the visualisation of the knowledge encoded, and
the presentation of interventions.
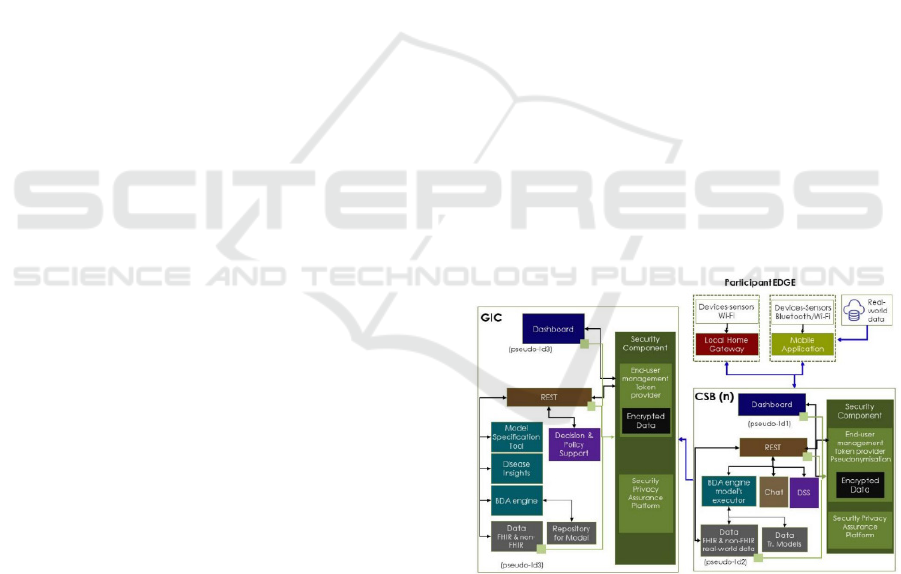
The following figure illustrates all the high-level
components of the system. Components are mainly
interconnected via REST API interfaces to facilitate
integration. As can be seen, the architecture is based
on a 3-layer model (arising from a structured IoT
architecture, modified for the RETENTION project):
the Global Insights Cloud (GIC);
the Clinical Site Backend (CSB); and
the Patient Edge (PE)
These layers interact to facilitate data collection,
analysis, and personalised interventions. The diagram
featured in Figure 1 provides a comprehensive
depiction of the RETENTION architecture,
illustrating the various actors that operate within each
respective layer.
Figure 1: RETENTION Architecture: (Global Insights
Cloud (GIC), Clinical Site Backend (CSB), and Patient
Edge (PE).
The Global Insights Cloud (GIC) serves as the
central repository for big data analytics. The GIC
layer encompasses several sub-components,
including the GIC Dashboard, Federated RW Data
Repository and Repository for Models, BDA Engine,
Model Specification Tool, Disease Insights, Decision
and Policy Support, Security Component, and GIC
Architectural Design for Enhancing Remote Patient Monitoring in Heart Failure: A Case Study of the RETENTION Project
711
Rest API. It collects anonymised patient data from all
sites, enabling global data analytics and insight
generation. The GIC hosts the analytics engine and
provides tools for data scientists, clinical experts, and
healthcare policymakers to make informed decisions
about HF disease management. Additionally, the GIC
supports incremental data analysis and model
refinement, ensuring evidence-based interventions.
The Clinical Site Backend (CSB) operates at each
clinical site and is responsible for patient data
management and local analytics. It comprises sub-
components such as the CSB Dashboard, FHIR
3
(Fast
Healthcare Interoperability Resources) and Non-
FHIR Repository, BDA Engine Models Executor,
Decision Support System (DSS), Security
Component, and CSB Rest API. It allows clinicians
to monitor their patients, gather medical and usage
data, and make informed decisions. The CSB
facilitates the execution of personalised interventions
based on trained machine learning models. It also
ensures pseudonymisation of patient data. This
protects privacy while granting clinicians access to
pertinent information.
