
A Hierarchical Framework for Apnea Detection and Respiration Pace
Assessment Using Seismocardiogram Signals
Berke Kizir and Beren Semiz
a
Department of Electrical and Electronics Engineering, Koc University, Istanbul, Turkey
Keywords:
Seismocardiogram, Respiration Rate, Apnea, Health Monitoring.
Abstract:
Sleep constitutes one-third of human life and plays a critical role in physical repair, mental functioning, and
memory consolidation. Although polysomnography (PSG) has been used to assess sleep performance; this
test requires participants to visit a sleep clinic and have multiple sensors attached to their bodies. Hence,
there is a need for alternative methods which can provide sleep monitoring outside clinical settings, but with
clinical standards. In this work, a novel hierarchical framework was built to leverage the seismocardiogram
(SCG) signals in apnea detection and respiration pace assessment using a simulated data collection protocol.
In the first step of the framework, a binary Light Gradient-Boosting Machine (LGBM) model was trained to
detect the breath-holding (apnea) episodes. If the prediction was not a breath-holding state, the data was fed
into a multi-class LGBM model to distinguish between normal, slow and fast breathing episodes. Overall, the
binary LGBM resulted in an accuracy, recall, precision and f1-score of 0.99, 0.95, 0.87 and 0.91, respectively;
whereas for the multi-class case all metrics were 0.96. Additionally, the optimum window length to achieve
real-time detection was determined as 5 seconds. The results show that the SCG signals hold substantial
information regarding the changes in breathing patterns, thus could potentially be leveraged in the design of
wearable systems as an alternative to the PSG test.
1 INTRODUCTION
Sleep constitutes one-third of human life and plays
a critical role in physical repair, mental functioning,
and memory consolidation (Kwon et al., 2021). Re-
cent surveys have shown that the 44% of adults have
experienced a decline in the quality of their sleep
over the past five years, and eight out of every ten
adults expressed a desire to improve their sleep qual-
ity (Philips, 2019). The most commonly observed
sleep problems include insomnia, sleep apnea, and
narcolepsy. Moreover, deteriorations in sleep effi-
ciency due to these problems are associated with sec-
ondary conditions such as depression, obesity, dia-
betes, heart diseases, and neurocognitive disorders
(Altevogt et al., 2006).
Traditionally, polysomnography (PSG) has been
used to assess sleep performance; however, this test
requires participants to visit a sleep clinic and have
multiple sensors attached to their bodies. Although
this system provides a thorough assessment of sleep
quality and related problems, assessing sleep in natu-
a
https://orcid.org/0000-0002-7544-5974
ral settings (at home and without multiple sensor at-
tachment) could potentially provide a more realistic
evaluation. On the other hand, there have emerged
watch-like systems (Apple Watch, etc.) providing
sleep monitoring and staging, however these systems
only use customized algorithms based on movement
and heart rate, and they cannot provide detailed infor-
mation regarding other vital parameters, such as res-
piration rate. Hence, there is a need for alternative
methods which can provide sleep monitoring outside
clinical settings, but with clinical standards.
Recent studies have shown that the seismocardio-
gram (SCG) signal collected from the thoracic re-
gion can provide information about various hemody-
namic parameters (Inan et al., 2014). SCG signal
corresponds to the chest micro-vibrations occurring
due to the ejection of blood and contraction of the
heart in each cardiac cycle. The part of the SCG be-
low 1 Hz corresponds to the chest movements associ-
ated with respiration, the frequencies between 1 - 20
Hz includes the cardiac vibrations, and the compo-
nent above 20 Hz represents the heart sounds (Pandia
et al., 2012). As SCG signals can assess the thoracic
region from different perspectives, they are widely
Kizir, B. and Semiz, B.
A Hierarchical Framework for Apnea Detection and Respiration Pace Assessment Using Seismocardiogram Signals.
