
Novel View Synthesis for Unseen Surgery Recordings
Mana Masuda
1 a
, Hideo Saito
1 b
, Yoshifumi Takatsume
3
and Hiroki Kajita
2
1
Department of Information and Computer Science, Keio University, Yokohama, Japan
2
Department of Plastic and Reconstructive Surgery, Keio University School of Medicine, Shinjuku-ku, Tokyo, Japan
3
Department of Anatomy, Keio University School of Medicine, Shinjuku-ku, Tokyo, Japan
Keywords:
Medical Image Application, Novel View Synthesis.
Abstract:
Recording surgery in operating rooms is a crucial task for both medical education and evaluation of medical
treatment. In this paper, we propose a method for visualizing surgical areas that are occluded by the heads or
hands of medical professionals in various surgical scenes. To recover the occluded surgical areas, we utilize
a surgery recording system equipped with multiple cameras embedded in the surgical lamp, with the aim of
ensuring that at least one camera can capture the surgical area without occlusion. We propose the application of
a transformer-based Neural Radiance Field (NeRF) model, originally proposed for normal scenes, to surgery
scenes, and demonstrate through experimentation that it is feasible to generate occluded surgical areas. We
believe this research has the potential to make our multi-camera recording system practical and useful for
physicians.
1 INTRODUCTION
The recording of surgeries in an operating room with
cameras has proven to be an indispensable task for a
variety of purposes, including education, the sharing
of surgical technologies and techniques, the perfor-
mance of case studies of diseases, and the evaluation
of medical treatment (Masuda et al., 2022; Hachiuma
et al., 2020; Matsumoto et al., 2013; Sadri et al., 2013;
Shimizu et al., 2020). The targets that depict the
surgery, such as the surgical field, surgeon’s hands,
and surgical tools, should be captured in the record-
ings of surgeries for these purposes.
It is challenging, however, to continuously record
these targets without any occlusion. The most
straightforward method for recording surgery is to at-
tach a camera to the operating room environment, but
this may result in occlusion of the surgical field by
surgeons, nurses, or surgical machinery. Another op-
tion is to attach the camera to the head of the sur-
geon and record from a first-person perspective, but
this video is often affected by motion blur due to head
movements and the surgeon may not always be look-
ing at the surgical field. Additionally, the camera at-
tached to the surgeon’s head may interfere with the
surgery itself. As a result, cameras attached to the op-
a
https://orcid.org/0000–0002–9050–5306
b
https://orcid.org/0000–0002–2421–9862
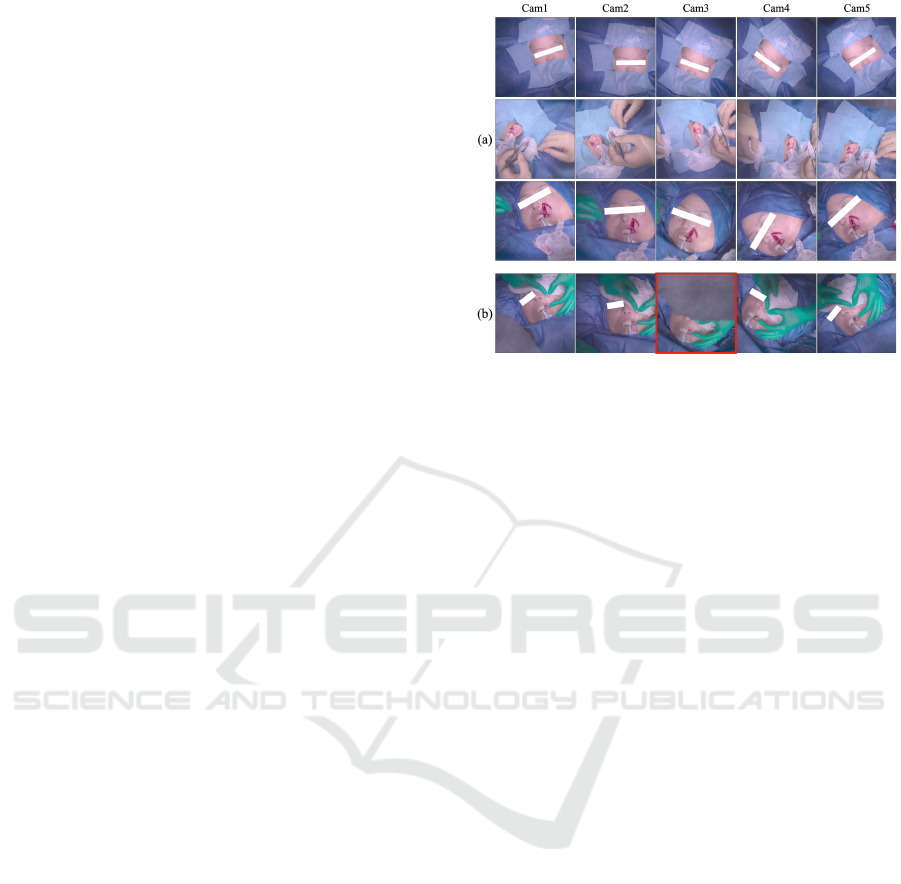
Figure 1: We expect that at least one of the cameras attached
to the surgical lamp will capture the surgical field (Cam1, 3,
4, 5), but not all of the cameras will for most of the cases
(Cam2).