The Patient Edge (PE) encompasses a mobile
application and a home gateway. It enables
continuous monitoring of patients and the collection
of real-world data. The mobile application serves as
an interface for patients to report symptoms, record
adherence to medication regimes, and report health
metrics in a user-friendly, semi-automated manner. It
collects and aggregates data from the patient’s
smartwatch and smart medical devices (blood
pressure metre, oximetre, weigh scales) that the
patient uses on a daily basis, transmitting it to the
CSB of the hospital monitoring the patient’s health.
The home gateway also contributes by aggregating
and transmitting to the CSB data from sensors in the
patient's indoor home environment, as well as
relevant weather open data capturing the external
environmental conditions of the patient’s home.
For the storage of medical data, a FHIR database
was utilised. Healthcare terminologies and coding
systems like SNOMED CT, LOINC, and ICD-10
were integrated into the FHIR standard to provide
standardised codes and terminologies for
representing clinical concepts, laboratory
observations, and disease classifications, enhancing
interoperability and allowing for consistent and
meaningful exchange of healthcare information
across different systems and applications that adhere
to the FHIR standard.
3
https://ecqi.healthit.gov/fhir
Security and privacy are paramount in the
RETENTION architecture. The Security Component
of the RETENTION project is responsible for
authentication, authorisation, and data protection
during transit and storage. This component plays a
pivotal role in ensuring the secure management of
personal data in compliance with GDPR regulations.
It facilitates secure data handling, distribution, and
presentation to authorised users while safeguarding
data privacy. This component is present in both the
GIC and CSB instances and encompasses various
mechanisms, including API management, role-based
access control (RBAC), data encryption, API logs,
device management, and RETENTION
pseudonymisation. API management ensures data
security and protection for exposed APIs, while
RBAC restricts access to authorised roles and
registered end-users. Data encryption safeguards
personal and identifiable information. API logs
monitor activity for potential security threats, and
device management allows efficient technical support
without compromising sensitive identification. The
Security Component employs pseudonymisation as a
measure of minimising the risk of data subjects’
identification. Data residing in GIC is anonymised.
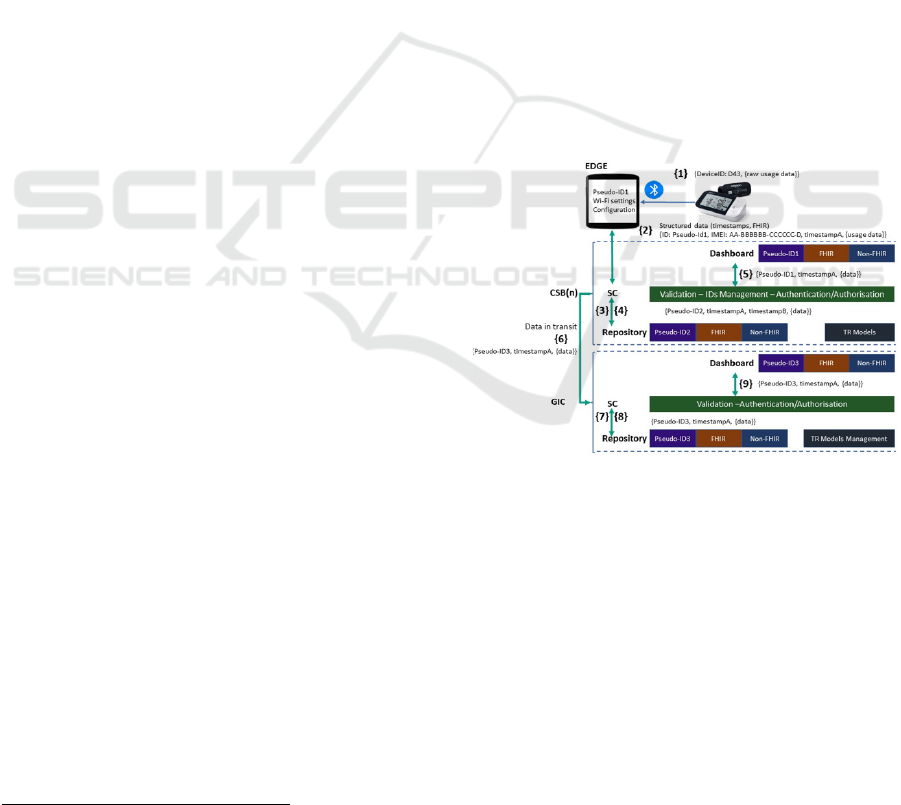
Figure 2: Transmission of data between PE, CSB and GIC.
