
Curcuma Extract as an Alternative and Safety Pain Reliever for
Geriatric with Knee Osteoarthritis: A Systematic Review and Meta
Analysis
Mohammad Satrio Wicaksono
a
, Clarissa Aulia Pravitha
b
and Hamdi Ramadhan Daulay
c
Faculty of Medicine, Diponegoro University, Semarang, Indonesia
Keywords: Curcuma Extract, Osteoarthritis, Geriatric.
Abstract: Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) as pain relievers for osteoarthritis patients that have
several side effects in long-term treatment. Meanwhile based on Global Burden of Disease 2019, about 528
million people have osteoarthritis, which 73% are geriatric patients. Therefore, this study aimed to evaluate
the efficacy and safety of curcuma extract compared to NSAIDs in the treatment of geriatric patients with
knee osteoarthritis. This study was made with a systematic literature search method from three databases,
such as PubMed, ScienceDirect, and ProQuest. Inclusion criteria included experimental randomized control
trials and discussed related topics. Mean difference and standard deviation were displayed as the results. With
an I2 value of less than 40%, a fixed-effect model was suggested. For randomized trials, the Cochrane risk-
of-bias tool was used to evaluate the risk of bias (RoB 2). There were a total of 671 participants in five
randomized control trial trials. The pooled mean difference of the VAS score decreased significantly, with a
95% confidence interval (CI) of (-2.97) - (-0.92), P=0.0002, and an I2 of 99%. The I2 data for the KOOS
index indicates 0%, and the pooled mean difference is a significant 2.82 [95% CI: 1.48-4.16, P<0.0001].
NSAID-like medications and curcuma extracts are similar in terms of effectiveness and safety.
1 INTRODUCTION
The most prevalent kind of arthritis worldwide is
called osteoarthritis (OA), affecting around 528
million individuals, 73% of whom are elderly.
(Global Burden of Disease Collaborative Network,
2019). More than half of OA patients experience knee
pain, generally called knee osteoarthritis (KOA),
which affects more than 300 million people around
the world (Vos et al., 2016). Globally, the average
yearly indirect expenditures per patient in 2013 were
between $300 and $17,700 (Salmon et al., 2016).
Meanwhile in Indonesia based on Riset Kesehatan
Dasar (Riskesdas) in 2018, the prevalence of joint
diseases including OA in the population over 15 years
old was 7.3% and the percentage of people over 55
years old was 53.15% (Badan Penelitian dan
Pengembangan Kesehatan Kementerian RI, 2018).
a
https://orcid.org/0000-0001-6004-9461
b
https://orcid.org/0009-0005-0629-2192
c
https://orcid.org/0009-0001-5694-0769
Multiple risk factors, mechanical stress, and
abnormal joint movement combine to cause OA, an
inflammatory disease that typically manifests as joint
pain and loss of function. Articular cartilage changes
lead to surface fibrillation, irregular cartilage, and
focal erosion (Stewart & Kawcak, 2018). Although
OA is not a deadly disease, previous studies showed
that pain, stiffness, and physical abilities of patients
with OA have impacted in decreasing their quality of
life such as physical, social, and environmental
health. The activities that were often reported as a
problem were using the toilet, walking up the stairs,
and heavy housework (Wojcieszek et al., 2022). Not
only disrupted activities but also OA can impact
mental issues like depressive disorders (Campbell et
al., 2015). Currently, the drugs needed to eliminate
OA are not available.
Therefore, therapies are needed that can manage
symptoms, reduce disease progression, minimize
disability, and improve quality of life. Available
Wicaksono, M. S., Pravitha, C. A. and Daulay, H. R.
Curcuma Extract as an Alternative and Safety Pain Reliever for Geriatric with Knee Osteoarthritis: A Systematic Review and Meta Analysis.
DOI: 10.5220/0013666200003873
Paper published under CC license (CC BY-NC-ND 4.0)
In Proceedings of the 1st International Conference on Medical Science and Health (ICOMESH 2023), pages 69-77
ISBN: 978-989-758-740-5
Proceedings Copyright © 2025 by SCITEPRESS – Science and Technology Publications, Lda.
69

therapies are pharmacological, non-pharmacological,
and surgical therapies. For pharmacologic therapy,
according to the IRA Recommendations for
Osteoarthritis, the most common management of OA
can be Analgesic Acetaminophen (paracetamol)
and/or topical and oral NSAIDs (Perhimpunan
Reumatologi Indonesia, 2014). Longterm use of
NSAID drugs will have side effects on the
development of gastric mucosal injury and induced
nephrotoxicity including electrolyte imbalance such
as hyperkalemia (Bindu et al., 2020; Wongrakpanich
et al., 2018). Moreover, in the cardiovascular system,
NSAIDs may be associated with increased blood
pressure by 5 mmHg on average and risk of
congestive heart failure (Wongrakpanich et al.,
2018).
Currently, treatment with the concept of back to
nature where the concept uses herbal ingredients is
widely used by the Indonesian people, especially in
elderly or geriatric patients. Turmeric (Curcuma
longa), is a natural ingredient which very often used
by Indonesians as an herbal treatment and as the main
choice as an adjuvant pharmacological treatment. In
addition to being cheap and easy to obtain, turmeric
(Curcuma longa) has minimal side effects compared
to pharmacological drugs (Mozaffari-Khosravi et al.,
2016).
