A Concept for Daily Assessments During Nutrition Intake: Integrating
Technology in the Nursing Process
Sandra Hellmers
1 a
, Tobias Krahn
2 b
, Martina Hasseler
3
and Andreas Hein
1 c
1
Assistance Systems and Medical Device Technology, Carl von Ossietzky University Oldenburg, Oldenburg, Germany
2
OFFIS e.V. – Institute for Information Technology, Oldenburg, Germany
3
Faculty of Health Sciences, Ostfalia University of Applied Sciences, Wolfsburg, Germany
fi
Keywords:
Nursing Documentation, Nursing Process, Generative AI, Nutrition, Body Tracking, Functional Assessment,
Nursing Language.
Abstract:
The nursing process involves a cyclic sequence of functional and cognitive assessments and diagnosis, care
planning, implementation, and evaluation of care. Ideally, this process should be performed regularly and
documented in a standardized nursing language. However, due to the high workload of nurses, this approach
is not systematically followed. Therefore, we developed a concept that enables a daily, technology-supported
assessment during the activity of nutrition intake. For this purpose, we used camera-based body tracking
to derive the hand and relevant object trajectories to analyze the movements regarding assistance needs and
functional changes over time. We tested the approach of using generative AI to create training data sets. Our
feasibility study has shown that trajectories can be derived and analyzed regarding assistance requirements.
Although the quality is not yet satisfactory, generative AI can be used to create training data. Considering the
rapid pace of further developments in generative AI, the approach seems to be promising. In conclusion, we
believe that the technical support and documentation of the nursing process have the potential to increase the
quality of care while reducing the workload of nurses.
1 INTRODUCTION
Due to the demographic change, the number of peo-
ple reaching old age increases. This development
will also result in an increasing demand for health
and care services. The number of people in need of
care in Germany will increase by 37% by 2055 due
to ageing alone (Statistisches Bundesamt (Destatis),
2023). There is already a gap between the supply
of carers and the demand for care. Additionally, it
was shown that the patient-to-caregiver ratio has mea-
surable negative effects on patient mortality rates and
the stress experienced by caregivers (H
¨
ohmann et al.,
2016; Aiken et al., 2012).
To realize qualified, patient-centered, and needs-
based care, the nursing process was established,
which is a systematic approach to organizing nurs-
ing practice, nursing knowledge, and nursing care
(Hojdelewicz, 2021; Doenges and Moorhouse, 2012).
a
https://orcid.org/0000-0002-1686-6752
b
https://orcid.org/0009-0001-5619-8138
c
https://orcid.org/0000-0001-8846-2282
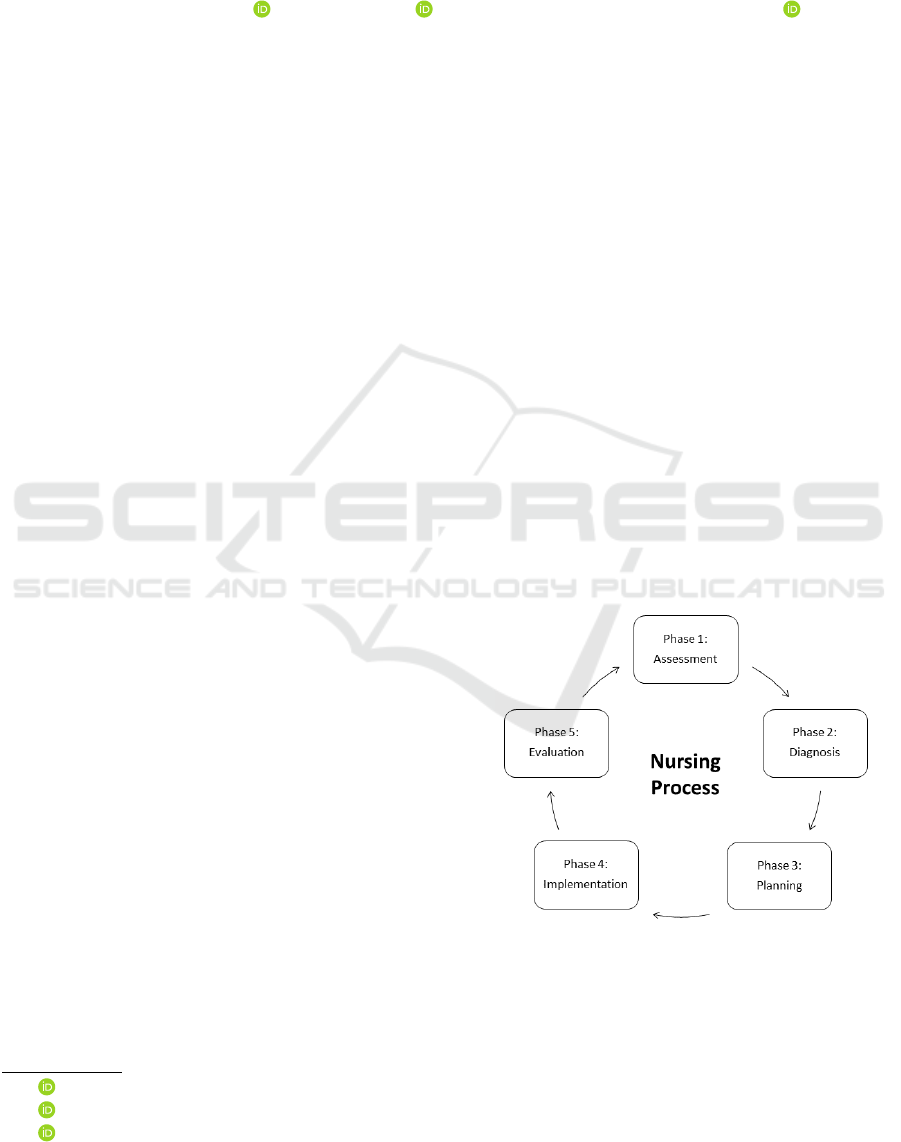
Figure 1: Five phases of the nursing process.