DOI: 10.5220/0012446400003657
Paper published under CC license (CC BY-NC-ND 4.0)
In Proceedings of the 17th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2024) - Volume 1, pages 793-798
ISBN: 978-989-758-688-0; ISSN: 2184-4305
Proceedings Copyright © 2024 by SCITEPRESS – Science and Technology Publications, Lda.
793

used in wearable systems aiming to monitor cardio-
vascular and cardiopulmonary diseases (Hayirlioglu
and Semiz, 2023). Indeed, previous studies have
shown that the SCG signals could potentially be used
in the detection of heart failure (Inan et al., 2018),
aortic stenosis (Yang et al., 2019), and atrial fibril-
lation (Hurnanen et al., 2016), as well as predicting
stroke volume values (Semiz et al., 2020), estimating
systolic time intervals (Shandhi et al., 2019), classify-
ing valvular heart disease locations (Erin and Semiz,
2023) and assessing respiration phases (Imirzalioglu
and Semiz, 2022; Pandia et al., 2012).
In this study, we developed a novel hierarchi-
cal framework to leverage the SCG signals in ap-
nea detection and respiration pace assessment using
a simulated data collection protocol including breath-
holding, slow-breathing, normal-breathing and fast-
breathing episodes. Instead of focusing on the com-
ponent below 1 Hz, we leveraged the vibration and
acoustic components of the signal (1-40 Hz) as all ap-
nea types are not necessarily associated with halted
chest movements. In the first step of the framework,
as the most crucial aspect of the study was to de-
termine the breath-holding states, a binary classifica-
tion model was trained to detect the breath-holding
(apnea) episodes. If the prediction was not breath-
holding state, the data was fed into a second model,
which was designed as a multi-class classification
model to distinguish between normal, slow and fast
breathing episodes. In addition, the optimum win-
dow length for achieving real-time apnea detection
and breathing rate assessment was studied. Overall,
the results show that the SCG signals hold substantial
information regarding the changes in breathing pat-
terns, thus could potentially be leveraged in the de-
sign of wearable systems as an alternative to the PSG
test.
2 METHODS
2.1 Data Collection Protocol
This study was conducted under a protocol approved
by the Koc University Institutional Review Board and
all subjects provided written consent. A total of 8
healthy subjects (6 females and 2 males) participated
in the study (Age: 21.9 ± 3.0, height: 171.6 ±
7.7, and weight: 65.4 ± 12.2). The signals were
simultaneously collected using the BIOPAC system
(BIOPAC Systems, Inc. Goleta, CA, USA) at 2 kHz.
The electrocardiogram (ECG) and respiration signals
were acquired using three gel electrodes and a respira-
tion transducer, respectively. The signals were trans-
Figure 1: The locations of the sensors.
ferred to the BIOPAC system using wireless Biono-
madix RSPEC-R module. To record the SCG signal, a
tri-axial low noise analog accelerometer (ADXL354,
Analog Devices, Inc., Norwood, MA) was used. It
was placed on the mid-sternum of the subject using
hypoallergenic transparent medical tape. The sensor
locations are detailed in Fig. 1. The X, Y, Z axes
of the accelerometer were corresponding to the vibra-
tions in lateral, head-to-foot and dorso-ventral direc-
tions, respectively.
Data collection protocol is detailed in Fig. 2.
The subject was first asked to breathe normally for
1 minute, followed by Valsalva maneuver where the
subject held breath for 15 seconds. It was followed by
another 1 minute-long normal breathing. The subject
was then asked to perform slow breathing at 40 beats-
per-minute (bpm) controlled by an online metronome.
After 1 minute-long normal breathing, the subject
performed fast breathing at 120 bpm, again controlled
by a metronome. The last steps were including an ad-
ditional 1 minute-long normal breathing, 15-seconds-
long Valsalva maneuver and another normal breathing
phase for 1 minute. The signals were recorded con-
tinuously during the protocol and the timestamps for
each transition were recorded thoroughly.
2.2 Preprocessing
SCG signals were filtered with a Kaiser window finite
impulse response filter to remove out-of-band noise.
