
A Multi-Modality Approach to Medical Case Retrieval for
Alzheimer's Disease
First Katarina Trojachanec Dineva
a
, Ivan Kitanovski, Ivica Dimitrovski, Suzana Loshkovska
and Alzheimer’s Disease Neuroimaging Initiative
*
Faculty of Computer Science and Engineering, Ss. Cyril and Methodius University,
Rugjer Boshkovik 16, PO Box 393, Skopje, N. Macedonia
Keywords: Alzheimer's Disease, Medical Case Retrieval, Multi-Modal, ADNI, TADPOLE.
Abstract: In this research, we evaluate medical case retrieval for AD on the bases of descriptors generated by combining
different modalities (Magnetic Resonance Imaging (MRI) markers, Fluorodeoxy-glucose Positron Emission
Tomography (FDG-PET) based measures, Cerebrospinal Fluid (CSF) protein levels, and Apolipoprotein-E
(APOE) genotype and age as risk factors). We investigated whether they would provide complementary
information aiming to improve medical case retrieval for AD. According to the obtained results, we concluded
that this approach outperformed the retrieval results in the current reported research by gaining MAP value
of 0.98 yet providing an efficient medical case retrieval for AD and keeping low dimensional feature vector.
1 INTRODUCTION
Alzheimer’s Disease (AD), as an irreversible,
progressive, neurodegenerative disorder, is one of the
most common forms of dementia. It causes neuronal
loss, spreading through different parts of the brain
(Alzheimer's Association, 2022; Porsteinsson, 2021).
A vast amount of data is continuously generated
as part of the medical cases related to AD in the
clinical and research centers, containing variety of
data types. Those include medical imaging markers
such as Magnetic Resonance Imaging (MRI),
Positron Emission Tomography (PET), and Diffusion
Tensor Imaging (DTI), biological markers, namely
Apolipoprotein E (APOE) status, cerebrospinal fluid
(CSF) measures, cognitive tests results etc., carrying
powerful information. The necessity for their efficient
organization, storage, and representation so to be able
to provide appropriate and easier access to the
medical cases, as well as, precise, efficient, and
clinically meaningful retrieval, analysis, knowledge
discovery, prediction and prognosis, is evident and
still, a challenge and an open question (Meyer, 2019).
a
https://orcid.org/0000-0002-7050-4947
* Data used in preparation of this article were obtained
from the Alzheimer’s Disease Neuroimaging Initiative
(ADNI) database (adni.loni.usc.edu). As such, the
investigators within the ADNI contributed to the design
The rapid development in machine learning (ML) is
having a profound impact in biomedical domain,
opening space for applying ML algorithms to provide
a solution to this challenge. This could support and
improve the diagnostic and therapeutic processes.
a
b
The aim of this research is to provide more
efficient and more comprehensive medical case
representation that will enable more precise and
clinically relevant medical case retrieval for AD.
Considering that multi-modality markers may capture
the variety of crucial aspects of the disease and its
progression (Marinescu, 2020; Moguilner, 2022), we
base the medical case representation on multiple
modalities, not the single one, to investigate whether
they can provide a complementary information
contribute to better retrieval results. Hence, we
combined information from MRI imaging markers,
Fluorodeoxyglucose (FDG) - PET based markers,
cognitive tests scores, CSF derived protein levels, as
well as risk factors provided by the Alzheimer's
Disease Neuroimaging Initiative (ADNI, 2022), to
represent each medical case.
and implementation of ADNI and/or provided data but did
not participate in analysis or writing of this report
(http://adni.loni.usc.edu/wp-content/uploads/how_to_apply/
ADNI_Acknowledgement_List.pdf)
554
Dineva, K., Kitanovski, I., Dimitrovski, I., Loshkovska, S. and Alzheimer’s Disease Neuroimaging Initiative, .
A Multi-Modality Approach to Medical Case Retrieval for Alzheimer’s Disease.
DOI: 10.5220/0011939800003414
In Proceedings of the 16th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2023) - Volume 5: HEALTHINF, pages 554-561
ISBN: 978-989-758-631-6; ISSN: 2184-4305
Copyright
c
2023 by SCITEPRESS – Science and Technology Publications, Lda. Under CC license (CC BY-NC-ND 4.0)

The paper is organized as follows. Section 2
provides the related work. The materials and methods
are covered in Section 3. The experimental results and
discussion are presented in Section 4. Section 5
contains the concluding remarks.
2 RELATED WORK
During the past years, AD has been intensively
researched, in an attempt to ensure an early diagnosis,
prognosis, and ultimately finding an appropriate
therapy, including a cure for the disease (Marinescu,
2020b; Weber, 2021; Alzheimer's Association,
2022;). In some research, the traditional approach for
feature extraction from the MRI is used, meaning that
the descriptors are based directly on the visual image
content (Vinutha, 2019; Chethan, 2020; Sagayam,
2021). Other research is using the domain knowledge
to overcome the limitations of the traditional
approach. In this regard, baseline images were used
to estimate of the volumes of the brain structures, and
cortical thickness of the cerebral cortex regions are
calculated in (Trojacanec, 2015; Kruthika, 2019) or to
calculate Spatial Pattern of Abnormality for Early
detection of Alzheimer's Disease (SPARE-AD score)
in (Trojacanec, 2017). On the other hand, longitudinal
approach to estimate static features at multiple time
points is used in (Trojacanec, 2015), and to estimate
dynamic features for patients' descriptors was
proposed in (Trojachanec, 2017). Combination of
static, dynamic features, as well as the SPARE-AD
index (Dineva, 2022) was evaluated for image
retrieval for AD. With the aim to increase the early
detection performance for AD, authors in (Kruthika,
2019) used pre-trained 3D-autoencoder, 3D Capsule
Network, and 3D-Convolutional Neural Network.