Overall, the RETENTION system architecture
will facilitate data-driven decision-making,
personalised interventions, and secure data
management. It supports multiple user roles,
including system administrators, clinicians, patients,
data scientists, and healthcare policymakers. By
leveraging the capabilities of the GIC, CSB, and PE,
the architecture will enable comprehensive
monitoring and management of patients with heart
failure, ultimately improving their clinical outcomes.
HEALTHINF 2024 - 17th International Conference on Health Informatics
712

3.3 Integration and Testing of the
RETENTION System
The integration and testing phases of the
RETENTION system were crucial for its successful
development and completion. These phases involved
the installation of the main components, the
confirmation of software quality, and ensuring the
functionality and performance of the system.
Software quality assurance included creating
scenarios, entering test data, and controlling
procedures to confirm the "quality" of the software
product. The integration process followed a staged
approach, which started with the installation and
customisation of software components. Docker
containers were used for deploying system
components (dashboard, security component, DSS,
data repositories) and integrating modules such as GIC,
CSB, and PE.
Testing encompassed various stages, including unit
tests, application tests, integration tests, system tests,
and user acceptance tests. Unit testing verified the
individual subsystems, while application testing
focused on checking the business logic. Integration
testing ensured successful communication and system
reliability. System testing guaranteed that the system
met operational requirements. User acceptance tests
validated system functionality and performance.
During the deployment phase, two distinct stages
will be undertaken. The first stage will involve data
collection, allowing AI models to be trained. In the
second stage, the system will be fully available to
support clinical teams and their respective patients.
Deployment will guarantee the availability,
security, and operational support of the RETENTION
system. It will adhere to GDPR regulations to ensure
the protection of sensitive data. The integration and
testing phases ensure the functionality, reliability, and
readiness of the RETENTION system for real-world
implementation.
4 DISCUSSION
The RETENTION platform presents a significant
advancement in the field of HF management through
enhanced remote patient monitoring. The discussion
section below elaborates on several key points and
implications arising from the architectural design and
conceptual framework of the RETENTION project.
The core objective of the RETENTION initiative
is to significantly improve HF management by
reducing mortality and hospitalisation rates while
simultaneously enhancing the overall quality of life
for HF patients. Through continuous data collection,
state-of-the-art data analytics, and machine learning,
the platform aims to provide personalised
interventions based on robust evidence. This
approach has the potential to revolutionise the way
HF is managed and significantly impact patient
outcomes. By leveraging a structured IoT
architecture, the RETENTION platform sets a new
standard for patient monitoring in chronic diseases.
The use of big data analytics and artificial
intelligence in HF management is pivotal. Machine
learning models, including Bayesian networks, ANN,
and SVM, hold promise for improving risk
assessments and mortality predictions. However,
these models must meet ethical standards and data
protection regulations, as emphasised by GDPR. The
RETENTION project's commitment to lawful,
ethical, and robust decision-making processes is
essential for ensuring the platform's trustworthiness
and compliance.
The importance of interpretability and
explainability in machine learning models cannot be
overstated. The RETENTION project's exploration of
model-agnostic methods for interpreting ML models
represents a significant step towards ensuring
transparency in decision-making. This approach
aligns with the broader trend in healthcare AI, where
the ability to understand and validate model decisions
is critical.
The integration of IoT devices into healthcare
holds enormous potential. These technologies can
provide real-time monitoring and personalised
interventions, transforming traditional healthcare into
a more efficient and patient-centric environment.
RETENTION's use of real-time sensor measurements
and personalised treatment exemplifies this potential,
enhancing the management of HF patients and
potentially extending to other chronic diseases.
Security and privacy are paramount in healthcare
systems, especially when IoT applications are
involved. The RETENTION project's approach to
security, including privacy-preserving encryption and
access control policies, addresses these challenges
comprehensively. Ensuring the protection of user
privacy while facilitating secure data exchanges is
vital for the success of any healthcare platform.
