
The Beyond 5G (B5G) Era of Next-Generation Digital Networks:
Preliminary Study of a Task-Technology Fit (TTF) Model for Remote
Robotic Surgery Applications
Maradona C. Gatara
1
, Mjumo Mzyece
2
and Sijo J. Parekattil
3,4
1
Independent Researcher, South Africa
2
Business & Economics Department, Northwestern College, Orange City, Iowa, U.S.A.
3
College of Medicine, University of Central Florida, Florida, U.S.A.
4
Avant Concierge Urology, Winter Garden, Florida, U.S.A.
Keywords: Beyond 5G (B5G), Task-Technology Fit (TTF), Predictive Modelling, Haptic-Enabled Internet of Skills
(IoS), Remote-Robotic Surgery Applications, Human-in-the-Loop (HITL), Minimally Invasive Surgery
(MIS), Health Informatics.
Abstract: The coming Beyond 5G (B5G) era could mark a paradigm shift towards user-centric Quality of Experience
(QoE) centred network architectures. The infusion of QoE user requirements into network architectures will
be crucial for future ultra-reliable, ultra-low latency haptic-enabled Internet applications. One such application
will be the mission-critical use case of remote (tele-haptic) robotic surgery, signifying a transition towards
skillset delivery networks that will augment user task performance experience. In extending traditional
Quality of Service (QoS)-oriented networks to user focused QoE and with it, Quality of Task (QoT)
components, human users in a global control loop (such as robotic surgeons) will be capable of true-to-life
immersive remote task performance through the manipulation of objects in real-time, and of transcending
geographical distance. In this preliminary study using data elicited from 20 practising robotic surgeons (n =
20), we examine the emergence of a future B5G network and haptic-enabled Internet of Skills (IoS)
architecture, applied to the task-sensitive mission-critical use case of remote (tele-haptic) robotic surgery. We
conceptualise and demonstrate the use of non-linear Task-Technology Fit (TTF) predictive modelling to
empirically assess this futuristic use case, and in doing so, provide a novel QoE/QoT perspective of future
B5G communication networks.
1 INTRODUCTION
The emergence of Beyond 5G (B5G) networks such
as 6G networks (Giordani et al., 2020) and quantum
communication networks (Bassoli et al., 2021) offer
much promise. These digital networks of the future
will transcend the limits of current 5G network
technologies (Nawaz et al., 2019). Originally, the
traditional Internet was envisaged as a global
computer network, signifying a paradigm shift in 20
th
century economies (Shapiro & Varian, 1999). This
era brought forth the revolutionary Mobile Internet,
connecting billions of devices and computers,
disrupting whole 21
st
century economies and
industries (Dohler, 2018). In the present day, the
Internet of Things (IoT), predicted to tether trillions
of smart devices and positioned to redefine industries
of the coming decade, has come to the fore. These
Internets will, however, be overtaken by the
emergence of a haptic-enabled Internet whereby
highly responsive secure networks will support the
rendition of real-time haptic impulses remotely. This
would amplify the capacities of the IoT by
introducing a new element to human-machine
interaction via the development of immersive real-
time communications technologies (Pierucci, 2015).
In future Internets, haptics will take the form of two
key attributes: the transmission of touch and actuation
in real-time will extend traditional audio-visual
feedback of current systems via the support of both
tactile (cutaneous) and kinaesthetic modalities.
Firstly, the tactile (cutaneous) modality would render
data on the dimensions of surface, texture, and
friction. Secondly, the kinaesthetic modality would
relay data on force, torque, position, and velocity
112
Gatara, M., Mzyece, M. and Parekattil, S.
The Beyond 5G (B5G) Era of Next-Generation Digital Networks: Preliminary Study of a Task-Technology Fit (TTF) Model for Remote Robotic Surgery Applications.
DOI: 10.5220/0012384400003657
Paper published under CC license (CC BY-NC-ND 4.0)
In Proceedings of the 17th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2024) - Volume 2, pages 112-122
ISBN: 978-989-758-688-0; ISSN: 2184-4305
Proceedings Copyright © 2024 by SCITEPRESS – Science and Technology Publications, Lda.
dimensions. With these transmission modes, human
users would be linked to remote environments with
more immersion. The sensations of sight and sound
augmented by audio-visual rendition and the
transmission of haptic impulses would be bi-
directional. Hence, touch would be detected by
imposing motion on an environment with feeling
rendered through a distortion or reactionary force.
Haptics will become critical to future Internet archite-
ctures with the emergence of the B5G era. A future
haptic-enabled Internet will shift conventional Quality
of Service (QoS) performance-related indicators
towards more dynamic, interactive and human-user-
centred Quality of Experience (QoE) and Quality of
Task (QoT) considerations (Gatara & Mzyece, 2023).
2 REMOTE ROBOTIC SURGERY
APPLICATIONS FOR
TELE-HAPTIC SURGICAL
TASK PERFORMANCE
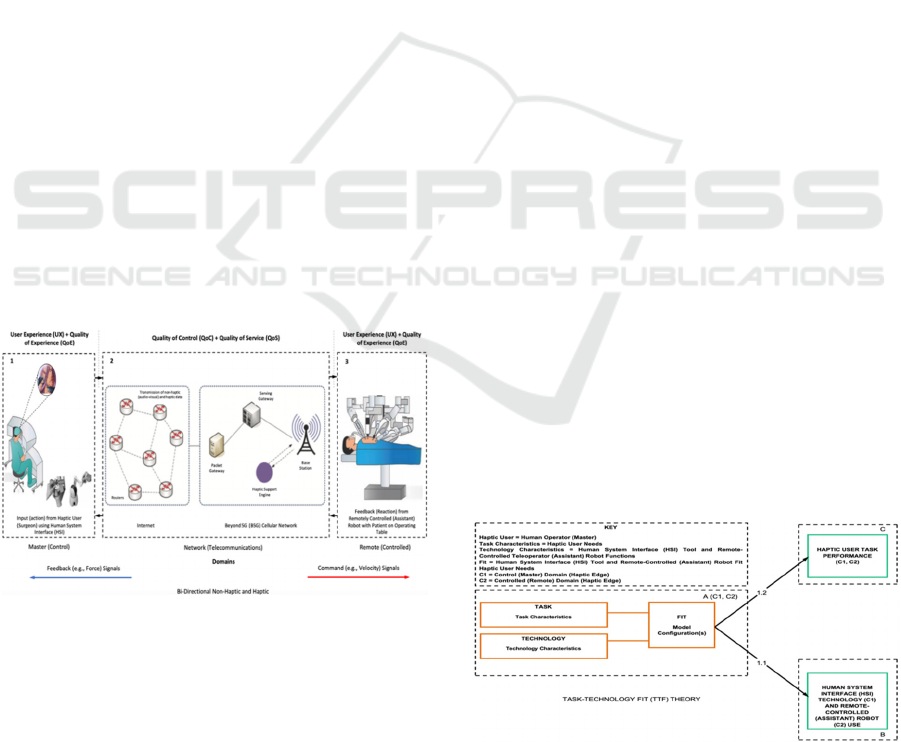
B5G networks will enable the future Internet of Skills
(IoS) (Dohler, 2018). The performance of real-time
tele-haptic robotic surgery tasks is a mission-critical
application that leverages the ultra-reliable and ultra-
low latency requirements that will become
synonymous with B5G networks of the future. To
envision the connection between QoS, QoT, and QoE
components of a haptic-enabled IoS architecture, we
present this robotic telesurgery use case in Figure 1.