erating room environment or the surgeon’s head are
not effective solutions for recording surgeries.
Shimizu et al. (Shimizu et al., 2020) proposed a
novel surgical lamp system with multiple embedded
cameras to record surgeries. A generic surgical lamp,
commonly used in open surgeries, has multiple light
bulbs that illuminate the surgical field from multiple
directions in order to reduce shadows caused by sur-
geons. Shimizu et al. expect that at least one of the
multiple light blubs will almost always illuminate the
surgical field. They embedded the cameras into each
944
Masuda, M., Saito, H., Takatsume, Y. and Kajita, H.
Novel View Synthesis for Unseen Surgery Recordings.
DOI: 10.5220/0011897200003417
In Proceedings of the 18th International Joint Conference on Computer Vision, Imaging and Computer Graphics Theory and Applications (VISIGRAPP 2023) - Volume 4: VISAPP, pages
944-949
ISBN: 978-989-758-634-7; ISSN: 2184-4321
Copyright
c
2023 by SCITEPRESS – Science and Technology Publications, Lda. Under CC license (CC BY-NC-ND 4.0)
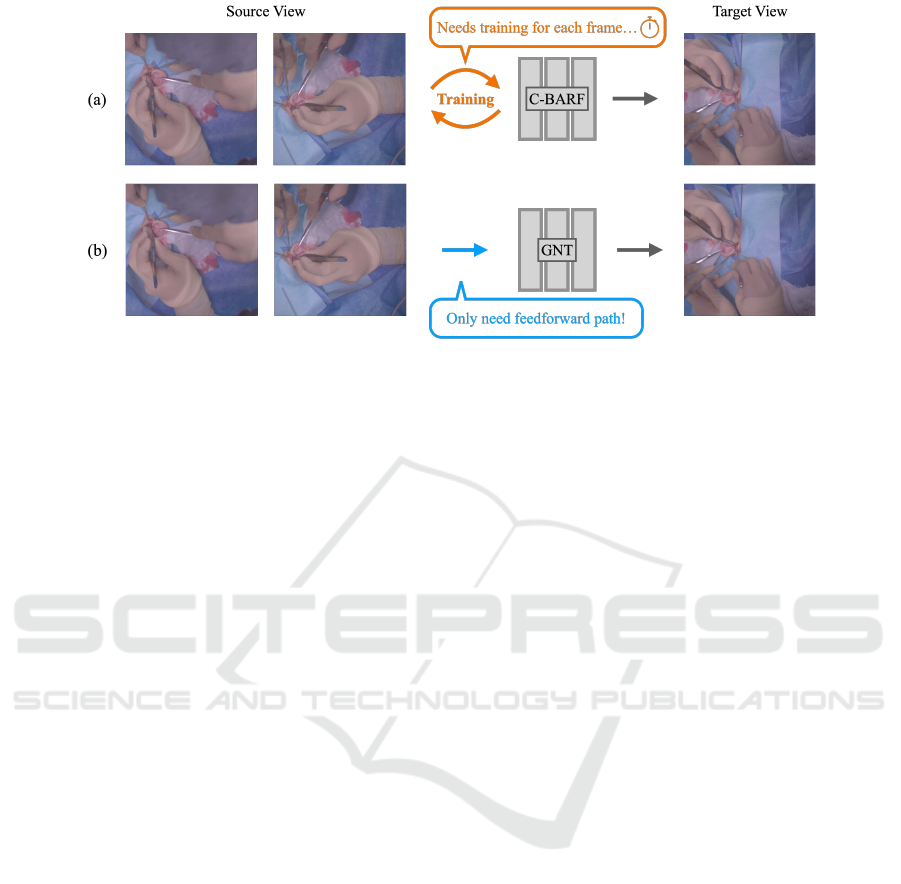
Figure 2: (a) Conditional-BARF (C-BARF) (Masuda et al., 2022) requires training the network for each frame, which takes a
tremendous amount of time to create a video from the beginning to the end of the surgery. (b) We propose using Generalizable
NeRF Transformer (GNT) (Wang et al., 2022) for surgery scenes. This method does not require training even when rendering
unseen scenes, so it is possible to create the video in significantly less time than C-BARF.