These natural ingredients can act as anti-
inflammatories by inhibiting inflammatory mediators
such as TNF-α, IL-1β, and PGE2 and reducing pain
in OA patients (Heidari-Beni et al., 2020; Singhal et
al., 2021). The mechanism of treatment with turmeric
(Curcuma longa) has the same goal as
pharmacological treatment, namely reducing
symptoms in geriatric patients with OA. There is a
main compound, curcumin, which is effective in
managing pain in OA patients. The mechanism itself
involves inhibiting the production of COX-2,
phospholipase A2 (cPLA2), and 5-lipoxygenase (5-
LOX); protection of IL-1β which causes chondrocyte
apoptosis; and preventing cartilage degeneration in
joints (Srivastava et al., 2016).
The purpose of this systematic review and meta-
analysis is to examine the safety and efficacy of
treating elderly people with osteoarthritis using
natural components vs NSAIDs.
2 MATERIAL AND METHOD
The Preferred Reporting Items for Systematic
Reviews and Meta-Analyses (PRISMA) guidelines,
which are available at (https://prisma-statement.org/),
served as the foundation for this systematic review.
2.1 Eligibility Criteria
Eligible criteria included in this study were original
research articles or research reports using human
studies with randomized controlled trial design.
Criteria for included studies were determined using
PICO criteria shown in Table 1. Technical reports,
editor answers, scientific posters, study protocols,
conference abstracts, narrative reviews, systematic
reviews, meta-analyses, non-comparative research, in
silico, in vitro, and in vivo investigations were among
the papers that were eliminated. Articles with non-
English, unrelated themes, and full-text availability
issues were also eliminated.
Table 1: PICO Criteria for Included Studies.
Population Geriatric patients with knee
osteoarthritis
Intervention Curcuma extract consumed orall
y
Com
p
arison Placebo and NSAID
Outcome Visual Analog Scale (VAS) and Knee
Injury and Osteoarthritis Outcome Score
(KOOS)
2.2 Outcome Measures
The Knee Injury and Osteoarthritis Outcome Score
(KOOS) and Visual Analog Scale (VAS) pain ratings
were the outcome measures evaluated in this
systematic review and meta-analysis. Both scoring
methods were applied to quantify the degree of
discomfort associated with osteoarthritis in the knee.
Patients with osteoarthritis utilized the VAS score
to gauge their level of knee discomfort. It has word
descriptions in the range of 0 to 10 (in centimetres),
where "0" denotes "no pain" and "10" denotes
"unbearable or severe pain." The patient filled it out
by checking the boxes for light, moderate, severe, and
no discomfort. (Burckhardt & Dupree Jones, 2003).
KOOS is a self-assessment questionnaire
designed to help people evaluate their own knee
injuries. Five subscales make up the KOOS, and each
is assessed independently: There are nine items
related to pain; seven items to symptoms; seventeen
items related to everyday living; five items related to
sports and leisure; and four things related to quality
of life. There are five alternative answers for each
item, ranging from 0 (none) to 4 (severe). The results
were converted to a 0-100 scale, where 0 denoted
ICOMESH 2023 - INTERNATIONAL CONFERENCE ON MEDICAL SCIENCE AND HEALTH
70
very serious knee issues and 100 denoted no knee
discomfort.
Table 2: Keyword Used in Literature Searching.
Database Ke
y
words
Pubmed ((((((curcuma[MeSH Major Topic]) OR
(Curcuma longa[Title/Abstract])) OR
(turmeric[Title/Abstract])) AND
(geriatric[MeSH Major Topic])) AND
(osteoarthritis[MeSH Major Topic])) OR
(arthritis[Title/Abstract])) OR
(degenerative[Title/Abstract])
ProQuest (Curcuma OR (Curcuma longa) OR
Turmeric AND (Osteoarthritis knee) AND
Geriatric)
Science
Direct
(Curcuma OR “Curcuma longa” OR
Turmeric) AND (Geriatric) AND
(Osteoarthritis OR Arthritis OR
Degenerative)
2.3 Data Source and Search
Acquired studies have been collected using searching
databases, such as PubMed, ProQuest, and Science
Direct. The search was conducted from the inception
of the database until December 2022. The keywords
used were using Boolean operator and mesh in each
database which can be seen in Table 2. The studies
are stored in the authors’ library using the Mendeley
group reference manager.
2.4 Selection Process
After searching keywords written in Table 2, we used
article type filters on each database to exclude the
non-RCT articles. Results from 3 databases were later
combined and screened by three independent
reviewers through title, year of publication, and DOIs
for duplicate removal. After duplicate removal,
studies were later screened through abstract and full
paper for irrelevance removal. The PRISMA flow
chart contained records of the study selection
procedures.
2.5 Data Collection Process
Studies after final screening are extracted for the
relevant data and recorded in Google Spreadsheet.
The recorded data were: (1) first author, year, (2)
country, (3) sample size, (4) gender, (5) mean age, (6)
name of intervention, length of intervention,
comparison, and (7) outcome that consist of VAS
score and KOOS index. All statistical tests for this
meta-analysis were conducted using Review
Manager (RevMan) v5.4 (Cochrane Collaboration,
UK).
2.6 Study Risk of Bias Assessment
(Quantitative Synthesis)
The Cochrane risk-of-bias tool for randomized trials
(RoB 2), which is available at
(https://methods.cochrane.org/bias/resources/rob-2-
revised-cochrane-risk-bias-tool-randomized-trials),
was used by three independent reviewers to evaluate
each research that was included in this investigation.
Later, the disparate conclusions made by reviewers
were reviewed and settled among themselves.