Figure 1: Haptic-Enabled Internet of Skills (IoS) for Tele-
Haptic Surgical Task Performance in Beyond 5G (B5G)
Networks.
In this scenario, a robotic surgeon with the
requisite expertise will be the Human-in-the-Loop
(HITL) supported to perform tele-haptic surgery
tasks. A master (control) and assistant surgical robot
in a remote-controlled environment must be
connected through a reliable high-speed
communication network to render real-time control
commands and multi-modal sensory data. This
enhanced form of tele-haptic surgery will require
high-precision manipulation and meet stringent
latency, jitter, and packet-loss metrics. Therefore,
future B5G networks will be expected to more
consistently and reliably ensure the ultra-low latency
and ultra-reliable characteristics necessary for
seamless two-way haptic feedback. On this basis, in a
future Internet, surgeons will be able to extend their
physical skillsets over remote geographical distances
via a B5G-supported telecommunications network.
Consequently, current shortages of surgeons and high-
quality surgical care, and long-distance limitations in
travel would be greatly reduced. Furthermore, surgical
precision and patient safety would be enhanced.
3 TASK-TECHNOLOGY FIT
(TTF) THEORY AND
PREDICTVE MODELLING
FOR REMOTE ROBOTIC
SURGERY APPLICATIONS
The theoretical construct of Task-Technology Fit
(TTF) denotes the measurement of the degree to
which the functional capacity of a tool or system is
adequate for user needs or requirements (Goodhue,
1995; Dishaw & Strong, 1998). The theory of TTF
can be traced to the earlier theories of Cognitive Fit,
which suggests that effective, efficient problem
solving relies on matching characteristics of problem
representation and problem task (Vessey, 1991, 1994;
Vessey & Galleta, 1991), and Task-System Fit, which
is “the fit between task requirements and the
functionality of the IS [Information Systems]
environment” (Goodhue, 1992). A TTF conceptual
model of a haptic-enabled IoS is proposed and
illustrated in Figure 2 (Gatara et al., 2021).
Figure 2: Conceptual Task-Technology Fit (TTF) Model
for Quality of Experience (QoE) with Quality of Task
(QoT) Perspective of a Haptic-Enabled Internet of Skills.
The Beyond 5G (B5G) Era of Next-Generation Digital Networks: Preliminary Study of a Task-Technology Fit (TTF) Model for Remote
Robotic Surgery Applications
113
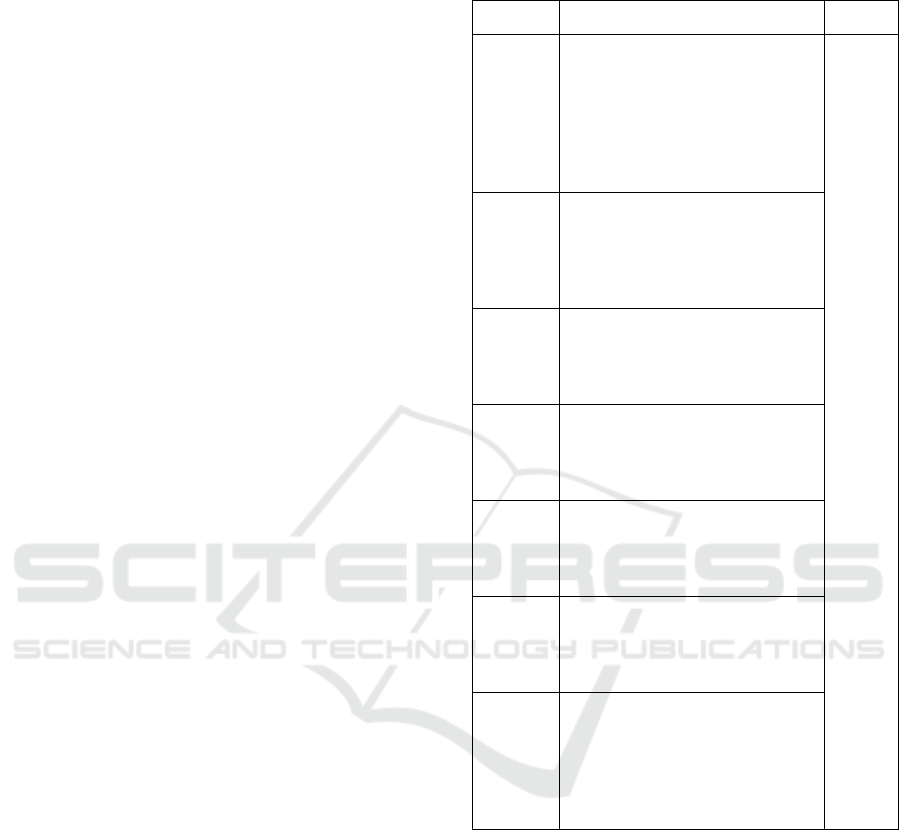
The model in Figure 2 links task and technology
characteristics in (i) the master (control) domain and
(ii) the remote (controlled) domains. First, task
characteristics denote the most critical needs of the
human technology user. User needs can be specified
as surgeons’ most critical task demands in remote
robotic surgery (tele-haptic surgical task
performance).
To perform critical minimally invasive robotic
surgery tasks (grasping, palpation, and incision), the
user (surgeon) concurrently uses (i) a manipulator
(hand controller) and touch haptic device (remote
controller) as part of the Human System Interface
(HSI) in the master (control) domain and (ii)
manipulators (grasper, palpation probe, and end-
effector tip (cutter)) in the remote (controlled)
domain.
4 INSTRUMENT SCALE (ITEM)
MEASURES FOR
TASK-TECHNOLOGY FIT
(TTF) MODEL VARIABLES
The Task-Technology Fit (TTF) model developed for
this research links task and technology characteristics
in (i) the master (control) domain and (ii) the remote
(controlled) domains.
First, task characteristics denote the most critical
needs of the human technology user (Nance, 1992).
User needs can be specified as surgeons’ most critical
task demands in remote robotic surgery (tele-haptic
surgical task performance). For example, these
include (i) control movement (motion) of remote
assistant robotic arms (telemanipulators) e.g. to
manipulate a needle drive (end effector) tool (surgical
instrument) with wrist-like movements (1A), (ii)
visualisation (with magnification) of the operative
(surgical) field (area) e.g. for immersive stereoscopic
view and endoscopic three-dimensional (3-D) High-
Definition (HD) imaging (2A), and (iii) feeling and
control of grasping force when operating on patient
e.g. to displace tender organs (retraction) and soft
tissue (clutching) (3A). The items used to measure
these dimensions are detailed in Table 1.
Second, technology characteristics denote critical
support functions for the most critical needs of the
task performer (human user) (Dishaw et al., 2002).
For example, there are critical corresponding support
tools used by the surgeon including (i)
interchangeable needle driver (end effector) tool
(surgical instrument) attached to a lateral robotic arm
with functional support i.e. movement up to 7
Table 1: Measurement Items for the Task (Characteristics)
Construct (TC).
Variable Scale Item Source
TC 1A Control movement (motion) of
remote assistant robotic arms
(telemanipulators) e.g. to
manipulate a needle driver (end
effector) tool (surgical
instrument) with wrist-like
movements.
