
Prototyping a Low-Cost Flexible Sensor Glove For Diagnostics and
Rehabilitation
Shival Indermun
1,2 a
and Taahirah Mangera
2 b
1
Mechanical and Mechatronic Department, Stellenbosch University, Western Cape, South Africa
2
School of Mechanical, Aeronautical and Industrial Engineering, University of Witwatersrand, Johannesburg, South Africa
Keywords:
Low-Cost, Diagnostics, Hand Rehabilitation, Flex Sensors, Prototype, Hand Impairment, Developing
Countries, Design, Evaluation.
Abstract:
Individuals in developing regions who require hand therapy for rehabilitation face difficulties accessing local
clinics. The objective of the current study was to create a cost-effective device capable of assessing finger
range of motion (ROM) for diagnostic and potential rehabilitation purposes in these disadvantaged areas. The
design employs flexible sensors and a soft glove that records the motion of key finger joints during a variety
of daily activities performed by ten healthy participants. The results demonstrated the glove’s effectiveness
in measuring dynamic ROM for both hands of all participants. This promising outcome suggests that the
flexible sensor holds great potential as a tool for hand rehabilitation and diagnosing hand impairment, offering
a valuable solution to address accessibility issues in developing countries.
1 INTRODUCTION
Low-cost prosthetic devices are well-researched,
while low-cost rehabilitative orthotic devices are less
well-addressed. Specifically, low-cost rehabilitation
of hand impairments using orthotic devices is not
commonly addressed. Many diseases and disorders
can lead to hand impairments that sees patients losing
full use of their upper limbs. One of the more preva-
lent disorders is cerebrovascular accidents, commonly
referred to as Stroke. Stroke is steadily increasing in
developing countries (Yan et al., 2016) and is one of
South Africa’s leading causes of disability (Maredza
and Chola, 2016). Stroke costs are at approximately
2-3% of the total health services expenditure in South
Africa (Maredza and Chola, 2016).
Although stroke is prominent in developing coun-
tries like South Africa, it is still one out of many that
affect the hand. Moodley (Moodley, 2018) highlights
the significance of radial nerve palsy in South Africa.
The radial nerve accounts for the extension of the
wrist and fingers, thus damage to this nerve results
in weakness and reduced mobility of the hand. The
causes of radial nerve palsy can stem from physical
injuries to infections, with the most common cause
being related to overuse of the arm. This injury is
more commonly seen in labourers where the radial
a
https://orcid.org/0000-0002-5569-5036
b
https://orcid.org/0000-0002-8113-8030
nerve could be compromised due to the extent of their
work.
Half of the Stroke patients in South Africa live in
rural areas where the nearest clinic equipped for ther-
apy is not easily accessed due to distance(Maredza
et al., 2015). Statistics South Africa (StatsSA, 2015)
found that lower-income households spend a higher
proportion of their income on public transport than
other expenses. Transport to clinics where rehabili-
tation can be accessed increases the expense of con-
tinual rehabilitation. In addition, due to the large
turnovers observed by therapists (De Klerk et al.,
2016), some patients may find themselves waiting
for long periods of time which may result in them
needing to return the next day to receive treatment.
De Klerk et al. (2016) studied additional issues that
South Africans face in terms of occupational hand
therapy. One of the more pertinent issues is the high
rates of cases and referrals. Each therapist is restricted
to a set time for each patient. Therefore, with the
rates of cases increasing, therapists are forced to min-
imize the time allocated for consultation and treat-
ment. Limited academic resources and opportunities
for hand occupational therapy in South Africa are a
further barrier. Arguably, other developing countries
may face similar difficulties. Methods of treatment
that are accessible to all patients in South Africa and
the developing world are thus required.
Given the number of medical diseases that can
hinder or injure the hand, rehabilitation that can stim-
Indermun, S. and Mangera, T.
Prototyping a Low-Cost Flexible Sensor Glove for Diagnostics and Rehabilitation.
DOI: 10.5220/0012314800003657
In Proceedings of the 17th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2024) - Volume 1, pages 103-110
ISBN: 978-989-758-688-0; ISSN: 2184-4305
Copyright © 2024 by Paper published under CC license (CC BY-NC-ND 4.0)
103

ulate recovery is imperative. However, before at-
tempting to produce methods that can provide effec-
tive therapy, consideration needs to be given to assess-
ing the level of hand impairment. Methods of mea-
suring the range of motion of the hand may result in a
means of quantifying impairment, monitoring patient
recovery and possibly diagnosing both neurological
and hand-specific disorders. Hart and Tepper (2001)
determined, through a questionnaire completed by pa-
tients with hand impairments, that patients who had
undergone rehabilitative therapy perceived improve-
ments in their functional abilities and health. By us-
ing a method of quantifying the range of motion of
the hand, the data recorded can possibly validate any
improvements observed in therapy.
Measuring the ROM of the hand has predomi-
nantly been achieved by using a goniometer. These
methods have been used in several studies (Bain et al.,
2015; Hayashi et al., 2014; Hume et al., 1990) to de-
termine the static ROM of patients performing activi-
ties of daily living (ADL). The accuracy and reliabil-
ity of the device are dependent on the patient’s ability
to hold a gesture, with minimal movements. In ad-
dition to this dependency, repeatedly measuring each
joint of each finger during activities or gestures, is te-
dious and time-consuming. This can affect the pa-
tient’s performance. Thus, a more efficient method of
measuring the ROM that addressed these areas was
developed.