The five-phases model of the nursing process (Do-
enges and Moorhouse, 2012) is shown in Figure 1 and
starts with an assessment to collect information about
the patient, the diseases, and the functional status. In
phase two a diagnosis is made on the basis of the as-
sessment results. Phase three is the treatment and care
planning. The treatments and nursing actions are im-
Hellmers, S., Krahn, T., Hasseler, M. and Hein, A.
A Concept for Daily Assessments During Nutrition Intake: Integrating Technology in the Nursing Process.
DOI: 10.5220/0012428700003657
Paper published under CC license (CC BY-NC-ND 4.0)
In Proceedings of the 17th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2024) - Volume 2, pages 613-619
ISBN: 978-989-758-688-0; ISSN: 2184-4305
Proceedings Copyright © 2024 by SCITEPRESS – Science and Technology Publications, Lda.
613
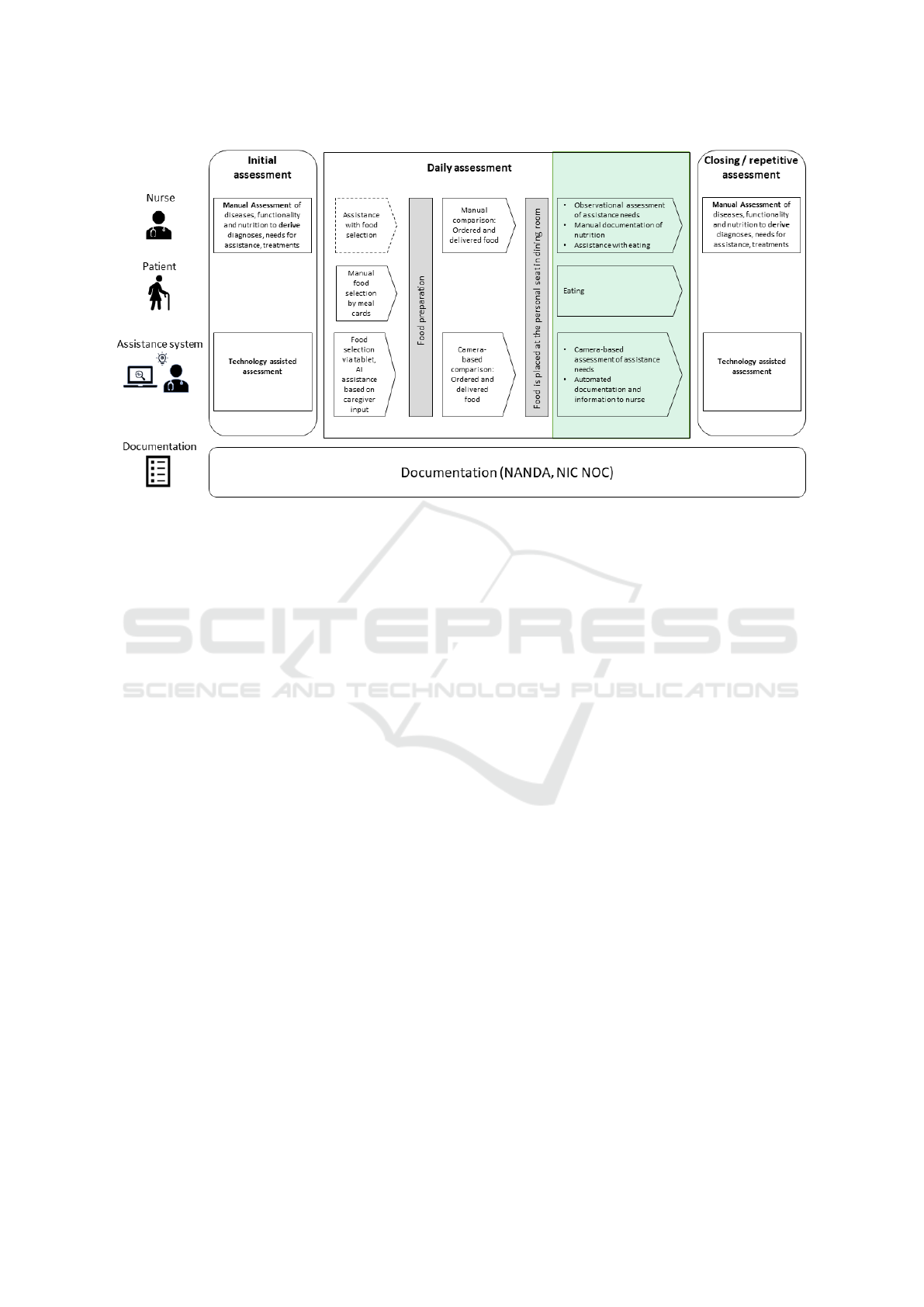
Figure 2: Assessment phases in a care process should be performed regularly. They can be done manually by a nurse or
technology assisted by an assistance system. The focus of this paper is to assess the activity of eating (green box).
plemented in phase four and evaluated in phase five.