The user-centric design approach adopted by the
RETENTION project acknowledges the importance
of considering user needs and usability factors. This
perspective is particularly relevant in healthcare,
where various user groups, including patients,
clinicians, and data scientists, interact with the
system. The emphasis on adaptive visualisations and
Architectural Design for Enhancing Remote Patient Monitoring in Heart Failure: A Case Study of the RETENTION Project
713

interfaces aligns with the broader trend of making
healthcare technologies accessible to a wide range of
users.
The RETENTION project's commitment to
validation through a clinical study involving at least
450 HF patients across multiple EU countries is a
crucial step. It ensures that the platform's benefits and
effectiveness are rigorously evaluated in a real-world
context with diverse patient populations and clinical
settings.
In conclusion, the RETENTION platform
represents a significant advancement in HF
management by leveraging cutting-edge technologies
and a comprehensive approach. By addressing
challenges related to data analytics, explainability, IoT,
security, and user-centric design, the project paves the
way for more effective, personalised, and secure
healthcare solutions. The clinical study will provide
valuable insights into the platform's real-world impact
and its potential for broader applications in healthcare
data management and personalised interventions.
5 CONCLUSIONS
Overall, this paper provides a comprehensive
understanding of the RETENTION system, focusing
on its technical aspects and the modules comprising
it. Specifically, the architecture for the RETENTION
Platform is presented, which encompasses the Global
Insights Cloud (GIC), Clinical Site Backend (CSB),
and Patient Edge (PE) components. The GIC serves
as the hub for data analysis and ML model training,
providing evidence-based personalised interventions.
The CSB supports daily patient check-ups, data
gathering, and the application of ML models for
interventions. The PE enables continuous patient
monitoring and feedback collection. The
infrastructure supporting the RETENTION system is
based on virtual machines (VMs) and Docker
containers, with a cloud-based deployment.
Integration and testing procedures were crucial to
ensuring the system's functionality and performance.
The presented reference architecture lays the
foundation for further development and
implementation of the system to improve healthcare
data management and personalised interventions.
ACKNOWLEDGEMENTS
The RETENTION project was financed by the
European Union’s Horizon 2020 Research and
Innovation Programme, Grant Agreement Number
965343.
REFERENCES
Akmandor, A. O., & Jha, N. K. (2017). Keep the Stress
Away with SoDA: Stress Detection and Alleviation
System. IEEE Transactions on Multi-Scale Computing
Systems, 3(4), 269–282. https://doi.org/10.1109/TMSC
S.2017.2703613
Assunção, M. D., Calheiros, R. N., Bianchi, S., Netto, M.
A. S., & Buyya, R. (2015). Big Data computing and
clouds: Trends and future directions. Journal of
Parallel and Distributed Computing, 79–80, 3–15.
https://doi.org/10.1016/j.jpdc.2014.08.003
Ayyadurai, P., Alkhawam, H., Saad, M., Al-Sadawi, M. A.,
Shah, N. N., Kosmas, C. E., & Vittorio, T. J. (2019). An
update on the CardioMEMS pulmonary artery pressure
sensor. In Therapeutic Advances in Cardiovascular
Disease (Vol. 13). SAGE Publications Ltd.
https://doi.org/10.1177/1753944719826826
Bashi, N., Karunanithi, M., Fatehi, F., Ding, H., & Walters,
D. (2017). Remote Monitoring of Patients With Heart
Failure: An Overview of Systematic Reviews. Journal
of Medical Internet Research, 19(1).
Bernell, S., & Howard, S. W. (2016). Use Your Words
Carefully: What Is a Chronic Disease? Frontiers in
Public Health, 4. https://doi.org/10.3389/fpubh.2016.0
0159
Black, J. T., Romano, P. S., Sadeghi, B., Auerbach, A. D.,
Ganiats, T. G., Greenfield, S., Kaplan, S. H., & Ong, M.