2.7 Quantitative Data Synthesis
(Meta-Analysis)
In this review, data on Mean Difference (MD) and
Standard Deviation (SD) were computed. When the
included studies were deemed homogeneous (little
variability in study findings or variance owing to
random error), as shown by an I2 value of less than
40%, a fixed-effect model (FEM) was applied. If not,
a random-effect model (REM) was employed. A
forest plot was used to display the pooled estimate.
3 RESULTS
3.1 Study Selection
After conducting literature searching from 3
databases which are PubMed, ProQuest, and
ScienceDirect, 290.368 studies were generated.
Automation tools from each database were used to
exclude non-RCT studies, resulting in 282.254
articles being excluded. Then, 1.414 were removed
due to duplicate articles. Later, authors assessed all of
the remaining articles from the title and abstract for
irrelevance to the topic, resulting in 6.669 articles
excluded. 5 articles were then excluded for the
unavailable full-text availability. Lastly, the author
assessed eligibility for all the studies and agreed to
exclude 17 studies because of an unpresent outcome
of interest. Five papers were included in this study for
the meta-analysis and systematic review. Figure 1
shows the flow chart of the PRISMA diagram used to
select our studies.
Curcuma Extract as an Alternative and Safety Pain Reliever for Geriatric with Knee Osteoarthritis: A Systematic Review and Meta Analysis
71
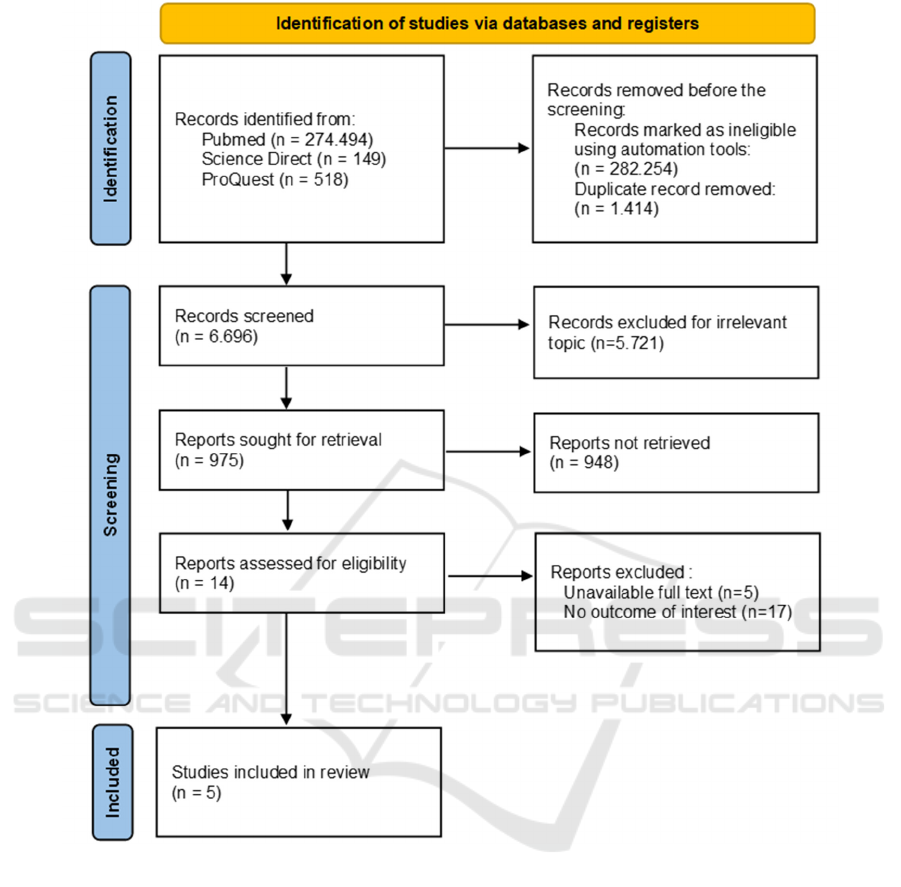
Figure 1: PRISMA 2020 Flow Diagram
3.2 Study Characteristic
From the five studies included in this review, the total
number of participants is 671 participants. Most of
the studies (n=5) observed the elderly participants for
their studies, but only 1 study from Henrotin et al,
researched geriatric (> 60-year-old) patients. The rest
of the included studies were approached 60 years of
age for their participants. The study characteristics
are shown in Table 3.
3.3 Risk of Bias in Studies
To assess the quality of each study, the Cochrane risk-
of-bias instrument for randomized trials (RoB 2) was
utilized. One study showed a high risk of bias
(Srivastava et al) because there is a bias due to the
intended intervention being balanced between groups
and missing outcome data causing participants lost to
follow-up. Four studies showed some concern (Shep
et al, Madhu et al. al, Henrontin et. al, Lopresti et. al)
because there is an intended intervention as a rescue
medication in each trial group. The risk of bias is
summarized in Figure 2.
