
Unpacking the Clinical Burden of Leukemia in GCC: Implications
for Patient Care
Hesham Ali Behary Aboelkhir
1
, Yousra El Alaoui
1
, Regina Padmanabhan
1
, Adel Elomri
1
,
Halima El Omri
2
and Abdelfatteh El Oomri
3
1
College of Science and Engineering, Hamad Bin Khalifa University, Doha, Qatar
2
National Center for Cancer Care and Research, Hamad Medical Corporation, Doha, Qatar
3
Surgical Research Section, Department of Surgery, Hamad Medical Corporation, Doha, Qatar
Keywords: Leukemia, Healthcare Expenditures, GCC, Global Figures, Clinical Burden.
Abstract: Cancer constitutes a substantial global health challenge, which is poised to intensify primarily due to the
growing elderly population globally. Leukemia, being a type of hematological cancer, presents unique
diagnostic complexities compared to solid cancers, contributing to elevated levels of morbidity and mortality
across various regions worldwide, resulting in a substantial clinical burden. Employing data sourced from the
WHO Global Health Expenditure Database and the Institute for Health Metrics and Evaluation (IHME)
Global Burden of Disease for the year 2019, this study undertakes an analysis of the prevalence, Years of Life
Lost (YLLs), Years Lived with Disability (YLDs), Disability-Adjusted Life Years (DALYs), and healthcare
expenditure in Gulf Cooperation Council (GCC) nations in comparison to the global figures.
1 INTRODUCTION
Global cancers are considered a major contributor to
disease burden worldwide and are expected to
continue growing for the next upcoming decades.
Cancer resulted in a total of 9.6 million deaths and
233.5 million disability-adjusted life years (DALYs)
in 2017 (Sung et al., 2021). Hence, the need for cancer
reduction strategies is regarded as a primary goal
recognized by the United Nations (UN) (Cheatley et
al., 2020).
Notably, leukemia is considered one of the most
concerning cancer types worldwide, and it is divided
into five major subcategories, namely acute myeloid
leukemia (AML), chronic myeloid leukemia (CML),
acute lymphocytic leukemia (ALL), chronic
lymphocytic leukemia (CLL), and others.
According to GLOBOCAN, leukemia was
classified as the 11
th
leading cause of all cancer-
related mortality (466,003 out of a total 9,958,133
cancer-related deaths) (Sung et al., 2021). Therefore,
an analysis of disease burden, leukemia in particular,
allows a better understanding of leukemia trends and
spreads, in order to assist health practitioners in
disease management and rational allocation of
healthcare resources (Cheatley et al., 2020).
In this study, we investigate the clinical burden of
leukemia through key indicators such as YLLs, YLDs,
DALYs, and healthcare expenditures in GCC
countries in comparison to global statistics. The aim
of this paper is to also understand leukemia’s
incidence and resulting deaths for more structured
prevention measures and improved clinical practice.
2 CLINICAL BURDEN
2.1 Related Works
Leukemia is a deadly hematological disease that not
only affects different age groups and poses a threat to
human development due to increased subsequent
deaths, but it also creates a significant burden on both
the healthcare system and society (Lin et al., 2021).
In 2015, leukemia resulted in 12 million DALYs
globally, with 97% and only 3% coming from YLLs
and YLDs, respectively (Ou et al., 2020). DALY is
used as an index of the combined quantity and quality
of life of a population, equating to the sum of YLDs
and YLLs.
Leukemia can be categorized into two main
categories: Acute and chronic. Unlike the acute type,
chronic leukemia is a class of slower growing cells
444
Aboelkhir, H., El Alaoui, Y., Padmanabhan, R., Elomri, A., El Omri, H. and El Oomri, A.
Unpacking the Clinical Burden of Leukemia in GCC: Implications for Patient Care.
DOI: 10.5220/0012373700003657
Paper published under CC license (CC BY-NC-ND 4.0)
In Proceedings of the 17th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2024) - Volume 2, pages 444-449
ISBN: 978-989-758-688-0; ISSN: 2184-4305
Proceedings Copyright © 2024 by SCITEPRESS – Science and Technology Publications, Lda.
that can take up to several years to progress.
According to Yao et al., global deaths and DALYs
decreased slightly for chronic lymphocytic leukemia
(CLL) from 1990 to 2019 (Yao et al., 2021).