Most of the current research is based on a single
modality, mainly MRI features. To induce
improvements in the current research, aiming to
provide more precise and relevant medical case
retrieval for AD, our research is focused on multi-
modal medical case retrieval. For that purpose, we
use multiple biomarkers, usually available as part of
the medical cases for AD acquired during the
examination period in the clinical centres. In fact, this
research aims to evaluate a representation based on a
combination of a variety of biomarkers, extracted
from MRI, FDG-PET, CSF protein levels, and risk
factors, such as APOE genotype and age.
Providing efficient and precise medical case
retrieval for AD might be very beneficial from
different aspects: (1) decision support by providing
clinicians with powerful and relevant information at
the right moment at the right place on the bases of the
existing medical cases of other examined patients; (2)
knowledge discovery from the large, continuously
growing, medical databases by retrieving the most
similar cases; (3) pattern discovery and understanding
of the disease, providing new insights, biomarkers
identification, and analysis of the disease progression;
(4) assessment and analysis of the response to a
possible therapy; (5) providing valuable knowledge
for students, clinicians and scientists.
3 MATERIALS AND METHODS
3.1 Medical Case Retrieval for
Alzheimer's Disease
The medical case retrieval process consists of
generating a representation of the query medical case
and all the medical cases previously stored in the
database using the same representation technique.
After that, the feature vector (descriptor) of the query
medical case is compared to the descriptors of all the
other medical cases. All the medical cases in the
database are then sorted by similarity to the query, so
that the most similar one is at the top. This sorted list
of the database medical cases is the result of the
retrieval. We used leave-one-out strategy because of
the small number of patients used in the evaluation.
To calculate the distance between the medical
case descriptors, we used Manhattan and Canberra
distance (Cha, 2007), chosen on an experimental
basis because they led to the best retrieval results
compared to several other distances such as
Euclidean, Chebyshev, Square Euclidean distance,
Bray-Curtis dissimilarity and Cosine similarity.
To evaluate the proposed strategy in this research,
we used the standard evaluation metric MAP (Mean
Average Precision) for quantitative measurement of
the retrieval performance.
3.2 Medical Case Representation
According to the recent research regarding AD, a
combination of different kinds of biomarkers may
provide complementary and powerful information
(Gupta, 2019; Marinescu, 2020b), possibly enriching
medical case representation. Thus, we combine
different biomarkers suggested by the TADPOLE
challenge (TADPOLE, 2022; Marinescu, 2018)
including MRI ROI derived measures, FDG-PET
based measures, CSF protein levels, APOE status,
and age, to represent the medical cases and we base
the medical case retrieval on multimodal descriptors.
A Multi-Modality Approach to Medical Case Retrieval for Alzheimer’s Disease
555

3.2.1 Magnetic Resonance Imaging
Regarding MRI measurements, we used dynamic and
static measures of the brain structures, as well as
SPARE-AD score, following the strategy used in
(Dineva, 2022) and the fully automated longitudinal
pipeline from the FreeSurfer version 5.3 (FreeSurfer,
2022; Reuter, 2012). According to the previous
research (Trojachanec, 2017), percent change with
respect to the value obtained from the linear fit at
baseline (PCfit) and symmetrized percent change
(SPC) of the volumetric measures of the cortical and
subcortical regions have proven to be most powerful
in longitudinal MRI retrieval for AD. Volumes and
cortical thickness (static) measurements form the
third and fourth time point (12- and 24- month follow-
up), led to the best retrieval precision (Trojacanec,
2015). We also used SPARE-AD score (Davatzikos,
2009; Trojacanec, 2017), available in ADNI database.
In this research, we used a combination of PCfit
or SPC of the volumetric measures (dynamic
features), static volumetric and cortical thickness
measurements at 12- and 24- month follow-ups, and
SPARE-A, because, they provided superior results in
longitudinal retrieval for AD (Dineva, 2022).
3.2.2 Fluoro-Deoxyglucose (FDG) PET
Molecular processes which are thought to be some of
the earliest to become abnormal due to AD
(Marinescu, 2020b), can be represented by PET.
(Jack Jr, 2018). FDG-PET measures of angular,
temporal, and posterior cingulate, are available on
ADNI website and used in this research.
We also use values for two global indices that
were recently added to ADNI: (1) hypometabolic
convergence index (HCI) (Chen, 2011), and (2)
statistical region of interest (sROI) (Chen, 2010; Van
Dyck, 2019). HCI is a cross-sectional measure,
indicating the extent to which the pattern and
magnitude of hypometabolism for a given patient
matches that of patients with AD, while, sROI
AD
was
established longitudinally. representing the standard
uptake value ratio between those regions affected by
the disease and the regions spared by AD.
In contrast, measures of the amyloid-beta load in
the brain (AV45 PET) and tau load in the brain
(AV1451 PET), are not available for most of the
subjects, hence, not used in this research.
3.2.3 Main Cognitive Tests
To be able to measure cognitive decline in patients,
cognitive test is administered by medical expert as
one of the latest indicators of AD, (Jack, 2013).
Regarding the cognitive tests results, as
recommended by the TADPOLE challenge, we used
the following: Clinical Dementia Rating Sum of
Boxes (CDRsb), Alzheimer’s Disease Assessment
Scale (we used both ADAS11, and ADAS13 results),
Mini-Mental State Examination (MMSE), and Rey
Auditory Verbal Learning Test (RAVLT)
(Marinescu, 2020b). Regarding RAVLT test results,
we used the following features: RAVLT immediate,
RAVLT learning, RAVLT forgetting, and RAVLT
forgetting percent. Тhe results of all cognitive tests
are available through the ADNI database.
3.2.4 CSF Biomarkers
Representing the concentration of amyloid-beta and
tau abnormal proteins, not related to any particular
part of the brain, CSF based measurements are
powerful AD indicator, reflecting abnormalities
many years before symptom onset (Marinescu,
2020a; Marinescu, 2020b). CSF biomarkers are
recommended by the TADPOLE challenge to be used
as early AD indicators (Marinescu, 2018), and
therefore we also use them in our research as
amyloid-beta level in CSF (ABETA), tau level
(TAU), and phosphorylated tau level (PTAU).