Saracino
et al.
(2019),
Yang et
al.
(2013)
TC 2A Visualisation (with magnification)
of the operative (surgical) field
(area) e.g. for immersive
stereoscopic view and endoscopic
3-D HD imaging.
TC 3A Feel and control grasping force
when operating on patient e.g. to
displace tender organs (retraction)
and soft tissue (clutching).
TC 4A Palpation manoeuvres when
operating on patient e.g. to detect
neoplastic lesions in solid organs
(hollow viscus).
TC 5A Incision (dissection) when
operating on patient e.g. to cut
soft tissue without damaging
embedded vessels and nerves.
TC 6A Suturing when operating on
patient e.g. to insert needle
(puncture tissue), loop the suture
thread (stitch), and tie the knot.
TC 7A Feel and reproduce true-to-life
(realistic) haptic feedback when
operating on patient e.g. to sense
kinaesthetic (force/joint-related)
and vibrotactile (cutaneous/skin-
related) sensations.
Degrees of Freedom (DoF) (1B), (ii)
digitalstereoscopic camera (optic lens) with
progressive magnification up to 15 times (15x) (2B),
and (iii) interchangeable grasper tool (surgical
instrument) attached to a lateral robotic arm with
functional support i.e. laparoscopic forceps (5mm,
37cm) or fenestrated-grasper (3B). These identified
corresponding task (user need) and technology
(support function) characteristics (A and B pairs) will
be measured using five seven (7)-point Likert
measures on a scale from 1 (= to an extremely small
extent) to 7 (= to an extremely large extent) (Yang et
al., 2013). The items used to measure these
dimensions are detailed in Table 2.
HEALTHINF 2024 - 17th International Conference on Health Informatics
114
Table 2: Measurement Items for the Technology
(Characteristics) Construct (TC).
Variable Scale Item Source
TC 1B Control movement (motion) of
remote assistant robotic arms
(telemanipulators) e.g. via
interchangeable needle drive (end
effector) tool (surgical instrument)
attached to lateral robotic arm with
functional support i.e. movement up
to 7 DoF.
Saracino
et al.
(2019),
Yang et
al.
(2013)
TC 2B Visualisation (with magnification)
of the operative (surgical) field
(area) e.g. digital stereo scoping
camera (optic lens) attached to
lateral robotic arm with functional
support i.e. progressive
magnification up to 15x.
TC 3B Feel and control grasping force
when operating on patient e.g. Feel
and control grasping force when
operating on patient e.g. via
interchangeable grasper tool
(surgical instrument) attached to
lateral robotic arm with functional
support i.e. laparoscopic forceps
(5mm, 37cm) or fenestrated grasper.
TC 4B Palpation manoeuvres when
operating on patient e.g. via
interchangeable
laparoscopic/ultrasound probe tool
(surgical instrument) attached to
lateral robotic arm with functional
support i.e. single-use and
disposable with cross-section of less
than 15 x 10 mm (diameter of 5 to
12 mm).
TC 5B Incision (dissection) when operating
on patient e.g. via interchangeable
end-effector tip (cutter) tool
(surgical instrument) attached to
lateral robotic arm i.e. sterile Carbon
steel blade.
TC 6B Suturing when operating on patient
e.g. via interchangeable needle
driver (end-effector) tool (surgical
instrument) attached to lateral
robotic arm i.e. on CT-2 needles cut
to 6 inches (for placement 0-Vicryl
sutures).
TC 7B Feel and reproduce true-to-life
(realistic) haptic feedback when
operating on patient e.g. via force-
sensing for multiple degrees of
motion and force-awareness
(combined) i.e. sigma.7 haptic
(master) interface
(kinaesthetic/vibrotactile feedback).
The Use construct in Table 3 reflects the extent to
which the task performer has come to depend on the
technology tool and its support functions (Thompson
et al., 1991; Igbaria et al., 1997; Junglas et al., 2009).
Table 3: Measurement Items for the Use (Dependence)
Construct (UD).
Variable Scale Item Source
UD 1
I am very dependent on the use
hand telemanipulators (finger
controllers) to perform tasks
using robotic arms (with
attached surgical tools e.g.
needle driver).
Saracin
o et al.
(2019),
Yang et
al,
(2013)
UD 2 My work is highly dependent on
the use of hand telemanipulators
(finger controllers) to perform
tasks using robotic arms (with
attached surgical tools e.g.
probe).
UD 3 The use of hand
telemanipulators (finger
controllers) to perform tasks
using robotic arms (with
attached surgical tools e.g.
cutter) allows me to do more
than would be possible without
them.
The User Performance construct in Table 4 on the
other hand reflects the effectiveness, efficiency, and
quality with which tasks are completed using the
technology and its support functions to perform the
most critical tasks needed (Hiltz & Johnson, 1990;
Torkzadeh & Doll, 1999; Hou, 2012).
Five seven (7)-point Likert measures on a scale
from 1 (= to an extremely small extent) to 7 (= to an
extremely large extent) measure the Use and User
Performance outcomes resulting from the “Fit”
between Task and Technology characteristics
depicted in Figure 3. The presence of this “Fit” is
essential for optimal use and user performance
(Nance, 1992).
Figure 3: The Fit between Task and Technology
Characteristics.
The Beyond 5G (B5G) Era of Next-Generation Digital Networks: Preliminary Study of a Task-Technology Fit (TTF) Model for Remote
Robotic Surgery Applications
115
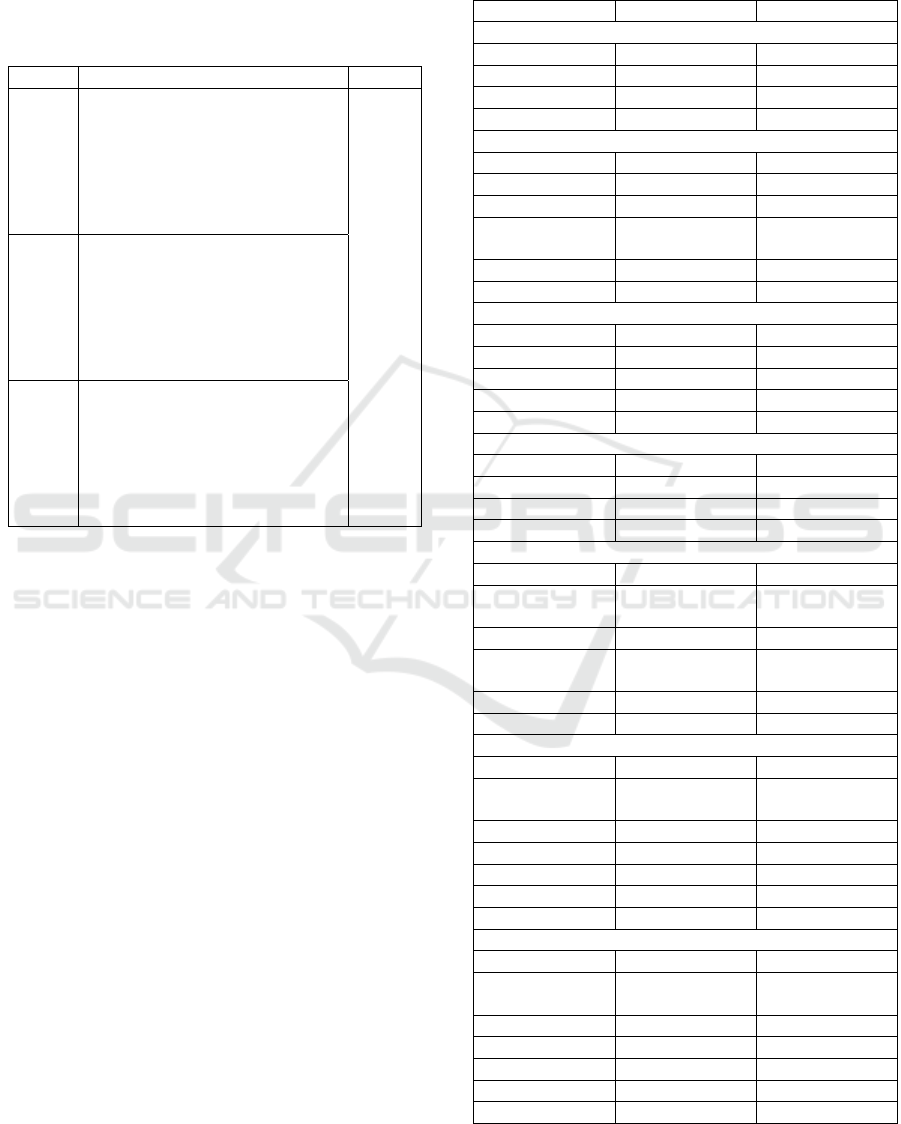
Thus, task-technology fit (TTF) is examined for its
effects on Use and User Performance. The specific
items used to measure these dimensions are detailed
in Table 3 (above) and Table 4 (below).