Moreover, the burden of death and DALY was mainly
affected by socio-demographic index (SDI), such that
the disease burden of CLL decreased in higher SDI
countries, while increasing in lower ones. This could
be due to the quality of healthcare provided in
developed countries compared to developing ones.
Similarly, the average potential years of life lost
(AYLL) was used for ALL to evaluate its societal
burden (Ahmad et al., 2023). Although ALL is
considered as a rare disease, it still represents a
significant health burden corresponding to a high
AYLL due to declining survival rates among adults
and increased incidence rate among children (Ahmad
et al., 2023).
In the same context, a study was performed to
investigate the incidence rate, mortality rate, DALY
and its change trend of AML during the period
extending from 1990 until 2017 in 195 countries. The
analysis revealed a gradual increase in both incidence
and mortality rates of AML, with males and elderly
being more prone to develop the disease (Lin et al.,
2021).
Comparably, a study undertaken to explore the
global burden of CML between 1990 and 2017
revealed a higher incidence and mortality of CML in
males compared to females. In addition, the highest
burden was reported in each of Andean Latin
America, Central Sub-Saharan Africa, and Southeast
Asia (Lin et al., 2021). While the age-standardized
death rate (ASDR) decreased during the period under
study in high SDI regions, the health-related burden
of CML remains a challenge for the low-SDI regions,
suggesting that appropriate strategies are yet to be
developed and adopted in these regions (Ning et al.,
2020).
2.2 Epidemiology
This section focuses on leukemia prevalence and
incidence rate analysis in the Gulf Cooperation
Council (GCC). The latter comprises Bahrain,
Kuwait, Oman, Qatar, Saudi Arabia, and the United
Arab Emirates (UAE), serving as a regional,
intergovernmental alliance with both political and
economic objectives. While these nations share a
common geographical region and numerous
connections, each country exhibits distinctive traits in
its healthcare systems, strategies, and various socio-
economic factors. This individuality underscores the
importance of studying the specific prevalence of
leukemia within this region.
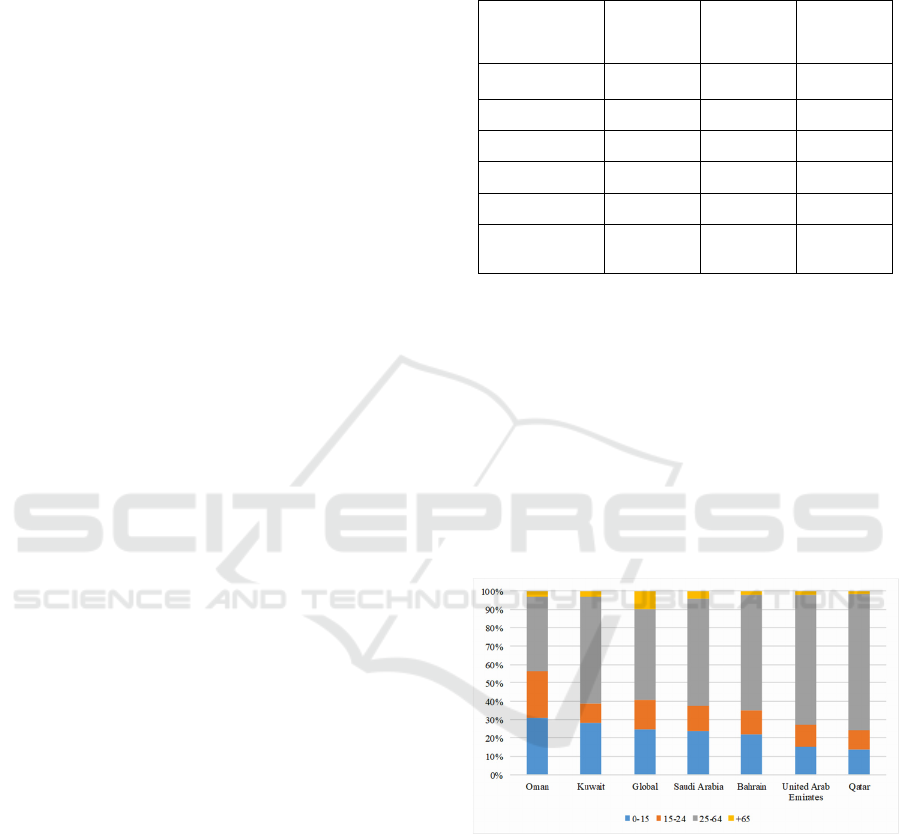
Table 1: Population structure of GCC.