Since the care process is of continuous nature, it starts
again with phase one.
Due to the high workload of nurses, there is of-
ten a lack of time to implement the nursing process
regularly at short intervals and, above all, to docu-
ment nursing care adequately. The use of a standard-
ized nursing language is particularly important for the
implementation of electronic health records (EHR)
(Lunney, 2006). Standardized nursing language in-
cludes NANDA (Ackley and Ladwig, 2010) for nurs-
ing diagnoses, the Nursing Interventions Classifica-
tion (NIC) (Bulechek et al., 2012), which describes
the activities that nurses perform as a part of the plan-
ning phase and the Nursing Outcomes Classification
(NOC) (Moorhead et al., 2023) to evaluate the effects
of nursing care.
Ongoing technological development is increasingly
finding its way into the care sector and can sup-
port nurses in their daily work. There are already
a number of approaches to technology-assisted as-
sessments (Hellmers, 2021), technical systems to re-
duce the physical strain on nurses (Brinkmann et al.,
2022), and applications of extended reality (XR) in
the care context (Carroll et al., 2020; W
¨
uller et al.,
2019). Artificial intelligence (AI) in nursing is mainly
used for early disease detection and clinical decision
making, support systems for patient monitoring and
workfow optimisation, nursing training and educa-
tion (Martinez-Ortigosa et al., 2023). Newer develop-
ments such as generative AI (GenAI) also offer inter-
esting possibilities, as they are able to generate syn-
thetic data, which can be used to augment training
data and create diverse datasets for research and med-
ical training (Lancet Regional Health-Europe, 2023).
Therefore, we will focus in this article on a holistic
approach to the technical support of the care process,
considering the application of GenAI. Figure 2 shows
the assessment phase of the care process and the ac-
tions of the nurse, the patient, and the assistance sys-
tem in this phase. This article focuses on the daily
assessment (green box). However, an initial assess-
ment is performed upon admission to a care facility to
determine the patient’s functional status, identify any
assistance needed, and plan care. For short-time stays
a closing assessment is usually performed before dis-
charge to determine the success of treatment. For
longer stays, the assessment should be repeated regu-
larly as part of the repetitive care process. The assess-
ments can be done manually by a nurse or technology-
assisted.
High frequent assessments can also be realized by
monitoring and analyzing daily activities like nutri-
tion intake. Inadequate nutritional and hydration sta-
tus in older people with healthcare needs has rele-
vant negative effects on the immune system, cogni-
tive function, and physical mobility. It is also a risk
factor for susceptibility to infection, delayed wound
healing, falls, delirium, altered metabolism of medi-
cations, deterioration of physical and cognitive func-
tion, and other adverse reactions (Volkert et al., 2022;
Feldblum et al., 2009). The high relevance of nutri-
tion and hydration for maintaining functional status,
autonomy, and quality of life (Volkert et al., 2022) is
HEALTHINF 2024 - 17th International Conference on Health Informatics
614

a major motivation for this work.
The food selection is often done by the patients
via meal cards and can be assisted by nurses if nec-
essary. Technological systems can also assist the pa-
tient with the food selection based on the individual
nurses’ input for each patient. After food preparation,
the nurses check if the ordered and delivered food
matches. This comparison is relevant for disease-
specific diets, allergies, or if the patient can only eat
soft food. Object recognition by assistance systems
can also be used for this comparison. Since the food
intake is at focus in this paper (green box in Figure 2),
the phase of eating is relevant to derive requirements
for assistance needs and changes in the functional
status. The assessment can be conducted through
observation and manual documentation by a nurse.
This observational assessment can also be supported
by a camera-based assessment, in which the assis-
tance systems derive assistance needs and functional
changes based on activity recognition and the analy-
sis of the activities, for example, the hand trajectories
while eating. The results can be automatically doc-
umented in a standardized language (NANDA, NIC,
NOC). In this case, the nurses can screen the informa-
tion and plan the nursing care regarding the nursing
process.
In summary, we concentrate on the overall con-
cept of a technology-assisted daily assessment using
new technological developments and focus on the fol-
lowing research questions:
• What can a high frequent assessment look like in
which the caregiver and the assistance system sup-
port each other in a meaningful way?
• How can new technological developments such as
generative AI be used?
• How can a standardized care language be imple-
mented in this concept?
2 METHODS
2.1 Concept of Daily Assessments
One point of criticism of monitored assessments is
that they only represent selective measurements and
often no progressions are recorded. The aim is there-
fore to derive care-relevant assessment parameters
from complex everyday activities. To do this, com-
plex activities must first be recognized and relevant
parameters derived on the basis of their performance.
