
Predictive Models of Ward Admissions from the Emergency
Department
Laiene Azkue
1,2 a
, Jon Kerexeta
1,3 b
, Jorge Sampedro
4
, Moisés Espejo
4
and Nekane Larburu
1,3 c
1
Vicomtech Foundation, Basque Research and Technology Alliance, (BRTA), 20009 Donostia, Spain
2
Biomedical Engineering Department, Mondragon Unibertsitatea, 20500 Mondragón, Spain
3
Biodonostia Health Research Institute, 20014 San Sebastián, Spain
4
Asunción Klinika, 20400 Tolosa, Spain
mespejo@clinicadelaasuncion.com
Keywords: Emergency Department, Ward Admission, Predictive Models, Machine Learning, Artificial Intelligence.
Abstract: The demand for emergency department (ED) care has increased significantly in recent years, mainly due to
factors such as the increase in chronic diseases, aging population and urban population growth. The large
influx of patients can lead to overcrowding and resource allocation problems, which impact the quality of
care. A new tool to improve patient severity classification systems could improve ED care and avoid
inappropriate admissions. Therefore, we propose the development of an artificial intelligence model to predict
ED ward admissions. The proposed model uses electronic medical records from the Asunción Klinika in Spain
and environmental data. Three models are created at different stages of ED: arrival model which predicts
admission upon patient arrival, triage model which predicts admission after clinicians’ triage and the last one,
laboratory model which make use of triage model data and laboratory analysis to estimate the risk among the
most critical patients. The arrival model achieved an AUC of 0.801, the triage model achieved an AUC of
0.854, and the laboratory model achieved an AUC of 0.781. These models provide valuable information for
efficient patient management and resource allocation in the ED, contributing to improved patient care and the
adequacy of hospital admissions.
1 INTRODUCTION
The demand for emergency department (ED) care has
increased considerably worldwide in recent years.
During the pandemic, it is evident that due to
COVID-19 there has been a disproportionate increase
in demand on EDs, leaving them overwhelmed
(WHS, 2023). However, regardless of the pandemic,
there is a considerable increase due to factors such as
an aging population, increase in chronic diseases, lack
of access to primary care, urban population growth,
and changes in lifestyles (McKenna et al.,
2019),(Lowthian et al., 2011) .
Hospital management is affected by the
increasing demand for ED care. The high influx of
patients can lead to overcrowding, long waiting times,
and challenges in resource allocation, which can
a
https://orcid.org/0009-0009-2266-7985
b
https://orcid.org/0000-0002-6516-8619
c
https://orcid.org/0000-0003-0248-7783
impact quality of care and patient satisfaction (Sun et
al., 2013). Rapid identification of the worst-off
patients to prioritise patient care could improve it.
Clinicians’ triage plays a crucial role in today's
EDs. It is a patient stratification system that allows
the identification and prioritization of patients
requiring immediate medical attention. The triage
evaluates parameters such as vital signs,
symptomatology, and initial clinical assessment
(Yancey and O’Rourke, 2023). This task involves the
intervention of the clinical caregivers, which can be
costly. Artificial intelligence (AI) can provide rapid
and improved evaluation when assessing patients
according to their severity.
To address this issue, we propose the
development of three AI models capable of predicting
ward admissions from the ED in three different
Azkue, L., Kerexeta, J., Sampedro, J., Espejo, M. and Larburu, N.
Predictive Models of Ward Admissions from the Emergency Department.
DOI: 10.5220/0012202700003657
Paper published under CC license (CC BY-NC-ND 4.0)
In Proceedings of the 17th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2024) - Volume 2, pages 277-284
ISBN: 978-989-758-688-0; ISSN: 2184-4305
Proceedings Copyright © 2024 by SCITEPRESS – Science and Technology Publications, Lda.
277
sequential stages. Each stage requires different grades
of clinical involvement and clinical tests. Thus, the
models may detect high risk patients, which faster the
process without clinical involvement. These models
are based on various clinical factors, including the
patient's health status, diagnostic test results, severity
of the medical condition, and environmental factors
which differ in each stage.
Previously, we have conducted the following
systematic review, (Larburu et al., 2023), focusing on
predictive models for ED ward admission. This
review showed that logistic regression is the most
used algorithm, along with the gradient boosting
algorithm. The most frequently used variables are
triage and age. It is worth noting that all the reviewed
articles have an unbalanced nature. The systematic
review cover articles published between 2011 and
2022, with sample sizes ranging from 2,476 to
3,189,204 number of patients. The highest
performance was achieved by (Hong et al., 2018)
with the XGBoost algorithm, obtaining an AUC of
0.92 (95% CI 0.92-0.93).