Country
Male-to-
Female
Ratio
Expatriate
(%)
Median
Age
Qatar 2.57 86% 33.8
UAE 2.18 89% 30.3
Kuwait 1.58 68% 37.2
Bahrain 1.54 54% 32.7
Oman 1.44 43% 29
Saudi Arabia 1.36 48% 30.4
Table 1 displays the population composition of GCC
countries. It underscores the significant male-to-
female ratio in all these nations, primarily resulting
from a substantial influx of expatriates who come to
this region for employment opportunities, but often
do not bring their families along. This migration
pattern also contributes to the notable proportion of
individuals aged 15-64, as indicated in Figure 1.
However, it's worth noting that this scenario may be
different for Oman, which has the lowest expatriate
percentage (43%) and the youngest median age (29
years) among all the GCC nations.
Figure 1: The population age structure of GCC countries in
2019.
On a global scale, the incidence rate of Leukemia
stands at approximately 8.3 cases per 100,000 people,
with a slight upward trend observed from 2010 to
2019. When compared to GCC countries, we find a
notably lower incidence rate, ranging from 3.86 to
5.12 cases per 100,000 individuals. Figure 2
illustrates the case of Oman, which experienced a
declining trend during this period. Kuwait, on the
other hand, displayed a decreasing trend up to 2013,
followed by an increasing trend from 2013 to 2019.
Unpacking the Clinical Burden of Leukemia in GCC: Implications for Patient Care
445
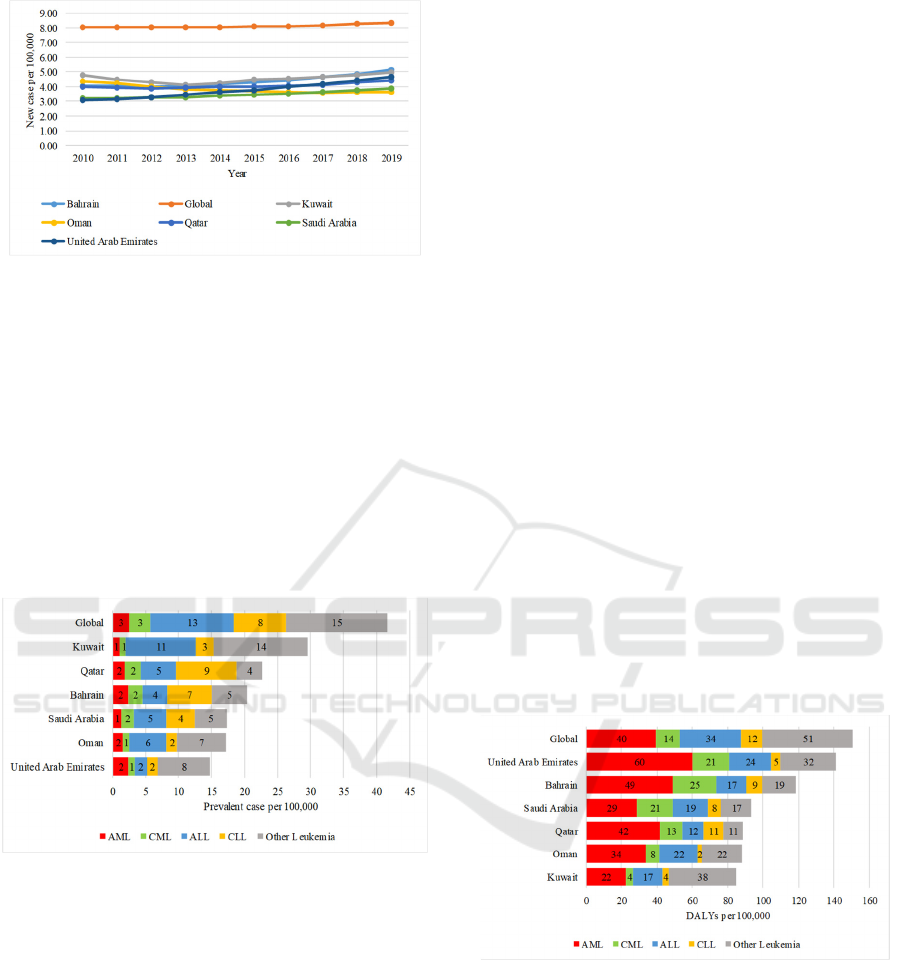
Figure 2: Incidence rate of GCC countries compared to
global rates in 2019 across all sexes and all ages.