3.2.5 Risk Factors
APOE ε4 is found to be very powerful genetic risk
factor lowering the age of onset AD (Marinescu,
2018; Gupta, 2019). Considering that the older
subjects are more likely to develop AD, another
important risk factor is the age (Marinescu, 2020b),
and following the recommendations from the
TADPOLE challenge, we used exactly these two.
3.3 Data
In this research, we used the data provided by ADNI,
acquired for the participants from the standardized list
from ADNI-1. The aim of ADNI is to enable research
that will provide an answer to the question whether
combining imaging markers and biological markers,
along with neuro-psychological and clinical
assessments, may indicate the presence and allow
assessment of the progression of MCI and AD.
Following the main goal of ADNI, we are
investigating whether multi-modal markers may lead
to a more precise and efficient medical case retrieval.
We also followed recommendations summarized
for the TADPOLE challenge, in terms of different
data modalities such as: (1) MRI, (2) main cognitive
tests, (3) PET, (4) DTI, (5) CSF biomarkers, and (6)
risk factors and demographic information.
HEALTHINF 2023 - 16th International Conference on Health Informatics
556
We applied several levels of selection to be able
to keep fully complete dataset, thus reducing the
influence of the missing data or the algorithm used to
cope with the missing data on the retrieval results.
Firstly, to provide the possibility of fair
comparison with other research about medical case
retrieval for AD, we selected the subjects that belong
to AD or normal control (NL) group and have
available MRI scans acquired at four time points, at
baseline, and the 6-, 12-, and 24-month follow-ups.
Thus, we obtained a total of 267 patients from the
standardized list, 168 AD, and 99 NL.
After the MRI processing, we selected only the
cases without global or regional failures in all time
points (153 patients in total, 41 AD and 112 NL), to
ensure a complete automatic processing and exclude
the necessity to involve a medical expert.
The cognitive tests results were not available for
three more patients, ending up with 150 patients in
total, 39 AD and 111 NL (subset 1). Significant
number of missing data were detected regarding FDG
PET measures, resulting in 68 patients, 17 AD, 47 NL
(subset 2). CSF biomarkers were available for 85
patients, 24 in AD group, 61 in NL group (subset 3).
3.4 Experimental Setup
To be able to obtain fully complete dataset for the
evaluation, each of the evaluations was conducted
using one of the subsets listed in subsection 3.3. The
goal is to provide a fair comparison between different
medical case representations, not influenced by the
missing data or the algorithm used to overcome the
problem of missing data. Hence, in this research, we
performed three separate evaluations, described in the
following subsections (3.4.1 – 3.4.3). To reduce the
dimension of the descriptor, select the most relevant
features, we also applied Correlation-based Feature
Selection (CFS) algorithm (Hall, 2003), chosen on an
experimental basis. The optimal feature subset was
determined separately in case of each query.
Because most of the current research addressing
the problem of medical case retrieval for AD is based
on MRI (Trojacanec, 2015; Trojachanec, 2017,
Trojacanec 2017; Kruthika, 2019a; Kruthika, 2019b,
Vinutha, 2019; Chethan, 2020), in each evaluation
scenario we used the case in which the descriptor
contains only MRI features for reference.
3.4.1 MRI Measures, Cognitive Scores, and
Risk Factors
The first evaluation was performed on using the
scenarios in Table 1, based on the following features:
MRI (combination of dynamic (VolPCfit or
VolSPC), static measures (Vol34+CT34), and
SPARE-AD)
Cognitive tests (combination of CDRsb,
ADAS11, ADAS13, MMSE, RAVLT
immediate, RAVLT learning, RAVLT
forgetting, and RAVLT forgetting percent)
Risk factors (APOE ε4 and Age)
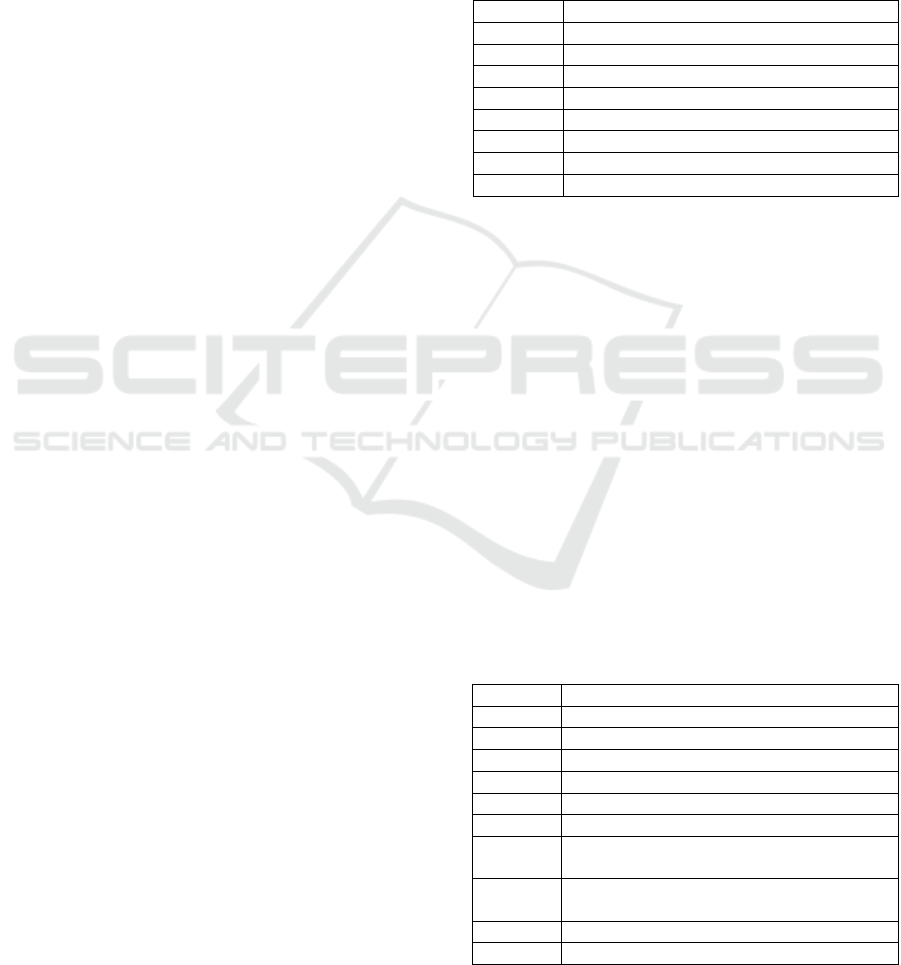
Table 1: Scenarios Based on MRI Measures, Cognitive
Tests and Risk Factors.