light blub, ensuring that there is always one camera
that captures the surgical field as long as the surgical
field is illuminated.
As not all cameras are capable of adequately
capturing the surgical field, as depicted in Fig. 1,
post-processing is often required to create reviewable
videos from multi-view video. Various methods have
been proposed for this post-processing (Masuda et al.,
2022; Hachiuma et al., 2020; Shimizu et al., 2020).
Shimizu et al. (Shimizu et al., 2020) and Hachiuma
et al. (Hachiuma et al., 2020) have proposed mod-
els to select the best view frames, while Masuda et
al. (Masuda et al., 2022) have proposed the use of
Conditional-BARF (C-BARF; see Fig.2-(a)) to syn-
thesize occlusion-free image, with the aim of gen-
erating videos with smooth camera pose transitions.
The C-BARF utilizes the relative position of the cam-
era as a condition for improved camera pose estima-
tion, as COLMAP (Sch
¨
onberger and Frahm, 2016) is
unable to accurately determine camera position from
only five images. However, this approach requires
the training of a network for every frame in order to
generate novel view images, leading to a significant
computational time when creating a video of an en-
tire surgery. Additionally, it may struggle to render
images if the target camera pose is not closely aligned
with the source view’s camera pose.
Recently, transformer-based Neural Radiance
Field (NeRF) has been attracting much attention.
Wang et al. proposed IBRNet (Wang et al., 2021),
which introduces the Ray Transformer, enabling the
learning of a generic vire interpolation that general-
izes to novel scenes. Varma et al. proposed the Gen-
eralizable NeRF Transformer (GNT) (Wang et al.,
2022), which introduced the View Transformer as the
first stage. This transformer-based architecture allows
for the generation of unseen scenes from source-view
images.
In this paper, we propose the use of GNT for syn-
thesizing surgical scenes (Fig. 2-(b)) with the aim
of synthesizing novel view images of new surgical
scenes without training the network using the GNT’s
features, which can be pre-trained using previous sur-
gical scenes. Our experimental results demonstrate
that GNT can generalize surgical scenes using real-
world surgical data, even though surgical data is typ-
ically less numerous than everyday scenes and in-
cludes complex shapes (e.g., faces, legs, surgeon’s
hands, and surgical instruments). We record all data at
Keio University School of Medicine using the record-
ing system proposed by Shimizu et al. (Shimizu et al.,
2020).
2 RELATED WORK
2.1 Surgical Recording Systems
Recording surgeries and generating videos for re-
viewing surgeries or teaching skills to future gener-
ations is an important task for doctors. Surgeries
performed through an endoscope camera, such as la-
paroscopic surgery, can be easily recorded. However,
surgeries in which the surgeon directly visualizes the
surgical field, such as open surgery, are difficult to
record due to spatial restrictions, as the head or hands
of the surgeons and medical equipment may occluded
the important field of the surgery.
Many attempts have been made to record the sur-
gical field (Shimizu et al., 2020; Matsumoto et al.,
Novel View Synthesis for Unseen Surgery Recordings
945
2013; Murala et al., 2010; Kumar and Pal, 2004; Byrd
et al., 2003). Kumar et al. (Kumar and Pal, 2004)
and Byrd et al. (Byrd et al., 2003) proposed recording
systems that place a camera in the surgery room envi-
ronment. However, the view is easily occluded by the
surgeon’s head or body. Observing the surgical field
with a single camera without any occlusion is a diffi-
cult task. Matsumoto et al. and Murala et al. proposed
recording systems that ask surgeons to wear cameras.