ICOMESH 2023 - INTERNATIONAL CONFERENCE ON MEDICAL SCIENCE AND HEALTH
72
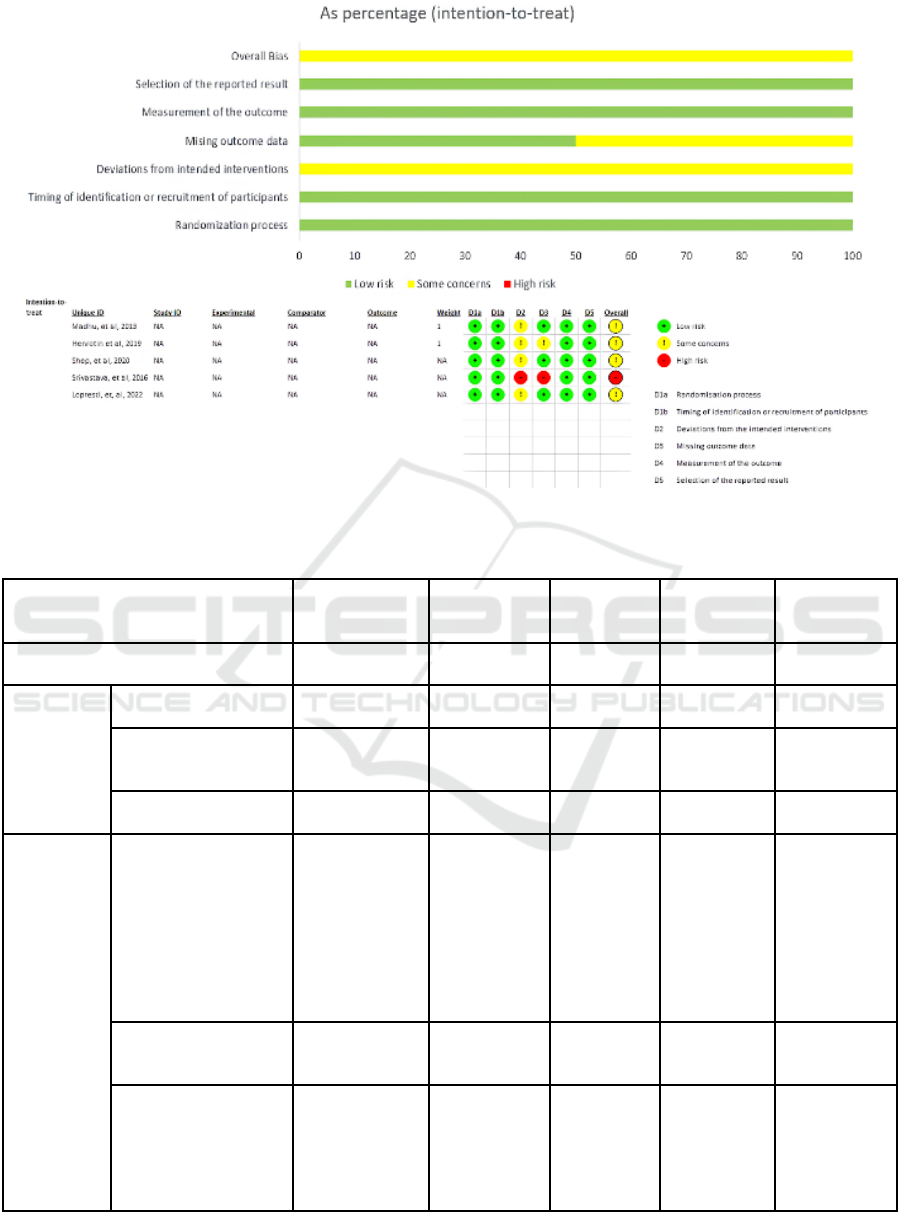
Figure 2: Risk of Bias Assessment Result
Table 3: Characteristic of Studies.
Author, Year
Madhu, et al,
2013
17
Srivastava, et
al, 2016
14
Lopresti, et
al. 2022
18
Shep, et al,
2020
19
Henrotin, et al.
2019
20
Countr
y
India India Australia India Bel
g
iu
m
Population
Sam
p
le size 120 160 101 140 150
Sex Female and Male
Female and
Male
Female and
Male
Female and
Male
Female and
Male
Mean A
g
e 57 50 58 52 60
Intervention
Name of intervention
1 capsule
(500mg)
curcuma extract
Curcuma
extract
500mg/capsule
with
Diclofenac 50
mg/capsule
1 capsule
(500 mg)
curcumin
extract
1 capsule
(500 mg)
curcuminoid
complex
(BCM-95)
and 1 capsule
(50 mg)
diclofenac
Bio-optimised
Curcuma
longa (BCL)
extract (500
mg/capsule)
Length of
intervention
42 days 4 months 2 months 28 days 3 months
Comparison
1 capsule
(400mg) Placebo
(Microcrystalline
cellulose)
Placebo
500mg/capsule
with
Diclofenac 50
m
g
/ca
p
sule
1 capsule
(500mg)
placebo
1 capsule (50
mg)
Diclofenac
Placebo
Curcuma Extract as an Alternative and Safety Pain Reliever for Geriatric with Knee Osteoarthritis: A Systematic Review and Meta Analysis
73
Outcome
VAS
Control
Before = 6.15 ±
1.37
After = 4.60 ±
2.08
Before = 7.66
± 0.14
After = 5.11 ±
0.14
N/A
Before =
7.81±0.73
After =
5.61±0.61
N/A
Intervention
Before = 6.65 ±
2.1
After = 1.95 ±
1.78
Before = 7.94
± 0.13