2 MATERIALS AND METHODS
The current study was divided into three segments:
(1) flexible sensor analysis, (2) development of the
prototype, and (3) candidate testing.
2.1 Flexible Sensor Analysis
Before developing a prototype of the device, it was
necessary to analyse the flexible sensor. The analysis
entailed the configuration of the flexible sensors and
multiple tests conducted to verify the application of
the sensors. Apart from the sensor signal drift and
the limitations, tests aimed to replicate the anatomical
variations of the finger joints of a human hand, were
included.
Flex sensors (Sparkfun Electronics, Colorado,
USA), were chosen due to their availability and cost.
Alternative sensors such as potentiometers, can be
used as they can be configured in a similar manner.
However, the difficulty arises when aligning the rota-
tion of the sensor in conjunction to the rotation of a
finger joint. Furthermore, designing and implement-
ing this system brings further complications when
considering the different hand sizes of patients.
The sensors are based on polymer ink and conduc-
tive particles. As the sensor is bent or flexed, the con-
ductive particles move further away, increasing the
path distance the applied current must travel through,
thereby increasing the resistance. By recording the
resistance at different angles of flexibility or bending,
a correlation can be made against the range of motion.
Oess et al. (2012) had sampled multiple flexible
sensors with respect to signal drift, comparing differ-
ences based on both type and sensor length. The re-
sults displayed a relation between signal drift and sen-
sor length, with an increased length leading towards
a decreased signal drift. In addition, the minimum
signal deviations were observed from the sensors that
had gone through a polyester over-lamination process.
This suggests that a cover medium may result in lower
variations of the signal. The current study is heav-
ily influenced over the availability of resources and
therefore confined to the use of locally sourced, sin-
gle branded and sized flexible sensors.
Apart from the comments made by Oess et al.
(2012), the sensor datasheet highlighted that the base
of the sensor should be supported, and no bending
should occur near the output pin of the sensors. In the
current study a 3D printed base was used to secure the
ends of the sensors.
The flexible sensors were used along the joints of
the fingers. Before any prototype was developed, con-
sideration had to be given to the anatomical variation
in hand sizes and shapes. As discussed, the sensors
output resistances based on the extent at which they
are bent. The greater the bend, the higher the resis-
tance. These resistances will be used to map angles
that represent the rotation of the joint. It was thus
necessary to determine the resistance fluctuations ob-
served from these sensors.The basic configured cir-
cuit consisted of an Arduino Uno, one flexible sensor,
a single bread board and a 100 kΩ resistor. Only the
flexible sensor was changed within the circuit when
testing for repeatability.
2.1.1 Signal Stability
The flexible sensors were configured with a resis-
tor to replicate a voltage divider. This allowed the
analog pins of the selected microcontroller to read
a variable voltage. It was also necessary to deter-
mine whether the straight resistances of various flex-
ible sensors were similar, had minimal signal fluctu-
ations and are around 30 000 Ω, as indicated by the
manufacturer. To ensure that the readings of the sen-