Deficits in self-care result for example from lack of
hand functionality and coordination skills. For sen-
sory recognition of activities, aspects such as con-
textualization and parallelism must be taken into ac-
count (actions have a certain duration and sequence
and may also involve interaction with objects). The
digital information should be collected uniformly and
documented in a standardized language. Nursing pro-
fessionals assess information collected through tech-
nology, extend it by own observations, and may uti-
lize a decision support system in the future to deter-
mine and implement practical interventions for nutri-
tion and hydration. With regard to activating care,
nursing interventions are also examined in order to
derive and document suitable strategies for food and
fluid intake. Based on the successful strategies, self-
help can be supported in a targeted manner and the
care staff can be relieved.
2.2 AI-Generated Norm-Trajectories
and Real Measurements
As a specific use case we concentrated on eating soup
in this paper, since holding and moving a spoon with-
out spilling can be quite challenging for people with
functional disabilities. Three study participants took
part in the study to demonstrate the feasibility of our
concept. We used the RGB-D-camera Azure Kinect
DK and its Azure Kinect Body Tracking SDK with
the Direct ML processing mode. The trajectories of
the right hand, right wrist, and right hand tip were
calculated. Since the mouth can’t be tracked with the
Azure Kinect Body Tracking SDK we calculated the
trajectories of the key points head and nose. The tra-
jectories were filtered with a first-order Butterworth
filter with a cutoff frequency of 5 Hz to reduce noise.
We also generated AI-based videos with the Run-
wayML Gen-2 text-to-video tool (RunwayML, 2023)
using the prompt: ”Old man is sitting at a table and
eats soup. He holds a spoon in the right hand”. We
performed a manual body and object tracking of the
AI-generated videos. However, machine learning so-
lutions like MediaPipe (Lugaresi et al., 2019) can be
used for automatic tracking.
3 RESULTS
3.1 Concept of Daily Assessment
Figure 3 shows the concept of a camera-based
technology-supported assessment. The main aspect
of realizing such an assessment is the recognition of
the human and the food. Therefore, body tracking is
used to recognize the position of the mouth and the
hand. Object recognition is used to determine the po-
A Concept for Daily Assessments During Nutrition Intake: Integrating Technology in the Nursing Process
615
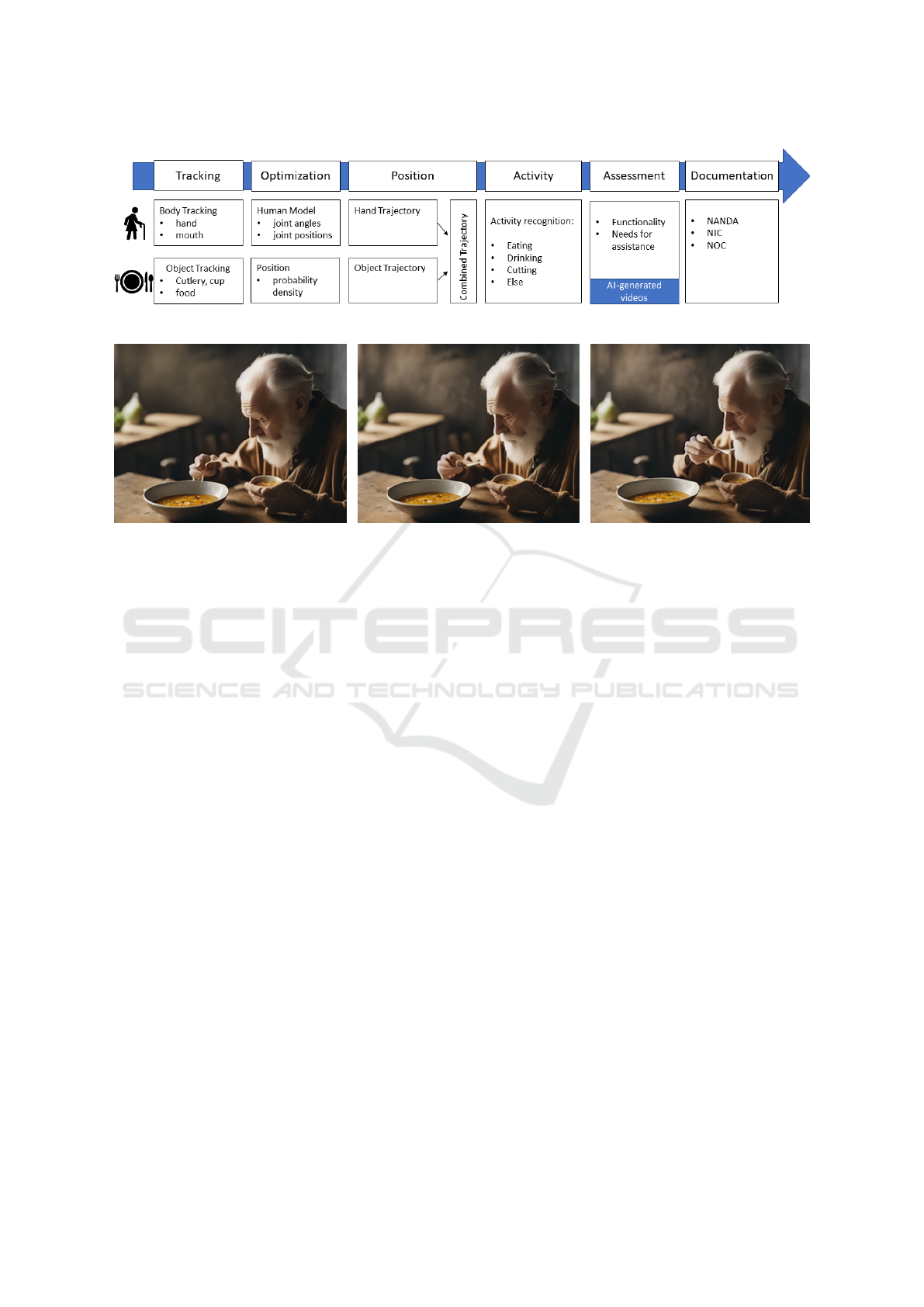
Figure 3: Technical process of activity recognition and assessment.