The cut-off frequencies were selected as 1-40 Hz for
all three axes. No other preprocessing steps were ap-
plied not to lose any information (spikes, oscillations,
etc.), which might be useful in determining different
breathing states.
In this work, one of the fundamental aims was
to assess the effect of window length in detection
performance. To that end, the analysis pipeline was
repeated using different window lengths (1, 2, 3, 4
and 5 seconds). Between the consecutive windows,
500 milliseconds-long (0.5 seconds) overlap was em-
ployed. By this way, the number of instances to be
used during training was increased, additionally the
subject’s state could be updated every 0.5 seconds.
BIOSIGNALS 2024 - 17th International Conference on Bio-inspired Systems and Signal Processing
794
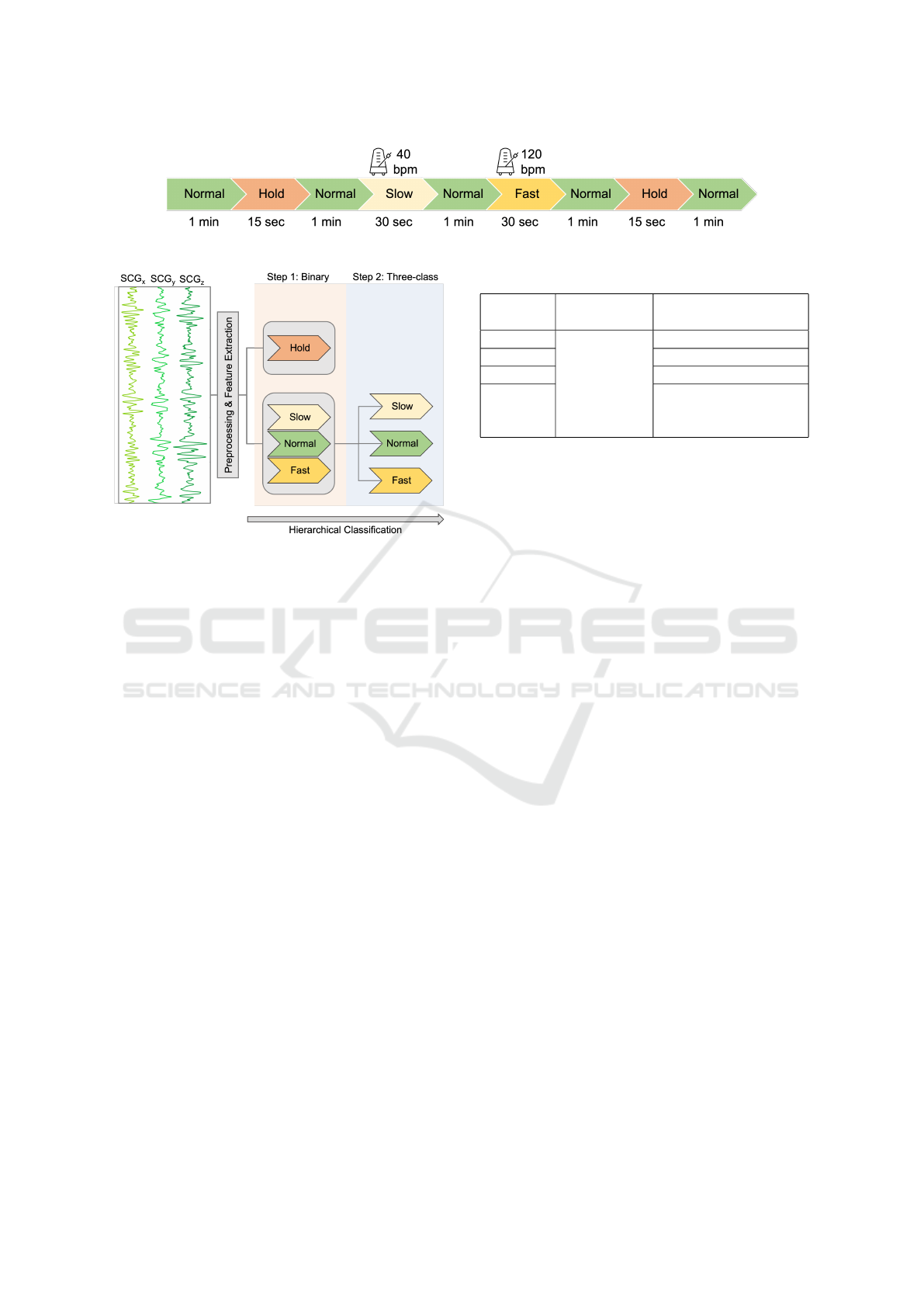
Figure 2: Experimental protocol.