The incidence rate reflects the number of new
cases diagnosed each year, offering insights into the
annual rate of occurrence. Nevertheless, when it
comes to understanding the overall impact of the
disease, the prevalence rate plays a pivotal role.
Prevalence represents the proportion of the
population that possesses a specific characteristic, in
this case, the ongoing burden of leukemia, over a
defined time period. It takes into account not only
new cases, but also those who have been living with
the condition for long.
Figure 3: Prevalence of leukemia and its subtypes per
100,000 cases in GCC compared with global trends for all
sexes and all ages in 2019.
As depicted in Figure 3, all GCC countries exhibit
lower prevalence rates for overall leukemia, ranging
from 14.72 to 29.55 cases per 100,000 people. These
figures contrast with the global prevalence rate of
41.64 cases per 100,000 individuals. Among the GCC
nations, Kuwait reports the highest prevalence rate
for total leukemia at 29.55 cases per 100,000 people,
while the UAE registers the lowest prevalence rate,
standing at 14.72 cases per 100,000.
Upon analyzing the prevalence of various
subcategories of leukemia in the GCC countries, the
following observations were made:
The prevalence rates for AML in GCC countries
range from 1.08 in Kuwait to 2.45 in the UAE, all of
which are lower than the global rate of 2.55.
In the case of CML, the prevalence rates in GCC
countries range from 0.88 in both Oman and the UAE
to 2.39 in Qatar, which are also lower than the global
rate of 3.25.
For ALL, the prevalence rate in the GCC ranges
from 1.83 in the UAE to 10.56 in Kuwait, all of which
are lower than the global rate of 12.61.
Additionally, Qatar is the exception, with a
prevalence rate of 9.22 for CLL, which exceeds the
global rate of 7.84. This particularity in Qatar's CLL
prevalence rate warrants further analysis to
understand the factors behind this higher pattern.
For other leukemia subtypes, while all GCC
countries exhibit prevalence rates lower than the
global rate of 15.40, only Kuwait's prevalence rate is
close to the global rate at 14.23. The remaining GCC
countries show prevalence rates ranging from 3.83 in
Qatar to 7.87 in the UAE.
To estimate the burden of leukemia, our study
utilizes DALYs (Disability-Adjusted Life Years),
where one DALY signifies the loss of one year of
complete health. DALYs are calculated by summing
the years of life lost due to premature mortality
(YLLs) and the years lived with a disability (YLDs)
attributed to prevalent cases of the disease within a
community (GBD, 2019).
The formula for DALYs is:
DALYs = YLLs + YLDs.
Figure 4: DALYs per 100,000 cases of leukemia in GCC
countries compared to global trends for all sexes and all
ages in 2019.
Figure 4 provides an insight into the total
leukemia burden in GCC countries, which ranges
from 84.77 to 141.26 DALYs per 100,000. These
rates are notably lower than the global average of
150.67 DALYs per 100,000. This is consistent with
the expectation that lower prevalence rates in GCC
countries would result in a lower overall burden.
HEALTHINF 2024 - 17th International Conference on Health Informatics
446
Nevertheless, we notice that despite having the
lowest prevalence rate of total leukemia among GCC
countries, the UAE has the highest burden.
Conversely, Kuwait, with the highest prevalence rate
of total leukemia, reports the lowest burden. These
discrepancies suggest that additional factors might be
influencing the burden and require further
investigation.
In addition, the burden of myeloid leukemia, both
acute and chronic, in GCC countries exceeds the
global burden. This is especially notable in the UAE
and Bahrain for AML and CML. In Qatar, only the
AML burden exceeds the global average, while in
Saudi Arabia, it's the CML burden that surpasses the
global level. Approximately 98% of the total
leukemia burden, calculated using DALYs, is
attributed to YLLs. This indicates that premature
mortality plays a substantial role in the overall disease
burden.
These findings underscore the need for further
research to understand the factors contributing to
variations in leukemia burden within the GCC
countries, including the unexpected burden
disparities between prevalence rates and the potential
factors influencing YLLs in this context.