Table 4: Measurement Items for the User Performance
Construct (UP).
Variable Scale Ite
m
Source
UP 1 The hand telemanipulators (finger
controllers) I use to control
assistant robot and perform tasks
using robotic arms (with attached
surgical tools e.g. grasper)
increases my productivity (easier
task execution
)
.
Saracino
et al
(2019),
Yang et
al (2013)
UP 2 The hand telemanipulators (finger
controllers) I use to control
assistant robot and perform tasks
using robotic arms (with attached
surgical tools e.g. probe) increases
my productivity (time reduction in
task com
p
letion
)
.
UP 3 The use of hand telemanipulators
(finger controllers) to perform
tasks using robotic arms (with
attached surgical tools e.g. optic
lens) decreases errors, increasing
quality (capability enhancement in
task execution).
5 DATA COLLECTION AND
DEMOGRAPHIC USER
PROFILE OF RESPONDENTS
We collected preliminary data from 20 practising
robotic surgeons (n = 20) via an electronic (online)
survey designed to elicit user responses.
There were 19 male users (95%) and 1 female user
(5%), mostly aged 51 years and above (40%) and
between 46 and 50 years (35%). There were 18 right-
handed dominant users (90%), plus 1 left-handed user
(5%) and 1 ambidextrous user (5%). Additionally, 17
robotic surgeons (85%) were trained as Senior
Faculty versus 3 as Junior Faculty (15%). Also, most
of the robotic surgeons (65%) were reported to have
undergone more than 10 simulator hours.
Furthermore, 9 users (45%) were reported to have
expert microsurgery experience, whereas 4 users
(20%) were proficient. A further 11 users (55%) had
expert robotic experience, whereas at least 7 robotic
surgeons (35%) were expert-level laparoscopic
practitioners. Notably, 5 users (25%) reported
proficient videogame experience. The respondent
user demographic profile for this preliminary cohort
of practising robotic surgeons (n = 20) is provided in
Table 5.
Table 5: Respondent User Demographic Profile (n = 20).
Variable(s) Frequenc
y
Percent (%)
Gender
Male 19 95%
Female 1 5%
Total 20 200%
Missing 0 0%
Age
36-40 years 3 15%
41-45
y
ears 2 10%
46-50
y
ears 7 35%
51 years and
above
8 40%
Total 20 100%
Missin
g
00%
Hand Dominance
Right-Hande
d
18 90%
Left-Hande
d
15%
Ambidextrous 1 5%
Total 20 100%
Missin
g
00%
Training Level
Junior Facult
y
3 15%
Senior Facult
y
17 85%
Total 20 100%
Missin
g
00%
Simulator Hours
None 2 10%
Less than 5
Hours
2 10%
6
–
10 Hours 3 15%
More than 10
Hours
13 65%
Total 20 100%
Missing 0 0%
Microsurgery Experience
Novice 4 20%
Advanced
Beginne
r
0 0%
Competent 3 15%
Proficient 4 20%
Ex
p
ert 9 45%
Total 20 100%
Missing 0 0%
Robotic Experience
Novice 1 5%
Advanced
Beginne
r
1 5%
Competent 4 20%
Proficient 3 15%
Ex
p
ert 11 55%
Total 20 100%
Missing 0 0%
HEALTHINF 2024 - 17th International Conference on Health Informatics
116
Table 5: Respondent User Demographic Profile (n = 20)
(cont.).
Variable(s) Frequenc
y
Percent (%)
Laparoscopic Experience
Novice 6 30%
Advanced
Beginne
r
1 5%
Competent 4 20%
Proficient 2 10%
Ex
p
ert 7 35%
Total 20 100%
Missin
g
0 0%
Videogame Experience
Novice 6 30%
Advanced
Beginne
r
3 15%
Competent 4 20%
Proficient 5 25%
Ex
p
ert 2 10%
Total 20 100%
Missin
g
0 0%
6 MEASUREMENT
INSTRUMENT (CONSTRUCT)
RELIABILITY AND VALIDITY
A Partial Least Squares Structural Equation
Modelling (PLS-SEM) algorithm was run to estimate
parameters of measurement model constructs.
Confirmatory Factor Analysis (CFA) was conducted
to test construct measures for their internal
consistency, convergent, and discriminant validities.
PLS-SEM functions efficiently with small sample
sizes and attains high statistical power levels with
small sample sizes even when the data is non-
parametric or highly skewed (Hair et al., 2021), such
as the preliminary sample (n = 20) used for
preliminary nature of analysis in this study.
Composite Reliability (p
c
) scores for the dimensions
of Task, Technology, Use, and User Performance were
satisfactory. Composite Reliability (p
c
) ranged from
0.000 to 1.000, with higher values indicating higher
levels of reliability (Hair et al., 2021). In more advanced
research however, values between 0.700 and 0.900 are
generally considered as satisfactory (Nunnally &
Bernstein, 1994; Hair et al., 2021). The composite
reliability scores for each latent Task, Technology, Use,
and User Performance dimensions were found to be
satisfactory (greater than 0.700). Thus, internal
consistent reliability was established.
The descriptive statistics for these four
dimensions are presented in Table 6.
Table 6: Descriptive Statistics.
Variable Range Mean SD Skewness Kurtosis
Tas
k
5.55 4.721 1.404 -0.189 0.127
Technology 6.00 4.173 1.578 0.073 0.014
Use 4.00 5.360 1.125 0.023 -0.502
User
Performance
6.20 5.391 1.466 -1.095 2.038
Further, the Average Variance Extracted (AVE)
values for each of the Task, Technology, Use, and
User Performance constructs exceeded the prescribed
threshold of 0.500 (Hair et al., 2021). Thus, results
also reflected acceptable convergent validity.