Scenario Descri
p
tor
S1.1 MRI_VolPCfit+Vol34+CT34+SPARE-AD
S1.2 MRI_VolSPC+Vol34+CT34+SPARE-AD
S1.3 S1.1+CognitiveT
S1.4 S1.2+Co
g
nitiveT
S1.5 S1.1+RiskF
S1.6 S1.2+RiskF
S1.7 S1.1+Cognitive + RiskF
S1.8 S1.2+Cognitive + RiskF
3.4.2 MRI, FDG PET Measures, Cognitive
Scores, and Risk Factors
The second evaluation was performed on the subset
2, following the scenarios given in Table 2 on the
bases of the following features:
MRI (combination of dynamic (VolPCfit or
VolSPC), static measures (Vol34+CT34), and
SPARE-AD),
Cognitive tests scores (CDRsb, ADAS11,
ADAS13, MMSE, RAVLT immediate,
RAVLT learning, RAVLT forgetting, and
RAVLT forgetting percent), and
Risk factors (APOE ε4 and Age)
FDG PET measurements (FDG PET, HCI,
sROI
AD
, for each of the following visits,
baseline, 6
th
, 12
th
and 24
th
month follow-ups)
Table 2: Scenarios Based on MRI Measures, FDG-PET
measures, Cognitive Tests and Risk Factors.
Scenario Descri
p
tor
S2.1 MRI
_
VolPCfit+Vol34+CT34+SPARE-AD
S2.2 MRI_VolSPC+Vol34+CT34+SPARE-AD
S2.3 S2.1+FDG_PET+HCI+sROI
AD
S2.4 S2.2+FDG_PET+HCI+sROI
AD
S2.5 S2.1+FDG
_
PET+HCI+sROI
AD
+RiskF
S2.6 S2.2+FDG
_
PET+HCI+sROI
AD
+RiskF
S2.7
S2.1+FDG_PET+HCI+sROI
AD
+Co
g
nitiveT
S2.8
S2.2+FDG_PET+HCI+sROI
AD
+CognitiveT
S2.9 S2.3+Cognitive + RiskF
S2.10 S2.4+Co
g
nitive + RiskF
A Multi-Modality Approach to Medical Case Retrieval for Alzheimer’s Disease
557
3.4.3 MRI Measures, Cognitive Scores, Risk
Factors, and CSF Biomarkers
The influence of the CSF biomarkers ABETA, TAU,
and PTAU to the retrieval performance is mainly
evaluated through the evaluation scenarios listed in
Табле 3. The following features are used to generate
the feature vector in these scenarios:
MRI (combination of dynamic (VolPCfit or
VolSPC), static measures (Vol34+CT34), and
SPARE-AD),
Cognitive tests (combination of CDRsb,
ADAS11, ADAS13, MMSE, RAVLT
immediate, RAVLT learning, RAVLT
forgetting, and RAVLT forgetting percent)
Risk factors (APOE ε4, Age)
CSF markers (ABETA, TAU, and PTAU)
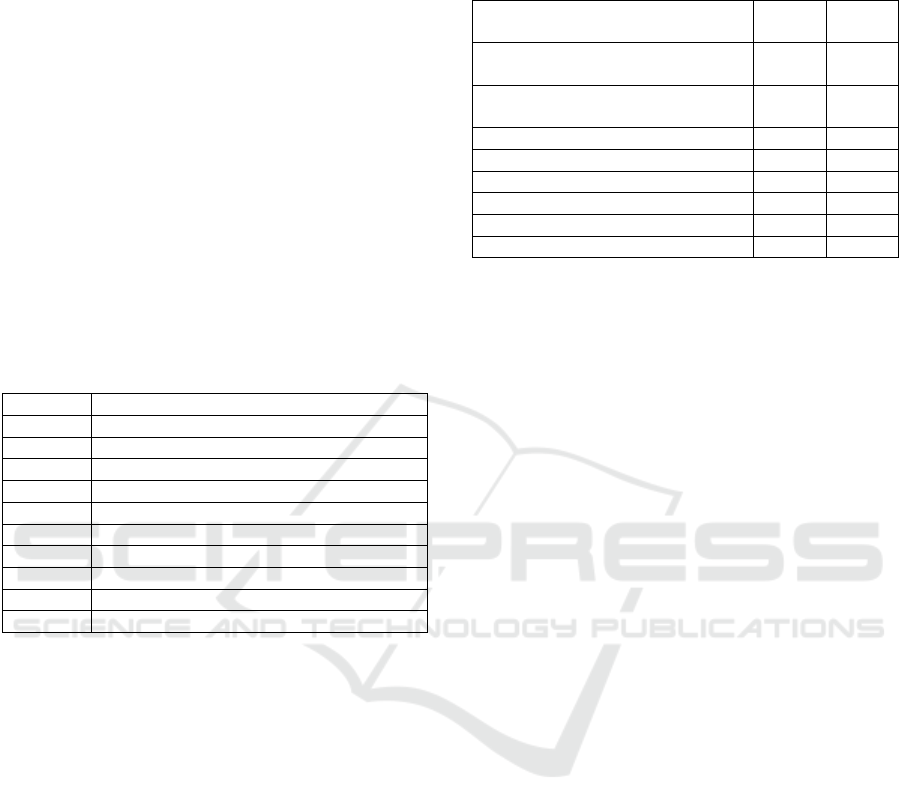
Table 3: Scenarios Based on MRI Measures, FDG-PET
measures, Cognitive Tests and Risk Factors.