However, this system is not only limited by hardware
in its ability to produce high-quality videos, but it is
also uncomfortable for surgeons to wear.
To solve this problem, Shimizu et al. proposed a
new system that embeds cameras on a surgical lamp.
This system not only allows one of the cameras to
record the surgical field while one of the light bulbs
illuminates it but also does not interfere with the sur-
geons during surgeries.
2.2 Camera Switching System
As the cameras obtain multiple videos of a single
surgery, Shimizu et al. proposed a method for au-
tomatically selecting the image with the best view
of the surgical field at each moment using Dijkstra’s
algorithm based on the size of the surgical field to
generate a single video. Hachiuma et al. (Hachiuma
et al., 2020) proposed Deep Selection, which selects
the camera with the best view of the surgery using
a fully supervised deep neural network. However, a
problem with these methods is that the video quality
is often low due to frequent changes in the viewing
direction.
2.3 Novel View Synthesis
Novel view synthesis is one of the fundamental func-
tionality and long-standing problem in computer vi-
sion (Gortler et al., 1996; Levoy and Hanrahan, 1996;
Davis et al., 2012).
For Non-medical Images: Recently, novel view
synthesis methods for everyday scenes have made sig-
nificant progress by using neural networks. Milden-
hall et al. (Mildenhall et al., 2020) proposed NeRF, a
method for synthesizing novel views of static, com-
plex scenes from a set of input images with known
camera poses. Wang et al. proposed IBRNet (Wang
et al., 2021), which introduced the Ray Transformer.
This method enables learning a generic view interpo-
lation function that generalizes to novel scenes, unlike
previous neural scene representation work that opti-
mized per-scene functions for rendering. Varma T.et
al. proposed the Generalizable NeRF Transformer
(GNT) (Wang et al., 2022), which introduced the
Figure 3: Examples of the data captured by the recording
system proposed by Shimizu et al. (Shimizu et al., 2020).
(a) The examples we used for the training, in which no cam-
eras were obstructed by the surgeon’s head. (b) A bad exam-
ple in which the surgical area was hidden by the surgeon’s
head (Cam3).
View Transformer as the first stage. They also demon-
strated that depth and occlusion could be inferred
from the learned attention maps, which implies that
the pure attention mechanism is capable of learning a
physically-grounded rendering process. Furthermore,
this transformer-based architecture makes it possible
to generate unseen scenes from source-view images.
For Medical Images: The novel view synthesis
method is begging to be used for medical scenes. Ma-
suda et al. (Masuda et al., 2022) proposed C-BARF,
which can synthesize novel view images of surgical
scenes. They used the relative position of the camera
to more accurately estimate the camera poses. They
achieved a novel view synthesis method for surgical
videos that consists of a small number of images.
3 METHOD
Our objective is to generate the surgical areas oc-
cluded by the surgeons’ or nurse’s head in order to
create a comprehensive video for reviewing the surgi-
cal procedure. Our methodology can be divided into
five distinct steps.
The first step is to prepare some sets of multi-
view training videos using the camera recording sys-
tem proposed by Shimizu et al.(Shimizu et al., 2020).
In order to train GNT with a diversity of surgeries and
surgical procedures, we recorded the surgeries with
multiple types and for various areas. Presently, there
are numerous frames with occlusions as dipicted in
Fig. 3-(b).