The article is structured as follows: dataset section
summarizes the databases used and the general
characteristics of the database. Later, in the
methodology section, the models to be created and the
methodology carried out are exposed. Finally, the
results are presented, together with a discussion and
conclusions in the following two sections.
2 DATASET
Two types of data are used: electronic health records
(EHR), and environmental data.
EHR: The data used for analysis were obtained
from Asunción Klinika of Tolosa, Basque Country,
Spain. Once the study was approved by the
committee, the necessary data for the analysis were
provided. These retrospective data include vital signs,
laboratory results, details of performed tests,
demographic information, and more. The data covers
a period from January 1, 2004, to December 31, 2022,
encompassing a total of 284,503 emergency cases
involving 75,913 unique patients. It also includes the
target variable, which indicates whether the patient is
admitted to the ward or not. This variable is
unbalanced since 16.4% are admitted to the ward.
Environmental: Environmental data is extracted
from (Open-Meteo, 2023), an open-source weather
API service. This API provides access to
meteorological data from around the world. The data
come from various governmental meteorological
services and research organizations. The data covers
the period from January 1, 2004 to December 31,
2022 and they are from Tolosa. The environmental
data collected include the variables of temperature,
wind chill, solar radiation, precipitation, evaporation,
relative humidity, pressure, wind speed and gusts.
The two datasets are unified and a database with
196,659 instances and 255 predictor variables, since
EDs have been reduced to the year range 2010 to
2022, as triage was implemented in 2010. The target
variable is unbalanced, since the number of patients
not admitted to the ward is greater than the number of
patients admitted to the ward.
A total of 255 predictor variables can be classified
into the following categories (Table 1): demographic
(2), triage information (16), clinical and laboratory
findings (199), environmental (19) and others, that is,
uncategorized EHR variable (19).
Table 1: Description of predictor variables.
Quantity type
Demographic 2 -
Sex -
Categorical
Female 45.4%
Male 54.6%
Unknown 0.001%
Age (50.76±23.77) -
Numerical
-20 11.34%
20-40 24.05%
40-60 26.41%
+60 38.2%
Triage information 16 -
Triage -
Ordinal
categorical
0 – Non-urgent 0.006%
1 – Minor Urgent 0.95%
2 – Urgent 3.45%
3 – Emergency 18.51%
4 – Critical emergency 66.55%
5 – Immediate Life
Threatening
7.33%
NaN 3.2%
Vital signs Numerical
Clinical and laboratory
findings
199 -
Laboratory data 64 Numerical
tests performed 135 Categorical
Environmental 19 Numerical
Others 19 -
ED data 18
Numerical /
Categorical
Cause of attendance 1
Categorical
Common Disease 68.69%
Personal Accident 20.05%
Laboral Accident 5.7%
Sports Accident 2.13%
Traffic Accident 1.77%
School Accident 1.34%
Pregnancy 0.18%
Professional disease 0.134%
Undetermined 0.006%
HEALTHINF 2024 - 17th International Conference on Health Informatics
278
3 METHODS
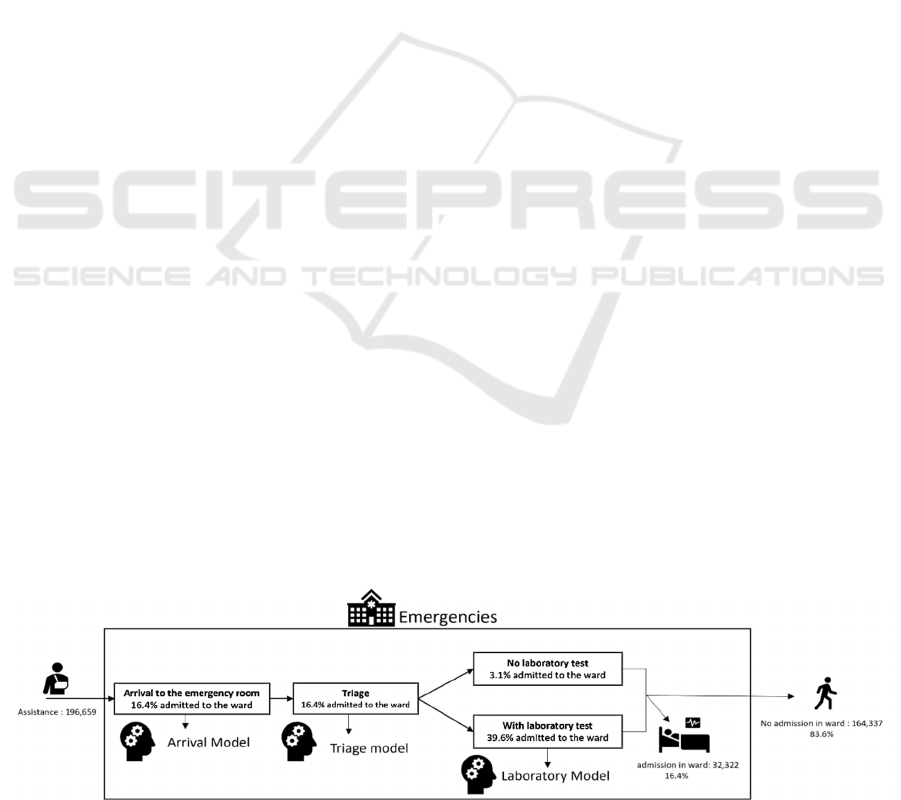
This section discusses the methodology to be carried
out for the creation of predictive models. The
objective is the prediction of ward admissions from
the ED. For this purpose, with the data provided by
Asunción Klinika and acquired by Open-Meteo, three
models are created at three different stages of the ED
attendance (Figure 1):
Arrival Model: Model able to predict ward