Figure 3: Study pipeline.
It should be noted that the ECG was not used as the
reference since the real-time apnea detection scenario
will necessitate the use of continuous data streaming,
which can be achieved through a sliding window.
2.3 Feature Extraction
Statistical, temporal and spectral features were ex-
tracted from each SCG window in all three axes (Ta-
ble 1). As the statistical features, mean, variance,
skewness (asymmetry) and kurtosis (tailedness) were
calculated. As the temporal feature, signal energy, i.e.
the squared sum of the samples, were computed. On
the other hand, spectral domain features were includ-
ing centroid, spread, rolloff and bandpowers. Rolloff
indicates the frequency at which a specific percent-
age of the signal energy is accumulated. On the other
hand, centroid and spread relate to the center of mass
and the distribution of frequencies in the spectrum, re-
spectively (Giannakopoulos and Pikrakis, 2014). Fi-
nally, bandpower frequency intervals were selected
as logarithmically spaced frequency bands between 1
and 40 Hz. After extracting all features, a dataframe
was generated where columns including the feature
values and rows indicating the corresponding SCG
frames. The whole feature extraction and data frame
generation steps were repeated for different window
lengths.
Table 1: Feature groups.
Statistical
Features
Temporal
Features
Spectral
Features
Mean
Signal Energy
Centroid
Variance Spread
Skewness Rolloff
Kurtosis
Bandpowers
(logarithmically spaced
between 1 - 40 Hz)
2.4 Model Training and Feature
Importance Analysis
2.4.1 Hierarchical Model Framework
In this study a hierarchical model framework was built
(Fig. 3). Since the most crucial aspect of the study
was to determine the breath-holding states, a binary
classification model was trained first. In this model,
breath-holding states were labeled as 1, while the oth-
ers (normal, slow, fast) were all labeled as 0. Test data
was first fed into the binary classifier. If the prediction
was not breath-holding state, the data was fed into a
second model, which was designed as a multi-class
classification model. In this secondary step, the aim
was to distinguish between the normal, slow and fast
breathing episodes. This hierarchical pipeline was
built so that the breath-holding states (i.e. apnea peri-
ods) could be determined as fast as possible regardless
of the changes in breathing pace in-between.
2.4.2 Model Selection and Validation
As the superior performance of the tree-based meth-
ods are well known in SCG-related applications,
four different tree-based models were trained and
compared: decision tree (DT), random forest (RF),
extreme gradient boosting trees (XGB) and light
gradient-boosting machine (LGBM). For all classifi-
cation models, 5-fold cross validation was applied.
• Decision Tree (DT): Decision tree is a tree-like
flowchart which utilizes a divide and conquer
strategy, employing a greedy search to find the
best split points. This splitting process is per-
formed in a top-down fashion until the data-of-
interest has been assigned class labels (Song and
Ying, 2015).
A Hierarchical Framework for Apnea Detection and Respiration Pace Assessment Using Seismocardiogram Signals
795
• Random Forest (RF): Instead of depending on a
single tree, RF involves bootstrapping multiple
trees by utilizing randomized subsets drawn from
the dataset. These trees are trained independently
and in parallel. Majority voting is then applied on
the outputs obtained from these trees to yield one
single class estimation (Breiman, 2001).
