
Balancing Resources and Demand: A Bi-Objective Mixed-Integer
Programming Approach of Healthcare Districts in Chile
Paulette Castillo
1
, Victor Bucarey
3 a
, Sebasti
´
an Davila
1,2
and Franco Quezada
1,2 b
1
University of Santiago of Chile (USACH), Faculty of Engineering, Industrial Engineering Department, Chile
2
University of Santiago of Chile (USACH), Faculty of Engineering,
Program for the Development of Sustainable Production Systems (PDSPS), Chile
3
Institute of Engineering Sciences, Universidad de O’Higgins, Rancagua, Chile
Keywords:
Healthcare System, Districting Problem, Mixed-Integer Linear Programming Formulation.
Abstract:
In the search for equitable and efficient health service delivery, geographical partition into operational districts
is a fundamental factor. This research delves into the intricate challenge of combinatorial optimization of
healthcare districts, with an application to the Metropolitan region of Santiago, Chile, where growing popula-
tion pressures exacerbate concerns about the distribution of healthcare resources. By emphasizing continuity
from primary to secondary healthcare levels, we underline the importance of a good district plan, considering
key parameters such as population homogeneity, compactness, and alignment between capacity and demand.
By applying a mixed integer linear programming model with a bi-objective function, our findings indicate sub-
stantial scope for improving resource allocation, potentially cutting overages by up to 38.77% at the primary
healthcare level and up to 15% at the secondary healthcare level.
1 INTRODUCTION
One of the foundations of healthcare service delivery
is the partitioning of geographical regions into opera-
tional units or districts. This partitioning aims to opti-
mize resource utilization and ensure equitable access
to healthcare services across diverse demographic and
socio-economic strata. With roots in various disci-
plines, including city planning, administrative juris-
diction allocation, and, notably, healthcare manage-
ment, the concept of districting—also referred to as
re-districting or territory design—emerges as a chal-
lenging combinatorial optimization problem (Validi
and Buchanan, 2022).
Mathematical modeling of the healthcare district-
ing problem entails formulating an objective function
that drives towards creating districts that uphold ge-
ographic cohesion while synchronizing several key
performance indicators, including but not limited to
resource allocation, population balancing, and de-
mand flux. Particularly in settings like Latin Amer-
ica, the diversity and disparity inherent in the pop-
ulation and regional geography fuel the complexity
a
https://orcid.org/0000-0002-3043-8404
b
https://orcid.org/0000-0001-5763-5582
of this optimization problem, resulting in a challeng-
ing environment for applying districting models and
strategies (Lin and Kao, 2008).
In this work, we focus on primary and secondary
healthcare planning, where the implications of dis-
tricting are prominently displayed. The pathway
through healthcare often commences with a primary
care encounter, typically with a General Practitioner
(GP), and is subsequently integrated with secondary
care depending on the patient’s needs. A meticulously
crafted districting plan becomes critical to orches-
trating a hierarchical network that seamlessly guides
patients along this journey, from primary care cen-
ters to advanced care centers, while balancing the
load across the entire healthcare infrastructure (R
´
ıos-
Mercado and L
´
opez-P
´
erez, 2013).
In-depth planning of healthcare systems involves
a cascade of intertwined decisions, spanning the loca-
tion of healthcare points, demarcation of service ar-
eas, capacity configuration, resource allocation, and
staff scheduling, to name a few. The design of health-
care service regions, or in other words, the districting
of healthcare services, surfaces as a cardinal dimen-
sion in this multifaceted planning landscape. Effec-
tive districting can pave the way towards minimizing
costs, enhancing capacity utilization, elevating patient
Castillo, P., Bucarey, V., Davila, S. and Quezada, F.
Balancing Resources and Demand: A Bi-Objective Mixed-Integer Programming Approach of Healthcare Districts in Chile.
DOI: 10.5220/0012410100003639
Paper published under CC license (CC BY-NC-ND 4.0)
In Proceedings of the 13th International Conference on Operations Research and Enterprise Systems (ICORES 2024), pages 341-349
ISBN: 978-989-758-681-1; ISSN: 2184-4372
Proceedings Copyright © 2024 by SCITEPRESS – Science and Technology Publications, Lda.
341

satisfaction, and, importantly, embedding equity into
the accessibility of healthcare services across the so-
ciety (Cort
´
es et al., 2018; R
´
ıos-Mercado, 2020). In
general, several criteria are considered in the literature
for planning of healthcare systems, including Popu-
lation Homogeneity, which seeks to minimize devi-
ations in population size, medical expenditure, or the
proportion of elderly individuals in each district. Pop-
ulation Homogeneity or balancing is one of the most
common objectives in healthcare districts as well as
Compactness, which aims to minimize patients’ travel
time inside a district and Contiguity that is defined as
the ability to move between territorial units within a
district without leaving the district. Other criteria in-
clude, for example, Capacity-Demand Match, which
imposes penalties for unmet demand or tries to mini-
mize excess of demand over available capacity; or Va-
riety of Medical Procedures, where each district must
ensure a number of basic procedures.
This research spotlight focuses on unraveling the
healthcare districting problem, specifically in the con-
text of the City of Santiago, Chile. In recent years,
this city has experienced a surge in population den-
sity, which has concurrently escalated the burden on
healthcare centers. This increased load is notably ev-
ident in the lengthening waiting lists for surgical and
medical consultations (del Gobierno de Chile, 2023).
One hypothesis suggests that a suboptimal distribu-
tion of resources across healthcare centers may be a
latent root cause. By re-evaluating and potentially
re-engineering the allocation of communes within the
City of Santiago relative to the current distribution,
a more balanced and potentially more efficient dis-
tribution of resources, aligned with the demands of
the growing population, might be achieved. Thus, ad-
dressing the Healthcare Districting problem emerges
as a potential strategy to design districts that harmo-
nize population and resource distributions, aiming for
a seamless and equitable healthcare experience for all.
The article is organized as follows. In Section 2,
a review of the relevant literature for the problem of
Primary and Secondary Healthcare Districting is pre-
sented. The problem description and a mathematical
formulation to solve it is introduced in Section 3. Sec-
tion 4.1 showcases the case study along with its re-
spective computational results and discussion. Con-
clusions and further research work are discussed in
Section 5.