After = 4.03 ±
0.08
N/A
Before =
7.90±0.64
After =
3.32±0.60
N/A
p
-value P < 0.05 P < 0.05 N/A P < 0.001 N/A
KOOS
Control N/A N/A
Before =
61.17 ±
13.65
After = 66.69
± 16.66
Before =
51.58 ± 5.49
After =
90.38±3.61
Before = 44.2
± 13.9
After = 55 ±
16.5
Intervention N/A N/A
Before =
60.08 ± 12
After = 72.66
± 16.77
Before =
53.15±4.24
After = 93.03
± 4.75
Before = 45.8
± 15.6
After = 58.6 ±
18.4
p
-value N/A N/A P = 0.009 P < 0.001 P <
0.001
Abbreviation list
VAS, Visual Analog Scale; KOOS, Knee Injury and Osteoarthritis Outcome Score; N/A, not
available
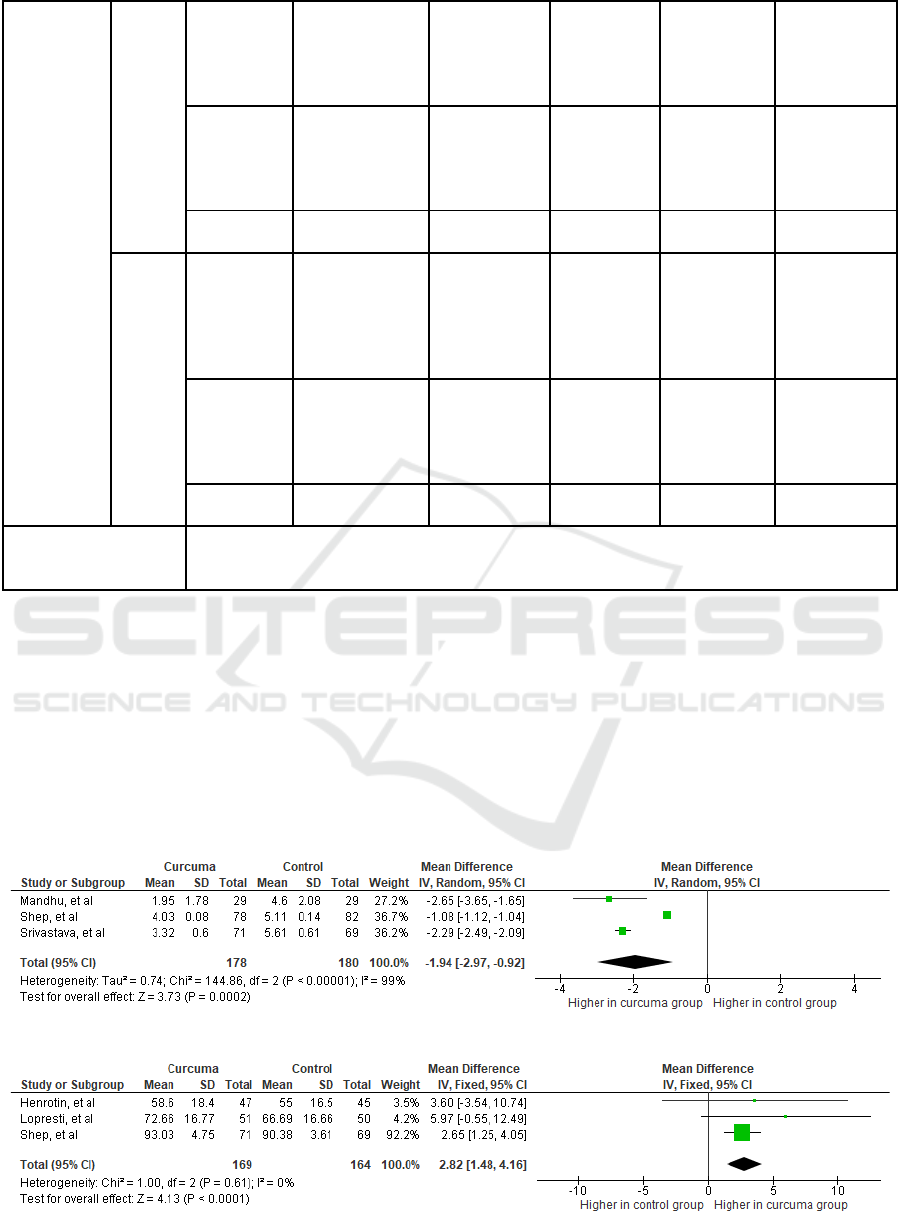
3.4 Meta Analysis
Review Manager (RevMan) v5.4 (Cochrane
Collaboration, UK) was used to conduct the statistical
analysis. In this review, the Mean Difference (MD)
and Standard Deviation (SD) were then computed
with a 95% Confidence Interval (CI). The data was
then processed into pooled standardized mean
difference forest plot form. Our study assessed
extractable quantitative data and grouped them into 2
outcomes which include VAS Score and KOOS
Index. The forest plot of the meta-analysis can be
seen in Figure 3-4.
A total of 5 studies with 671 participants of knee
osteoarthritis patients, dominated by elderly patients
>50 years old. Two included studies have VAS score
outcomes, two included studies have KOOS index
outcomes, and one study has VAS and KOOS
outcomes that are analysed in this review.
Figure 3: VAS Score.
Figure 4: KOOS Index.