K. (2014). A remote monitoring and telephone nurse
coaching intervention to reduce readmissions among
patients with heart failure: Study protocol for the Better
Effectiveness After Transition - Heart Failure (BEAT-
HF) randomized controlled trial. Trials, 15(1).
https://doi.org/10.1186/1745-6215-15-124
Blandford, A. (2019). HCI for health and wellbeing:
Challenges and opportunities. International Journal of
Human Computer Studies, 131, 41–51. https://doi.org/
10.1016/j.ijhcs.2019.06.007
Braunschweig, F., Cowie, M. R., & Auricchio, A. (2011).
What are the costs of heart failure? Europace,
13(SUPPL. 2). https://doi.org/10.1093/europace/eur081
Bryan, M., & Heagerty, P. J. (2016). Multivariate Analysis
of Longitudinal Rates of Change. PubMed Central,
35(28).
Calmette, L., & Clauser, S. (2018). Von Willebrand
disease. In Revue de Medecine Interne (Vol. 39, Issue
12, pp. 918–924). Elsevier Masson SAS. https://
doi.org/10.1016/j.revmed.2018.08.005
Crema, C., Depari, A., Flammini, A., Lavarini, M., Sisinni,
E., & Vezzoli, A. (2015). A smartphone-enhanced pill-
dispenser providing patient identification and in-take
recognition. 2015 IEEE International Symposium on
Medical Measurements and Applications, MeMeA 2015
- Proceedings, 484–489. https://doi.org/10.1109/MeMe
A.2015.7145252
HEALTHINF 2024 - 17th International Conference on Health Informatics
714

Du, M., Liu, N., & Hu, X. (2018). Techniques for
Interpretable Machine Learning. http://arxiv.org/abs/
1808.00033
Groenvold, M., Petersen, M. A., Aaronson, N. K., Arraras,
J. I., Blazeby, J. M., Bottomley, A., Fayers, P. M., de
Graeff, A., Hammerlid, E., Kaasa, S., Sprangers, M. A.
G., & Bjorner, J. B. (2006). Letter to the Editor.
Palliative Medicine, 20(2), 59–61. https://doi.org/10.11
91/0269216306pm1133xx
Hassija, V., Chamola, V., Saxena, V., Jain, D., Goyal, P., &
Sikdar, B. (2019). A Survey on IoT Security:
Application Areas, Security Threats, and Solution
Architectures. In IEEE Access (Vol. 7, pp. 82721–
82743). Institute of Electrical and Electronics
Engineers Inc. https://doi.org/10.1109/ACCESS.20
19.2924045
Khodadadi, M., Shayanfar, H., Maghooli, K., & Mazinan,
A. H. (2019). Fuzzy cognitive map based approach for
determining the risk of ischemic stroke. IET Systems
Biology, 13(6), 297–304. https://doi.org/10.1049/iet-
syb.2018.5128
Koehler, F., Koehler, K., Deckwart, O., Prescher, S.,
Wegscheider, K., Kirwan, B. A., Winkler, S.,
Vettorazzi, E., Bruch, L., Oeff, M., Zugck, C., Doerr,
G., Naegele, H., Störk, S., Butter, C., Sechtem, U.,
Angermann, C., Gola, G., Prondzinsky, R., … Stangl,
K. (2018). Efficacy of telemedical interventional
management in patients with heart failure (TIM-HF2):
a randomised, controlled, parallel-group, unmasked
trial. The Lancet, 392(10152), 1047–1057. https://
doi.org/10.1016/S0140-6736(18)31880-4
Li, J., Zhang, Y., Chen, X., & Xiang, Y. (2018). Secure
attribute-based data sharing for resource-limited users
in cloud computing. Computers and Security, 72, 1–12.
https://doi.org/10.1016/j.cose.2017.08.007
Linkous, L., Zohrabi, N., & Abdelwahed, S. (2019). Health
Monitoring in Smart Homes Utilizing Internet of
Things. Proceedings - 4th IEEE/ACM Conference on
Connected Health: Applications, Systems and
Engineering Technologies, CHASE 2019, 29–34.
https://doi.org/10.1109/CHASE48038.2019.00020
Mielczarek, B. (2016). Review of Modelling Approaches
For Healthcare Simulation. Operations Research and
Decisions, 26(1), 55–72.