Scenario Descriptor
S3.1 MRI_VolPCfit+Vol34+CT34+SPARE-AD
S3.2 MRI
_
VolSPC+Vol34+CT34+SPARE-AD
S3.3 S3.1+RiskF
S3.4 S3.2+RiskF
S3.5 S3.1+CognitiveT
S3.6 S3.2+CognitiveT
S3.7 S3.1+CFS
S3.8 S3.2+CFS
S3.9 S2.3+Co
g
nitiveT+CFS
S3.10 S2.4+CognitiveT+CFS
4 EXPERIMENTAL RESULTS
AND DISCUSSION
In this section, results of the medical case retrieval
evaluated through the three evaluation scenarios
described in subsection 3.4 are provided and
discussed.
4.1 Results Based on MRI, Cognitive
Scores, and Risk Factors
Results of the medical case retrieval based on a
combination of MRI imaging markers, cognitive tests
scores as well as risk factors, are given in Table 4.
This table lists the MAP values for each scenario in
case of two distances for calculation of the similarity
between the query patient's descriptor and all the
patients' descriptors stored in the database, Canberra
and Manhattan. For each subset, we include the
results for MRI based descriptors proposed in
(Dineva, 2022) for reference.
Table 4: Evaluation of the Medical Case Representation
Based on MRI ROI Measures and Cognitive Tests – value
of MAP.
Descriptor
MAP
(MD)
MAP
(CD)
S1.1:MRI_VolPCfit+Vol34+CT34
+SPARE-AD
0.88 0.86
S1.2:MRI_VolSPC+Vol34+CT34+
SPARE-AD
0.88 0.86
S1.3:S1.1+Co
g
nitiveT 0.95 0.97
S1.4:S1.2+Co
g
nitiveT 0.95 0.97
S1.5:S1.1+RiskF 0.87 0.86
S1.6:S1.2+RiskF 0.88 0.86
S1.7:S1.1+Cognitive + RiskF 0.95 0.97
S1.8:S1.2+Co
g
nitive + RiskF 0.95 0.97
Table 4 shows significant improvement of the
value of MAP when cognitive tests are included in the
descriptor (S1.3 i S1.4). The MAP value considering
these scenarios increased to 0.95 in case of Manhattan
distance, while in case of Canberra distance, the MAP
is 0.97, meaning that the inclusion of the cognitive
tests provides great improvement. Despite that
Canberra distance is a weighted version of the
Manhattan distance, we believe that its nature to be
more robust to outliers, but very sensible to values
around 0, which might happen in the case with
cognitive scores values, led to these results.
Additional benefit in the case of the combination
of MRI with the cognitive test scores is that the
dimension of the descriptor is lower than in the case
of MRI-based descriptor. In fact, in S1.3 and S1.4
scenarios, in most of the cases only 28-29 features
were selected, while in S1.1 and S1.2 scenarios, 34-
40 features were selected in most of the cases. From
the cognitive tests taken into consideration in this
research, CDR-SB, ADAS_13, MMSE, RAVLT
(5_sum), RAVLT (perc. forgetting), and FAQ were
selected in almost all cases as most relevant features.
On the other side, the combination of the MRI
imaging markers and risk factors such the Age and
APOE status (S1.5 and S1.6 scenarios), did not
induce any improvement. In only 19 cases the age
was selected to be a part of the descriptor, while the
APOE status was not selected at all.
Similarly, the influence of the risk factors in terms
of improvement of medical case retrieval for AD is
not the case also when all measures were
concatenated (S1.7 and S1.8 scenarios).
4.2 Results Based on MRI, FDG PET,
Cognitive Scores, and Risk Factors
Results of the evaluation for the descriptors S2.1-
S2.10 using the subset 2 are given in Table 5.
HEALTHINF 2023 - 16th International Conference on Health Informatics
558
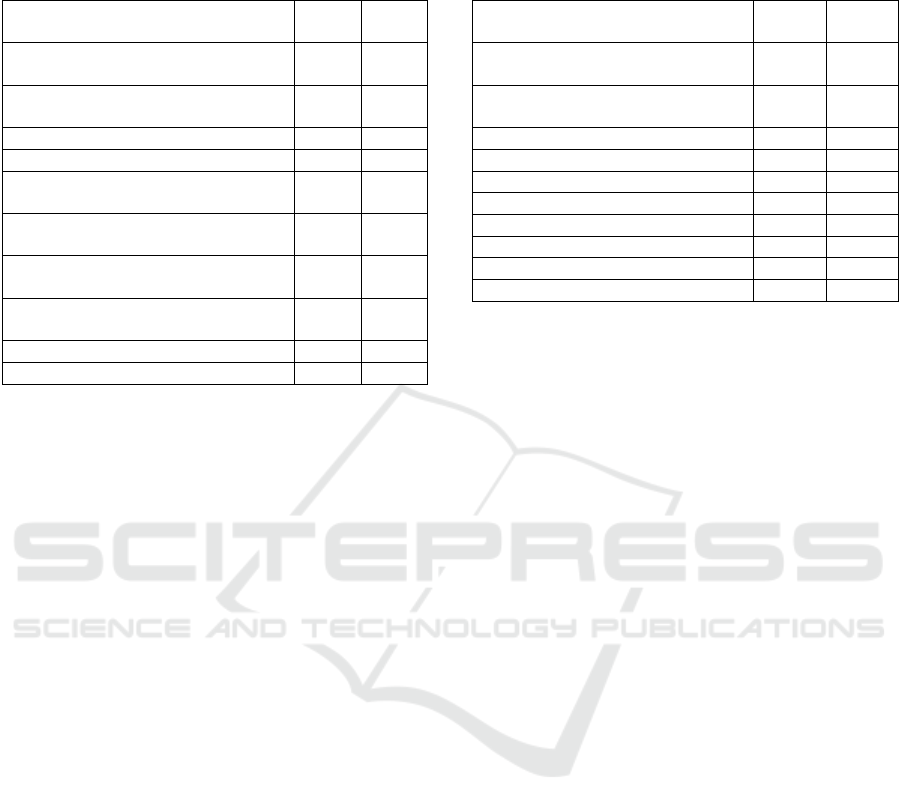
Table 5: Evaluation of the Medical Case Representation
Based on MRI ROI Measures, Cognitive Tests, Risk
Factors, and FDG PET measures – value of MAP.