admission from the ED upon patient arrival. This
model is trained with data prior to triage, such as
demographic data and environmental variable data.
Triage Model: Model capable of predicting ward
admission from the ED after triage. This model is
trained with data available at triage, such as,
demographic data, environmental variables data and
data obtained at triage: the triage value and vital signs
acquired at triage.
Laboratory Model: Model able to predict ward
admission from the ED for patients undergoing
laboratory tests after triage (smaller population). This
model is trained with post-laboratory test data, such
as demographic data, environmental variable data,
triage data and laboratory test data.
These three models are an efficient and fast way
to classify urgent patients from non-urgent patients
from the first moment of care. As new tests/analyses
are carried out in the ED, more accurate models will
be used as they make use of this new information.
First, on arrival at the ED, we will have a result of the
arrival model to be able to estimate the patient's risk.
Secondly, after clinicians triage the patient, we will
be able to obtain the updated risk with this new
variable (triage model). Finally, in case the patient
has not yet been discharged and laboratory tests have
been conducted, the risk will be updated with these
tests (laboratory model).
3.1 Data Preprocessing
To ensure the data is clean and suitable for predictive
modelling, several preprocessing steps are applied.
Initially, One-Hot Coding is performed to transform
the categorical variables into numerical ones.
Subsequently, missing values are imputed using the
KNN (K-Nearest Neighbors) method (Juna et al.,
2022). Finally, the classes of the target variable are
balanced, but only in the training database (70%)
using the random undersampling technique.
3.2 Feature Selection
The most related variables with the admission in ward
are estimated using a combination of the Boruta
method and the importance of the dependent feature
of the XGBoost model. On the one hand, the Boruta
method is a feature selection technique that helps to
identify the most relevant variables in a dataset
(Kursa and Rudnicki, 2010). On the other hand, the
importance of the dependent feature of the XGBoost
model allows to evaluate the degree of influence that
each variable has on the prediction of the model. The
variables selected by both techniques have been
selected as the relevant ones for the predictive models.
This methodology is carried out on the triage
model, since this is the model that has been given
more importance. This is because in the state of the
art it is the most studied model, that is, all models use
the triage variable and focus on the instant after
triage. Then, among these variables, the clinicians’
triage related variables are discarded for arrival model
training. Similarly, the laboratory model is trained
with the variables selected for the triage model, plus
variables acquired after triage.
3.3 Predictive Models
The predictive models implemented include the
following algorithms: Logistic Regression, K-NN,
Gaussian Naives Bayes, Bernoulli Naives Bayes,
Decision Tree Classification, Random Forest
Figure 1: Predictive system workflow for the emergency department.
Predictive Models of Ward Admissions from the Emergency Department
279
Classification, Gradient Boosting Classifier (GBC),
eXtreme Gradient Boosting (XGBoost), AdaBoost
(Adaptive), CatBoosting (Categorical), LightGBM
(Light Gradient Boosting Machine), MLP (Multilayer
Perceptron) (Juna, 2022; Theng, 2020; Kelleher,
2020; Natras, 2022).