Figure 4: Screenshots of an AI-generated video of an old man eating soup (RunwayML, 2023).
sition of the food and other relevant objects like cut-
lery or cups. For optimization of the body tracking a
human body model should be considered. This model
consists of valid joint angles and relative positions so
that unrealistic positions are automatically removed.
For objects a position probability density should be
considered, to remove outliers and unrealistic posi-
tions as well as the problem of suddenly disappearing
objects for example due to occlusions. Based on the
optimized body tracking results the hand and object
trajectories can be calculated and related to each other
to get a combined trajectory. Analyzing the combined
trajectories leads to activity recognition. Machine
learning based methods for activity recognition can
be divided into two categories: Direct classification
and sequential modeling (Poppe, 2010). When the
temporal sequence of an activity is important, sequen-
tial models are required to represent this sequence in
the form of state models. Eating and drinking corre-
spond to a sequential activity: the glass must first be
grasped, then brought to the mouth and tilted slightly
in order to drink. Then the glass is put down again.
In the next step the activity can be analyzed and as-
sessed regarding functional and assistance needs. A
focus of inquiry could be the shapes of the trajecto-
ries (intentional movement, movement disorders such
as tremors) and the effectiveness of food consump-
tion, exemplified by the ability to hold and use cutlery
successfully.
Machine learning approaches often require a huge
set of training data of normal and pathological ac-
tivities. The ongoing development of generative AI
might be a game changer in this field. We proved the
concept of using AI-generated videos to create train-
ing data. Since the AI models are trained on many
videos mostly without pathological findings, these
videos are used as norm trajectories. The last step
includes the documentation of the assessment with a
standardized nursing language.
3.2 AI Generated Norm-Trajectories
We created AI-generated videos with textual input.
Figure 4 shows three screenshots of one video. This
video fits the description very well. From the patient
information (old man) and the delivered food (soup)
as well as the context (eating food while sitting at the
table), the correct objects (bowl, spoon) as well as
the correct trajectories (spoon to mouth) and hand ori-
entations (horizontal posture) are derived. However,
there are also some contextual errors or curiosities.
For example, the man is also holding a second plate
of soup in his left hand. The manual body and ob-
ject tracking is shown in Figure 5. The trajectories of
the mouth (green), the knuckles (blue), and the tip of
the spoon (orange) are visualized. The man sits in a
slightly bent posture during the video. There is almost
no movement of the upper body and the head. There-
fore, the position of the mouth varies only in a small
range. The trajectory of the hand starts with an arc to
fill the spoon with soup, followed by a direct trajec-
tory to the mouth. The video stops before the spoon
HEALTHINF 2024 - 17th International Conference on Health Informatics
616
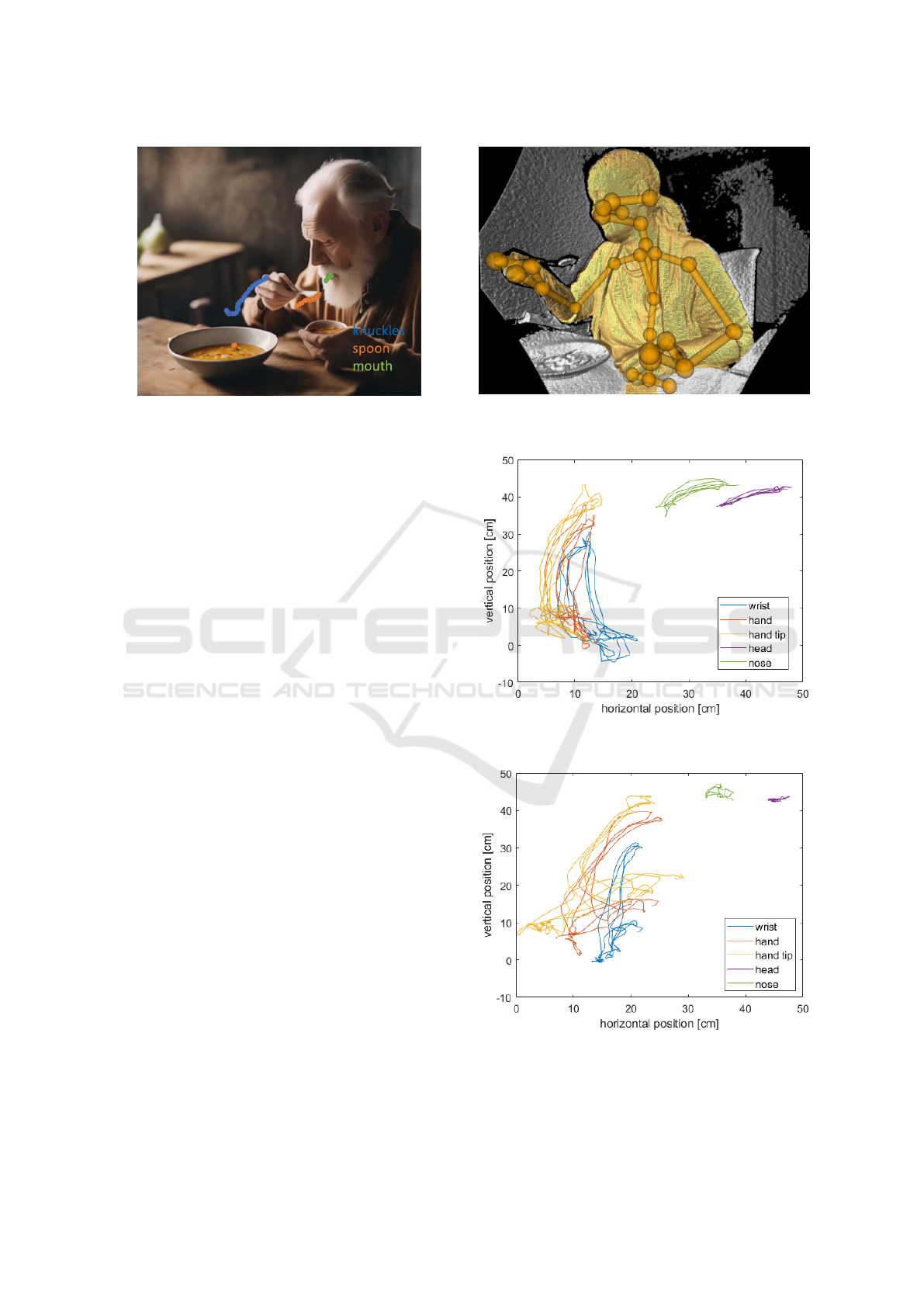
Figure 5: Manual tracking of mouth, knuckles, and spoon
in the AI-generated video (RunwayML, 2023).