2 RELATED WORKS
Different approaches and techniques have been ap-
plied to the healthcare districting problem to meet de-
sirable attributes of the geographical partition, such
as population balance and resource distribution. Two
pioneer works in the area are the one of Ghiggi et
al. (1975) and Pezzella et al. (1981). The for-
mer laid down several key assumptions for districting
the healthcare system, such as the idea that regions
are composed of indissoluble communities with cen-
tralized populations, geographical connectivity of the
districts, and balance of district populations. Their
overarching goal was to devise a hybrid method for
districting, ensuring each district’s self-sufficiency
concerning health systems while satisfying planners
and citizens alike. Pezzella et al. (1981) presents a
two-step methodology for partitioning a given geo-
graphical area, ensuring an optimal allocation of the
available healthcare services. The first step consists
of determining an optimal partition by taking into ac-
count the demand and capacity of each territorial unit.
Then, in the second step, the first partition is aggre-
gated into new partitions by considering the lower and
upper bounds for the population in each district.
In addition, a crucial aspect that multiple studies
have highlighted is the consideration of multiple ob-
jective functions. Datta et al. (2013) emphasizes geo-
graphical compactness, alignment with existing local
authorities, and size and population homogeneity. On
a similar note, Steiner et al. (2015) looked at optimiz-
ing population homogeneity, medical procedure vari-
ety per district, and intradistrict distances in a study
in Brazil. Meanwhile, Yanık et al. (2020) introduced
the innovative concept of gradual assignment. Here,
demands could be split among neighboring districts,
enriching their multi-period, multi-criteria model.
In terms of approaches employed to solve the
healthcare districting problem, both exact and heuris-
tic methods have been observed. However, recogniz-
ing the NP-Hard nature and computational intractabil-
ity of the problem, several researchers have turned to
heuristic and metaheuristic algorithms. Notably, Gray
Wolf Optimizer and Antlion Optimizer algorithms
were implemented in Farughi et al. (2019). These ap-
proaches find resonance in the works of Farughi et al.
(2020) that also used the Gray Wolf Optimizer heuris-
tic and compared its performance with an improved
genetic algorithm. Additionally, genetic algorithms to
solve single- and multi-objective healthcare district-
ing problems have also been investigated in Datta et
al. (2013) and Steiner et al. (2015).
The complexity of the problem and the introduc-
tion of newer dimensions like stochastic demand have
led to innovative solutions. A robust optimization
approach is investigated in Darmian et al. (2022),
whereas Fan and Xie (2022) adopted a two-stage dis-
tributionally robust optimization approach consider-
ICORES 2024 - 13th International Conference on Operations Research and Enterprise Systems
342

ing the unpredictability of demand, especially rele-
vant in the backdrop of the pandemic and vaccination
drives.
The application of these methodologies and ap-
proaches is best understood through real-world case
studies. Van Minh et al. (2014) assessed the capa-
bilities of a primary healthcare system in a district,
encompassing both physical and human resources,
in a rural city in central Vietnam. Steiner et al.
(2015) shows the application of a multi-objective op-
timization approach for dealing with a real-world
spatial problem of aggregating the municipalities of
the Parana State in Brazil into some microregions.
Farughi et al. (2019) and Farughi et al. (2020) demon-
strated their model in the South Khorasan Province
of Iran, offering insights into practical implications.
Yanık et al. (2020) applied its multi-criteria and
multi-period formulation with the concept of grad-
ual assignment to Istanbul, Turkey. Lastly, among
the recent studies, Darmian et al. (2022) not only in-
troduced a model considering contiguity and popula-
tion balance but also factored in demand uncertainty,
showcasing its practicality for a real-world case study
of Iran’s healthcare system.
This work is closely related to previous research
on districting, as it considers several relevant fea-
tures of the healthcare districting problem simultane-
ously. However, most studies focus on maximizing
population homogeneity and/or compactness, treating
other features such as capacity-demand match as con-
straints or service levels to be satisfied. In this work,
we aim to minimize the largest excess of population
across different healthcare levels over the available
resources in the forming districts, while considering
population homogeneity, compactness, and contigu-
ity as constraints that must be met. Table 1 provides a
summary of pertinent information from selected stud-
ies, including this work.
3 PROBLEM DESCRIPTION AND
MATHEMATICAL
FORMULATION
In this section, we provide a formal definition of
the problem and mathematical formulation that con-
sider several attributes discussed in the literature, such
as population balance, compactness, contiguity, and
capacity-demand match.
3.1 Problem Definition and Notation
We first formally describe the healthcare districting
problem faced in this article.
The districting problems involve grouping a set of
territorial units to form a district. This can be done for
various purposes, such as administrative or political
reasons. Territorial units represent individual parts of
the territory that structure spatial organization. The
main objective is to establish the assignment of ter-
ritorial units to districts. These units have a certain
allocation of resources. The objective of the district-
ing problem in this article is to establish a territorial
partition, which minimizes the maximum excess of
demand over capacity among all districts for primary
and secondary healthcare services individually.
To achieve this objective, we formulate this prob-
lem as a mixed-integer program based on the span-
ning tree formulation. This formulation allows us to
impose the connectivity of territorial units into a dis-
trict explicitly. Note that a spanning tree of an undi-
rected graph is a subgraph in which any two vertices
are connected by exactly one path and includes all of
the vertices of the graph. Let V be the set of ver-
tices, which represent the territorial units, defined as
V = {1, 2,3,.. ., |V |}. Let E be the set of edges, im-
plying that if there exists an edge between vertex i and
j, then {i, j} ∈ E.
The model requires an auxiliary graph G(V
′
,E
′
),
where the set of nodes corresponds to the territorial
units, with an additional node {0}, given by V
′
=
{0} ∪ V . The set of edges represents border relation-
ships, and the 0 node is adjacent to each territorial
unit. Thus, E
′
= E ∪ {{0,i} | ∀i ∈ V }. Moreover, we
define a set A of directed edges derived from E, along
with the directed edges emerging from node 0. This is
given by A = {(i, j),( j,i) | {i, j} ∈ E} ∪ {(0,i) | i ∈
V }. The population for each territorial unit is denoted
as p
j
for all j ∈ V . Similarly, the resources for each
territorial unit j are denoted by r
p
j
(resp. r
t
j
) and rep-
resent the number of people served by the primary
(resp. secondary) medical supplies within that unit.