VISAPP 2023 - 18th International Conference on Computer Vision Theory and Applications
946
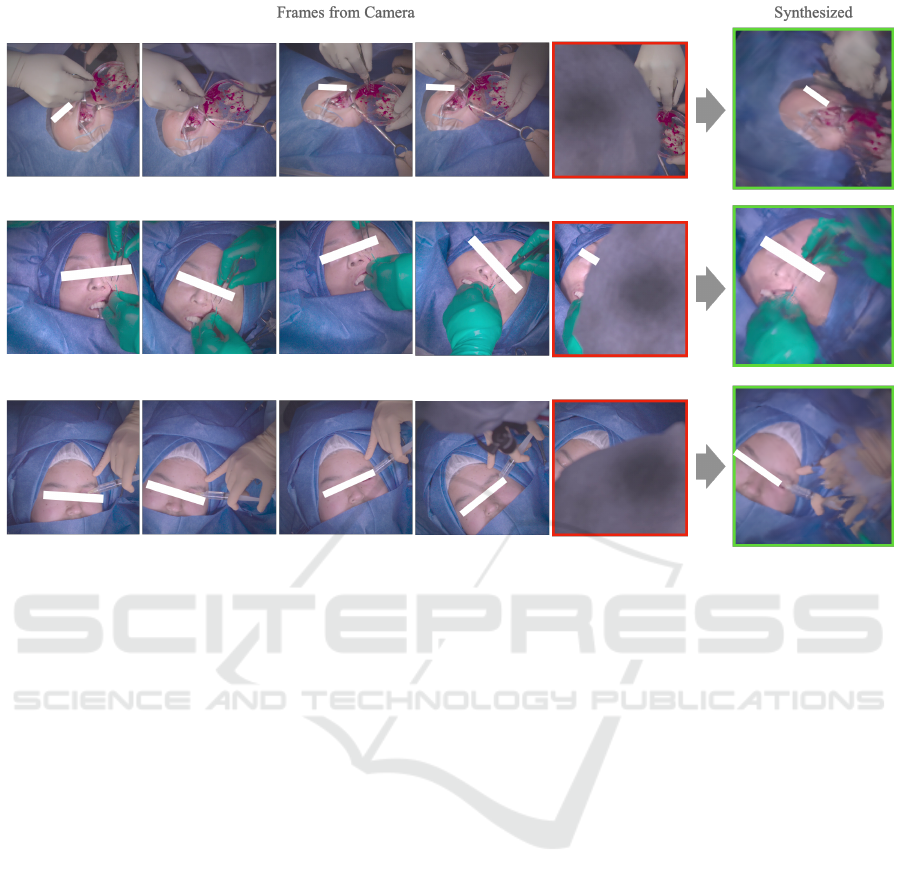
Figure 4: Novel view synthesis result for frames not included in the training set. The GNT has the capabiity to generate the
surgical area occluded by the surgion’s head. The images framed in red dipict the frames that are surgical areas occluded by
the surgion’s head. The images framed in green illustrated the generated result for the same camera positions as the red-framed
images.
The second step is to extract the frames from the
training videos. In this step, we only extract the
frames that are not occluded by the doctors or nurses,
as shown in Fig. 3-(a).
The third step is to run COLMAP (Sch
¨
onberger
and Frahm, 2016) to obtain the camera parameters
for the extracted frames. This step also removes
the frames in which COLMAP failed to map feature
points from the dataset. This third step finalizes the
creation of the training dataset.
The fourth step is to train the GNT using the
dataset we create in Steps 1 through 3. Through
training in many types of surgical scene frames, GNT
learns a neural representation of the surgical scenes.
The fifth step is generating occluded areas using
the new multi-view images. In this step, we also use
COLMAP to obtain the camera parameters.
4 EXPERIMENTS
4.1 Real Surgical Scene Dataset
As no available dataset contains surgery recordings
with multiple cameras, we use the system proposed
by Shimizu et al. (Shimizu et al., 2020) to create
our dataset. All surgeries were recorded at Keio
University School of Medicine. Video recording of
the patients were approved by the Keio University
School of Medicine Ethics Committee, and written
informed consent is obtained from all patients or
their legal guardians. We recorded nine different
types of surgeries with five cameras attached to the
surgical lamp in a regular pentagon manner, as de-
picted in Fig. 1. We estimated the camera position
using the COLMAP structure-from-motion package
(Sch
¨
onberger and Frahm, 2016) for both training and
evaluation data.
4.2 Training Data
We used six different types of surgeries as the training
data (three of these examples are shown in Fig. 3-(a)).
For the training data, we extracted frames from the
videos at regular intervals. We excluded some time
stamps where the doctor’s head obscured the opera-
tive area in some cameras, as shown in Fig. 3-(b).