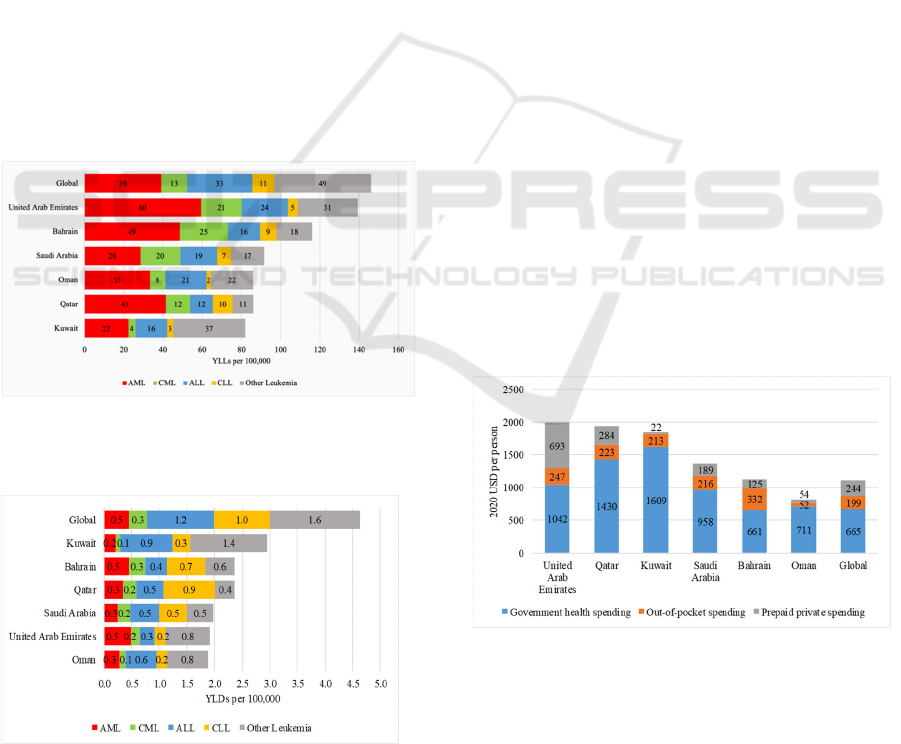
Figure 5: YLLs per 100,000 cases of leukemia in GCC
countries compared to the global rates for all sexes and all
ages in 2019.
Figure 6: YLDs per 100,000 cases of leukemia in GCC
countries compared to global rates for all sexes and all ages
in 2019.
3 HEALTH EXPENDITURES
Health expenditure encompasses all financial outlays
related to the provision of healthcare services, family
planning initiatives, nutrition programs, and
assistance for health-related disasters. However, it
does not include expenses for drinking water and
sanitation. Health funding represents a critical
element within healthcare delivery systems (WHO,
2023).
In the GCC region, healthcare expenditure draws
from three primary sources:
• Government Health Expenditure, which
represents the portion of a country's Gross
Domestic Product (GDP) allocated to healthcare
by the government.
• Out-of-Pocket Payments (OOP), which are
direct payments made by individuals to
healthcare providers as compensation for the
services they receive.
• Prepaid Private Spending, which includes the
combined spending through both compulsory
and voluntary private health insurance schemes
(WHO, 2023).
As per Figure 7, it is clear that the healthcare
expenditures in all GCC countries surpass the global
average of 1,108 USD per person, with one exception
being Oman. Oman reports a healthcare expenditure
of 817 USD per person. These differences in
healthcare expenditure levels among GCC countries
can reflect varying economic capacities, healthcare
system structures, and government healthcare
funding policies.
Figure 7: Health expenditure and spending sources in GCC
compared to global trends in 2019.
Among GCC countries, the breakdown of
healthcare expenditure shows some interesting
variations, including the UAE leading the GCC with
the highest healthcare expenditure per person at 1,983
USD. It also has the highest prepaid spending at 693
Unpacking the Clinical Burden of Leukemia in GCC: Implications for Patient Care
447

USD per person. Next, Qatar follows the UAE with a
healthcare expenditure of 1,938 USD per person.
While Kuwait has the highest government health
spending at 1,609 USD per person, it reports the
lowest prepaid private spending at 22 USD per
person. Finally, Bahrain has the highest out-of-pocket
spending at 332 USD per person.