Meanwhile, the distance between a pair of territorial
units (i, j) is represented by d
i j
.
Additionally, we restrict the number of territorial
units in each district to fall within an interval (s
1
,s
2
),
preventing too many or too few territorial units in
each district. In addition, a maximum distance L
max
is
imposed between any two territorial units that belong
to the same district. This condition, know as compact-
ness, seeks to avoid generating districts with a terri-
tory too large. Thus, the model aims to find K disjoint
territory subsets that minimize the largest excess of
population over the resources capacity among the K
Balancing Resources and Demand: A Bi-Objective Mixed-Integer Programming Approach of Healthcare Districts in Chile
343
Table 1: Selected publications on the healthcare districting problem in primary and secondary healthcare services.
Attributes
Article
Population
Homogeneity
Compactness Contiguity Accessibility
Capacity-demand
Match
Variety of Medical
Procedures Offered
Case
study
1 (Ghiggi et al., 1975) x x x
Province of
Imperia Italy
2 (Pezzella et al., 1981) x x x x
Province of
Cosenza Italy
3 (Datta et al., 2013) x x x
East
England
4 (Steiner et al., 2015) x x x
Parana
State, Brazil
5 (Farughi et al., 2019) x
South Khorasan
Province, Iran
6 (Farughi et al., 2020) x x x x
South Khorasan
Province, Iran
7 (Yanık et al., 2020) x x x x x
Istanbul,
Turkey
8 (Fan and Xie, 2022) x x
-
9 (Darmian et al., 2022) x x x x
Iran
10 This work x x x x
Metropolitan Region
of Santiago, Chile
districts.
It is worth noting that, within the general con-
ditions of the healthcare districting problem for par-
titioning the geographical area, each district d ∈
K = {1, .. ., K} forms a subgraph G
d
. Together, they
should cover the entire set V . These conditions are
expressed as follows:
V
d
̸=
/
0 d ∈ K (1)
V
d
∩ V
d
′
≡
/
0 d, d
′
∈ K , d ̸≡ d
′
(2)
V
1
∪ V
2
∪ ... ∪ V
K
≡ V (3)
3.2 Spanning Tree-Based MIP Model
In this section, we present the Mixed Integer Pro-
gramming (MIP) formulation of the healthcare dis-
tricting problem.
Firstly, we define the variables involved in the
model, described as follows:
• Let x
i j
∈ {0,1} be a binary variable where x
i j
= 1
if edge {i, j} ∈ E
′
is part of the spanning tree of
G that determines the solution, and x
i j
= 0 other-
wise.
• Let y
i jk
∈ {0, 1} be a binary vector such that y
i jk
=
1 if arc (i, j) ∈ A is used to define the connectivity
between the node 0 and territory k, where k ∈ V ,
and y
i jk
= 0 otherwise.
• Let η
p
and η
t
be the continuous variables that
quantify the maximum excess of the population
primary and secondary service capacity, respec-
tively, over all districts.
The mathematical formulation is presented as fol-
lows:
min βη
p
+ (1 − β)η
t
(4)
subject to:
∑
i∈V
x
0i
= K (5)
∑
(i, j)∈E
′
x
i j
= |V
′
| − 1 (6)
∑
(0,i)∈A
y
0ik
= 1 ∀k ∈ V
(7)
∑
(i, j)∈A
y
i jk
−
∑
( j,i)∈A
y
jik
= 0 ∀ j,k ∈ V : i ̸= j
(8)
∑
( j,k)∈A
y
jkk
= 1 ∀k ∈ V
(9)
x
i j
≥ y
i jk
+ y
jik
∀(i, j) ∈ E
′
,∀k ∈ V
(10)
∑
k∈V
(p
k
− r
p
k
)y
0 jk
≤ η
p
∀ j ∈ V
(11)
∑
k∈V
(p
k
− r
t
k
)y
0 jk
≤ η
t
∀ j ∈ V
(12)
¯
Px
0 j
−
∑
k∈V
p
k
y
0 jk
≤ α
¯
P ∀ j ∈ V
(13)
−
¯
Px
0 j
+
∑
k∈V
p
k
y
0 jk
≤ α
¯
P ∀ j ∈ V
(14)
s
1
x
0 j
≤
∑
k∈V
y
0 jk
≤ s
2
x
0 j
∀ j ∈ V
(15)
ICORES 2024 - 13th International Conference on Operations Research and Enterprise Systems
344

(y
0 jk
+ y
0 ji
)d
ki
≤ L
max
∀ j,i,k ∈ V : i ̸= k
(16)
x
i j
∈ {0,1} ∀{i, j} ∈ E
′
(17)
y
i jk
∈ {0,1} ∀(i, j) ∈ A,∀ k ∈ V
(18)
The objective function (4) aims to minimize the
maximum gap between resources and population
among all districts. Note that the parameters β al-
low us to adjust the objective function to focus on
minimizing the excess at the primary healthcare level
(β = 1), at secondary healthcare level (β = 0) or at
both levels at the same time (β ∈]1, 0[). Constraint
(5) establishes the number of districts to be formed.
It is done by limiting the number of edges that can
be connected to node 0. Constraints (6) ensure that
the number of edges active in a solution defines a
spanning tree in the auxiliary graph. Constraints (7)-
(10) entails that a path must exist between each node
k ∈ V and the node 0. Constraints (11)-(12) quan-
tify the excess of the population over the available re-
sources in each district for the primary and secondary
healthcare services. Constraints (13)-(14) entail that
the population assigned to each district can only de-
viate an α value from the mean population. Con-
straints (15) ensure that each district has a number of
territorial units between the discrete interval (s
1
,s
2
).
Constraints (16) impose that the distance between
any two territorial units belonging to the same district
must be at most L
max
. Finally, the domain of the deci-
sion variables is represented in Constraints (17)-(18).
Figure 1 illustrates the method for deriving a solu-
tion to the healthcare districting problem via the span-
ning tree approach. Observing the figure from left to
right, the initial step involves converting a given in-
stance of the problem into a preliminary graph. This
graph represents the territorial units as nodes and their
adjacency as edges; that is, an edge is drawn between
any two neighboring territorial units to signify their
connection. Subsequently, in the central figure, an
auxiliary graph is constructed by linking each node
to an additional, artificial node. The constraints de-
lineated by (7) to (10) are then applied to identify a
path from each node k ∈ V to the artificial node 0.