ICOMESH 2023 - INTERNATIONAL CONFERENCE ON MEDICAL SCIENCE AND HEALTH
74
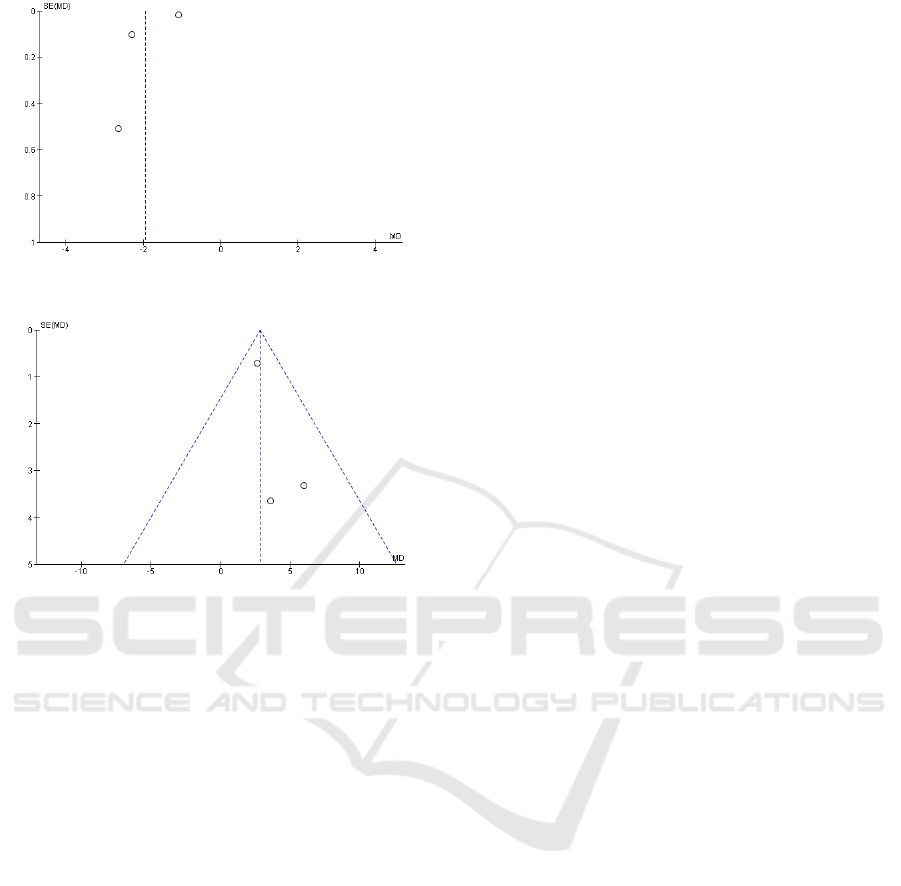
Figure 5: Funnel Plot of VAS Score.
Figure 6: Funnel Plot of KOOS Index.
4 DISCUSSIONS
4.1 Curcuma Extract Improves Knee
Pain on Knee Osteoarthritis
As a result of cartilage damage, osteoarthritis (OA) is
an inflammatory disease that mostly manifests as
joint discomfort and loss of joint function. Damage to
the collagen matrix triggers chondrocyte proliferation
and the production of hypertrophic chondrocyte cell
clusters, which in turn promote the growth of ossified
cartilage and the development of osteophytes
(Stewart & Kawcak, 2018; Dobson et al., 2018; Loef
et al., 2019). Increases in matrix metalloproteinase
(MMP) and inflammatory cytokines like TNF-α and
IL-1β are linked to this damage. Nitric oxide and
reactive oxygen species (ROS) will rise as a result,
leading to an increase in oxidative stress and
worsening symptoms of joint inflammation (Sohn et
al., 2012). Therefore, a treatment that acts as a good
anti-inflammatory and antioxidant is needed to
reduce pain and inflammation in geriatric patients
with OA.
Curcuma extract has been shown to improve knee
pain using VAS score on geriatric patients with knee
osteoarthritis with a significant pooled mean
difference (MD) of -1.94 [95% CI: (-2.97) - (-0.92),
P = 0.0002] with I
2
showing 99%. Heterogenous
results because there are 2 studies from Srivastava et
al. and Shep et al. that use Diclofenac in both groups
can produce biased results. Different formulations for
curcuma extract also can induce bias in the study.
Furthermore, curcuma extract has been shown to
improve knee pain using the KOOS index with a
significant pooled mean difference (MD) of 2.82
[95% CI: 1.48 - 4.16, P<0.0001] with I
2
showing 0%.
The components of curcuma extract include
phenolic pigments (which contain the active
ingredient curcumin, which acts as an anti-
inflammatory agent), essential oils (such as cineole,
linalool, α-terpinene, caryophyllene, ar-curcumene,
zingiberen, curcumol, DL-turmerone, arturmerone,
and dehydrocurdione), cholesterol, fatty acids,
potassium, sodium, magnesium, calcium, manganese,
iron, copper, and zinc, among other elements)
(Karlowicz-Bodalska et al., 2017). The pain
improvement in knee osteoarthritis was facilitated by
the anti-inflammatory of curcuma extract that inhibits
TNF-α, IL-1β, and PGE2. Curcumin, the main
ingredient in curcuma extract, can reduce pain by
inhibiting the production of COX-2 which produces
the pain sensation (Srivastava et al., 2016).
The combination of curcuma and other NSAID
medication can improve better outcomes compared
with NSAID alone. Studies are being conducted to
assess if curcuma extract is more effective as an
adjuvant treatment for OA-related pain than NSAIDs
alone. As seen from the VAS score data before and
after treatment, the intervention group receiving a
combination of curcuma and NSAID has a lower
VAS score after treatment than just giving the NSAID
alone (Shep et al., 2020; Srivastava et al., 2016).
4.2 Safety of Curcuma Extract
In some studies, curcuma extract has fewer adverse
effects, such as dyspepsia, diarrhea, other
gastrointestinal symptoms, and musculoskeletal
symptoms compared to the placebo (Srivastava et al.,
2016; Wang et al., 2020). In some OA cases, 6.6% of
patients treated with curcuma exhibited the least
number of adverse effects during the intervention
period (Madhu et al., 2013). When curcuminoid
complex is added to diclofenac as an adjuvant
treatment, it helps to lessen the GI adverse effects
caused by the drug and lessens the need for H2
blockers (Lopresti et al., 2021).