Healthcare expenditure serves several essential
purposes, including reducing the burden of diseases,
addressing capacity constraints, and improving
access to healthcare facilities by reducing waiting
times. The GCC region has implemented various
quality assurance strategies to bring their healthcare
systems in line with global standards, ensuring high-
quality healthcare services in multiple dimensions.
Universal Health Coverage (UHC) is a crucial
index that assesses the effectiveness of healthcare
coverage. It examines service coverage across various
population health needs and evaluates the extent to
which these services contribute to enhanced health
outcomes. UHC is an essential framework for
measuring and promoting equitable access to
healthcare services for all individuals within a
population (WHO, 2023).
Table 2 indicates that all GCC countries are
experiencing an annual increase in the UHC Index.
This positive trend aligns well with some of the
countries that have the highest healthcare spending. It
demonstrates a commitment to expanding and
improving access to healthcare services and
achieving equitable coverage across the GCC region,
even in comparison to countries with significant
healthcare expenditures (The Institute for Health
Metrics and Evaluation, 2019).
Table 2: Comparison between GCC countries and three of
the highest-ranked countries in terms of UHC index from
2010-2019.
Country 2010 2019
Australia 88.3 89.4
UK 86 87.9
USA 81.2 82.1
Kuwait 75 81.8
Qatar 76.3 80.4
Oman 61.6 71.2
Bahrain 66.3 70.6
Saudi 58.5 64.2
UAE 63.3 63.4
4 DISCUSSION
The rising incidence of leukemia in GCC countries
necessitates an increase in healthcare capacity. The
number of hospitals is steadily increasing in all GCC
nations, reflecting a long-term strategy to address the
growing demand for healthcare services. Qatar leads
with the highest hospital-per-population ratio at
0.0019%, followed by Oman (0.0017%), the UAE
(0.0016%), Saudi Arabia (0.0014%), Bahrain
(0.0014%), and Kuwait (0.0006%). This reflects a
commitment to enhancing healthcare infrastructure to
meet the clinical burden of leukemia.
Figure 8: Hospital to population ratio in GCC in 2022.
The number of hospitals in Qatar increased from
30 in 2011 to 57 in 2022, while in Oman, it grew from
65 in 2012 to 88 in 2022. Further analysis on the
capacity of these hospitals is needed in future studies.
Variations in leukemia prevalence in GCC
countries may be attributed to risk factors in
healthcare. These factors fall into three categories:
Metabolic risks, behavioral risks, and environmental
and occupational risks. Table 3 ranks these risk
factors across GCC nations, providing insight into the
differences in leukemia prevalence and trends.
Table 3: Risk Factors Ranking among GCC in 2019.
Risk Factors UAE Qatar
Saudi
Arabia
Oman Bahrain Kuwait
High Body-Mass
Index
1 1 1 1 1 1
High Fasting
Plasma Glucose
4 2 3 3 2 2
High Blood
Pressure
2 5 2 2 3 3
High LDL 5 9 7 5 7 7
Kidney
Dysfunction
8 10 8 9 8 9
Tobacco 3 3 6 8 4 4
Dietary risks 7 6 4 4 6 5
Malnutrition
_
8 10 7
_
8
Low physical
Activity
_ _ 9 _ 10 _
Drug Usage 9
_
_
_
_
_
Air pollution 6 4 5 6 5 6
Occupational Risks 10 7
_
10 9 10
HEALTHINF 2024 - 17th International Conference on Health Informatics
448

Table 3 underscores that metabolic risks,
particularly high body-mass index, high fasting
plasma glucose, and high blood pressure are the
dominant risk factors in the GCC region. These
factors consistently rank as the top risks in all GCC
countries. Moreover, Tobacco intake is the third risk
factor in Qatar and the UAE, and the fourth in Bahrain
and Kuwait, while drug usage risk only features in the
top ten risk factors in the UAE.
The age structure of the population is another
factor influencing the variation in leukemia
prevalence and clinical burden across GCC countries.
Leukemia incidence rates tend to rise with age.
Hence, countries with a significant elderly population
may experience a greater leukemia burden as the
proportion of elderly individuals increases. The
GCC countries have a substantial expatriate
population, originating from various regions
worldwide, with a notable concentration from South
Asian countries. This diversity calls for further
studies to investigate potential relationships between
nationality and leukemia incidence, considering
genetic factors based on genome mapping.
5 CONCLUSIONS
In summary, the rising leukemia incidence in GCC
countries necessitates increased healthcare capacity,
with a steady growth in the number of hospitals.