This step ensures that each territorial unit is allocated
to a district. Moreover, the number of active edges
connected to node 0 is restricted by the predetermined
number of districts to be established. Consequently, a
node k that does not serve as a district center must be
connected to node 0 via a path that traverses through a
sequence of neighboring nodes, which are also inter-
connected. This results in a cohesive cluster of nodes,
thereby fulfilling the contiguity requirement for the
districts.
In the next section, we apply the model (4)-(18) to
the Metropolitan region of Santiago of Chile and seek
to analyze how well the current geographical parti-
tion regarding the present population and available re-
sources at each territorial unit.
4 COMPUTATIONAL RESULTS
In this section, we assess the solutions provided by the
formulation (4)-(18) at solving a real instance based
on the Metropolitan region of Santiago, Chile.
4.1 Case Study
The Metropolitan region of Santiago, Chile, as per
the census conducted in 2017, has a total population
of 7,112,808 residents spanning an area of 15,403
km
2
. This equates to a density of 461.7 inhabitants
per square kilometer. Demographically, the region
is divided into 52 municipalities, which are grouped
into six provinces: Chacabuco, Cordillera, Maipo,
Melipilla, Santiago, and Talagante. However, when
it comes to health administration, the structure is
different. As stipulated by the Ministry of Health,
the region is segmented into six distinct health-
care services, which are: North Metropolitan Health
Service (North); Western Metropolitan Health Ser-
vice (West);Central metropolitan health service (Cen-
tral); Eastern Metropolitan Health Service (East);
South Metropolitan Health Service (South); South-
East Metropolitan Health Service (South-East). Var-
ious types of healthcare services are located within
these health services. Consequently, different lev-
els are established, leading to the following organi-
zational structure for the establishments:
• Primary Healthcare Centers: They are charac-
terized by being the first point of contact with the
patient. Thus, they aim to provide high-quality
initial outpatient care to identify the ailment. The
facilities that offer these services include:
• Secondary Healthcare Centers: This pertains to
emergency hospital care and inpatient hospitaliza-
tion, which includes complex surgical procedures.
Hospitals responsible for providing this service
have high, medium, and low levels of complexity.
Based on the definition above, this research focuses
on proposing new districts that take into account
the capacities of both primary and secondary health-
care levels. The primary level, which includes Fam-
ily Healthcare Centers (abbreviated as CESFAM in
Balancing Resources and Demand: A Bi-Objective Mixed-Integer Programming Approach of Healthcare Districts in Chile
345
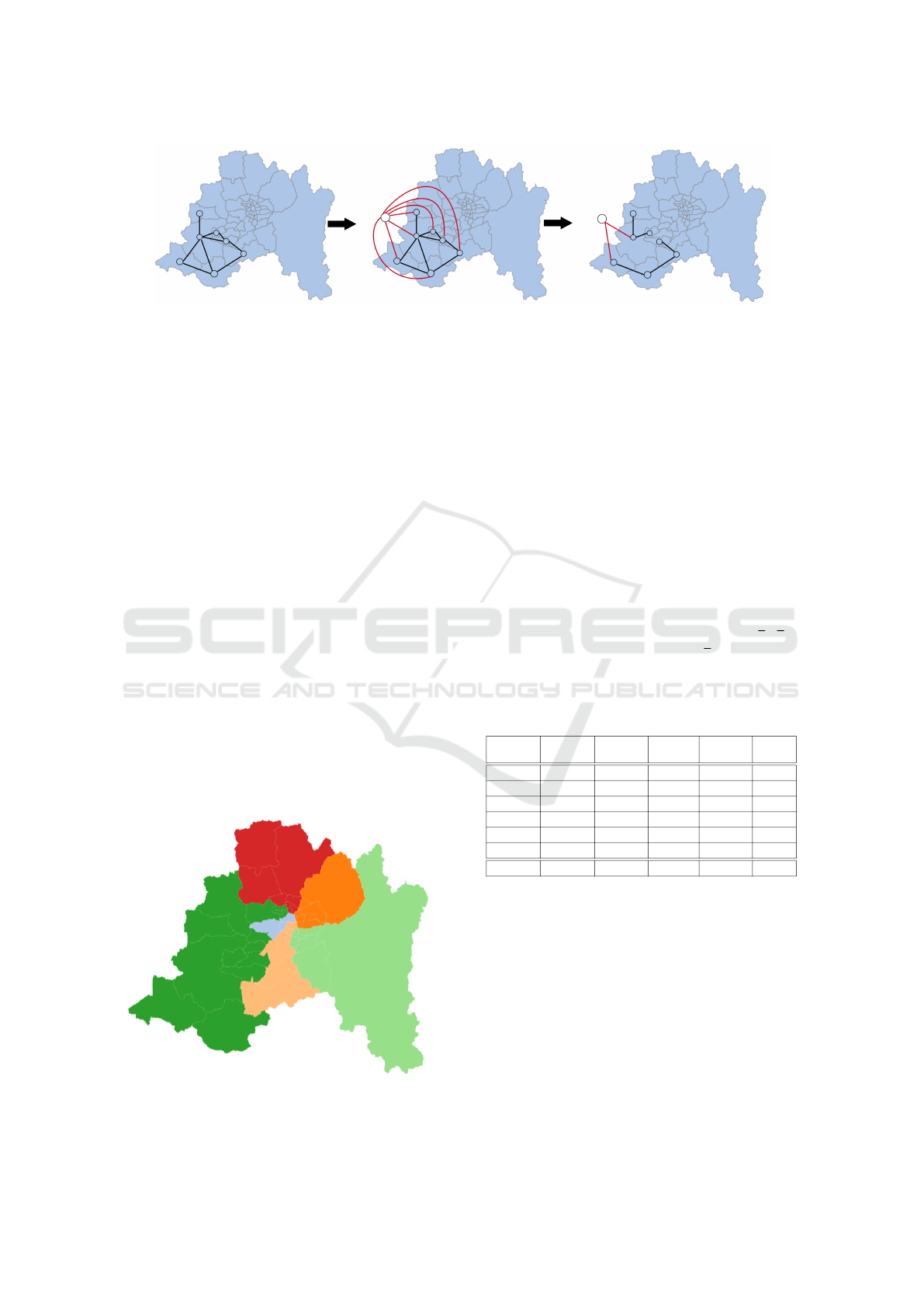
Figure 1: A solution of the healthcare districting problem represented as a spanning tree.