Curcuma extract as an alternative to NSAIDs in
patients with osteoarthritis which mostly has adverse
Curcuma Extract as an Alternative and Safety Pain Reliever for Geriatric with Knee Osteoarthritis: A Systematic Review and Meta Analysis
75

effects that are mild and transient (Lopresti et al.,
2021). From a pharmacological perspective,
curcumin is a full choleretic-cholagamic agent.
Because they compress the gallbladder, the curcumin
cleavage products (ferulic and hydrofluoric acids)
have cholecystokinin characteristics. On the other
hand, paratholil methyl carbinol, another major
component, has potent choleretic action. The
choleretic action of curcumin causes a 62% rise in
bile output (Shep et al., 2020). Despite the negative
effects of curcumin extract, blood reports for liver,
kidney, and complete blood counts did not
significantly alter before or after the research drugs
were taken (Henrotin et al., 2019).
4.3 Strengths and Limitations
The effectiveness of curcuma extract on elderly
individuals with osteoarthritis in the knee is the
subject of the first systematic review and meta-
analysis conducted on this subject. This systematic
review assessed the curcuma therapy effect that were
consumed orally to reduce osteoarthritis pain in the
elderly age. All studies included are randomized
controlled trials with significant results in pain score
by VAS score and KOOS index.
Nonetheless, this study is not without limitations.
The studies that were included have a high and
moderate risk of bias. The heterogeneity in the
included studies is the different formulations but still
given orally. Also, the use of other medications
combined with curcuma extract, such as NSAID, can
cause bias in the study result. Study duration can be
the limitation of included studies because curcuma
can’t work significantly in a short time duration.
Other factors, such as the severity and type of
osteoarthritis are not discussed in including studies.
There might be a possibility of missing some
important information in studies written in other
languages than English or Indonesian. Irretrievable
full-text is also the limitation of this study. We
suggest conducting more randomized control studies
with a bigger sample size to notice more about the
safety and efficacy of curcuma extract therapy and to
optimize the impact of curcuma extract.
5 CONCLUSIONS
The use of curcuma extract is a potential treatment for
knee osteoarthritis in elderly people, according to this
systematic review and meta-analysis. It has been
shown that curcuma extract is quantitatively
significant in improving knee pain in osteoarthritis
using the VAS score and KOOS index.
CONFLICT OF INTEREST
Every author stated that there are no conflicting
interests in this research.
ACKNOWLEDGMENT
The authors would like to express gratitude for the
lecturers and supervisor of our team, particularly dr.
Ghana Adyaksa, M.Si.Med, Sp.OT and dr. Desy
Armalina, M.Si.Med for the great advices.
REFERENCES
Badan Penelitian dan Pengembangan Kesehatan
Kementerian RI. (2018). Riset Kesehatan Dasar
(Riskesdas) 2018. Kementerian Kesehatan Republik
Indonesia.
Bindu, S., Mazumder, S., & Bandyopadhyay, U. (2020).
Non-steroidal anti-inflammatory drugs (NSAIDs) and
organ damage: A current perspective. Biochemical
Pharmacology, 180, 114147.
Burckhardt, C., & Dupree Jones, K. (2003). Adult measures
of pain: The McGill Pain Questionnaire (MPQ),
Rheumatoid Arthritis Pain Scale (RAPS), Short-Form
McGill Pain Questionnaire (SF-MPQ), Verbal
Descriptive Scale (VDS), Visual Analog Scale (VAS),
and West Haven-Yale Multidisciplinary Pain Inventory
(WHYMPI). Arthritis Care & Research, 49, S96–S104.
Campbell, C. M., Buenaver, L. F., Finan, P., Bounds, S. C.,
Redding, M., McCauley, L., Robinson, M., Edwards, R.
R., & Smith, M. T. (2015). Sleep, Pain Catastrophizing,
and Central Sensitization in Knee Osteoarthritis
Patients With and Without Insomnia. Arthritis Care &
Research, 67(10), 1387–1396.
Dobson, G. P., Letson, H. L., Grant, A., McEwen, P.,
Hazratwala, K., Wilkinson, M., & Morris, J. L. (2018).
Defining the osteoarthritis patient: Back to the future.
Osteoarthritis and Cartilage, 26(8), 1003–1007.
Global Burden of Disease Study 2019 (GBD 2019)
Results, Global Burden of Disease Collaborative
Network (2019)
Heidari-Beni, M., Moravejolahkami, A. R., Gorgian, P.,
Askari, G., Tarrahi, M. J., & Bahreini-Esfahani, N.
(2020). Herbal formulation “turmeric extract, black
pepper, and ginger” versus Naproxen for chronic knee
osteoarthritis: A randomized, double-blind, controlled
clinical trial. Phytotherapy Research: PTR, 34(8),
2067–2073.
Henrotin, Y., Malaise, M., Wittoek, R., de Vlam, K.,
Brasseur, J.-P., Luyten, F. P., Jiangang, Q., Van den
Berghe, M., Uhoda, R., Bentin, J., De Vroey, T.,
ICOMESH 2023 - INTERNATIONAL CONFERENCE ON MEDICAL SCIENCE AND HEALTH
76

Erpicum, L., Donneau, A. F., & Dierckxsens, Y.
(2019). Bio-optimized Curcuma longa extract is
efficient on knee osteoarthritis pain: A double-blind
multicenter randomized placebo controlled three-arm
study. Arthritis Research & Therapy, 21(1), 179.
Karlowicz-Bodalska, K., Han, S., Freier, J., Smolenski, M.,
& Bodalska, A. (2017). CURCUMA LONGA AS
MEDICINAL HERB IN THE TREATMENT OF
DIABET- IC COMPLICATIONS. Acta Poloniae
Pharmaceutica, 74(2), 605–610.