reaches the mouth. The measurement of the trajectory
of the spoon (orange) is interrupted quite extensively
due to the disappearance of the spoon in the middle
of the video. The presented video is one of the best-
fitting videos. The challenges and further observa-
tions in generating AI-based videos are described in
the discussion section 4. However, the feasibility of
using generative AI to create training data for activity
recognition could be confirmed. A selection of some
further videos with similar textual prompts as input is
uploaded here (AI-generated Videos, 2023).
3.3 Measurement of Real Trajectories
Figure 6 shows the body tracking results of one par-
ticipant based on depth data using the Azure Kinect
SDK. Similar to the tracking in the AI-generated
video, the trajectories of the relevant key points were
recorded and presented in Figure 7. For the right
hand, the key points are the wrist, the hand itself as
well as the hand tip. Since the mouth can’t be tracked
with the Azure Kinect SDK, the key points head and
nose are visualized. For better comparison and in-
terpretation of the trajectories with the video screen-
shot in Figure 6, a 2D representation was chosen.
However, the positions of the key points are avail-
able in 3D so that the perspective can be adjusted.
The trajectories for three cycles (spoon to mouth) are
shown. The trajectories are similar for each cycle.
The hand position is stable while bringing the spoon
to the mouth. The head is moved in the direction of
the spoon.
Figure 8 shows the trajectories of the same person
while eating with a fork. The trajectories differ from
eating with a spoon. There is a 90-degree tilt of the
hand while using a fork. It can also be seen that the
head movement varies in a smaller range than while
Figure 6: Body tracking of a real measurement of a person
eating with a spoon.
Figure 7: Trajectories of relevant key points of a person
eating with a spoon.
Figure 8: Trajectories of relevant key points of a person
eating with a fork.
eating with a spoon. Comparisons with trajectories of
the other study participants (not shown here) indicate
A Concept for Daily Assessments During Nutrition Intake: Integrating Technology in the Nursing Process
617

that each person has an individual trajectory, but the
trajectories stay similar during several cycles.
3.4 Documentation
The use of a standardized nursing language in daily
work and communication is particularly important for
the care of patients and those in need of care be-
tween the various actors in health and nursing care
(Bernhart-Just et al., 2010).
The nursing diagnosis, which can be derived from
the presented daily assessment is ”feeding self-care
deficit”, which includes for example the inability to
bring food to mouth, get food onto utensils, handle
utensils, open containers, pick up a cup or a glass
(Wilkinson, 2014; Herdman et al., 2021). These in-
abilities can be derived from the evaluated videos and
the object and hand trajectories. Consider the exam-
ple of eating soup: If, for example, the trajectory for
eating soup is similar to the trajectory of the (AI-
) generated norm trajectories, no deficit in eating is
coded. However, if the trajectory deviates from the
norm trajectories, inabilities such as bringing food to
the mouth or handling utensils can be assumed. In
this case, a feeding deficit is documented.