Variations in leukemia prevalence result from factors
like metabolic risks, age structure, and the significant
expatriate population. Metabolic risks, particularly
high body-mass index, are prominent. Further research
is needed to explore the relationship between natio-
nality and leukemia incidence, considering genetic
factors among the diverse expatriate population.
ACKNOWLEDGEMENTS
This article was made possible by National Priorities
Research Program-Standard (NPRP-S) Twelfth (12th)
Cycle grant# NPRP12S-0219-190108, from the Qatar
National Research Fund (a member of the Qatar
Foundation). The findings herein reflect the work, and
are solely the responsibility, of the author[s].
REFERENCES
Sung, H., Ferlay, J., Siegel, R. L., Laversanne, M.,
Soerjomataram, I., Jemal, A., & Bray, F. (2021). Global
cancer statistics 2020: Globocan estimates of incidence
and mortality worldwide for 36 cancers in 185
countries. CA: A Cancer Journal for Clinicians, 71(3),
209–249. https://doi.org/10.3322/caac.21660
Cheatley, J., Aldea, A., Lerouge, A., Devaux, M., Vuik, S.,
& Cecchini, M. (2020). Tackling the cancer burden:
The economic impact of primary prevention policies.
Molecular Oncology, 15(3), 779–789. https://doi.org/
10.1002/1878-0261.12812
Lin, X., Wang, J., Huang, X., Wang, H., Li, F., Ye, W.,
Huang, S., Pan, J., Ling, Q., Wei, W., Mao, S., Qian,
Y., Jin, J., & Huang, J. (2021). Global, regional, and
national burdens of leukemia from 1990 to 2017: A
systematic analysis of the global burden of disease 2017
study. Aging, 13(7), 10468–10489. https://doi.org/
10.18632/aging.202809
Ou, Z., Yu, D., Liang, Y., He, W., Li, Y., Zhang, M., You,
F., He, H., & Chen, Q. (2020). Analysis of the global
burden of disease study highlights the trends in Death
and disability‐adjusted life years of leukemia from 1990
to 2017. Cancer Communications, 40(11), 598–610.
https://doi.org/10.1002/cac2.12094
Yao, Y., Lin, X., Li, F., Jin, J., & Wang, H. (2021). The
Global Burden and Attributable Risk Factors of
Chronic Lymphocytic Leukemia in 204 Countries and
Territories from 1990 to 2019: Analysis Based on the
Global Burden of Disease Study 2019.
https://doi.org/10.21203/rs.3.rs-824063/v1
Ahmad, A. S., Offman, J., Delon, C., North, B. V., Shelton,
J., & Sasieni, P. D. (2023). Years of life lost due to
cancer in the United Kingdom from 1988 to 2017.
British Journal of Cancer. https://doi.org/10.1038/
s41416-023-02422-8
Lin, Q., Mao, L., Shao, L., Zhu, L., Han, Q., Zhu, H., Jin,
J., & You, L. (2020). Global, regional, and national
burden of chronic myeloid leukemia, 1990–2017: A
systematic analysis for the global burden of disease
study 2017. Frontiers in Oncology, 10.
https://doi.org/10.3389/fonc.2020.580759
Ning, L., Hu, C., Lu, P., Que, Y., Zhu, X., & Li, D. (2020).
Trends in disease burden of chronic myeloid leukemia
at the Global, regional, and national levels: A
population-based epidemiologic study. Experimental
Hematology & Oncology, 9(1). https://doi.org/
10.1186/s40164-020-00185-z
Global burden of disease study 2019 (GBD 2019) Data
Resources. GHDx. (n.d.). https://ghdx.healthdata.org/
gbd-2019
World Health Organization. (n.d.). Health expenditure.
World Health Organization. https://www.who.int/
data/nutrition/nlis/info/health-expenditure
World Health Organization. (n.d.-b). Total expenditure on
health as a percentage of gross domestic product.
World Health Organization.https://www.who.int/
data/gho/data/indicators/indicator-details/GHO/total-
expenditure-on-health-as-a-percentage-of-gross-dome
stic-product
Health by location. The Institute for Health Metrics and
Evaluation. (n.d.). https://www.healthdata.org/
research-analysis/health-by-location
Unpacking the Clinical Burden of Leukemia in GCC: Implications for Patient Care
449