Spanish), plays a vital role in alleviating congestion
in secondary service levels, such as hospitals.
We gathered the information for this case study
from sources within the Ministry of Health and na-
tionally certified surveys, such as the Census con-
ducted in 2017 to determine the population in each
municipality. The Metropolitan Region of Santiago
currently has 22 secondary healthcare centers and
171 primary healthcare centers. The Ministry of
Health mandates that each primary (resp., secondary)
care center should be assigned at most 30,000 (resp.,
100,000) people, representing its capacity to provide
healthcare services. However, this number is only an
approximation of the actual capacity of each center
and does not consider the heterogeneity of the cen-
ters and their efficiency in providing services. To
address this issue, we assume that the capacity of
each center follows a discrete uniform distribution
U((1−ε)
¯
d, (1+ε)
¯
d), where
¯
d represents the assigned
capacity and ε = 0.1 (resp., ε = 0.2) for primary
(resp., secondary) care centers. The lower and up-
per bounds for the number of territorial units in each
district, i.e., (s
1
,s
2
), are set to 4 and 15, respectively.
We select each parameter in the formulation by
considering the current geographical partition and its
characteristics. This ensures that the current solution
Figure 2: Current districts of the health care services in the
Metropolitan region of Santiago.
is indeed a feasible solution to formulation (4)-(18).
This consideration is crucial as the primary aim of
this research is to ascertain whether, under the pre-
vailing conditions and regulations of the Metropolitan
region’s healthcare system, there exists an improved
geographical partition that can diminish the popula-
tion excess over the current system’s capacity. By do-
ing so, this could partially alleviate the stress on the
existing system and reduce both the waiting list and
wait times.
Figure 2 displays the current districts stipulated by
the Ministry of Health, and Table 2 shows the com-
position of population and resources of each district
as well as their excess of population over their avail-
able capacity in the primary and secondary level. The
MAPD line stands for Median Absolute Percentage
Deviation, which is calculated as (
∑
n
t
|x
t
− x|/x)/n,
where x
i
represents the ith data and x denotes the av-
erage value of the n data set.
Table 2: Current composition of healthcare services in the
Metropolitan region of Santiago.
District Population
Secondary
Capacity
Primary
Capacity
Secondary
Excess
Primary
Excess
Central 1,153,995 206,227 550,238 947,768 603,757
East 1,216,177 303,286 695,714 912,891 520,463
South 1,151,126 519,389 1,051,794 631,737 99,332
West 1,202,137 590,346 1,117,597 611,791 84,540
South East 1,356,538 363,570 974,520 992,968 382,018
North 961,721 224,287 766,596 737,434 195,125
MAPD 18.05% 39.03% 35.97% 23.23% 92.15%
4.2 Experimental Setup
The mixed-integer linear programming formulation
(4)-(18) was implemented in Python 3.11 and solved
using GUROBI 10.0.1 with the default settings. All
tests were run on the computing infrastructure of the
Universidad de Santiago de Chile, which consists of
a Lenovo ThinkStation machine with 12th genera-
tion Intel Core i7-12700. We set the machine to use
four 3.60GHz cores and 31GB RAM to solve each in-
stance. We impose a time limit of 43,200 seconds (12
hours) to solve the same instance with three different
ICORES 2024 - 13th International Conference on Operations Research and Enterprise Systems
346
values of the parameter β ∈ {0,0.5,1}.
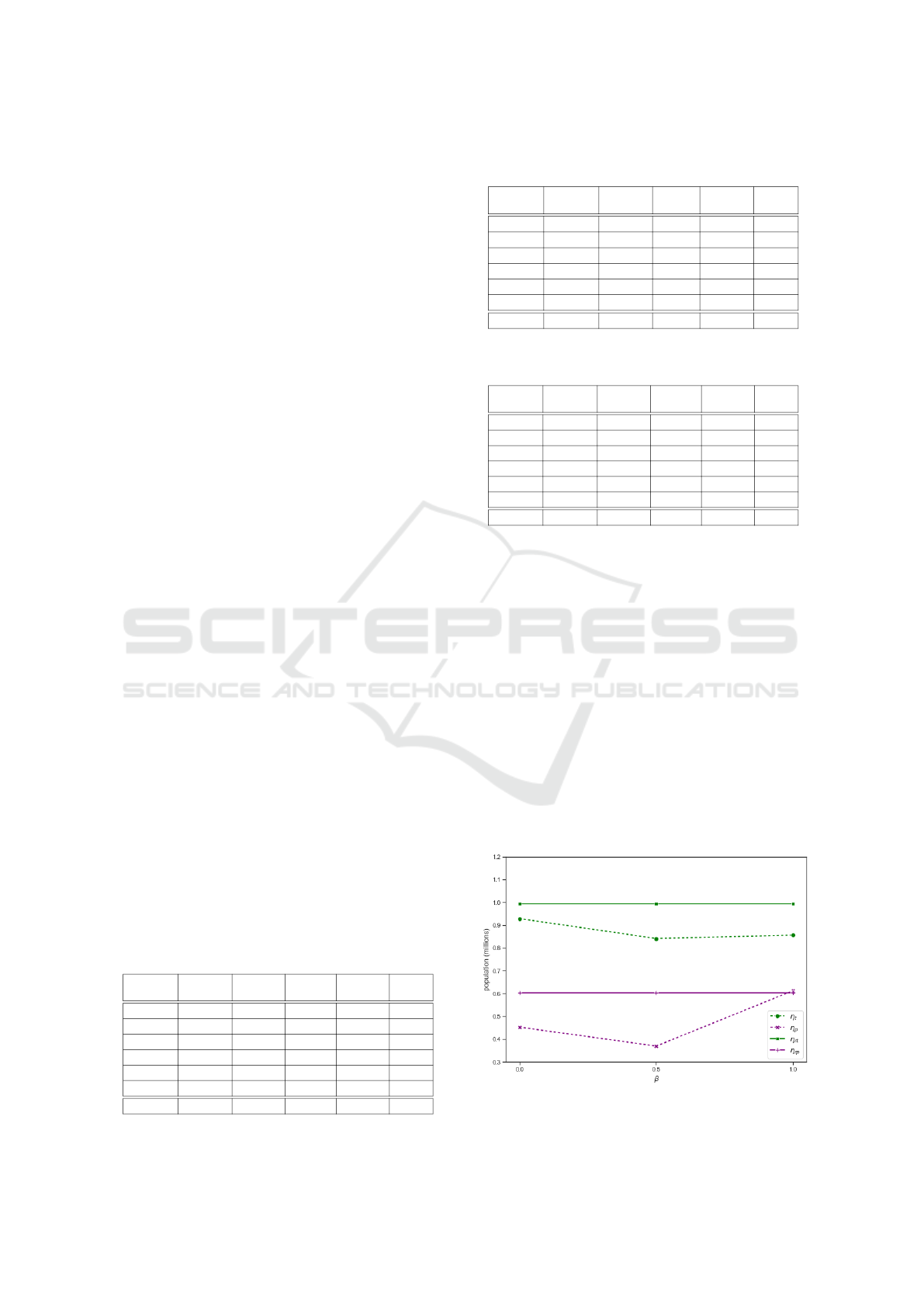
4.3 Results
Tables 3-5 and Figure 4-6 display the results obtained
for each value of β ∈ {0.0,0.5, 1.0}. Recall that β
determines which healthcare services are a priority
to minimize the overall population surplus concern-
ing its medical offer. When β = 0.0, the emphasis
is solely on the primary healthcare level (β = 1.0).