• Extreme Gradient Boosting Trees (XGB): XGB is
one of the popular boosting algorithms. As RF re-
lies of bagging, XGB operates sequentially, i.e.,
each subsequent tree relies on the the outcome of
the previous one. Overall, in the training process,
multiple decision trees are trained iteratively, al-
lowing the prediction and adjustment of residual
errors from the previous iteration as the training
advances (Chen and Guestrin, 2016).
• Light Gradient-Boosting Machine (LGBM):
LGBM is another popular type of boosting algo-
rithms, however unlike the horizontal, level-wise
growth seen in XGB, LGBM follows a vertical,
leaf-wise growth pipeline. This approach leads
to increased loss reduction, resulting in higher
accuracy and faster processing (Ke et al., 2017).
To assess the performance of the models, accuracy
and weighted precision, recall and f1-score were used.
These equations are presented in Equations 1, 2, 3 and
4, respectively (TP: true positives, FP: false positives,
TN: true negatives and FN: false negatives). In addi-
tion, the area under the receiver operating character-
istics curve (ROC AUC) was computed for the binary
classification task.
Accuracy =
T P + T N
T P + T N + FP + FN
(1)
Precision =
T P
T P + FP
(2)
Recall =
T P
T P + FN
(3)
f
1
score = 2 ∗
precision ∗ recall
precision + recall
(4)
2.4.3 Feature Importance Ranking
Feature importance scores were computed from the
best performing model (LGBM) to find out the most
important features. The procedure was repeated for
both the binary and multi-class tasks. After all folds
were completed, average of the normalized LGBM
scores was calculated and determined as the final im-
portance score. The corresponding scores were then
ranked in descending order to determine the feature
importance ranking.
Table 2: Performance comparison (binary).
Model Accuracy AUC Recall Precision F1
LGBM 0,99 0,99 0,95 0,87 0,91
RF 0,94 0,95 0,95 0,30 0,46
XGB 0,99 0,99 0,95 0,85 0,90
DT 0,92 0,73 0,56 0,49 0,52
Table 3: Performance comparison (multi-class).
Model Accuracy Recall Precision F1
LGBM 0,96 0,96 0,96 0,96
RF 0,88 0,88 0,94 0,90
XGB 0,95 0,95 0,96 0,96
DT 0,85 0,85 0,85 0,85
3 RESULTS AND DISCUSSION
3.1 Apnea Detection Results
The first step of the hierarchical classification frame-
work was to distinguish between the breath-holding
episodes and breathing (normal, fast, slow) periods.
To that end, a binary classification model was trained.
The results obtained from different models with a
5-sec window were presented in Table 2. Overall,
LGBM and XGB outperformed DT and RF in all met-
rics. Indeed, the precision values obtained from the
RF and DT were significantly lower than the other
models, which led to again low f1-scores. On the
other hand, XGB and LGBM indeed had compara-
ble performance, however LGBM performed slightly
better in terms of precision and f1-score. Having an
accuracy value of 0.99 revealed that there is almost no
carried-error from the binary model to the multi-class
task.
3.2 Breathing Rate Assessment
Using the primary model, the SCG windows were
labeled as breath-holding or not. If the prediction
was not breath-holding state, the data was fed into a
second model, which was designed as a multi-class
classification model. In this secondary step, the aim
was to distinguish between the normal, slow and fast
breathing episodes. The performances of different
models are presented in Table 3. Similar to the bi-
nary case, LGBM and XGB outperformed RF and DT
in terms of all metrics, however the precision and f1-
score obtained from RF and DT in multi-class task
were significantly higher than the ones obtained in
the binary task. Overall, the LGBM model performed
slightly better than the XGB, similar to the binary
case.