3.4 Evaluation Methods
For model evaluation, the database is divided into
training (70%) and validation (30%). The best
hyperparameters are searched in the training set using
GridSearch. Finally, a 10-fold cross-validation is
used during the training phase (Browne, 2000).
The
evaluation metrics used to assess the model's
performance in both the validation set and during
cross-validation training are as follows (Hossin and
Sulaiman, 2015): confusion matrix, ROC-AUC,
accuracy, precision, recall and F1.
4 RESULTS
This section presents the results obtained from each
of the three models (see Figure 1), along with their
optimal hyperparameters.
4.1 Triage Model
The triage model is the model that predicts ward
admission after the clinical caregivers have
conducted the triage. Hence, it makes use of triage
information for the prediction.
4.1.1 Training Triage Model
After the feature importance (see Section 3.2), it was
observed that triage, cause of attendance, age, and sex
are the main variables.
Table 2: Result of algorithm XGBoost in the training of
model triage.
XGBoos
t
AUC 0.854(95% IC 0.849-0.858)
Accurac
y
0.773(95% IC 0.768-0.777)
Precision 0.757(95% IC 0.750-0.763)
Recall 0.803(95% IC 0.796-0.810)
F1 0.779(95% IC 0.775-0.784)
With these variables, predictive models were
created using the 10-fold cross validation technique
with 70% of the database.
XGBoost algorithm obtained the best results with an
AUC value of 0.854 (95% CI 0.849-0.858) (Table 2).
4.1.2 Triage Model Validation Results
Validation is performed with the XGBoost algorithm
at the default threshold of 0.5. The model is validated
with the remaining 30% of the database. This model
obtains an AUC of 0.858. This model classifies
74.29% of the negative class correctly, in addition to
classifying 81.22% of the positive class correctly.
Table 3 shows that the value of precision and F1
score decreases due to the imbalance of the validation
dataset.
Table 3: Triage model comparison in training and
validation.
Trainin
g
Validation
AUC 0.854 0.858
Accurac
y
0.773 0.755
Precision 0.757 0.384
Recall 0.803 0.812
F1 0.779 0.521
4.2 Arrival Model
The arrival model is the model that predicts ward
admissions at the time of arrival at the ED, before the
triage. Therefore, an estimate of the triage or patient
status could be made with the output of the arrival
model, since clinicians have not yet get involved and
this model can help them in their decision making.
4.2.1 Training Arrival Model
For this model we have used the same variables as in
the triage model, except from triage information,
which has been removed, since this model aims to
predict the risk of ward admission before the triage.
Hence, the cause of attendance, age and sex are solely
used. With these variables, predictive models were
created using the 10-fold cross validation technique
with 70% of the database.
The best performing model is Gradient boosting
with an AUC value of 0.801 (95% CI 0.796-0.806)
(Table 4).
Table 4: Result of algorithm Gradient Boosting in the
training of model arrival.
Gradient Boostin
g
AUC 0.801(95% IC 0.796-0.806)
Accurac
y
0.731(95% IC 0.726-0.735)
Precision 0.721(95% IC 0.716-0.725)
Recall 0.753(95% IC 0.748-0.757)
F1 0.736(95% IC 0.732-0.741)
HEALTHINF 2024 - 17th International Conference on Health Informatics
280
4.2.2 Arrival Model Validation Results
The Gradient Boosting model was validated with the
0.5 threshold. The model obtained an AUC value of
0.805. It predicts well 76.82% of patients admitted to
the ward and 70.45% of those not admitted to the
ward.
Table 5 shows the difference between the training
and validation results. In general, all the metrics have
maintained their training value in the validation,
except the accuracy, and therefore, the f1 score. This
is because the training dataset is balanced, and the
validation dataset is not.
Table 5: Arrival model comparison in training and
validation.
Trainin
g
Validation
AUC 0.801 0.805
Accurac
y
0.731 0.715
Precision 0.721 0.338
Recall 0.753 0.768
F1 0.736 0.469
4.3 Laboratory Model
Laboratory model is the model which predicts ward
admission from the ED for patients after triage and
with laboratory tests. The database used in this model
is reduced from 196,659 emergencies to 71,982
emergencies since those were the ones that had
laboratory information. This is the 36.6% from
previous cases. The imbalance of the data changes:
from the total number of these cases (n=71,982),
39.59% are admitted to the ward.