Novel View Synthesis for Unseen Surgery Recordings
947
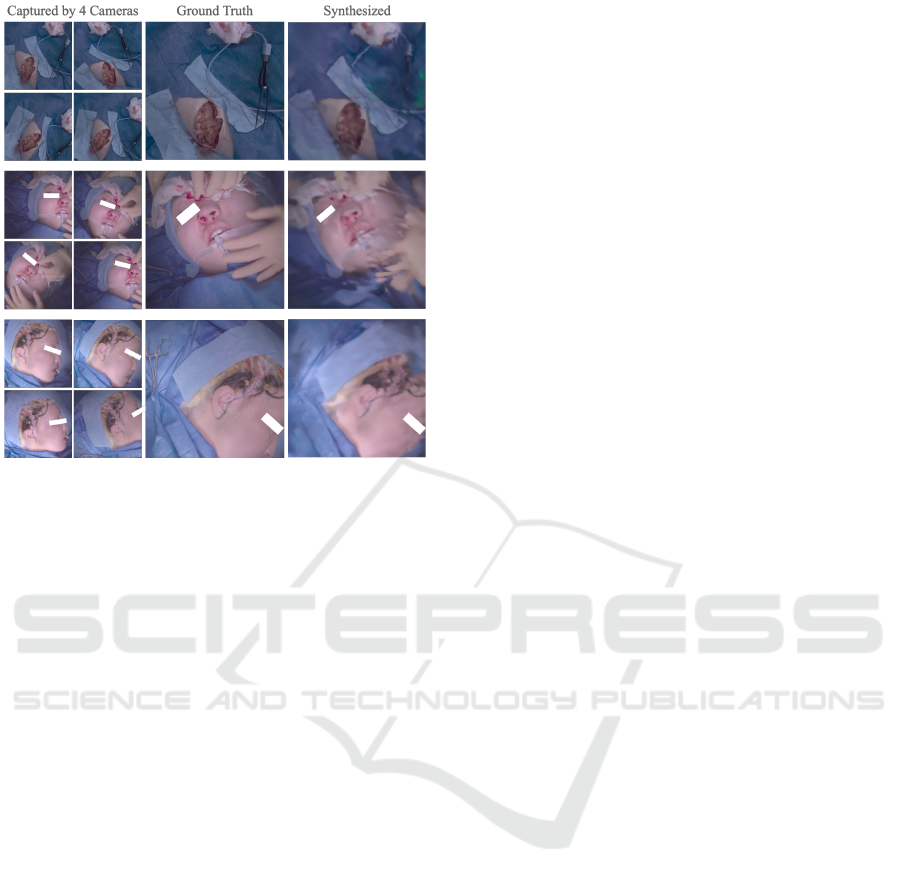
Figure 5: Novel view synthesis result for the multi-view
videos not in the training set. The GNT could generate the
occluded areas for three different kinds of surgical proce-
dures that are not in the training set.
4.3 Evaluation Data
For the evaluation, we used two different types of
datasets. The first one is the unknown “frames“ that
are excluded from the training data because they have
some frames that do not capture the surgical areas hid-
den by the doctor’s head. The second one is an un-
known “surgical scene“. These data are not included
in the training set and are different from the training
data for both the surgical type and the patient.
4.4 Training/Inference Setup
Following the official implementation of the GNT
network, we train both the feature extraction net-
work and the GNT end-to-end on datasets of multi-
view posed images using the Adam (Kingma and Ba,
2014) optimizer to minimize the mean-squared error
between predicted and ground truth RGB pixel val-
ues. For all our experiments, we trained for 250, 000
steps with 512 rays sampled in each iteration. We fol-
lowed the GNT’s multi-scene training setup for other
experimental parameters.
4.5 Result
On the Unknown Frames: The result of the unknown
frame dataset is shown in Fig. 4. The synthesized
frames are bordered with green and the frames with
the target camera pose are bordered with red. We can
see that the surgical area completely hidden by the
head is properly synthesized.
On the Unknown Surgical Scenes: The result of
the unknown surgical scenes dataset is shown in Fig.
5. We can see that the surgical area is properly syn-
thesized even though the GNT does not train in these
surgical scenes.
5 CONCLUSION
In this paper, we propose the utilization of a
transformer-based NeRF network called GNT (Wang
et al., 2022) for the purpose of generation of occluded
areas of surgical scenes. The aim of this approach
is to generate the occluded areas for new surgical
scenes without the need for a training network dur-
ing inference, using the GNT’s feature which can be
pre-trained by the previous surgical scenes. Our ex-
periments demonstrated that the GNT can effectively
learn real-world surgical scenarios, and can also gen-
erates the occluded surgical areas not only for un-
known frames as well as for unknown surgical scenar-
ios. As a future endeavor, we intend to devise a model
that can accurately determine the optimal camera po-
sition for rendering videos, to make it easier to create
review videos from the acquired multi-view videos.