sors remain undisturbed by any movements, a simple
rig was created to keep the sensor in a straight posi-
BIODEVICES 2024 - 17th International Conference on Biomedical Electronics and Devices
104
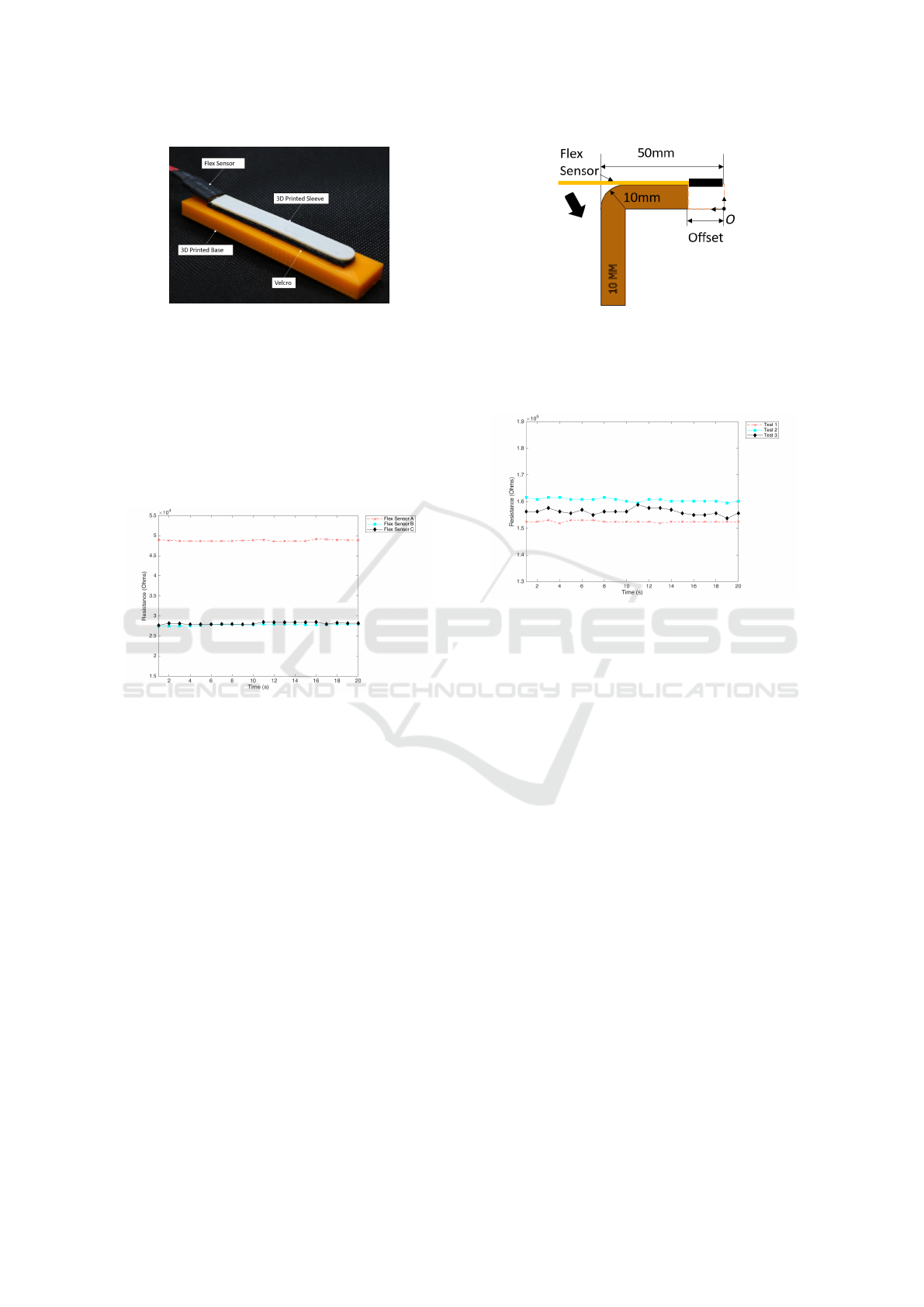
Figure 1: Flat Test Rig.
tion. This is shown in Figure 1. The straight test rig
holds the sensor in place using a 3D printed flexible
sleeve. The sleeve is attached to a solid 3D printed
base using velcro.
Each flexible sensor had a consistent straight line
with minor fluctuations, as shown in Figure 2. This
was repeated 3 times across each sensor, resulting in
a negligible, calculated coefficient of variance of less
than 1%.
Figure 2: Flat Resistances.
2.1.2 Anatomical Variations
The current investigation represented the anatomical
variations observed across patients, through a bend lo-
cation and radius test. These tests were used to deter-
mine the effect of anatomical variation on the output
of a flexible sensor.
The bend location test indicated whether readings
across the length of the sensor were consistent. This
was significant as some patients may have hands of
similar size, however the length and location of their
joints may vary. In addition, the results also deter-
mined the required positioning of the sensors in order
to produce stable outputs. Multiple flexible sensors
were bent at several different locations. The locations
were determined by three offsets (20, 30 and 40 mm),
from the origin O , as seen in Figure 3.
The bend location test was repeated three times on
several sensors, to determine whether a trend was ob-
served. However, all of the sensors produced results
of varying magnitude irrespective of the offset. Fig-
ure 4 represents the three bend locations tests at a 30
Figure 3: Radius and Bend Location Test.
mm offset for a sample flexible sensor. All three tests
resulted in a variation of magnitude. A coefficient of
variance of less than 2.2% was calculated.
Figure 4: Repeatable Tests for Flex Sensor A (30mm Off-
set).
For the 40 mm offset (bending occurring close to
the base of the sensor) higher variations occurred, up
to 4.6%. Thus, the sensors in the current research
were positioned away from the base, towards the cen-
tre of the sensor.
Considering the structure of the hand, physical
variations may be present along the joints of the fin-
gers. Some people may have bony knuckles and joints
while others may have rounded and smoother joints.
Nevertheless, it is necessary to replicate such scenar-
ios by bending the flexible sensors at various radii
(r = 5, 10 and 12 mm). The test setup was similar
to that of the bend location test, shown in Figure 3,
by keeping a zero offset and using different radi rigs.
The results showed no significant trends, apart from
fluctuations in magnitude, with no definitive correla-
tion with the radii. However, considering the variation
in the resistances across the multiple sensors a maxi-
mum coefficient of variance was calculated as 3.7%.
This difference is greater than the difference evaluated
in the bend location test, suggesting that the curvature
of bending the sensors has a greater effect than the
location at which the sensors are bent.
Based on the two tests, it was evident that the sen-
sors can produce repeatable results with deviations
being limited to under 4%. However, a calibration
Prototyping a Low-Cost Flexible Sensor Glove for Diagnostics and Rehabilitation
105

phase was introduced to the study to minimize the de-
viation as well as cater for signal drift, which will be
discussed in the next section.