4.3.1 Training Laboratory Model
In this model we used triage variables, cause of
attendance, age, sex, laboratory data (red blood cells,
hemoglobin, hematocrit, MCV, MCH, MCHC, etc),
vital signs and environmental variables (temperature,
thermal sensation, precipitation, etc). The Gradient
boosting model obtains the best results with an AUC
value of 0.788 (95% CI 0.785-0.792) (Table 6).
Table 6: Result of algorithm Gradient Boosting in the
training of model laboratory.
Gradient Boostin
g
AUC 0.788 (95% IC 0.785-0.792)
Accurac
y
0.715 (95% IC 0.712-0.718)
Precision 0.719 (95% IC 0.716-0.723)
Recall 0.705 (95% IC 0.699-0.711)
F1 0.712 (95% IC 0.709-0.716)
4.3.2 Laboratory Model Validation Results
The selected model has been validated and the results
of the Table 7 are obtained. Considering that the
population has been reduced by discarding patients
who are initially in the best condition (n=71,982), it
is understandable that the predictive ability decreases
among the severe patients. Therefore, we have
applied the triage model in this reduced cohort to
compare whether the use of laboratory data improves
the predictive ability.
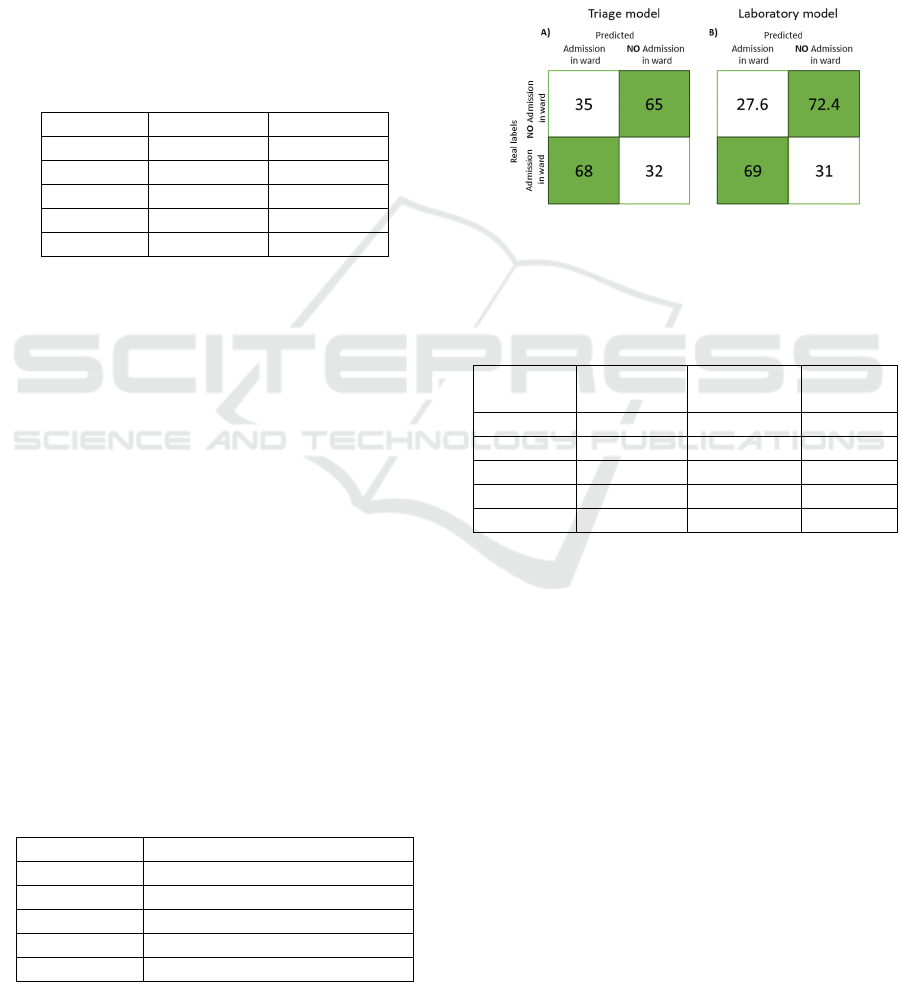
Figure 2: Confusion matrices (in %) to compare the triage
model (a) and the laboratory model (b) in the validation set
of the reduced data.
Table 7: Laboratory model comparison in training and
validation with the triage model in the reduced database.