BIOSIGNALS 2024 - 17th International Conference on Bio-inspired Systems and Signal Processing
796
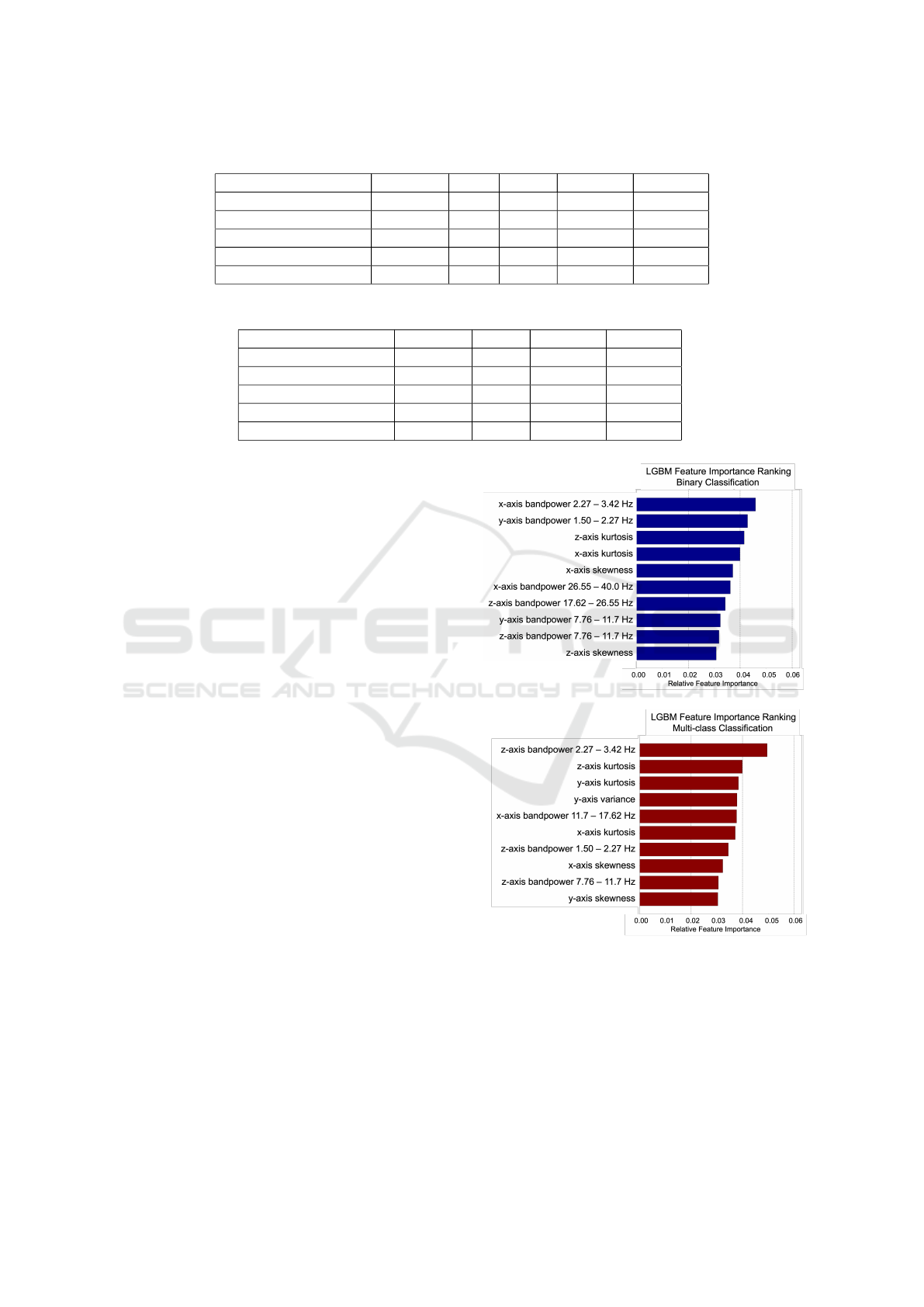
Table 4: LGBM results for different window lengths (binary).