Descriptor
MAP
(MD)
MAP
(CD)
S2.1:MRI_VolPCfit+Vol34+CT34+
SPARE-AD
0.87 0.84
S2.2:MRI_VolSPC+Vol34+CT34+S
PARE-AD
0.87 0.84
S2.3:S2.1+FDG
_
PET+HCI+sROI
AD
0.88 0.84
S2.4:S2.2+FDG
_
PET+HCI+sROI
AD
0.88 0.84
S2.5:S2.1+FDG_PET+HCI+sROI
AD
+RiskF
0.89 0.82
S2.6:S2.2+FDG_PET+HCI+sROI
AD
+RiskF
0.89 0.82
S2.7:S2.1+FDG_PET+HCI+sROI
A
D
+Co
g
nitiveT
0.98 0.98
S2.8:S2.2+FDG_PET+HCI+sROI
A
D
+Co
g
nitiveT
0.98 0.98
S2.9:S2.3+Co
g
nitive + RiskF 0.98 0.98
S2.10:S2.4+Co
g
nitive + RiskF 0.98 0.98
According to the results, we came to the conclusion
that FDG-PET based measures provide a slight
increase of the MAP value (gaining a value of 0.88)
when Manhattan distance is used to calculate the
similarity. It should be emphasized that in this case,
from the used FDG-PET measures, HCI at 6- and 24-
month follow-up, as well as sROI
AD
at 12- and 24-
month follow-ups were selected, and the descriptor
was long 36 features in most of the cases.
Moreover, the inclusion of the risk factors APOE
and age also led to an improvement when evaluation
was performed on the subset 2 with Manhattan
distance, by selecting the age as a relevant feature, but
not the APOE. The dimension of the feature vector in
most of the cases was 21 features.
Similarly like in the case of the evaluation based
on the subset 1, the cognitive tests scores provided
significant improvement of the retrieval precision in
the case on both similarity measures. But the
combination of all the features considered in this
evaluation, did not contribute to additional
improvement. In most of the cases, 23 features were
selected.
4.3 Results Based on MRI, Cognitive
Scores, Risk Factors, and CSF
Table 6 contains the results of the performed
evaluation for the descriptors S3.1-S3.10. Their
influence on the retrieval results is evaluated using
the subset 3. It is selected so that contains fully
competed data for all of the measures evaluated in this
scenario (MRI, cognitive tests, risk factors, and CSF
biomarkers: ABETA, TAU, and PTAU)
Table 6: Evaluation of the Medical Case Representation
Based on MRI ROI Measures, Cognitive Tests, Risk
Factors, and CSF biomarkers – value of MAP.
Descriptor
MAP
(MD)
MAP
(CD)
S3.1:MRI_VolPCfit+Vol34+CT34
+SPARE-AD
0.86 0.87
S3.2:MRI_VolSPC+Vol34+CT34+
SPARE-AD
0.86 0.87
S3.3:S3.1+RiskF 0.86 0.87
S3.4:S3.2+RiskF 0.86 0.87
S3.5:S3.1+Co
g
nitiveT 0.96 0.98
S3.6:S3.2+CognitiveT 0.96 0.98
S3.7:S3.1+CFS 0.86 0.88
S3.8:S3.2+CFS 0.86 0.88
S3.9:S2.3+Co
g
nitiveT+CFS 0.96 0.98
S3.10:S2.4+Co
g
nitiveT+CFS 0.96 0.98
The results showed that CFS biomarkers led to a
slight improvement of the medical case retrieval
precision. In almost all of the cases, ABETA level
was selected automatically by the algorithm, and
TAU and PTAU values were selected in fewer cases.
In most of the cases, the dimension of the descriptor
was 20 features.
Following the trend of the evaluation results
obtained on the subset 1 and 2, the combination with
the cognitive tests scores provided the best MAP.
4.4 Discussion
Instead of focusing on one modality, i.e. one type of
data, usually MRI, this research takes into
consideration multi-modal medical case
representation appropriate to AD, and evaluates the
medical case retrieval in terms of different
information contained in the medical case descriptor.
Following the TADPOLE recommendations, and the
considering that the reported research about medical
case retrieval for AD (mostly focused on information
extracted from the MRI images, cross-sectionally or
longitudinally) (Trojacanec, 2015; Trojachanec,
2017, Trojacanec 2017; Kruthika, 2019a; Kruthika,
2019b, Vinutha, 2019; Chethan, 2020; Dineva, 2022)
and less on other modalities (Gupta, 2019), we
performed a wide evaluation on different kinds of
medical case representations.