2.2 Development of the Prototype
2.2.1 Design
The device design involves two main aspects: the
glove attachment and the circuit design. Golf gloves
were chosen for simplicity and availability, eliminat-
ing the need for manufacturing. They also facilitated
easy size selection for both right and left-handed indi-
viduals. Various attachment methods were evaluated,
including velcro and 3D printed sleeves, which were
either glued or sewn onto the glove.
While the velcro method offered modularity for
sensor attachment, it posed issues with separation
during repeated finger bending, potentially affecting
sensor readings. On the other hand, the 3D printed
sleeves effectively secured the sensors regardless of
attachment method.
Initially, flexible sleeves were placed only on the
proximal interphalangeal (PIP) joints, providing rea-
sonable comfort. However, when extended to both
PIP and metacarpophalangeal (MCP) joints, it re-
sulted in increased resistance to motion, potentially
causing discomfort or harm to hand-impaired users.
The PIP joint is situated in the middle section of the
finger, while the MCP joint is located at the knuckle.
Due to the discomfort the flexible sleeve attachment
was deemed impractical. To address this, medical
tape was used to secure the flexible sensors, reducing
joint resistance and minimizing manufacturing costs
(see Figure 5).
Figure 5: Medical Tape Prototype.
Figure 6 represents the final circuit that was de-
signed for the prototype. The Arduino Uno was
replaced with a different microcontroller (Micro-
robotics, Johannesburg, SA) that is similar to the Ar-
duino MEGA but is more compact. This is due to the
number of analogue pins required to connect all 10
sensors. However, the circuit in Figure 6 acts as an
example of how a single sensor is connected, but still
incorporates the main components of the circuit used
within the prototype.
Figure 6: Final Circuit.
For the testing procedure, the user wears the glove
and lays the hand on a flat surface in a flat position.
The first calibration phase begins, with Push Button
1 pressed. The sensor readings are recorded and are
used as the 0° reference.
After 30s has elapsed the user changes the gesture
into a fisted position for the second calibration. The
sensor readings recorded during this are used as a ref-
erence for 90°. The user is expected to hold the fisted
position after the second calibration phase. This step
is used to record a set of data and compare these val-
ues with the calibration results. This procedure aims
to quantify the physical slack in the glove, signal drift
and possible anatomical variations by calculating the
difference between the two sets of data for each joint.
Thus, the difference will be used as a unique correc-
tion factor for each candidate.
LEDs acted as visual cues for each phase. All
LEDs remained off after calibration 2, signalling the
commencement of activity testing in which the user
performed the directed tasks, while the glove records
the ROM of the hand.
2.2.2 Validation
The validation of the glove consisted of testing each
joint at 30°, 45° and 60°. This was done by using a
finger goniometer. The results of the validation are
shown in Table 1. Each set of tests were repeated
three times across 3 different sensors, similar to that
of Section 2.1.
The RMSE (Root Mean Square Error) is a mea-
sure of the average of the differences between values
predicted and the values observed. The average error
across the left and right hands is 4.8 and 5.2, respec-
tively. These errors do not consider the correction fac-
tor and thus the signal drift and physical slack of the
glove.
The average deviations shown in Table 1 were cal-
culated including the correction factor as discussed in
the previous section. In comparison with the RMSE
error, it was evident that the signal drift and slack of
the glove produced additional error and thus the cor-
rection factor had to be applied. The results indicate
an accuracy of ± 5° which was congruent with re-
BIODEVICES 2024 - 17th International Conference on Biomedical Electronics and Devices
106
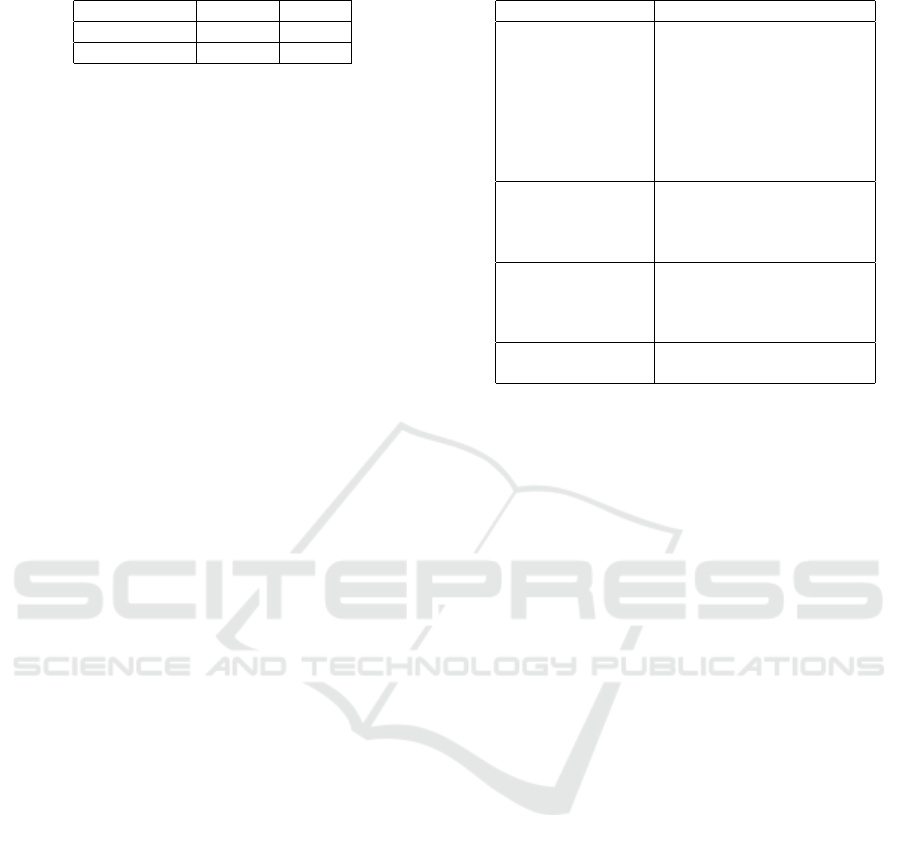
Table 1: Validation Results.