Loef, M., Schoones, J. W., Kloppenburg, M., & Ioan-
Facsinay, A. (2019). Fatty acids and osteoarthritis:
Different types, different effects. Joint Bone Spine,
86(4), 451–458.
Lopresti, A. L., Smith, S. J., Jackson-Michel, S., &
Fairchild, T. (2021). An Investigation into the Effects
of a Curcumin Extract (Curcugen®) on Osteoarthritis
Pain of the Knee: A Randomised, Double-Blind,
Placebo-Controlled Study. Nutrients, 14(1), 41.
Madhu, K., Chanda, K., & Saji, M. J. (2013). Safety and
efficacy of Curcuma longa extract in the treatment of
painful knee osteoarthritis: A randomized placebo-
controlled trial. Inflammopharmacology, 21(2), 129–
136.
Mozaffari-Khosravi, H., Naderi, Z., Dehghan, A.,
Nadjarzadeh, A., & Fallah Huseini, H. (2016). Effect of
Ginger Supplementation on Proinflammatory
Cytokines in Older Patients with Osteoarthritis:
Outcomes of a Randomized Controlled Clinical Trial.
Journal of Nutrition in Gerontology and Geriatrics,
35(3), 209–218.
Perhimpunan Reumatologi Indonesia. (2014).
Rekomendasi IRA untuk Diagnosis dan
Penatalaksanaan Osteoartritis. Divisi Reumatologi
Departemen Ilmu Penyakit Dalam FKUI/RSCM.
Roos, E. M., Roos, H. P., Lohmander, L. S., Ekdahl, C., &
Beynnon, B. D. (1998). Knee Injury and Osteoarthritis
Outcome Score (KOOS)—Development of a self-
administered outcome measure. The Journal of
Orthopaedic and Sports Physical Therapy, 28(2), 88–
96.
Salmon, J. H., Rat, A. C., Sellam, J., Michel, M., Eschard,
J. P., Guillemin, F., Jolly, D., & Fautrel, B. (2016).
Economic impact of lower-limb osteoarthritis
worldwide: A systematic review of cost-of-illness
studies. Osteoarthritis and Cartilage, 24(9), 1500–1508.
Shep, D., Khanwelkar, C., Gade, P., & Karad, S. (2020).
Efficacy and safety of combination of curcuminoid
complex and diclofenac versus diclofenac in knee
osteoarthritis: A randomized trial. Medicine, 99(16)
Singhal, S., Hasan, N., Nirmal, K., Chawla, R., Chawla, S.,
Kalra, B. S., & Dhal, A. (2021). Bioavailable turmeric
extract for knee osteoarthritis: A randomized, non-
inferiority trial versus paracetamol. Trials, 22(1), 105.
Sohn, D. H., Sokolove, J., Sharpe, O., Erhart, J. C.,
Chandra, P. E., Lahey, L. J., Lindstrom, T. M., Hwang,
I., Boyer, K. A., Andriacchi, T. P., & Robinson, W. H.
(2012). Plasma proteins present in osteoarthritic
synovial fluid can stimulate cytokine production via
Toll-like receptor 4. Arthritis Research & Therapy,
14(1), R7. https://doi.org/10.1186/ar3555
Srivastava, S., Saksena, A. K., Khattri, S., Kumar, S., &
Dagur, R. S. (2016). Curcuma longa extract reduces
inflammatory and oxidative stress biomarkers in
osteoarthritis of knee: A four-month, double-blind,
randomized, placebo-controlled trial.
Inflammopharmacology, 24(6), 377–388.
Stewart, H. L., & Kawcak, C. E. (2018). The Importance of
Subchondral Bone in the Pathophysiology of
Osteoarthritis. Frontiers in Veterinary Science, 5, 178.
Vos, T., Allen, C., Arora, M., Barber, R., Bhutta, Z., Brown,
A., Carter, A., Casey, D., Charlson, F., Chen, A.,
Coggeshall, M., Cornaby, L., Dicker, D., Dilegge, T.,
Erskine, H., Ferrari, A., Fitzmaurice, C., Fleming, T., &
Murray, C. (2016). Global, regional, and national
incidence, prevalence, and years lived with disability
for 310 diseases and injuries, 1990–2015: A systematic
analysis for the Global Burden of Disease Study 2015.
The Lancet, 388, 1545–1602.
Wang, Z., Jones, G., Winzenberg, T., Cai, G., Laslett, L. L.,
Aitken, D., Hopper, I., Singh, A., Jones, R., Fripp, J.,
Ding, C., & Antony, B. (2020). Effectiveness of
Curcuma longa Extract for the Treatment of Symptoms
and Effusion-Synovitis of Knee Osteoarthritis: A
Randomized Trial. Annals of Internal Medicine,
173(11), 861–869.
Wojcieszek, A., Kurowska, A., Majda, A., Liszka, H., &
Gądek, A. (2022). The Impact of Chronic Pain,
Stiffness and Difficulties in Performing Daily
Activities on the Quality of Life of Older Patients with
Knee Osteoarthritis. International Journal of
Environmental Research and Public Health, 19(24),
16815.
Wongrakpanich, S., Wongrakpanich, A., Melhado, K., &
Rangaswami, J. (2018). A Comprehensive Review of
Non-Steroidal Anti-Inflammatory Drug Use in The
Elderly. Aging and Disease, 9(1), 143–150.
Curcuma Extract as an Alternative and Safety Pain Reliever for Geriatric with Knee Osteoarthritis: A Systematic Review and Meta Analysis
77