The Task, Technology, Use, and User
Performance constructs were also tested for their
discriminant validity.
First, their indicator cross-loadings were
evaluated. The outer loadings on all indicators on the
associated construct did not score higher than any of
its cross-loadings (correlations) on other constructs.
Therefore, discriminant validity was established.
Results of indicator cross-loadings are presented in
Table 7.
Table 7: Cross-Loadings.
Task Technol
o
gy
Use User
Performance
TaC1 0.705 0.383 0.216 -0.191
TaC2 0.732 0.587 0.407 -0.017
TaC3 0.867 0.732 0.253 0.210
TaC4 0.611 0.543 0.209 0.316
TaC5 0.793 0.511 0.358 0.170
TaC6 0.817 0.539 0.340 0.183
TaC7 0.845 0.778 0.283 0.101
TeC1 0.664 0.618 0.391 0.097
TeC2 0.602 0.761 0.444 0.194
TeC3 0.768 0.875 0.445 0.308
TeC4 0.661 0.819 0.308 0.476
TeC5 0.546 0.818 0.497 0.486
TeC6 0.584 0.854 0.549 0.324
TeC7 0.569 0.835 0.440 0.412
UDe1 0.429 0.285 0.618 0.245
UDe2 0.196 0.456 0.855 0.471
UDe3 0.410 0.556 0.935 0.518
UP1 0.141 0.273 0.565 0.883
UP2 0.214 0.474 0.484 0.964
UP3 0.203 0.045 0.224 0.116
Second, the Fornell-Larker Criterion was used to
further establish discriminant validity. The square
root of the AVE for each of the Task, Technology,
Use, and User Performance variables was higher than
correlations between these constructs and other latent
variables. Therefore, discriminant validity was
further established. Results of the Fornell-Larker
criterion valuation with the square root of the
The Beyond 5G (B5G) Era of Next-Generation Digital Networks: Preliminary Study of a Task-Technology Fit (TTF) Model for Remote
Robotic Surgery Applications
117
reflective constructs’ AVE on the diagonal, the means
and standard deviations of study constructs, and
correlations between the constructs in the off-
diagonal positions, are presented in Table 8.
Table 8: Fornell-Larker Criterion Results.
Mean
(SD)
Task Technology Use
User
Performance
Task
4.72
(1.40)
0.771
Technology
4.17
(1.58)
0.769 0.801
Use
5.36
(1.12)
0.398 0.552 0.814
User
Performance
5.39
(1.47)
0.181 0.431 0.529 0.758
Third, we further assessed discriminant validity using
the Heterotrait-Monotrait (HTMT) ratio of
correlations. Using HTMT as a criterion, all ratios
were found to be below the conservative threshold
value of 0.85, thus ascertaining the discriminant
validity of the Task, Technology, Use, and User
Performance measures. Results of the HTMT ratio
values for all pairs of constructs in the measurement
model are presented in Table 9.
Table 9: Heterotrait-Monotrait (HTMT) Ratio of
Correlations.
Task Technology Use
User
Performance
Tas
k
Technolog
y
0.868
Use 0.517 0.646
User
Performance
0.409 0.478 0.778
7 RESULTS: POLYNOMIAL
REGRESSION AND RESPONSE
SURFACE ANALYSIS
We modelled a relationship between Task and
Technology characteristics as independent variables
and Use and User Performance as dependent
variables, respectively, as a non-linear function. This
approach can have greater explanatory potential than
traditional moderated regression analyses. Moreover,
it can be used as an alternative method, as it outputs
more precise information on combinations
(interactions) of variables, beyond the results of more
conventional moderator analyses.
First, polynomial regression (Edwards, 1993) was
used to examine task and technology impacts on use
and user performance.
Latent variable scores obtained from PLS-SEM
analysis were used to compute Task (X) and
Technology (Y) characteristics, their interaction
(X*Y), and the quadratic terms (X
2
, Y
2
), in turn used
to predict Use and User Performance outcomes (Z) as
per the following polynomial equation [where b
n
denotes the respective beta coefficients for
corresponding X, Y, and Z terms, and e represents a
random disturbance term]:
Z = b
0
+ b
1
X + b
2
Y + b
3
X
2
+ b
4
XY + b
5
Y
2
+ e (1)
where:
Z = Use or User Performance
X = The Task
Y = The Technology
The above variables were centred at their
midpoints i.e. ‘4’ for 7-point Likert scales. Centring
is recommended for polynomial regression analyses
(Edwards, 1994). Further, Aiken and West (1991)
suggested that centering reduces the likelihood of
collinearity. With the above formula, coefficients for
the terms X (b
1
), Y (b
2
), X
2
(b
3
), XY (b
4
) and Y
2
(b
5
)
were obtained.
Table 10: Polynomial Regression Results (Use).
Use
Predictor
Beta (β)
Standard
Error
Constant (b
0
) 1.222*** 0.336
Task
(
b
1
X
)
-0.215 0.580
Technolo
gy
(
b
2
Y
)
0.541 0.516
Tas
k
2
(
b
3
X
2
)
0.067 0.288
Task*Technology (b
4
XY) -0.074 0.171
Technology
2
(b
5
Y
2
) 0.074 0.359
R
2
= 0.333, F = 1.399
Table 11: Polynomial Regression Results (User
Performance).
User Performance
Predictor
Beta (β)
Standard
Error
Constant (b
0
) 1.121*** 0.376
Task (b
1
X) -1.046 0.649
Technolo
gy
(
b
2
Y
)
0.925 0.577
Tas
k
2
(
b
3
X
2
)
0.475 0.322
Task*Technolo
gy
(
b
4
XY
)
-0.254 0.402
Technology
2
(b
5
Y
2
) 0.072 0.192
R
2
= 0.508, F = 2.896
Second, Response Surface Methodology (RSM)
(Edwards, 2002) was used to plot three-dimensional
(3D) surfaces relating Task and Technology to Use
and User Performance.
Regression beta (β) coefficients resulting from
equation (1) as presented in Tables 10 and 11 above,
HEALTHINF 2024 - 17th International Conference on Health Informatics
118
were used to estimate stationary points (X
0
, Y
0
),
principal axes (p
10
, p
11,
p
20,
p
21)
, and shapes along lines
of congruence and incongruence (a
1
, a
2
, a
3
, a
4)
.
Surface values for prediction of Use and User
Performance are shown in Tables 12 and 13.
Table 12: Response Surface Analysis Results (Use).
Use
Stationary
Point
X
0
-0.572
(
-0.014
)
Y
0
-3.941
(
-0.058
)
First Principal
Axis
Intercept (P
10
)
-4.570
(-0.064)
Slope (P
11
)
-1.099
(
-0.029
)
(-P
10
/(1+P
11
)
-46.138
(
-0.019
)
Second
Principal Axis
Intercept (P
20
)
-3.421
(-0.044)
Slope (P
21
)
0.910
(
0.030
)
Shape Along
Line of
Congruence (Y
= X)
Slope: a
1
(b
1
+
b
2
)
0.326
(
0.639
)
Curvature: a
2
(b
3
+ b
4
+ b
5
)
0.067
(0.350)
Shape Along
Line of
Incongruence
(Y = -X)
Slope: a
3
(b
1
-
b
2
)
-0.756
(-0.463)
Curvature: a
4
(
b
3
-
b
4
+ b
5
)
0.215
(
0.097
)
Table 13: Response Surface Analysis Results (User
Performance).