Training Validation
Triage
model
AUC 0.781 0.779 0.728
Accurac
y
0.711 0.710 0.662
Precision 0.622 0.622 0.561
Recall 0.691 0.685 0.680
F1 0.654 0.652 0.615
The results of the laboratory model based on
laboratory data outperform both in validation and
training the results of the triage model in the reduced
database, as shown in the Table 7. A comparison of
the classification of laboratory model (b) and the
triage model in this cohort (a) can be seen in Figure 2
For positive predictions, laboratory model improves
by 1.08% over the triage model. In the case of
negative predictions, it improves by 7.33%, taking
into account that this class is the majority class.
5 DISCUSSION
Promising results were obtained using three
predictive models at different times during
emergency care: arrival model, triage model and
laboratory model. These three models predict ward
admission, but at different stages of Emergency
Predictive Models of Ward Admissions from the Emergency Department
281
Department (ED): arrival model predicts admission to
the ward on arrival of the ED, whereas the triage
model predicts it after triage has been performed.
Finally, laboratory model predicts ward admission for
patients undergoing laboratory tests, that is, it is a
model trained with a smaller population than the other
two models.
These models benefit healthcare personnel in
patient management by providing the ability to
evaluate ward admission at different points of care.
The accuracy of the models improves with an
increased number of tests conducted. Consequently,
the laboratory model demonstrates greater predictive
capacity compared to the arrival model. In addition,
the arrival model proves valuable in estimating
potential ward admissions prior to triage. Thus,
during periods of high demand, it may be possible to
create two care pathways: one with patients with a
high probability of admission and the other with
patients with a low probability of admission. This
approach could minimize the collapse in the ED and
enhance overall management. These models are
useful tools for the effective management of patients
according to their needs and can avoid unnecessary
admissions, improving not only the quality of care but
also patient safety. The following Table 8 shows the
results obtained for each model.
Table 8: Results of the ED workflow.
Nº Va
r
n AUC
Arrival model 3 196,659 0.805
Triage model 4 196,659 0.858
Laborator
y
model 55 71,982 0.779
There are 196,659 emergency room attendances.
The arrival model has obtained an AUC value of
0.805, with the use of 3 predictor variables (cause of
attendance, age and sex) and the Gradient Boosting
model.
Afterwards, the patient is triaged by nursing and
with this evaluation, another model (triage model) is
created to improve the capacity of the initial model
(arrival model). The triage model makes use of the
XGBoost algorithm and uses 4 variables, which are
the same as those used in the arrival model, together
with the triage value. An AUC value of 0.858 and a
precision of 0.440 is obtained. A low precision value
is obtained since the data are unbalanced (83.6%
negative class and 16.4% positive class). This implies
that the model has a tendency to predict the majority
(negative) class more frequently due to the higher
number of examples in the dataset. As a result, the
model accuracy is affected. But actually, the model is
able to correctly predict 72.70% of the positive class
and to incorrectly predict 18.13% of the negative
class. However, having the database unbalanced the
number of patients in the 18.13% of the negative class
is higher than the 72.70% of the positive class, which
lowers the accuracy result.
Finally, an additional model (laboratory model) is
developed with the aim of predicting the need for
ward admission for those patients undergoing
laboratory tests. It is important to note that these
patients, in general, present a more severe health
condition compared to those who do not undergo such
tests. Therefore, this model is trained with a reduced
database (n=71,982) with the gradient boosting
algorithm, of which 39.6% are admitted to the ward.
In this model the 4 variables of the previous arrival
model used together with laboratory results data, vital
signs data and environmental data, obtaining an AUC
value of 0.781. The AUC decreases with respect to
the triage model, but this model is not the best model
to compare whether the AUC has improved. This is
because the two models have been trained with
different databases, that is, the triage model has been
trained with a database of 196,659 urgencies,
including those in best condition, and the laboratory
model with a database of 71,982 urgencies, which are
supposed to be the most severe patients. Therefore,
these results have been compared with a new triage
model, which makes use of the same reduced
database, but only with triage model variables, i.e.
without laboratory tests information. As for the AUC
value, the value of this new triage model is 0.728 and
the laboratory model obtains a value of 0.781, thus
improving predictivity. This model does not greatly
increase the correct prediction of the positive class,
but it reduces the number of false positives.
6 CONCLUSION
Three machine learning models have been developed
to predict ward admissions from the ED at various
stages during the emergency care process. In these
three models triage, age and cause of care variables
are the most important ones in terms of prediction. In
addition, the best performing models are XGBoost
and Gradient boosting. The arrival model is useful for
identifying patients who may require ward admission
from the beginning of their ED care, without triage.