When β = 1.0, the focus is on the secondary level, Fi-
nally, with β = 0.5, there is a balanced consideration
of both the total exceeding of both the primary and
secondary healthcare level.
Table 3 (β = 1) shows a reduction of 25.07% in
the largest excess of population over resources at the
primary healthcare level, decreasing from 603,757 to
452,258 people. In addition to this reduction, Ta-
ble 3 also indicates a decrease in the largest abso-
lute deviation as a percentage among districts regard-
ing the excess of population over resources at the pri-
mary healthcare level, from 92.15% to 83.13%. These
positive results are also partially observed at the sec-
ondary healthcare level, where the largest excess of
population over resources is reduced from 992,968 to
928,651 people (6.48%). However, the largest mean
absolute deviations as a percentage at the secondary
healthcare level increases from 23.23% to 32.31%,
leading to a reduction in the homogeneity of resource
distribution among districts.
In Table 5 (β = 0), we observe that the largest ex-
cess of the population over resources is reduced from
992,968 to 856,352 people (13.76%), and the largest
mean absolute deviation as a percentage among dis-
tricts is reduced from 23.23% to 13.38%. Nonethe-
less, these improvements come with a slight increase
in the largest excess of population over resources at
the primary healthcare level, rising from 603,753 to
612,519 people (1.45%), and an increase in the largest
mean absolute deviation as a percentage of 2.79%
(from 92.15% to 94.94%). This results in a deteri-
oration of the homogeneity in the distribution of re-
sources at the primary healthcare level.
Table 3: Composition of healthcare services in the
Metropolitan region of Santiago with β = 1.
District Population
Secondary
Capacity
Primary
Capacity
Secondary
Excess
Primary
Excess
Central 1,341,551 486,207 889,183 855,344 452,368
East 953,995 109,457 509,841 844,538 444,154
South 1,402,653 611,261 1,147,692 791,392 254,961
West 1,011,354 412,323 958,347 599,031 53,007
South-East 1,179,203 363,570 822,923 815,633 356,280
North 1,152,938 224,287 828,473 928,651 324,465
MAPD 19.52% 70.24% 40.68% 32.31% 83.13%
Table 4: Composition of healthcare services in the
metropolitan region of Santiago with β = 0.5.
District Population
Secondary
Capacity
Primary
Capacity
Secondary
Excess
Primary
Excess
Central 1,281,187 492,453 950,799 788,734 330,388
East 1,066,277 303,286 696,645 762,991 369,632
South 1,199,911 395,434 967,622 804,477 232,289
West 1,239,516 427,337 983,002 812,179 256,514
South-East 1,094,376 269,316 735,223 825,060 359,153
North 1,160,427 319,279 823,168 841,148 337,259
MAPD 9.17% 33.9% 18.94% 5.31% 26.07%
Table 5: Composition of healthcare services in the
metropolitan region of Santiago with β = 0.
District Population
Secondary
Capacity
Primary
Capacity
Secondary
Excess
Primary
Excess
Central 1,254,276 397,924 641,757 856,352 612,519
East 1,130,793 303,286 665,257 827,507 465,536
South 1,354,982 519,389 1,233,226 835,593 121,756
West 1,202,137 504,195 1,117,597 697,942 84,540
South-East 1,152,682 363,570 793,088 789,112 359,594
North 946,824 118,741 705,534 828,083 241,290
MAPD 19.3% 67.72% 43.50% 13.38% 94.94%
Results in Table 4 (β = 0.5) equate the importance
of the primary and secondary healthcare level in the
objective function. This results in the decrease of both
maximum absolute deviations as a percentaje. For
the case of the secondary healthcare level, this goes
from 23.23% to 5.31%, while at the primary health-
care level, it decreases from 92.15% to 26.07%. On
the other hand, considering the largest excess of popu-
lation over available resources compared to the initial
case, these decrease from 992,968 to 841,148, result-
ing in a reduction of 15.28% for secondary healthcare
level; meanwhile, the excess for primary healthcare
level goes from 603,757 to 369,632, decreasing by
38.77%.
Table 6 and Figure 3 summarize the results for
each value of β. In the case that the decision maker
is more interested in minimizing the largest excess in
Figure 3: Capacity-demand match at primary and secondary
levels according to different values of β.