We performed the evaluation using fully complete
datasets, to be able to provide fair evaluation not
influenced by the missing data or the strategy used to
cope with the missing data. But, on the other hand,
trying to provide fully compete datasets, we ended up
with small subsets for some of the evaluation
scenarios and unbalanced classes (subset 2 and 3). In
this regards, FDG-PET measures were available for a
A Multi-Modality Approach to Medical Case Retrieval for Alzheimer’s Disease
559

very small number of patients (64), while CSF
measures for only 85 patients from ADNI 1.
According to the obtained results, with this
research we got significant improvement over the
current results in the reported research (Trojacanec,
2015; Trojachanec, 2017, Trojacanec 2017; Kruthika,
2019a; Kruthika, 2019b, Vinutha, 2019; Chethan,
2020, Gupta, 2019. In fact, cognitive tests scores
significantly increased the MAP in all three
evaluation subsets, leading to MAP value of 0.98.
Among the cognitive scores, CDR-SB, ADAS_13,
MMSE, RAVLT (5_sum), RAVLT (perc.
Forgetting), and FAQ were most frequently selected
features. Additionally, the FDG–PET based measures
(among which HCI at 6- and 24- month, and sROI
AD
at 12- and 24- month follow-ups were automatically
selected in most of the cases) and the age as a risk
factor, provided a slightly better performance or no
improvement at all. Regarding the CSF, the most
frequently selected feature was ABETA level, but did
not significantly improved the retrieval results.
It should be emphasized that the features (of a
given modality) selected in most of the cases for a
given scenario, were similarly selected through all the
evaluations for which they were available. Despite
the fact that most of them are significant markers for
AD, this frequent automatic selection makes them
stable and appropriate to be used to represent medical
cases for AD.
The strategy for medical case representation used
in this research reflects the current condition of the
brain / atrophy, the degree of degeneration and the
progression of the disease, the nerve cells damage and
the brain metabolism, covering all the stages of the
disease in the medical case retrieval for AD, using the
entire cascade of disease indicators. Moreover, it can
be easily adopted for addressing specific aspects of
other neurological disease. Additionally, considering
the low number of features in the descriptor and high
precision at the same time, this strategy can be easily
adopted and integrated as an efficient and clinically
relevant decision support in the standard practice and
to assist medical experts. However, the challenging
part that needs to be addressed and involved in the
clinical workflow is rapid information processing
regarding different modalities for the a patient
currently examined (all other medical cases may be
processed off-line and stored in the database).
5 CONCLUSIONS
This research investigated the medical case retrieval
for AD based on different modalities of data. For this
purpose, we made a research in order to find a
relevant and efficient representation of the medical
case that will provide precise, efficient and clinically
relevant retrieval. Particularly, we focus our research
on multi-modal patient representation including the
following kinds of data: structural MRI, FDG-PET
based measures, CSF protein levels, and APOE
genotype and age as risk factors.
According to the performed evaluation, we
outperformed the results gained by the other research
on medical case retrieval for AD, which is mostly
based on single modality. We also provided a good
basis for further investigation and analysis in this
domain, by using a comprehensive approach. In the
future, we are going to extend the research to a wider
dataset, including more subjects and more phases of
the disease (early-MCI, late-MCI, …). We are also
are going to investigate deep learning methods in
terms of feature engineering.
ACKNOWLEDGEMENT
Data collection and sharing for the research in this
paper was funded by the Alzheimer's Disease
Neuroimaging Initiative (ADNI) (National Institutes
of Health Grant U01 AG024904) and DOD ADNI
(Department of Defense award number W81XWH-
12-2-0012).
REFERENCES
Alzheimer's Association, 2022. 2022 Alzheimer's disease
facts and figures. [https://www.alz.org/media/docu
ments/alzheimers-facts-and-figures.pdf] Аccessed:
30.10.2022.
Alzheimer's Disease Neuroimaging Initiative: ADNI, 2017.
[https://adni.loni.usc.edu/] Accessed: 5.11.2022.
Cha, S. H. (2007). Comprehensive survey on
distance/similarity measures between probability
density functions. City, 1(2), 1.
Chen, K., Langbaum, J. B., Fleisher, A. S., Ayutyanont, N.,
Reschke, C., Lee, W., ... & Alzheimer's Disease
Neuroimaging Initiative. (2010). Twelve-month
metabolic declines in probable Alzheimer's disease and
amnestic mild cognitive impairment assessed using an
empirically pre-defined statistical region-of-interest:
findings from the Alzheimer's Disease Neuroimaging
Initiative. Neuroimage, 51(2), 654-664.
Chen, K., Ayutyanont, N., Langbaum, J. B., Fleisher, A. S.,
Reschke, C., Lee, W., ... & Reiman, E. M. (2011).
Characterizing Alzheimer's disease using a
hypometabolic convergence index. Neuroimage, 56(1),
52-60.
HEALTHINF 2023 - 16th International Conference on Health Informatics
560

Chethan, K., & Bhandarkar, R. (2020). Hybrid Feature
Extraction Technique on Brain MRI Images for
Content-Based Image Retrieval of Alzheimer’s
Disease. In Advances in Communication, Signal
Processing, VLSI, and Embedded Systems (pp. 127-
141). Springer, Singapore.
Davatzikos, C., Xu, F., An, Y., Fan, Y. and Resnick, S.M
(2009). Longitudinal progression of Alzheimer's-like
patterns of atrophy in normal older adults: the SPARE-
AD index. Brain, 132(8), 2026-2035.
Dineva, K. T., Kitanovski, I., Dimitrovski, I., &
Loshkovska, S. (2022). Combining Static and Dynamic
Features to Improve Longitudinal Image Retrieval for
Alzheimer’s Disease. In International Conference on
ICT Innovations (pp. 107-120). Springer, Cham.
FreeSurfer. [https://surfer.nmr.mgh.harvard.edu/].
Accessed: 21.10.2022.