User Performance
Stationary
Point
X
0
-1.167
(-0.003)
Y
0
-8.481
-0.011
)
First Principal
Axis
Intercept (P
10
)
-8.818
(
-0.010
)
Slope (P
11
)
-0.289
(-0.018)
(-P
10
/(1+P
11
)
-46.138
(
-0.019
)
Second
Principal Axis
Intercept (P
20
)
-4.443
(
-0.014
)
Slope (P
21
)
3.462
(0.012)
Shape Along
Line of
Congruence (Y
= X)
Slope: a
1
(b
1
+
b
2
)
-0.121
(-0.177)
Curvature: a
2
(
b
3
+ b
4
+ b
5
)
0.293
(
1.124
)
Shape Along
Line of
Incongruence
(Y = -X)
Slope: a
3
(b
1
-
b
2
)
-1.971
(-0.993)
Curvature: a
4
(b
3
-
b
4
+ b
5
)
0.801
(0.234)
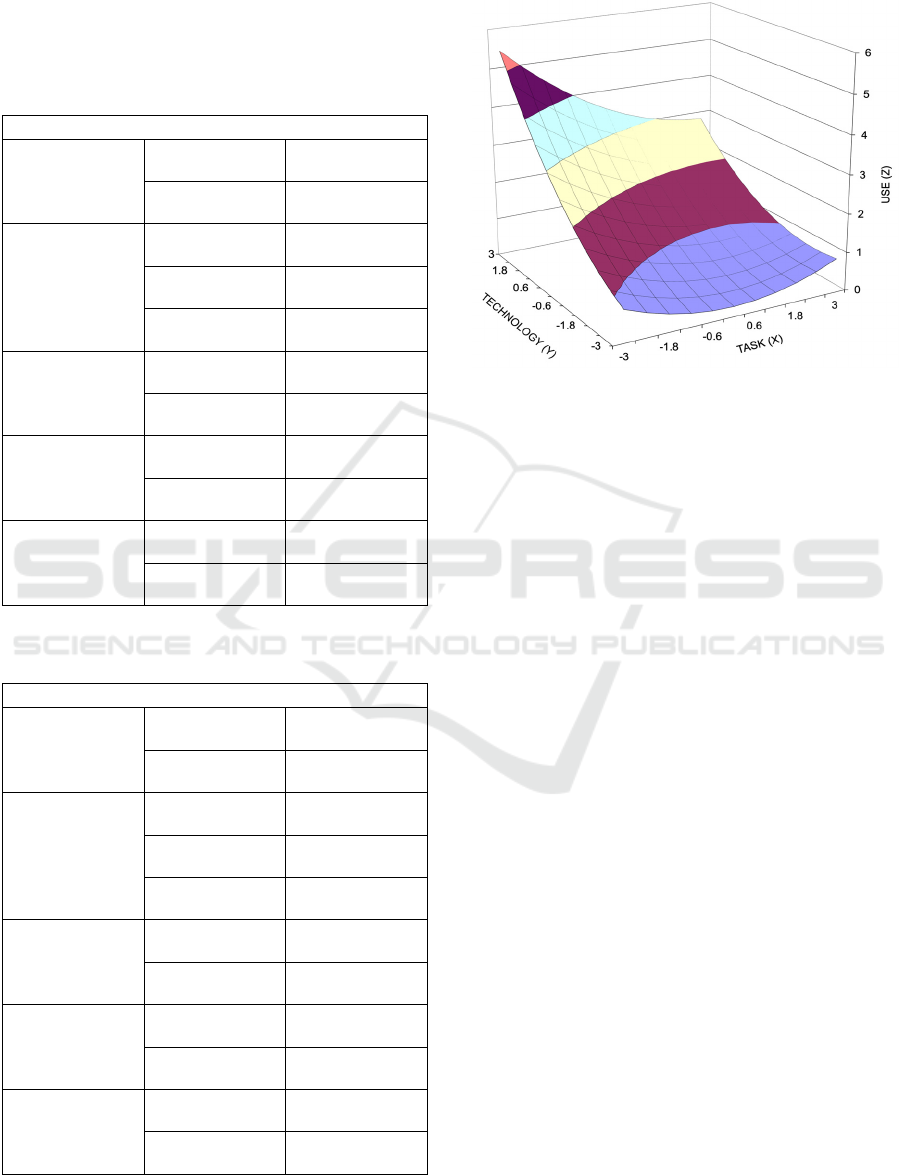
The response for the Task (X) and Technology
(Y) predicting Use (Z) is shown in Figure 4.
Figure 4: Response Surface for Task-Technology Fit (TTF)
and Use.
The response surface for TTF effects on use was
saddle-shaped (stationary point: X
0
= -0.572, Y
0
= -
3.941). The first principal axis is not significantly
different [t = -0.029 (P
11
), t = -0.019 (-P
10
//P
11
+1)]
from the line of congruence (Y = X). Thus, a perfect
fit between the Task and Technology leads to
maximal use. The upward slope along the line of
congruence (Y = X) was negative but not significant.
The curvature along the line of congruence (Y = X)
was positive but not significant (a
2
= 0.293, t = 1.124),
indicating that the relationship between TTF and use
is linear. Therefore, the curvature along the line Y =
X does not significantly change for use. The
downward slope along the line of incongruence (Y =
-X) was negative but not significant (a
3
= -1.971, t =
-0.993). A lack of fit between the robotic surgery task
and support tools leads to a decrease in use. The
curvature along the line of incongruence (Y = -X) was
positive but not significant (a
4
= 0.801, t = 0.234),
further evidencing a linear association between TTF
and use.
The response for the Task (X) and Technology
(Y) predicting User Performance (Z) is shown in
Figure 5.