Average Drift Right(°) Left(°)
RMSE 5.2 4.8
Deviations 3.9 3.6
search conducted by Oess et al. (2012). The accuracy
of the glove is within an acceptable range for its ap-
plication, namely the measurement of large changes
in the ROM of the patients.
2.3 Candidate Testing
2.3.1 Study Participants
A total of 10 healthy participants were recruited. Par-
ticipation was completely voluntary with the recorded
data to remain disclosed through the use of num-
ber profiling. All participants were right-handed and
male, however this was not due to a selection crite-
rion, as the only requirement was the fit of the glove.
Both hands were tested across the same set of activ-
ities. This study was authorized and approved from
the Human Research Ethics Committee (Medical) at
the University of Witwatersrand. Both the principle
investigator and each participant signed a declaration
of consent before each test session.
2.3.2 Performing ADLs
To determine the dynamic range of motion of an in-
dividual participant as an active member of society,
testing must include activities that encompass the ex-
pected daily routine of said individual. Gracia et al.
(2017) investigated the suitability between the active
range of motion and the functional range of motion of
the dominant hand, during various activities of daily
living. The selection of the activities was based on the
International Classification of Functioning, Disability
and Health (ICF). The ICF is a basis for measuring
the level of health and disability for an individual or
a population. The ICF categories selected by Gracia
et al. (2017) were as follows: communication, mobil-
ity, self-care, and domestic life. By adhering to the
ICF chapters in the activity selection process, the cur-
rent study will be consistent with previous research.
Each candidate was required to perform a set of ac-
tivities derived from ICF categories using each hand.
The categories and corresponding activities selected
can be seen in Table 2.
The content of the study was explained to each po-
tential participant and an assessment of the fit of the
glove was made to determine whether a participant
was suitable. Participants then completed a question-
naire to determine hand dominance and whether the
participant had any relevant medical history.
Table 2: Activities measured in each ICF category.
ICF Category Action
Self-care Brushing teeth
Buttoning a shirt
Tying a shoelace
Pouring liquid
Drinking water
Eating with a spoon
Cutting with a knife
Eating with a fork
Mobility Holding a ball
Placing a ball in a cup
Flip a card
Open a lock
Technology and
Communication
Turning pages of a book
Typing numbers on a phone
Typing
Writing
Domestic Spray a white board
Wipe a white board
The principal investigator ensured the flexible sen-
sors were correctly positioned and secured before be-
ginning calibration. During calibration, the partici-
pant was required to keep their hand in a flat posi-
tion on top of a desk. This represents the 0
◦
position,
which was recorded by the device. Thereafter, the
participant gestured a specific fist, while ensuring that
all joints were as close to 90
◦
as possible. The prin-
cipal investigator closely investigated and corrected
the required hand positions. Once more, the data was
recorded. These two streams of data were averaged
and mapped to 0
◦
and 90
◦
, respectively.
The participant was directed to perform a certain
activity. Once observed, the candidate repeated the
activity while the device recorded the data. Follow-
ing data recording on both hands, an evaluation was
completed by the participant, indicating the level of
comfort while using the glove and any overall com-
ments that they may have had about the study.
3 COST
Components were sourced locally. The flexible sen-
sors were the highest-cost component (61% of the to-
tal cost), followed by the golf gloves and the micro-
controller. This is dependent on the number of sen-
sors used which was 10 in this study. Since this is
a critical component, cost reduction must be directed
elsewhere.
Nylon or nitrile gloves are non-stretch and will
thus simplify attaching the sensors to the gloves.
These therefore present a lower-cost alternative.
The resulting material cost of the prototype was
approximated to $121. Comparing the costs of the
Prototyping a Low-Cost Flexible Sensor Glove for Diagnostics and Rehabilitation
107
goniometer and the glove is not straightforward solely
based on their price. The goniometer, while more af-
fordable, involves a labor-intensive process for ther-
apists and may be particularly challenging for hand-
impaired patients. This could potentially lead to ex-
tended therapy sessions and higher overall costs in
terms of time and resources.
In contrast, the glove offers a more efficient
and technologically advanced approach. It not only
streamlines the measurement process, making it less
burdensome for both therapists and patients, but it
also introduces mechatronics into the rehabilitation
process, aligning with the broader goal of integrating
technology into local and rural healthcare practices.