Window Length (sec.) Accuracy AUC Recall Precision F1-Score
1 0,95 0,91 0,72 0,51 0,59
2 0,97 0,96 0,86 0,71 0,78
3 0,98 0,97 0,91 0,77 0,83
4 0,98 0,99 0,93 0,83 0,87
5 0,99 0,99 0,95 0,87 0,91
Table 5: LGBM results for different window lengths (multi-class).
Window Length (sec.) Accuracy Recall Precision F1-Score
1 0,85 0,85 0,88 0,86
2 0,90 0,90 0,92 0,91
3 0,93 0,93 0,94 0,93
4 0,95 0,95 0,96 0,95
5 0,96 0,96 0,96 0,96
3.3 Effect of Window Length
As previously discussed, the ECG was not used as
the reference since the real-time apnea detection sce-
nario necessitates the use of continuous data stream-
ing, which can be achieved through a sliding window.
However, determining the size of the optimum analy-
sis window is an important research question. Hence,
different window lengths (1, 2, 3, 4, 5 seconds) were
tested to find the optimum length for the current ap-
plication. Throughout the experiments, the model was
set to LGBM.
For the binary and multi-class tasks, the perfor-
mance values for varying window lengths are pre-
sented in Tables 4 and 5. When window length was
selected as 1 second, the results got worse signifi-
cantly for both tasks. For the binary case, the re-
call value was calculated as 0.72 when 1-sec windows
were used, i.e., there was a %24 decrease compared
to the case where 5-sec windows were used. Win-
dow lengths longer than 5-sec resulted in similar re-
sults, and when the length exceeded 10-sec, the per-
formance started to decrease. A similar pattern was
also valid for the multi-class task. Based on these
observations, the optimum window length was deter-
mined as 5-sec.
3.4 Feature Importance Ranking
Feature importance scores were computed from the
LGBM classifier. After all folds were completed, av-
erage of normalized scores were calculated as the fi-
nal score. The feature importance results for both
task are presented in Figure 4. Overall, bandpowers,
kurtosis and skewness were dominating in both bi-
nary and multi-class classification tasks. Considering
that the kurtosis represents the tailedness and skew-
Figure 4: Feature importance ranking for the binary and
multi-class tasks.
ness represents asymmetry in the data, they are impor-
tant indicators of how the data is distributed. Having
kurtosis and skewness of multiple axes as the most
important features thus reveals that the distributions
of different breathing episodes were indeed different
than each other.
A Hierarchical Framework for Apnea Detection and Respiration Pace Assessment Using Seismocardiogram Signals
797

4 CONCLUSION
In this work, a novel hierarchical framework was built
using a simulated data collection protocol for evaluat-
ing the potential use of SCG signals in apnea detec-
tion and respiration pace assessment. In the first step
of the framework, a binary Light Gradient-Boosting
Machine (LGBM) model was trained to detect the
breath-holding (apnea) episodes. If the prediction was
not a breath-holding state, the data was fed into a
multi-class LGBM model to distinguish between nor-
mal, slow and fast breathing episodes.
Overall, the binary LGBM model resulted in an
accuracy, recall, precision and f1-score of 0.99, 0.95,
0.87 and 0.91, respectively; whereas for the multi-
class case all metrics were 0.96. Additionally, differ-
ent window lengths (1, 2, 3, 4, 5 seconds) were tested
and the optimum window length was determined as 5
seconds.
The results show that the SCG signals hold sub-
stantial information regarding the changes in breath-
ing patterns, thus could potentially be leveraged in the
design of wearable systems as an alternative to the
PSG test. Future work will focus on validating these
results in larger datasets including real data from pa-
tients having sleep apnea.
REFERENCES
Altevogt, B. M., Colten, H. R., et al. (2006). Sleep dis-
orders and sleep deprivation: an unmet public health
problem.
Breiman, L. (2001). Random forests. Machine learning,
45:5–32.
Chen, T. and Guestrin, C. (2016). Xgboost: A scalable
tree boosting system. In Proceedings of the 22nd acm
sigkdd international conference on knowledge discov-
ery and data mining, pages 785–794.