Balancing Resources and Demand: A Bi-Objective Mixed-Integer Programming Approach of Healthcare Districts in Chile
347
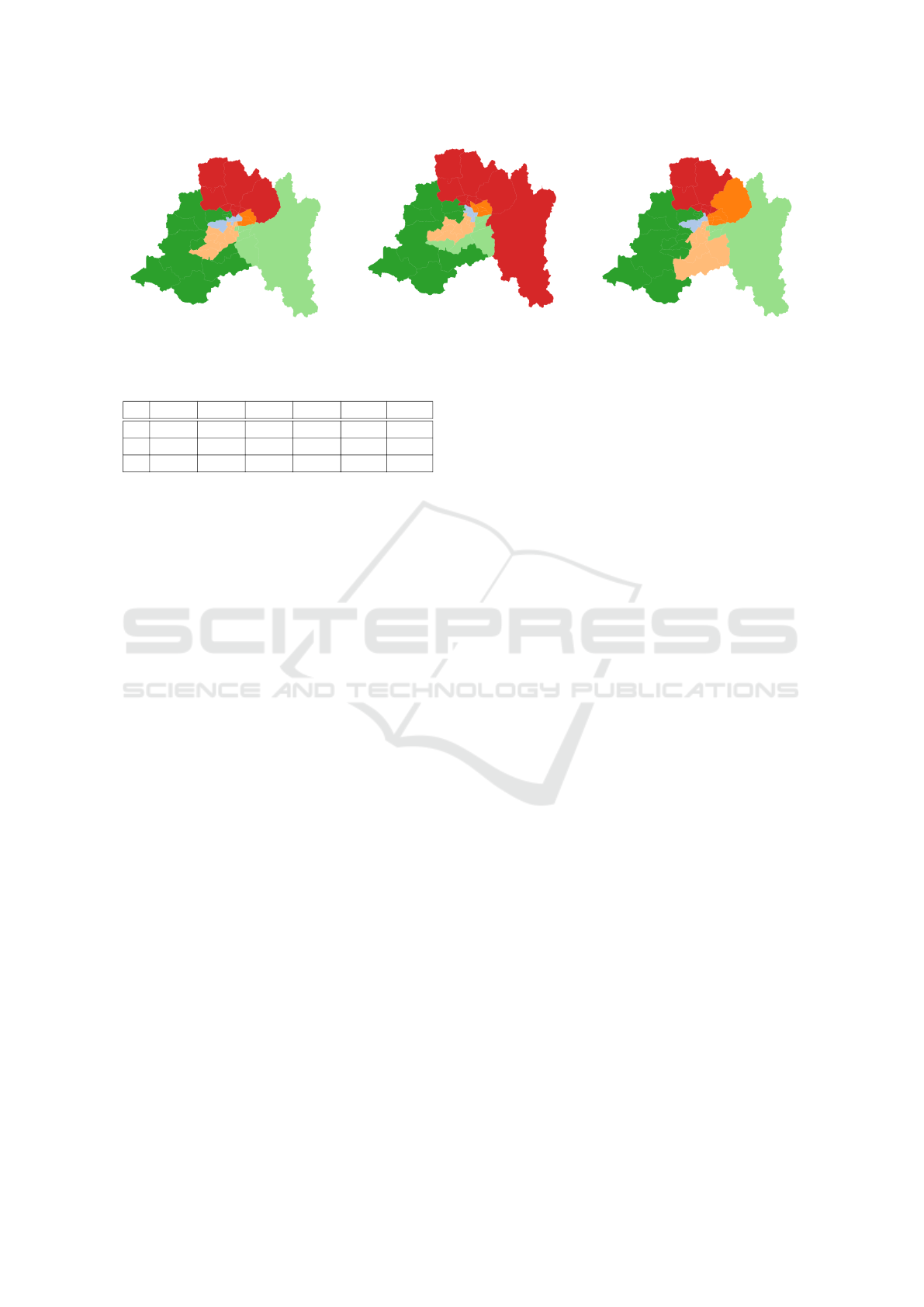
Figure 4: Obtained districts with β = 1.
Figure 5: Obtained districts with β =
0.5.
Figure 6: Obtained districts with β = 0.
Table 6: Summary of results for each value of β.
β η
t
η
p
η
rt
η
rp
Gap
t
Gap
p
1 928,651 452,368 992,968 603,757 6,48% 25,07%
0.5 841,148 369,632 992,968 603,757 15.29% 38.78%
0 856,352 612,519 992,968 603,757 13,76% -1,45%
the primary healthcare level (β = 1), the results sug-
gest that it is possible to achieve an improvement of
up to 25%, i.e., reduce up to 25% the largest excess of
the population over the available resources. However,
this will have an impact on the secondary healthcare
level, which might increase their largest mean abso-
lute deviation as a percentaje by 10%. In the opposite
case, if the decision maker is more interested in mini-
mizing the largest excess in the secondary healthcare
level (β = 0), the results suggest that it is possible to
achieve an improvement of almost up to 14%, how-
ever, as it is expected, an increase in the largest excess
of the primary healthcare level of 1,45% is reported.
In that case, both healthcare levels are considered si-
multaneously in the objective function, i.e., β = 0.5,
the results suggest an improvement in both levels, pri-
mary and secondary healthcare levels. The former
might reduce the largest excess up to 15%, while the
latter might be reduced up to almost 39%. These re-
sults suggest that these decisions must not be taken
independently, and considering both healthcare lev-
els at the same time might provide a more efficient
geographical partition of the Metropolitan region of
Santiago in terms of balance between population and
available resources. It is worth noticing that the dif-
ference between the improvements in the secondary
(resp. primary) healthcare level using β = 0.5 and
β = 0 (resp. β = 1) might be explained due to the for-
mulation (4)-(18) could not find an optimal solution
within the imposed time limit. More specifically, the
optimality gaps reported after the 12 hours of compu-
tation were 58.5% for β = 1, 44.7% for β = 0.5 and
44.4% for β = 0.
5 CONCLUSIONS
The geographical partitioning of healthcare services
is a fundamental pillar for ensuring efficient and eq-
uitable healthcare delivery. This research focuses on
the City of Santiago, Chile, and sheds light on the
complex issue of healthcare districting, a combina-
torial optimization problem that, when addressed ef-
ficiently, can bring transformative improvements to
healthcare service delivery.
Our study illustrates the intricate balancing act
required between primary and secondary healthcare
levels. Through mathematical modeling, we have
demonstrated that a conscientiously designed district-
ing plan can play a pivotal role in harmonizing the
healthcare journey for patients, from their initial en-
counters with primary care to more advanced care
needs. The complex interplay between population ho-
mogeneity, compactness, and capacity-demand match
emerges as the cornerstone of this optimization prob-
lem.