Patel, V., Kannampallil, T., & Kaufman Editors, D. (2015).
Health Informatics Human Computer Interaction in
Healthcare. http://www.springer.com/series/1114
Ponikowski, P., Voors, A. A., Anker, S. D., Bueno, H.,
Cleland, J. G. F., Coats, A. J. S., Falk, V., González-
Juanatey, J. R., Harjola, V. P., Jankowska, E. A.,
Jessup, M., Linde, C., Nihoyannopoulos, P., Parissis, J.
T., Pieske, B., Riley, J. P., Rosano, G. M. C., Ruilope,
L. M., Ruschitzka, F., … Davies, C. (2016). 2016 ESC
Guidelines for the diagnosis and treatment of acute and
chronic heart failure. In European Heart Journal (Vol.
37, Issue 27, pp. 2129-2200m). Oxford University
Press. https://doi.org/10.1093/eurheartj/ehw128
Quaglini, S., Sacchi, L., Lanzola, G., & Viani, N. (2015).
Personalization and Patient Involvement in Decision
Support Systems: Current Trends. In
Yearbook of
medical informatics (Vol. 10, Issue 1, pp. 106–118).
https://doi.org/10.15265/IY-2015-015
Reiss, N., Schmidt, T., Boeckelmann, M., Schulte-Eistrup,
S., Hoffmann, J.-D., Feldmann, C., & Schmitto, J. D.
(2018). Telemonitoring of left-ventricular assist device
patients-current status and future challenges. Journal of
Thoracic Disease, 10(15).
Rosen, D., McCall, J. D., & Primack, B. A. (2017).
Telehealth Protocol to Prevent Readmission Among
High-Risk Patients With Congestive Heart Failure. The
American Journal of Medicine, 130(11), 1326–1330.
Salah, K., & Khan, M. (2017). IoT Security: Review,
Blockchain Solutions, and Open Challenges. Future
Generation Computer Systems.
Smith, S. C., Collins, A., Ferrari, R., Holmes, D. R.,
Logstrup, S., McGhie, D. V., Ralston, J., Sacco, R. L.,
Stam, H., Taubert, K., Wood, D. A., & Zoghbi, W. A.
(2012). Our time: A call to save preventable death from
cardiovascular disease (heart disease and stroke).
Journal of the American College of Cardiology, 60(22),
2343–2348. https://doi.org/10.1016/j.jacc.2012.08.962
Sparks, E. R., Venkataraman, S., Kaftan, T., Franklin, M.
J., & Recht, B. (n.d.). KeystoneML: Optimizing
Pipelines for Large-Scale Advanced Analytics.
http://www.keystone-ml.org/
Sung, J. M., Cho, I.-J., Sung, D., Kim, S., Kim, H. C., Chae,
M.-H., Kavousi, M., Rueda-Ochoa, O. L., Ikram, M. A.,
Franco, O. H., & Chang, H.-J. (2019). Development
and verification of prediction models for preventing
cardiovascular diseases. PLOS ONE.
The global cardiovascular disease pandemic, current status
and future projections. (2015).
Tripoliti, E. E., Karanasiou, G. S., Kalatzis, F. G.,
Bechlioulis, A., Goletsis, Y., Naka, K., & Fotiadis, D.
I. (2019). HEARTEN KMS – A knowledge
management system targeting the management of
patients with heart failure. Journal of Biomedical
Informatics, 94. https://doi.org/10.1016/j.jbi.2019.10
3203
Weiss, E. S., Allen, J. G., Kilic, A., Russell, S. D.,
Baumgartner, W. A., Conte, J. V., & Shah, A. S. (2012).
Development of a quantitative donor risk index to
predict short-term mortality in orthotopic heart
transplantation. Journal of Heart and Lung
Transplantation, 31(3), 266–273. https://doi.org/10.10
16/j.healun.2011.10.004
Architectural Design for Enhancing Remote Patient Monitoring in Heart Failure: A Case Study of the RETENTION Project
715