4 RESULTS
The dynamic tests were successfully conducted on 10
participants. Both the dominant and non-dominant
hands were measured across a set of 20 activities.
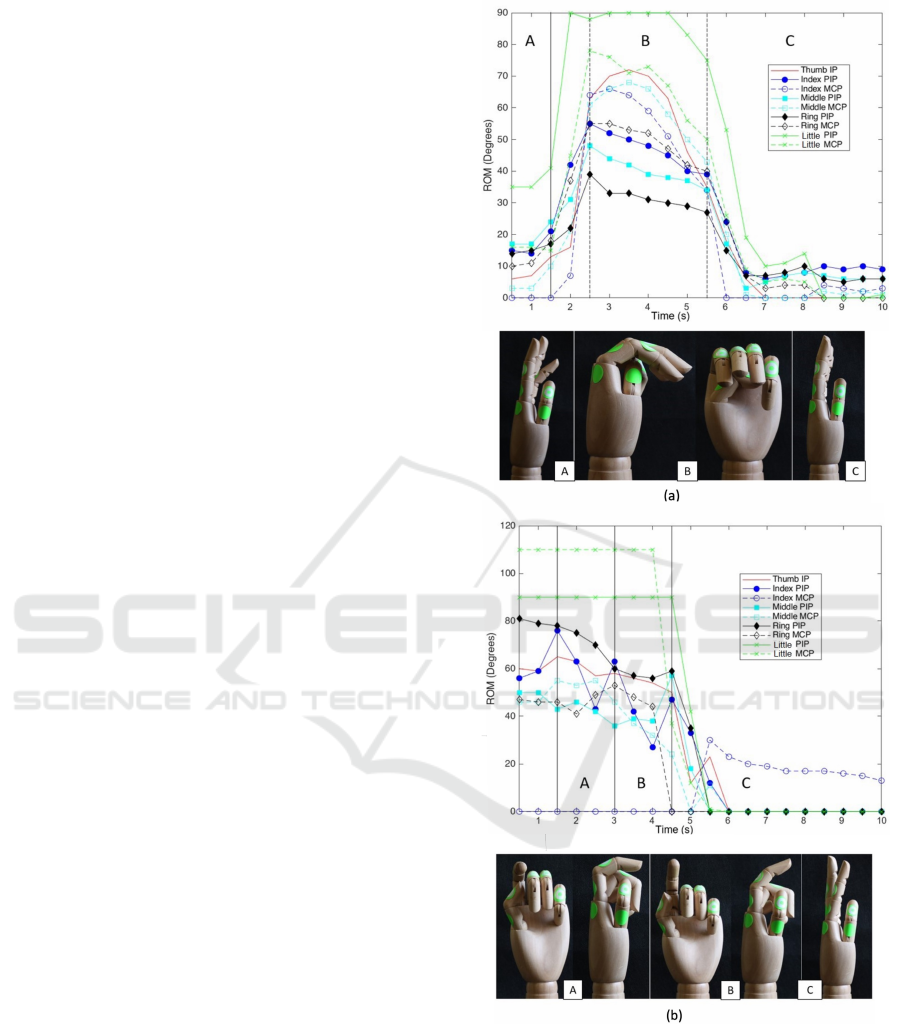
In Figure 7 (a) and (b), the ROM measured is de-
picted for two activities: (a) placing the ball into the
cup (Candidate 1 - left hand) and (b) pressing a spray
bottle (Candidate 10 - right hand). A wooden hand
model visually depicts the ROM by taking a few ref-
erence points from the graphs to position the hand
model.
4.1 Dynamic ROM
Figure 7(a) represents a collected motion of all the
finger joints while Figure 7(b) describes an action that
can be explained by the movements of a single joint
(PIP joint of the index finger).
4.2 Dominant vs. Non-Dominant Hand
and Joint Variation
An approximate of the amount of change observed be-
tween the joints can determine which joint or hand has
a greater degree of controlled motion. Based on this
premise, the coefficient of variance was calculated for
each hand and each joint for every participant, across
all activities. These values were then summed for
each participant to represent the total variation for
each hand. The total variation of both hands can be
seen in Figure 8.
Considering all participants as a whole, the varia-
tion amongst the joints were summed and are shown
in Figure 9.
Figure 7: (a) Candidate 1: Placing Ball Into a Cup, (b) Can-
didate 10: Using a Spray Bottle.