A relevant NOC outcome for these patients is
”Self-Care: Eating”, which is related to the patient’s
ability to prepare and ingest food and fluid indepen-
dently with or without assistive device. Relevant NIC
interventions include ”Feeding” for a patient who is
unable to feed him- or herself, or ”Self-Care Assis-
tance: Feeding,” which means assisting a person to
eat. ”Nutrition monitoring” as another intervention
involves the collection and analysis of patient data to
prevent or minimize malnutrition (Wilkinson, 2014).
Nursing activities also include ”Eating Techniques In-
struction” to demonstrate the proper use of utensils,
assistive devices, and adaptive activities to teach pa-
tients alternative methods of eating and drinking.
4 DISCUSSION
We developed a concept that enables a daily,
technology-supported assessment during the activity
of nutrition intake. For this purpose, we used camera-
based body tracking to derive the hand and rele-
vant object trajectories to analyze the movements re-
garding assistance needs and functional changes over
time. Additionally, we tested the feasibility of using
generative AI to create training data sets.
We were able to demonstrate the general imple-
mentation of the assessment concept in this paper
in a pilot study, although only the nursing diagnosis
of feeding self-care deficit can be included. Other
nutrition-relevant nursing diagnoses like frailty syn-
drome, unbalanced diet, impaired swallowing, fluid
imbalance, and inadequate fluid intake have yet not
been considered. Especially, the feasibility of assess-
ing the diagnosis of impaired swallowing and the un-
balanced diet could be realized in the next step via
video analyses and digital before and after plate pro-
tocols.
Generative AI seems to be a promising approach
to creating training data, especially when consider-
ing the high pace of further developments. We ex-
pect that the quality of AI-generated videos by the
text-to-video function will highly increase in the next
years. This enables the possibility to generate training
data sets without involving and burdening patients. It
holds also the possibility to generate videos with pa-
tients with specific symptoms like tremors or paraly-
sis in the future. However, in addition to the still poor
match between text input and generated videos, and
contextual or physical errors or abnormalities (second
cup of soup, oversized spoon, spoon disappears or
seems to melt), we also observed ethical issues. The
videos with an ”old person” as input often generated a
clich
´
ed video background with dark old wooden fur-
niture. Stereotypes are also used, e.g. by generat-
ing videos where instead of a woman eating soup, an
old woman spills the soup and it runs down her chin.
This also shows the dangers of artificial intelligence in
terms of prejudice and stigmatization. Therefore, syn-
thetically generated data should be used with caution
and it is important to bear in mind that the expertise
of care professionals is required for the meaningful
training of AI and the integration of meaningful data.
This is particularly important if the AI is to take over
clinical pathways, disease progression, or the pre-
diction of deterioration and thus prepare the ground
for professional action for example in clinical deci-
sion support systems. According to the literature, IT-
and AI-based processes in nursing can support clini-
cal decisions or even generate automatic warning sys-
tems and thus also systematically support the nursing
workflow and enable personalized patient care (Sens-
meier, 2017; Buchanan et al., 2020). But new tech-
nologies in nursing influence the interaction between
the actors (caregivers and care recipients), the organi-
zational processes in the nursing setting, and the as-
sociated information relationships between the actor
(Zerth et al., 2021). Therefore, we suggest that deci-
sions need to be made with the actors, especially the
nurses, about what data needs to be collected and in-
tegrated, for what reasons, and with what purpose, so
that it is adequate for the care process and decision-
making.
HEALTHINF 2024 - 17th International Conference on Health Informatics
618

ACKNOWLEDGEMENTS
This work was funded by the Lower Saxony Ministry
of Science and Culture under grant number 11-76251-
12-10/19 ZN3491 within the Lower Saxony “Vorab”
of the Volkswagen Foundation and supported by the
Center for Digital Innovations (ZDIN). We would like
to thank Linda B
¨
uker and Lea Ortmann for their valu-
able input and feedback.
REFERENCES
Ackley, B. J. and Ladwig, G. B. (2010). Nursing diagnosis
handbook-e-book: An evidence-based guide to plan-
ning care. Elsevier Health Sciences.
AI-generated Videos (2023). https://cloud.uol.de/s/bKcKG
y3QKG7LdEm.
Aiken, L. H., Sermeus, W., Van den Heede, K., Sloane,
D. M., Busse, R., McKee, M., Bruyneel, L., Raf-
ferty, A. M., Griffiths, P., Moreno-Casbas, M. T., et al.
(2012). Patient safety, satisfaction, and quality of hos-
pital care: cross sectional surveys of nurses and pa-
tients in 12 countries in europe and the united states.
BMJ, 344:e1717.
Bernhart-Just, A., Lassen, B., and Schwendimann, R.
(2010). Representing the nursing process with nursing
terminologies in electronic medical record systems: a
swiss approach. CIN: Computers, Informatics, Nurs-
ing, 28(6):345–352.
Brinkmann, A., B
¨
ohlen, C. F.-v., Kowalski, C., Lau, S.,
Meyer, O., Diekmann, R., and Hein, A. (2022).