Gupta, Y., Lama, R. K., Kwon, G. R., & Alzheimer's
Disease Neuroimaging Initiative. (2019). Prediction
and classification of Alzheimer’s disease based on
combined features from apolipoprotein-E genotype,
cerebrospinal fluid, MR, and FDG-PET imaging
biomarkers. Frontiers in computational neuroscience,
13, 72.
Hall, M. A., & Holmes, G. (2003). Benchmarking attribute
selection techniques for discrete class data mining.
IEEE Transactions on Knowledge and Data
engineering, 15(6), 1437-1447.
Jack Jr, C. R., Bennett, D. A., Blennow, K., Carrillo, M. C.,
Dunn, B., Haeberlein, S. B., ... & Silverberg, N. (2018).
NIA-AA research framework: toward a biological
definition of Alzheimer's disease. Alzheimer's &
Dementia, 14(4), 535-562.
Kruthika, K. R., Maheshappa, H. D., & Alzheimer's Disease
Neuroimaging Initiative. (2019a). Multistage classifier-
based approach for Alzheimer's disease prediction and
retrieval. Informatics in Medicine Unlocked, 14, 34-42.
Kruthika, K. R., Maheshappa, H. D., & Alzheimer's Disease
Neuroimaging Initiative. (2019b). CBIR system using
Capsule Networks and 3D CNN for Alzheimer's disease
diagnosis. Informatics in Medicine Unlocked,14,59-68.
Marinescu, R. V., Oxtoby, N. P., Young, A. L., Bron, E. E.,
Toga, A. W., Weiner, M. W., ... & Alexander, D. C.
(2018). Tadpole challenge: Prediction of longitudinal
evolution in Alzheimer's disease. arXiv preprint
arXiv:1805.03909.
Marinescu, R. V., Oxtoby, N. P., Young, A. L., Bron, E. E.,
Toga, A. W., Weiner, M. W., ... & Alexander, D. C.
(2020a). The alzheimer's disease prediction of
longitudinal evolution (TADPOLE) challenge: Results
after 1 year follow-up. arXiv preprint
arXiv:2002.03419.
Marinescu, R. V. (2020b). Modelling the Neuroanatomical
Progression of Alzheimer's Disease and Posterior
Cortical Atrophy. arXiv preprint arXiv:2003.04805.
Meyer, P.F., Tremblay-Mercier, J., Leoutsakos, J., Madjar,
C., Lafaille-Maignan, M.É., Savard, M., Rosa-Neto, P.,
Poirier, J., Etienne, P., Breitner, J. and PREVENT-AD
research group (2019). INTREPAD: A randomized trial
of naproxen to slow progress of presymptomatic
Alzheimer disease. Neurology, 92(18), e2070-e2080.
Moguilner, S., Birba, A., Fittipaldi, S., Gonzalez-Campo,
C., Tagliazucchi, E., Reyes, P., ... & Ibáñez, A. (2022).
Multi-feature computational framework for combined
signatures of dementia in underrepresented settings.
Journal of Neural Engineering, 19(4), 046048.
Porsteinsson, A.P., Isaacson, R.S., Knox, S., Sabbagh,
M.N. and Rubino, I. (2021) Diagnosis of early
alzheimer’s disease: Clinical practice in 2021. The
Journal of Prevention of Alzheimer's Disease, 8(3),
371-386.
Reuter, M., Schmansky, N.J., Rosas, H.D. and Fischl, B
(2012). Within-subject template estimation for
unbiased longitudinal image analysis. Neuroimage,
61(4), 1402-1418.
The Alzheimer's Disease Prediction Of Longitudinal
Evolution (TADPOLE) Challenge
[https://tadpole.grand-challenge.org/] Accessed:
20.11.2022.
Trojacanec, K., Kitanovski, I., Dimitrovski, I. and
Loshkovska, S. October. Medical image retrieval for
Alzheimer’s disease using data from multiple time
points. In International Conference on ICT Innovations,
pp. 215-224. Springer, Cham (2015).
Trojacanec, K., Kalajdziski, S., Kitanovski, I., Dimitrovski,
I., Loshkovska, S. and Alzheimer’s Disease
Neuroimaging Initiative. Image Retrieval for
Alzheimer’s Disease Based on Brain Atrophy Pattern.
In International Conference on ICT Innovations, pp.
165-175. Springer, Cham (2017).
Trojachanec, K., Kitanovski, I., Dimitrovski, I. and
Loshkovska, S. Longitudinal brain MRI retrieval for
Alzheimer's disease using different temporal
information. IEEE Access, 6, 9703-9712 (2017).
Van Dyck, C. H., Nygaard, H. B., Chen, K., Donohue, M.
C., Raman, R., Rissman, R. A., ... & Strittmatter, S. M.
(2019). Effect of AZD0530 on cerebral metabolic
decline in Alzheimer disease: a randomized clinical
trial. JAMA neurology, 76(10), 1219-1229.
Vinutha, N., Sandeep, S., Kulkarni, A. N., Shenoy, P. D., &
Venugopal, K. R. (2019, March). A Texture based
Image Retrieval for Different Stages of Alzheimer’s
Disease. In 2019 IEEE 5th International Conference for
Convergence in Technology (I2CT) (pp. 1-5). IEEE.
Weber, C. J., Carrillo, M. C., Jagust, W., Jack Jr, C. R.,
Shaw, L. M., Trojanowski, J. Q., ... & Weiner, M. W.
(2021). The Worldwide Alzheimer's Disease
Neuroimaging Initiative: ADNI‐3 updates and global
perspectives. Alzheimer's & Dementia: Translational
Research & Clinical Interventions, 7(1), e12226.
Jack Jr, C. R., Knopman, D. S., Jagust, W. J., Petersen, R.
C., Weiner, M. W., Aisen, P. S., ... & Trojanowski, J.
Q. (2013). Update on hypothetical model of
Alzheimer’s disease biomarkers. Lancet neurology,
12(2), 207.
A Multi-Modality Approach to Medical Case Retrieval for Alzheimer’s Disease
561