The triage model, with the inclusion of the triage
value, improves predictive ability later in the process.
On the other hand, laboratory model focuses on
patients undergoing laboratory tests, offering greater
predictive accuracy for this specific group.
HEALTHINF 2024 - 17th International Conference on Health Informatics
282

Regarding the results obtained and the results of
the systematic review by (Larburu et al., 2023) which
summarizes the articles dealing with predictive
models of ward admissions, it can be seen that even
without the clinicians triage variable, the arrival
model exceeds a quarter of the articles in the
systematic review, which make use of variables at
triage. Therefore, this initial model, achieves results
comparable with the literature but without the need of
clinician’s involvement.
In the case of the triage model, we observe that
three studies demonstrate superior results in terms of
AUC: 0.92 (Hong et al., 2018), 0.89 (Cusidó et al.,
2022), and 0.877 (Cameron et al., 2015). It is worth
noting that these three articles have been trained on
much larger databases, consisting of 560 thousand, 3
million, and 255 thousand instances, respectively. We
have identified six articles that achieve similar AUC
value (confidence intervals overlap), generally
characterized by a comparable database size (Sun et
al., 2011; Martinez et al., 2012; Zlotnik et al., 2016;
Graham et al., 2018; Lucke et al., 2018; De Hond et
al., 2021). Lastly, our model outperforms five
articles, all of which, except for one (more than a
million instances), make use of much smaller
databases (Noel et al., 2019; Parker et al., 2019; Brink
et al., 2020; Feretzakis, Karlis, et al., 2022;
Feretzakis, Sakagianni, et al., 2022).
Finally, it is important to note that the laboratory
model cannot be directly compared with the models
in the systematic review. This is because the
laboratory model is trained on a small population
consisting specifically of patients undergoing
laboratory tests in the ED, patient in worse condition.
These machine learning models offer an
opportunity to improve the management and
efficiency of emergency departments from a clinical
perspective. These models can help prioritize and
allocate resources more effectively, streamlining
floor admission processes and optimizing patient
care, as well as achieving more efficient management
of available resources, ensuring timely and
appropriate care for each patient, and thus improving
clinical outcomes in the ED setting. Additionally,
these models can play a relevant role in reducing
hospital admission inadequacy, which directly
translates into improvements in patient safety (Puig et
al., 2004).
However, it is important to mention some
limitations of the study. One important limitation to
consider is the applicability of the model to different
clinical contexts or settings. Since machine learning
models are trained with data specific to a particular
institution or context, it is possible that their
performance and predictive ability may be affected
when applied in other settings with different
characteristics. The variables used in the model may
be related to clinical practice and procedures specific
to the home institution, which could limit its
usefulness elsewhere where the relevant variables
may vary.
ACKNOWLEDGEMENTS
The authors would like to thank INVIZA-Asunción
Klinica and STT Systems for their support in the
INURGE project. This work has been funded by the
research project INURGE (ZL-2022/00571) of the
Basque Government’s HAZITEK programme from
the public agency SPRI.
ETHICAL COMMITEE
The study was conducted in accordance with the
Declaration of Helsinki and approved by the Research
Ethics Committee of the Gipuzkoa Health Area
(protocol code SAMURG-2022-01, 6 February
2023).
REFERENCES
Brink, A., Alsma, J., Brink, H. S. et al. (2020). Prediction
admission in the older population in the Emergency
Department: the CLEARED tool. Neth J Med 78, 357–
367
Browne, M. W. (2000). Cross-Validation Methods. J Math
Psychol 44, 108–132. https://doi.org/10.1006/jmps.19
99.1279.
Cameron, A., Rodgers, K., Ireland, A. et al. (2015). A
simple tool to predict admission at the time of triage.
Emerg Med J 32, 174–179
Cusidó, J., Comalrena, J., Alavi, H. et al. (2022). Predicting
Hospital Admissions to Reduce Crowding in the
Emergency Departments. Appl Sci 12, 10764
De Hond, A., Raven, W., et al. (2021). Machine learning
for developing a prediction model of hospital admission
of emergency department patients: Hype or hope? Int J
Med Inf 152, 104496
Feretzakis, G., Karlis, G., et al. (2022). Using machine
learning techniques to predict hospital admission at the
emergency department. J Crit Care Med 8, 107–116
Feretzakis, G., Sakagianni, A., Loupelis, E. et al. (2022).
Predicting Hospital Admission for Emergency
Department Patients: A Machine Learning Approach.