Providing physical relief for nurses by collaborative
robotics. Scientific Reports, 12(1):8644.
Buchanan, C., Howitt, M. L., Wilson, R., Booth, R. G., Ris-
ling, T., and Bamford, M. (2020). Predicted influences
of artificial intelligence on the domains of nursing:
scoping review. JMIR nursing, 3(1):e23939.
Bulechek, G. M., Butcher, H. K., Dochterman, J. M. M.,
and Wagner, C. (2012). Nursing interventions classi-
fication (NIC). Elsevier Health Sciences.
Carroll, W. M. et al. (2020). Emerging technologies for
nurses: Implications for practice. Springer Publishing
Company.
Doenges, M. E. and Moorhouse, M. F. (2012). Application
of nursing process and nursing diagnosis: an interac-
tive text for diagnostic reasoning. FA Davis.
Feldblum, I., German, L., Bilenko, N., Shahar, A., Enten,
R., Greenberg, D., Harman, I., Castel, H., and Sha-
har, D. R. (2009). Nutritional risk and health care use
before and after an acute hospitalization among the el-
derly. Nutrition, 25(4):415–420.
Hellmers, S. (2021). Technikgest
¨
utztes klinisches Assess-
ment der k
¨
orperlichen Funktionalit
¨
at f
¨
ur
¨
altere Men-
schen. Verlag Dr. Hut.
Herdman, T. H., Kamitsuru, S., and Lopes, C. (2021).
NANDA International Nursing Diagnoses: Defini-
tions and Classification 2021-2023. New York:
Thieme, 12th edition.
H
¨
ohmann, U., Lautenschl
¨
ager, M., and Schwarz, L. (2016).
Belastungen im pflegeberuf: Bedingungsfaktoren, fol-
gen und desiderate. Pflege-Report, pages 73–89.
Hojdelewicz, B. M. (2021). Der Pflegeprozess:
Prozesshafte Pflegebeziehung. Wien: facultas.
Lancet Regional Health-Europe, T. (2023). Embracing gen-
erative ai in health care. The Lancet Regional Health-
Europe, 30.
Lugaresi, C., Tang, J., Nash, H., McClanahan, C., Uboweja,
E., Hays, M., Zhang, F., Chang, C.-L., Yong, M., Lee,
J., et al. (2019). Mediapipe: A framework for per-
ceiving and processing reality. In Third workshop on
computer vision for AR/VR at IEEE computer vision
and pattern recognition (CVPR), volume 2019.
Lunney, M. (2006). Helping nurses use nanda, noc, and
nic: Novice to expert. JONA: The Journal of Nursing
Administration, 36(3):118–125.
Martinez-Ortigosa, A., Martinez-Granados, A., Gil-
Hern
´
andez, E., Rodriguez-Arrastia, M., Ropero-
Padilla, C., Roman, P., et al. (2023). Applications of
artificial intelligence in nursing care: A systematic re-
view. Journal of Nursing Management, 2023.
Moorhead, S., Swanson, E., and Johnson, M. (2023). Nurs-
ing Outcomes Classification (NOC)-e-book: Mea-
surement of health outcomes. Elsevier Health Sci-
ences.
Poppe, R. (2010). A survey on vision-based human action
recognition. Image and vision computing, 28(6):976–
990.
RunwayML (2023). https://runwayml.com. accessed:
2023-11-15.
Sensmeier, J. (2017). Harnessing the power of artificial in-
telligence. Nursing management, 48(11):14–19.
Statistisches Bundesamt (Destatis) (2023). Pflegevoraus-
berechnung: 1,8 millionen mehr pflegebed
¨
urftige bis
zum jahr 2055 zu erwarten. Pressemitteilung Nr. 124
vom 30. M
¨
arz 2023, https://www.destatis.de/DE/Press
e/Pressemitteilungen/2023/03/PD23\ 124\ 12.html.
Volkert, D., Beck, A. M., Cederholm, T., Cruz-Jentoft, A.,
Hooper, L., Kiesswetter, E., Maggio, M., Raynaud-
Simon, A., Sieber, C., Sobotka, L., et al. (2022). Es-
pen practical guideline: Clinical nutrition and hydra-
tion in geriatrics. Clinical Nutrition, 41(4):958–989.
Wilkinson, J. M. (2014). Pearson nursing diagnosis hand-
book with NIC interventions and NOC outcomes.
Pearson.
W
¨
uller, H., Behrens, J., Garthaus, M., Marquard, S., and
Remmers, H. (2019). A scoping review of augmented
reality in nursing. BMC nursing, 18(1):1–11.
Zerth, J., Jaensch, P., and M
¨
uller, S. (2021). Technik,
pflegeinnovation und implementierungsbedingungen.
In Jacobs, K., Kuhlmey, A., Greß, S., Klauber, J., and
Schwinger, A., editors, Pflege-Report 2021: Sicher-
stellung der Pflege: Bedarfslagen und Angebotsstruk-
turen, pages 157–172, Berlin, Heidelberg. Springer
Berlin Heidelberg.
A Concept for Daily Assessments During Nutrition Intake: Integrating Technology in the Nursing Process
619