Erin, E. and Semiz, B. (2023). Spectral analysis of cardio-
genic vibrations to distinguish between valvular heart
diseases.
Giannakopoulos, T. and Pikrakis, A. (2014). Introduction
to audio analysis: a MATLAB® approach. Academic
Press.
Hayirlioglu, Y. Z. and Semiz, B. (2023). A novel multi-
modal sensing system prototype for cardiovascular
and cardiopulmonary monitoring.
Hurnanen, T., Lehtonen, E., Tadi, M. J., Kuusela, T.,
Kiviniemi, T., Saraste, A., Vasankari, T., Airaksinen,
J., Koivisto, T., and P
¨
ank
¨
a
¨
al
¨
a, M. (2016). Auto-
mated detection of atrial fibrillation based on time–
frequency analysis of seismocardiograms. IEEE jour-
nal of biomedical and health informatics, 21(5):1233–
1241.
Imirzalioglu, M. and Semiz, B. (2022). Quantifying respira-
tion effects on cardiac vibrations using teager energy
operator and gradient boosted trees. In 2022 44th An-
nual International Conference of the IEEE Engineer-
ing in Medicine & Biology Society (EMBC), pages
1935–1938. IEEE.
Inan, O. T., Baran Pouyan, M., Javaid, A. Q., Dowling, S.,
Etemadi, M., Dorier, A., Heller, J. A., Bicen, A. O.,
Roy, S., De Marco, T., et al. (2018). Novel wearable
seismocardiography and machine learning algorithms
can assess clinical status of heart failure patients. Cir-
culation: Heart Failure, 11(1):e004313.
Inan, O. T., Migeotte, P.-F., Park, K.-S., Etemadi, M.,
Tavakolian, K., Casanella, R., Zanetti, J., Tank, J.,
Funtova, I., Prisk, G. K., et al. (2014). Ballistocardio-
graphy and seismocardiography: A review of recent
advances. IEEE journal of biomedical and health in-
formatics, 19(4):1414–1427.
Ke, G., Meng, Q., Finley, T., Wang, T., Chen, W., Ma, W.,
Ye, Q., and Liu, T.-Y. (2017). Lightgbm: A highly
efficient gradient boosting decision tree. Advances in
neural information processing systems, 30.
Kwon, S., Kim, H., and Yeo, W.-H. (2021). Recent ad-
vances in wearable sensors and portable electronics
for sleep monitoring. Iscience, 24(5).
Pandia, K., Inan, O. T., Kovacs, G. T., and Giovangrandi, L.
(2012). Extracting respiratory information from seis-
mocardiogram signals acquired on the chest using a
miniature accelerometer. Physiological measurement,
33(10):1643.
Philips (2019). The global pursuit of better sleep health.
Semiz, B., Carek, A. M., Johnson, J. C., Ahmad, S.,
Heller, J. A., Vicente, F. G., Caron, S., Hogue, C. W.,
Etemadi, M., and Inan, O. T. (2020). Non-invasive
wearable patch utilizing seismocardiography for peri-
operative use in surgical patients. IEEE Journal
of Biomedical and Health Informatics, 25(5):1572–
1582.
Shandhi, M. M. H., Semiz, B., Hersek, S., Goller, N.,
Ayazi, F., and Inan, O. T. (2019). Performance
analysis of gyroscope and accelerometer sensors for
seismocardiography-based wearable pre-ejection pe-
riod estimation. IEEE journal of biomedical and
health informatics, 23(6):2365–2374.
Song, Y.-Y. and Ying, L. (2015). Decision tree methods: ap-
plications for classification and prediction. Shanghai
archives of psychiatry, 27(2):130.
Yang, C., Aranoff, N. D., Green, P., and Tavassolian, N.
(2019). Classification of aortic stenosis using time–
frequency features from chest cardio-mechanical sig-
nals. IEEE Transactions on Biomedical Engineering,
67(6):1672–1683.
BIOSIGNALS 2024 - 17th International Conference on Bio-inspired Systems and Signal Processing
798