The first principal axis is not significantly
different [t = -0.018(p
11
), t = -0.019(=p
10
/p
11+1
)] from
the line congruence (Y=X). Hence, a perfect fit
between the task and technology leads to maximised
user performance. The upward slope along the line of
congruence (Y=X) is negative and not significant (a
1
= -0.121, t = -0.177). The curvature along the line
The Beyond 5G (B5G) Era of Next-Generation Digital Networks: Preliminary Study of a Task-Technology Fit (TTF) Model for Remote
Robotic Surgery Applications
119
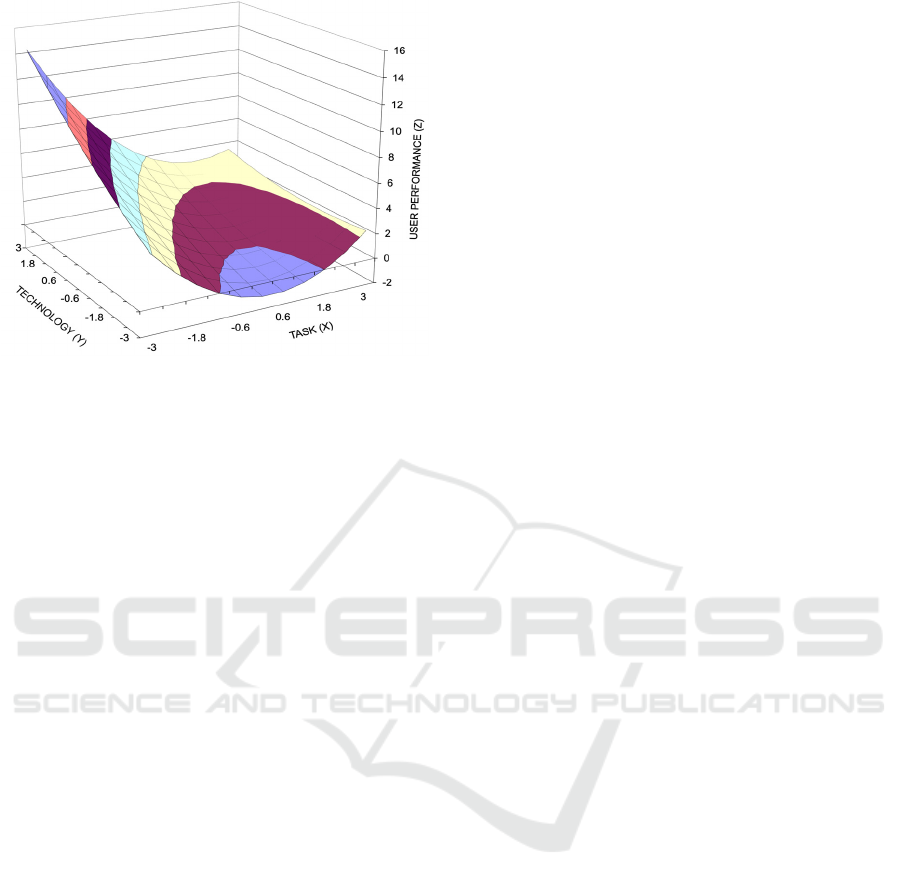
Figure 5: Response Surface for Task-Technology Fit (TTF)
and User Performance.
of congruence (Y=X) was positive but not significant
(a
2
= 0.293, t = 1.124), indicating that the relationship
between TTF and user performance is linear. This
indicates that the curvature along the line Y=X does
not significantly change for user performance. The
downward slope along the line of incongruence (Y=-
X) was negative but not significant (a
3
= -0.971, t = -
0.993). Hence, the lack of fit between the robotic
surgery task and support tools leads to a decrease in
user performance. The curvature along the line of
incongruence (Y=-X) was positive but not significant
(a
4
= 0.801, t = 0.234), further indicating a linear
relationship between TTF and user performance. The
curvature along the line Y=-X did not, therefore,
change significantly for user performance.
The lateral shift (Atwater et al., 1998) in use and
user performance, in the surface along and
perpendicular to the line of congruence (Y = X) was
determined using the following equation:
b
2
– b
1
Lateral Shift = ——————————
2 (b
3
– b
4
+ b
5
)
where:
b
1
= The beta value for Task
b
2
= The beta value for Technology
b
3
= The beta value for Task
2
b
4
= The beta value for Task*Technology
b
5
= The beta value for Technolo
gy
2
(2)
The lateral shift in use along the line of
congruence (Y = X) was positive (1.758), indicating
movement of approximately two units towards the
region where functional support levels surpass user
needs (Y > X). Here, the technology over-fits the task.
Hence, when the robotic surgery task and support tool
functions over-fit user needs, there is a sharp decline
in robotic surgeons’ dependence on use. Similarly,
the lateral shift in user performance along the line of
congruence (Y = X) was positive (1.230), indicating
movement of approximately one unit toward the
region where the robotic surgery task and support tool
functions over-fit user needs. Thus, when the robotic
surgery task and support tool functions over-fit user
needs, there is a sharp decline in the effectiveness,
efficiency, and quality, of robotic surgery task
performance.
8 DISCUSSIONS
In this paper, we investigated the potential transition
from technical system-oriented QoS to user-focused
QoE and QoT Internet configurations of the future.
We also explored the advent of an ultra-reliable and
ultra-low-latency B5G network and haptic-enabled
Internet. We applied this configuration to the use case
of remote robotic surgical task performance (tele-
haptic surgery applications) from the novel data-
driven evidence-based QoE/QoT perspective of
Task-Technology Fit (TTF) theory and predictive
modelling.
The analysis of non-linear impacts on use and
user performance represents a perspective of task-
technology equilibrium. This mechanism enables
more sophisticated and dynamic insights into the
effectiveness of TTF, and is useful for observing the
extent to which Information Technology (IT)
functions affect tool use and user performance levels.
Our findings show that when there is excessive
functional support for robotic surgery tasks, there is
an increasing likelihood of a lower dependence
among users, on using the technology whereby they
will more likely perceive that they deliver lower
quality MIS robotic surgery task performance, with
diminishing effectiveness and efficiency. This
finding represents an “IT surplus”, the supply of tool
functions that could exceed user task requirements
(Yang et al., 2013, p. 700). This is an extreme that
signifies a misfit, which can adversely affect task
productivity (Oh and Pinsonneault, 2007). Further, an
overfit can result in declining information
accessibility and processing performance, and has
been attributed to an excess of support functions that
can be termed as redundant (Jarvenpaa, 1989).
HEALTHINF 2024 - 17th International Conference on Health Informatics
120

9 IMPLICATIONS FOR
RESEARCH AND PRACTICE:
THEORETICAL AND APPLIED
CONTRIBUTIONS
From a more theoretical standpoint, an atomistic
approach (Yang et al., 2013), said to involve the
articulation and measurement of separate components
(p. 712) was used. This novel approach signifies a
more pragmatic, nuanced perspective of TTF
impacts. It can be applied to subsequent research
where the interaction effects of TTF warrant further
investigation. Moreover, the detailed analysis of use
and user performance effect differentials modelled
using three-dimensional (3-D) surfaces represents
richer insights into testing non-linear TTF.
From a more practical standpoint, the findings of
this study can serve as key guidelines with which to
enhance or reduce functional support related to
robotic surgery support tool use and surgeon user
performance. This can be an important benchmark
with which robotic surgery support tool designers can
calibrate the responsiveness of functional support to
user task needs. Further, the findings indicate that
excess or inadequate functional robotic surgery tool
support for surgeons’ user needs can lead to adverse
use and user performance impacts. Hence, robotic
surgery support tool designers must be acutely aware
of these task-technology differentials to attain a state
of congruence between supporting functions and
robotic surgeon’s needs.
10 CONCLUSIONS
In light of recent developments in ultra-reliable and
ultra-low latency communications that will come to
define next-generation digital networks, we
conceptualised the emerging transition from QoS-
centric content-delivery networks to QoE and QoT
focused skillset-delivery network configurations that
will typify closed-loop control architectures for
haptic-enabled and B5G Internets. We offer the novel
task-technology fit (TTF) conceptualisation and
predictive modelling and empirical analysis
perspective as a diagnostic tool. This vision of an
Internet of the future will involve the task performer
in a domain-specific technology user-focused context
(remote setting) performing tasks as the human-in-
the-loop (HITL), through immersive real-time
human-to-machine/robot (H2M/R) interactions.
Through this preliminary study, we examine the
mission-critical user scenario of tele-haptic (remote)
robotic surgery, expected to become a reality in the
era of B5G. With a haptic-enabled Internet and B5G
network to augment user skills, future robotic
microsurgeons will be ably supported to perform
seamless tele-haptic (remote) surgical tasks.