5 DISCUSSION
All 10 candidates performed all of the required activi-
ties with ease. The results produced from the study
were successful in recording the dynamic range of
motion. From Figure 7(a), all 9 joints began to in-
BIODEVICES 2024 - 17th International Conference on Biomedical Electronics and Devices
108
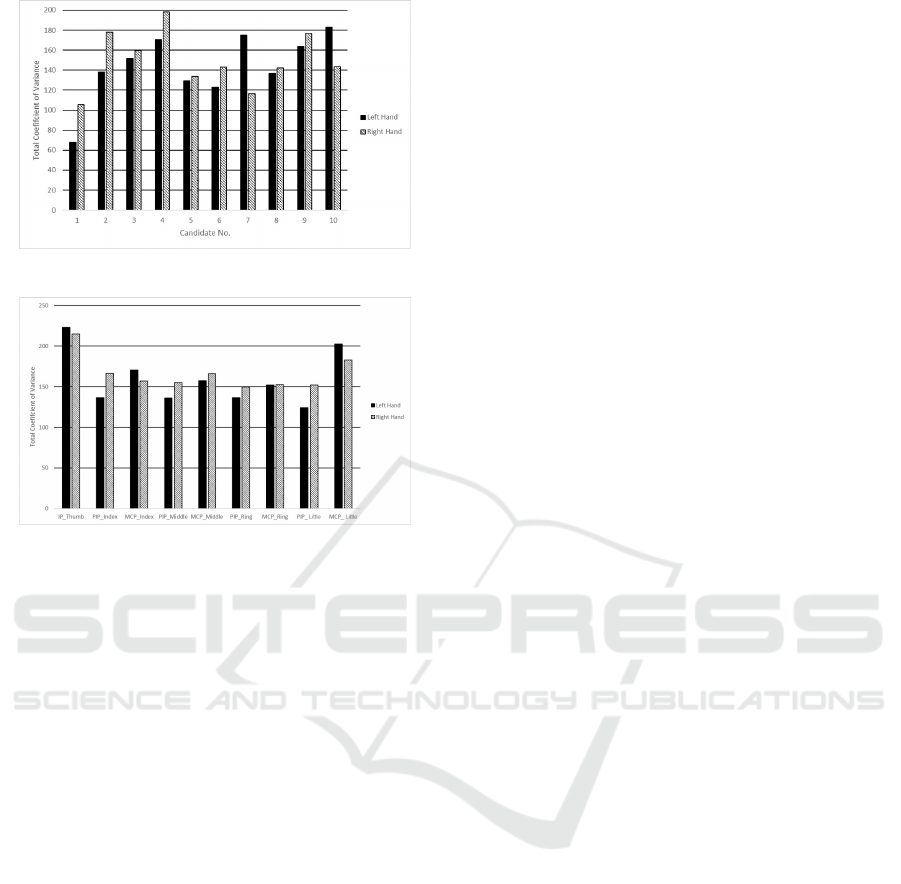
Figure 8: Total Hand Variation of all Candidates.
Figure 9: Total Variation across each Joint.
crease in ROM from time t = 1.5-2.5s. Thereafter a
slow decrease was observed until time t = 5.5 s, fol-
lowed by a rapid reduction in ROM. This behaviour
described the participants physical movements. For
example, from times t = 0 - 1.5 s (A) the candidate
was reaching for the ball. From times t = 2.5 - 5.5 s
(B) the ball was then picked up and placed into the
cup. Finally, from time t = 5.5 s (C) onwards the par-
ticipant had released the ball and their hand was back
in a neutral position.
Figure 7(b) describes an action that can be ex-
plained by the movements of a single joint. The task
was the action of pressing a spray bottle. The graph
shows two stages, times t = 1.5 -3 s (A), t = 3 - 4.5
s (B) corresponding to a dip and rise in the ROM of
the PIP joint in the index finger. These stages can be
seen as the pressing of the head on the spray bottle.
According to the ROM of all the joints, the spray bot-
tle is released from time t = 5 s onwards. The hand
model represents the changes of the PIP Joint.
Being able to correlate the results to a hand model
that resembles the requested activities can validate the
application of the glove as a device to monitor the
ROM of the hand. Previous studies have used fin-
ger goniometers (Bain et al., 2015; Hume et al., 1990;
Hayashi et al., 2014) as they are reliable devices for
joint measurements. However, they will require a pa-
tient to hold the requested gestures for longer peri-
ods as the therapist needs to measure each joint of
each finger. This may be difficult for hand-impaired
patients. Irrespective of the duration of the measure-
ments, the finger goniometer is targeted towards static
hand gestures while the current study is focused on
dynamic motions. Each activity was performed in
10 s with a recording every 0.5 s. By manipulating
the recording times, a smoother representation of the
hand motion can be attained. Thus, replacing the in-
stantaneous drops observed in the various plots with
a more detailed reduction in ROM.
It was expected that most participants would have
a greater variation in their right hands due to their
right-hand dominance. This can be seen in Figure
8. However, this was not the case for Candidate 7
and 10. This can be due to over-gripping gesture, ob-
served during the testing phase, of the non-dominant
hand when attempting the various activities as a result
of lack of control.
The IP joint of the thumb experiences the most
variation in both the left and right hands of all par-
ticipants (Figure 9). This is expected, as the thumb
is what separates humans from most animals because
it allows for complicated hand gestures. The thumb
promotes functionality in the forms of gripping and
pinching, which can correlate to the majority of the
tasks within the current study. Excluding the thumb
and summing the variation across each finger showed
that the maximum variation occurred in the little, in-
dex, middle and ring finger, in order of highest to low-
est. This trend was present in both the right- and
left-hand results. The little finger does not domi-
nate motion with respect to functionality however it
does achieve a full ROM due to its closed positioning
throughout the fundamental movements. For exam-
ple, when gripping or pinching a pencil from a neutral
position, the little finger would move from an opened
to a completely fisted position. This is due to the
thumb, index and middle finger dominating the ac-
tion. The index and middle finger support the thumb
in functional movements of the hand and thus exhibit
the next highest variation.