Stud Health Technol Inf, 297–300
Predictive Models of Ward Admissions from the Emergency Department
283

Graham, B., Bond, R., et al. (2018). Using data mining to
predict hospital admissions from the emergency
department. IEEE Access 6, 10458–10469
Hong, W. S., Haimovich, A. D. and Taylor, R. A. (2018).
Predicting hospital admission at emergency department
triage using machine learning. PloS One 13, e0201016
Hossin, M. and Sulaiman, M. N. (2015). A review on
evaluation metrics for data classification evaluations.
Int J Data Min Knowl Manag Process 5, 1
Juna, A., Umer, M., Sadiq, S. et al. (2022). Water quality
prediction using KNN imputer and multilayer
perceptron. Water 14, 2592
Kelleher, J. D., Namee, B. M. and D’Arcy, A. (2020).
Fundamentals of Machine Learning for Predictive
Data Analytics, second edition: Algorithms, Worked
Examples, and Case Studies. MIT Press.
Kursa, M. B. and Rudnicki, W. R. (2010). Feature Selection
with the Boruta Package. J Stat Softw 36, 1–13.
https://doi.org/10.18637/jss.v036.i11.
Larburu, N., Azkue, L. and Kerexeta, J. (2023). Predicting
Hospital Ward Admission from the Emergency
Department: A Systematic Review. J Pers Med 13, 849.
https://doi.org/10.3390/jpm13050849.
Lowthian, J. A., Curtis, A. J., Cameron, P. A. et al. (2011).
Systematic review of trends in emergency department
attendances: an Australian perspective. Emerg Med J
28, 373–377. https://doi.org/10.1136/emj.2010.099226.
Lucke, J. A., de Gelder, J., et al. (2018). Early prediction of
hospital admission for emergency department patients:
a comparison between patients younger or older than 70
years. Emerg Med J 35, 18–27
Martinez, E., Fernández, C., et al. (2012). Prediction model
for in-hospital admission in patients arriving in the
emergency department. In Anales del Sistema Sanitario
de Navarra (207–217)
McKenna, P., Heslin, S. M., et al. (2019). Emergency
department and hospital crowding: causes,
consequences, and cures. Clin Exp Emerg Med 6, 189–
195. https://doi.org/10.15441/ceem.18.022.
Natras, R., Soja, B. et.al. (2022). Ensemble Machine
Learning of Random Forest, AdaBoost and XGBoost
for Vertical Total Electron Content Forecasting.
Remote Sens 14, 3547. https://doi.org/10.3390/
rs14153547.
Noel, G., Bonte, N., et al. (2019). Real-time estimation of
inpatient beds required in emergency departments. Eur
J Emerg Med 26, 440–445
Open-Meteo (2023). Open-Meteo. Available at:
https://openmeteo.substack.com/embed [Accessed
December 22, 2023].
Parker, C. A., Liu, N., Wu, S. X. et al. (2019). Predicting
hospital admission at the emergency department triage:
A novel prediction model. Am J Emerg Med 37, 1498–
1504
Puig, C., Carrasco, G., et al. (2004). Factores asociados a la
inadecuación de los ingresos por urgencias en un
hospital privado de tercer nivel. Rev Calid Asist 19,
363–369. https://doi.org/10.1016/S1134-282X(04)777
25-8.
Sun, B. C., Hsia, R. Y., et al. (2013). Effect of emergency
department crowding on outcomes of admitted patients.
Ann Emerg Med 61, 605-611.e6. https://doi.org/10.1016
Sun, Y., Heng, B. H., Tay, S. Y. et al. (2011). Predicting
hospital admissions at emergency department triage
using routine administrative data. Acad Emerg Med 18,
844–850
Theng, M. and Theng, D. (2020). Machine Learning
Algorithms for Predictive Analytics: A Review and New
Perspectives. https://doi.org/10.37896/HTL26.06/1159.
WHS (2023). World health statistics 2023: monitoring
health for the SDGs, sustainable development goals.
Yancey, C. C. and O’Rourke, M. C. (2023). Emergency
Department Triage. In StatPearls. Treasure Island (FL):
StatPearls Publishing. Available at: http://www.
ncbi.nlm.nih.gov/books/NBK557583/ [Accessed June
23, 2023].
Zlotnik, A., Alfaro, M. C., et al. (2016). Building a decision
support system for inpatient admission prediction with
the Manchester triage system and administrative check-
in variables. CIN Comput Inform Nurs 34, 224–230
HEALTHINF 2024 - 17th International Conference on Health Informatics
284