ACKNOWLEDGEMENT
This work was supported by MHLW Health, Labour,
and Welfare Sciences Research Grants Research
on Medical ICT and Artificial Intelligence Pro-
gram Grant Number 20AC1004, the MIC/SCOPE
#201603003, and JSPS KAKENHI Grant Number
22H03617.
REFERENCES
Byrd, R. J., Ujjin, V. M., Kongchan, S. S., and Reed, H. D.
(2003). Surgical lighting system with integrated digi-
tal video camera. US Patent 6,633,328.
Davis, A., Levoy, M., and Durand, F. (2012). Unstructured
light fields. In Computer Graphics Forum, volume 31,
pages 305–314. Wiley Online Library.
Gortler, S. J., Grzeszczuk, R., Szeliski, R., and Cohen, M. F.
(1996). The lumigraph. In Proceedings of the 23rd
Annual Conference on Computer Graphics and inter-
active techniques, pages 43–54.
Hachiuma, R., Shimizu, T., Saito, H., Kajita, H., and Takat-
sume, Y. (2020). Deep selection: A fully supervised
VISAPP 2023 - 18th International Conference on Computer Vision Theory and Applications
948

camera selection network for surgery recordings. In
International Conference on Medical Image Comput-
ing and Computer-Assisted Intervention, pages 419–
428. Springer.
Kingma, D. P. and Ba, J. (2014). Adam: A
method for stochastic optimization. arXiv preprint
arXiv:1412.6980.
Kumar, A. S. and Pal, H. (2004). Digital video recording of
cardiac surgical procedures. The Annals of thoracic
surgery, 77(3):1063–1065.
Levoy, M. and Hanrahan, P. (1996). Light field rendering. In
Proceedings of the 23rd annual conference on Com-
puter graphics and interactive techniques, pages 31–
42.
Masuda, M., Saito, H., Takatsume, Y., and Kajita, H.
(2022). Novel view synthesis for surgical recording.
In MICCAI Workshop on Deep Generative Models,
pages 67–76. Springer.
Matsumoto, S., Sekine, K., Yamazaki, M., Funabiki, T.,
Orita, T., Shimizu, M., and Kitano, M. (2013). Digital
video recording in trauma surgery using commercially
available equipment. Scandinavian journal of trauma,
resuscitation and emergency medicine, 21(1):1–5.
Mildenhall, B., Srinivasan, P. P., Tancik, M., Barron, J. T.,
Ramamoorthi, R., and Ng, R. (2020). Nerf: Repre-
senting scenes as neural radiance fields for view syn-
thesis. In European conference on computer vision,
pages 405–421. Springer.
Murala, J. S., Singappuli, K., Swain, S. K., and Nunn, G. R.
(2010). Digital video recording of congenital heart
operations with ”surgical eye”. The Annals of thoracic
surgery, 90(4):1377–1378.
Sadri, A., Hunt, D., Rhobaye, S., and Juma, A. (2013).
Video recording of surgery to improve training in plas-
tic surgery. Journal of Plastic, Reconstructive & Aes-
thetic Surgery, 66(4):e122–e123.
Sch
¨
onberger, J. L. and Frahm, J.-M. (2016). Structure-
from-motion revisited. In Conference on Computer
Vision and Pattern Recognition (CVPR).
Shimizu, T., Oishi, K., Hachiuma, R., Kajita, H., Takat-
sume, Y., and Saito, H. (2020). Surgery recording
without occlusions by multi-view surgical videos. In
VISIGRAPP (5: VISAPP), pages 837–844.
Wang, P., Chen, X., Chen, T., Venugopalan, S., Wang, Z.,
et al. (2022). Is attention all nerf needs? arXiv
preprint arXiv:2207.13298.
Wang, Q., Wang, Z., Genova, K., Srinivasan, P., Zhou, H.,
Barron, J. T., Martin-Brualla, R., Snavely, N., and
Funkhouser, T. (2021). Ibrnet: Learning multi-view
image-based rendering. In CVPR.
Novel View Synthesis for Unseen Surgery Recordings
949