For the evaluation of the glove, the average rat-
ing (between 1-5, 5 being the most discomfort) was
2.02. Therefore, the prototype was mostly comfort-
able, throughout the procedure. However, this rating
is with respect to healthy candidates. Any level of
discomfort indicated by healthy participants could be
magnified in the case of a patient suffering with hand
impairment.
The reasoning of the slight discomfort had to do
with the sizing of the glove. Expanding the study will
require gloves of varying sizes. While the current de-
vice acts as a prototype, newer designs must be de-
veloped to cater for variation in hand size, but most
importantly patient comfort.
Prototyping a Low-Cost Flexible Sensor Glove for Diagnostics and Rehabilitation
109

6 CONCLUSIONS
The flexible sensor glove proved capable of measur-
ing the dynamic range of motion for each hand of all
10 participants. A hand model was positioned accord-
ing to the dynamic plots and resulted in replicated
hand gestures that would have occurred during the
specific activities. Being able to correlate the data to
the specific activity, confirms the capability of gloves
in measuring the dynamic ROM.
Comparisons were made between the dominant
and non-dominant hand of some participants. The re-
sults showed a greater ROM in the dominant hand for
most candidates. However, a few participants expe-
rienced a higher ROM in their non-dominant hand.
Based on these results and observations made during
the testing procedure, it was evident that some partic-
ipants would exaggerate their grip onto objects due to
lack of control with their non-dominant hand.
The variation of the motion between joints was
calculated using the coefficient of variance. The vari-
ation was more prominent amongst the right hand and
therefore could suggest dominance. The IP joint of
the thumb had a maximum variation of ROM for both
the left and right hand. The thumb is a significant joint
with respect to hand functionality and thus would ob-
serve a higher ROM throughout the activities.
According to the participants, the glove was mod-
erately comfortable, however new designs must be
implemented for the application on hand-impaired pa-
tients to achieve a maximum level of comfort and
safety. Apart from the design aspect, future work
should include a larger test scale, while introducing
static gestures for comparisons with previous work.
The prospective applications of the glove include
diagnostics, patient monitoring and rehabilitation. In
the case of diagnostics and patient monitoring the
glove can act as an aid to quantify the level of im-
pairment. Rehabilitation methods can incorporate
the glove with virtual reality systems or exoskele-
tons in the form of bilateral therapy. Specifically,
the glove holds promise in aiding individuals facing
challenges associated with stroke, radial nerve palsy,
tendinopathies and similar pathologies. However, for
the glove to act as an effective tool clinically, the study
needs to implement the above recommendations as
well as further testing.
REFERENCES
Bain, G., Polites, N., Higgs, B., and et al. (2015). The func-
tional range of motion of the finger joints. J Hand
Surg Eur Vol, 40(4):406–411.
De Klerk, S., Badenhorst, E., Buttle, A., and et al. (2016).
Occupation-based hand therapy in south africa: Chal-
lenges and opportunities. S Afr J Occup Ther,
46(3):10–15.
Gracia, V., Vergara, M., Sancho-Bru, J., and et al. (2017).
Functional range of motion of the hand joints in activ-
ities of the international classification of functioning,
disability and health. J Hand Ther, 30:337–343.
Hart, D. L. and Tepper, S. (2001). Changes in health status
for persons with wrist or hand impairments receiving
occupational therapy or physical therapy. American
Journal of Occupational Therapy, 55(1):68–74.
Hayashi, H., Shimizu, H., Okumura, S., and et al. (2014).
Necessary metacarpophalangeal joints range of mo-
tion to maintain hand function. Hong Kong J Occup
Th, 24(2):51–55.
Hume, M., Gellman, H., McKellop, H., and et al. (1990).
Functional range of motion of the joints of the hand. J
Hand Surg Am, 15(2):240–243.
Maredza, M., Bertram, M., and Tollman, S. (2015). Disease
burden of stroke in rural south africa: An estimate of
incidence, mortality and disability adjusted life years.
BMC Neurology, 15(1).
Maredza, M. and Chola, L. (2016). Economic burden of
stroke in a rural south african setting. eNeurologi-
calSci, 3:26–32.
Moodley, D. (2018). Radial nerve injuries. Interview - Oc-
cupational Therapist at Charlotte Maxeke Johannes-
burg Academic Hospital, SA.
Oess, N., Wanek, J., and Curt, A. (2012). Design and evalu-
ation of a low-cost instrumented glove for hand func-
tion assessment. J NeuroEng Rehabil, 9(1):1–11.
StatsSA (2015). Measuring household expenditure on pub-
lic transport. http://www.statssa.gov.za/?p=5943 - Ac-
cessed 28 January 2019.
Yan, L., Li, C., Chen, J., and et al. (2016). Preven-
tion, management, and rehabilitation of stroke in
low and middle-income countries. eNeurologicalSci,
2(8):21–30.
BIODEVICES 2024 - 17th International Conference on Biomedical Electronics and Devices
110