ACKNOWLEDGEMENTS
We sincerely thank the robotic surgeons who
participated in the study in conjunction with the
Robotic Assisted Microsurgical and Endoscopic
Society (RAMSES).
REFERENCES
Aiken, L. S., & West, S. G. (1991). Multiple Regression:
Testing and Interpreting Interactions. Sage
Publications.
Atwater, L. E., Ostroff, C., Yammarino, F. J., & Fleenor, J.
W. (1998). Self-Other Agreement: Does it Really
Matter?. Personnel Psychology, 51(3), 577- 598.
Bassoli, R., Boche, H., Deppe, C., Ferrara, R., Fitzek, F. H.
P., Janssen, G., & Saeedinaeeni, S. (2021). Quantum
Communication Networks. Springer.
Dishaw, M. T., & Strong, D. M. (1998). Supporting
Software Maintenance with Software Engineering
Tools: A Computed Task-Technology Fit Analysis. The
Journal of Systems and Software, 44(2), 107-120.
Dishaw, M. T., Strong, D. M., & Bandy, D. B. (2002).
Extending the Task-Technology Fit Model with Self-
Efficacy Constructs. Proceedings of the 8th Americas
Conference on Information Systems (AMCIS), August
9-11, 2002, Dallas, USA.
Dohler, M. (2018) The Future and Challenges of
Communications – Toward a World Where 5G Enables
Synchronised Reality and Internet of Skills. Internet
Technology Letters, 1(2), 1-3.
Edwards, J. R. (1993). Problems with the Use of Profile
Similarity Indices in the Study of Congruence in
Organizational Research. Personnel Psychology, 46(3),
641-665.
Edwards, J. R. (1994). The Study of Congruence in
Organizational Behaviour Research: Critique and a
Proposal and a Proposed Alternative. Organizational
Behaviour and Human Decision Processes, 58(1), 51-
100.
Edwards, J. R. (2002). Alternatives to difference scores:
Polynomial regression analysis and response surface
methodology. In F. Drasgow & N. W. Schmitt (Eds.),
Measuring and Analyzing Behavior in Organizations:
Advances in Measurement and Data Analysis (pp. 350-
400). Wiley.
Gatara, M. C., Mzyece, M., & Parekattil. S. J. (2021).
Towards a Fifth (5th) Generation (5G) Network and
Haptic-Enabled Internet for Remote Robotic Surgery:
The Beyond 5G (B5G) Era of Next-Generation Digital Networks: Preliminary Study of a Task-Technology Fit (TTF) Model for Remote
Robotic Surgery Applications
121

A Task-Technology Fit (TTF) Model. Proceedings of
the 45th Meeting of the Wireless World Research
Forum (WWRF), January 18-21, 2021, Kuala Lumpur,
Malaysia.
Gatara, M. C., & Mzyece, M. (2023). From QoS to QoE
plus QoT in Beyond 5G Networks. Journal of Mobile
Multimedia, 19(1), 135-146.
Giordani, M., Polese, M., Mezzavilla, M., Rangan, S., &
Zorzi, M. (2020). Toward 6G Networks: Use Cases and
Technologies. IEEE Communications Magazine, 58(3),
55-61.
Goodhue, D. L. (1992). User Evaluations of MIS Success:
What are we Really Measuring?. Proceedings of the
25th Hawaii International Conference on Systems
Sciences (HICSS), January 7-10, 1992, Hawaii, USA.
Goodhue, D. L. (1995). Understanding User Evaluations of
Information Systems. Management Science, 41(12),
1827-1844.
Hair, J. F., Jr., Hult, G. T. M., Ringle, C. M., & Sarstedt, M.
(2021). A primer on partial least squares structural
equation modeling (PLS-SEM) (3rd ed.). Sage
Publications.
Hiltz, S. R., & Johnson, K. (1990). User Satisfaction with
Computer-Mediated Communication Systems.
Management Science, 36(6), 739-764.
Hou, C.-K. (2012). Examining the Effects of User
Satisfaction on System Usage and Individual
Performance with Business Intelligence Systems: An
Empirical Study of Taiwan’s Electronics Industry.
International Journal of Information Management,
32(6), 560-573.
Igbaria, M., Zinatelli, N., Cragg, P., & Cavaye, A. L. M.
(1997). Personal Computing Acceptance in Small
Firms: A Structural Equation Model. MIS Quarterly,
21(3), 279-305.
Jarvenpaa, S. L. (1989). The Effect of Task Demands and
Graphical Format on Information Processing
Strategies. Management Science, 35(3), 285-303.
Junglas, I., Abraham, C., & Ives, B. (2009). Mobile
Technology at the Frontlines of Patient Care:
Understanding Fit and Human Drives in Utilization
Decisions and Performance. Decision Support Systems,
46(3), 634-647.
Nance, W. D. (1992). Task/Technology Fit and Knowledge
Worker Use of Information Technology: A Study of
Auditors. Ph.D. Dissertation, University of Minnesota,
Minnesota, USA.
Nawaz, S. J., Sharma, S. K., Wyne, S., Patwary, M. N., &
Asaduzzaman, M. (2019). Quantum Machine Learning
for 6G Communication Networks: State-of-the-Art and
Vision for the Future. IEEE Access, 7, 46317-46350.
Nunnally, J. C., & Bernstein, I. H. (1994). Psychometric
Theory (3rd ed.). McGraw-Hill.
Oh, W. and Pinsonneault, A. (2007). On the Assessment of
the Strategic Value of Information Systems:
Conceptual and Analytical Approaches. MIS Quarterly,
31(2), 239-265.
Pierucci, L. (2015). The Quality of Experience Perspective
Toward 5G Technology. IEEE Wireless
Communications, 22(4), 10-16.
Saracino, A., Deguet, A., Staderini, F., Boushaki, M. N.,
Cianchi, F., Menciassi, A., & Sinibaldi, E. (2019).
Haptic Feedback in the da Vinci Research Kit (dVRK):
A User Study Based on Grasping, Palpation, and
Incision Tasks. The International Journal of Medical
Robotics and Computer Assisted Surgery, 15(4), 1-13.
Shapiro, C., & Varian, H. R. (1999). Information rules: A
strategic guide to the network economy. Harvard
Business School Press.
Thompson, R. L., Higgins, C. A., & Howell, J. M. (1991).
Personal Computing: Toward a Conceptual Model of
Utilization. MIS Quarterly, 15(1), 125-143.
Torkzadeh, G., & Doll, W. J. (1999). The Development of
a Tool for Measuring the Perceived Impact of
Information Technology on Work. Omega, The
International Journal of Management Science, 27(3),
327-339.
Vessey, I. (1991). Cognitive Fit: A Theory-Based Analysis
of the Graphs Versus Tables Literature. Decision
Sciences, 22(2), 219-240.
Vessey, I. (1994). The Effect of Information Presentation
on Decision Making: A Cost-Benefit Analysis.
Information and Management, 27(2), 103-119.
Vessey, I., & Galletta, D. (1991). Cognitive Fit: An
Empirical Study of Information Acquisition.
Information Systems Research, 2(1), 63-84.
Yang, H.-D., Kang, S., Oh, W., & Kim, M. S. (2013). Are
All Fits Created Equal? A Nonlinear Perspective on
Task-Technology Fit. Journal of the Association for
Information Systems, 14(12), 694-721.
HEALTHINF 2024 - 17th International Conference on Health Informatics
122