Relying on a variety of methodologies, rang-
ing from exact solutions to heuristic approaches, re-
searchers have made commendable progress in ad-
dressing the healthcare districting problem. In our
study, we consider a mixed-integer linear program-
ming formulation with a bi-objective function assess-
ing equity at two layers of the health service system
(namely, primary and secondary). We represent and
assess three scenarios and explore the implications
of prioritizing primary, secondary, or both healthcare
levels. Our findings underscore that considering both
levels of healthcare simultaneously can lead to a more
balanced geographic partitioning in terms of aligning
population demand with available resources.
Results indicate significant potential for improve-
ments. Specifically, for a balanced approach, the
largest excesses of population over available re-
sources could be reduced by up to 15.29% and
38.78% for secondary and primary healthcare levels,
respectively. While optimizing for a particular level
ICORES 2024 - 13th International Conference on Operations Research and Enterprise Systems
348

offers specific benefits, it can have consequential ef-
fects on the other level. Thus, decision-makers are
tasked with judiciously evaluating trade-offs.
The intricate nature of this problem, coupled with
the computational challenges encountered during op-
timization, implies that more efficient algorithms or
hybrid methodologies could further improve the solu-
tion quality found in this work.
A logical extension of the current study would
be to consider a range of medical specialties, which
would offer a more comprehensive view of health-
care needs across the city. Alongside this, there is
a clear need to refine and enrich the data concerning
actual demand and the healthcare system’s capacity.
Enhancing data collection and analysis can provide
more accurate insights and lead to better-informed
decisions about resource allocation and distribution.
One strong underlying assumption of this work is that
primary healthcare resources are homogeneously dis-
tributed across districts; however, given the geograph-
ical location of primary centers and district sizes, it is
unrealistic to assume that people can attend any center
within their district. This issue should be addressed
by considering a more realistic model, such as a two-
level districting problem or an integrated approach
that might consider decisions on the location and ca-
pacity of new primary centers. Furthermore, an area
that warrants particular focus is determining the opti-
mal number of districts required to meet healthcare
demands. Pursuing this additional research would
provide a critical perspective for long-term planning
and expansion decisions.
Regarding the modeling approach, there is an ev-
ident requirement to embrace a more dynamic ap-
proach that factors in demand shifts over time and ac-
knowledges the inherent variability in healthcare ca-
pacity. Such dynamic models would render a more
realistic representation of healthcare system needs
and behaviors. To further strengthen this analysis, it
would be valuable to delve into advanced optimiza-
tion techniques such as robust optimization and inte-
grated approaches. These methodologies could gener-
ate more resilient solutions in the face of uncertainties
and help identify optimal locations for future medical
centers.
REFERENCES
Cort
´
es, S., Guti
´
errez, E. V., Palacio, J. D., and Villegas, J. G.
(2018). Districting decisions in home health care ser-
vices: Modeling and case study. In Applied Computer
Sciences in Engineering: 5th Workshop on Engineer-
ing Applications, WEA 2018, Medell
´
ın, Colombia,
October 17-19, 2018, Proceedings, Part II 5, pages
73–84. Springer.
Darmian, S. M., Fattahi, M., and Keyvanshokooh, E.
(2022). An optimization-based approach for the
healthcare districting under uncertainty. Computers
& Operations Research, 135:105425.
Datta, D., Figueira, J., Gourtani, A., and Morton, A.
(2013). Optimal administrative geographies: An al-
gorithmic approach. Socio-Economic Planning Sci-
ences, 47(3):247–257. Health Care Modelling.
del Gobierno de Chile, O. (2023). Ministerio de salud,
cuenta p
´
ublica 2023. Technical report, Government
of Chile.
Fan, Z. and Xie, X. (2022). A distributionally robust opti-
misation for covid-19 testing facility territory design
and capacity planning. International Journal of Pro-
duction Research, 60(13):4229–4252.
Farughi, H., Mostafayi, S., and Arkat, J. (2019). Healthcare
districting optimization using gray wolf optimizer and
ant lion optimizer algorithms (case study: South kho-
rasan healthcare system in iran). Journal of Optimiza-
tion in Industrial Engineering, 12(1):119–131.
Farughi, H., Tavana, M., Mostafayi, S., and Santos Arteaga,
F. J. (2020). A novel optimization model for design-
ing compact, balanced, and contiguous healthcare dis-
tricts. Journal of the Operational Research Society,
71(11):1740–1759.
Ghiggi, C., Puliafito, P. P., and Zoppoli, R. (1975). A com-
binatorial method for health-care districting. In IFIP
Technical Conference on Optimization Techniques,
pages 116–130. Springer.
Lin, H.-Y. and Kao, J.-J. (2008). Subregion districting anal-
ysis for municipal solid waste collection privatization.
Journal of the Air & Waste Management Association,
58(1):104–111.
Pezzella, F., Bonanno, R., and Nicoletti, B. (1981). A sys-
tem approach to the optimal health-care districting.
European Journal of Operational Research, 8(2):139–
146.
R
´
ıos-Mercado, R. Z. (2020). Optimal districting and terri-
tory design, volume 284. Springer.
R
´
ıos-Mercado, R. Z. and L
´
opez-P
´
erez, J. F. (2013).
Commercial territory design planning with realign-
ment and disjoint assignment requirements. Omega,
41(3):525–535.
Steiner, M. T. A., Datta, D., Neto, P. J. S., Scarpin, C. T., and
Figueira, J. R. (2015). Multi-objective optimization in
partitioning the healthcare system of Parana State in
Brazil. Omega, 52:53–64.
Validi, H. and Buchanan, A. (2022). Political districting
to minimize cut edges. Mathematical Programming
Computation, 14(4):623–672.
Yanık, S., Kalcsics, J., Nickel, S., and Bozkaya, B. (2020).
A multi-period multi-criteria districting problem ap-
plied to primary care scheme with gradual assignment.
International Transactions in Operational Research,
26(5):1676–1697.
Balancing Resources and Demand: A Bi-Objective Mixed-Integer Programming Approach of Healthcare Districts in Chile
349
