
A Protocol to Assess Usability and Feasibility of e-SpeechT,
a Web-based System Supporting Speech Therapies
Vita Santa Barletta
a
, Miriana Calvano
b
, Antonio Curci
c
and Antonio Piccinno
d
Computer Science Department, University of Bari Aldo Moro, 70125 Bari, Italy
Keywords:
Speech Therapy, e-Health, Speech Impairment, Gamification, Usability Study, Telemedicine, Game-based
Learning.
Abstract:
Speech disorders and impairments are a heterogeneous group of dysfunctions that concern linguistic abilities
and, in the majority of cases, they affect people during their childhood from 4 to 6 years old. Appropriate
treatment should be defined for each patient according to their problems, which can be physical, such as
muscle weakness, brain damage, vocal cord damage, or paralysis, and psychological, such as autism, PTSD
or Down Syndrome. Therefore, considering these aspects, this research work aims at supporting patients in
carrying out therapies to solve speech impairments through gamification, game-based learning, e-health, and
telemedicine. A web-based system is proposed to achieve the goals by supporting all stakeholders involved in
speech therapy. The design and plan of a usability and a longitudinal study have been presented, with the goal
of testing the system’s usability and medical efficacy by involving real end-users and domain experts.
1 INTRODUCTION
Speech therapy is the treatment of speech disorders
founded on the application of notions and methods
pertaining primarily to phoniatrics but also to other
disciplines such as glottology, psychology, pedagogy,
and neurology (Law et al., 2003).
Speech disorders refer to the disruption of ”nor-
mal speech”: they affect the vocal cords, muscles,
nerves, and other structures within the throat, due for
example to vocal cord damage, brain damage, mus-
cle weakness, or vocal cord paralysis. So, the ar-
eas of communication involved in this disorder are
phonology, the pattern of sounds used by the child;
grammar, the way that language is constructed; vo-
cabulary, the words that a child can say and under-
stand, morphology, meaningful changes to words to
signal tense, number, etc.; narrative skills, the ability
to relate a sequence of ideas; pragmatic language that
refers to the social language skills in the interaction
with others and in a given situation (Hourcade, 2015;
Law et al., 2003; Adams et al., 2012).
Nowadays, rehabilitation therapies for speech
a
https://orcid.org/0000-0002-0163-6786
b
https://orcid.org/0000-0002-9507-9940
c
https://orcid.org/0000-0001-6863-872X
d
https://orcid.org/0000-0003-1561-7073
problems are administered by specialists, who are
called speech therapists, and consist in the perfor-
mance of exercises calibrated and chosen with the
aim of solving the specific problems of each subject.
Assessment of eligibility for intervention includes
a combination of standardized assessment, observa-
tions of linguistic and communicative performance,
and professional judgment (Law et al., 2003). Thanks
to speech therapies, speech disorders can improve: in
order to strengthen the muscles of the face and throat,
a professional therapist guides the patient through dif-
ferent types of exercises (Barletta et al., 2022). It is
important to underline that therapists prescribe chil-
dren to also practice also at home. In some cases,
exercises are perceived as boring, which causes chil-
dren to underperform, to carry them out incorrectly,
or to refuse to perform them. Unfortunately, this as-
pect is not verifiable by therapists and it is out of their
control. Thanks to the currently available technology,
these limitations can be overcome and patients can
feel more comfortable.
In speech therapy, three categories of stakeholders
are involved:
1. Speech therapists, who are doctors who have the
goal of resolving problems involving speech im-
pairment and disorders. They usually define a
personalized treatment program to help solve chil-
dren’s speech difficulties and prevent subsequent
546
Barletta, V., Calvano, M., Curci, A. and Piccinno, A.
A Protocol to Assess Usability and Feasibility of e-SpeechT, a Web-based System Supporting Speech Therapies.
DOI: 10.5220/0011893300003414
In Proceedings of the 16th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2023) - Volume 5: HEALTHINF, pages 546-553
ISBN: 978-989-758-631-6; ISSN: 2184-4305
Copyright © 2024 by Paper published under CC license (CC BY-NC-ND 4.0)

literacy problems.
2. Caregivers, who are parents or anyone who looks
after the children when they have to follow speech
therapies.
3. Patients, who are children from 4 to 6 years old
who are affected by speech disorders.
Currently, limited technological applications sup-
port speech therapists and patients during therapy at
home (Cassano et al., 2022). But at the same time, the
researchers demonstrate that the idea of supporting
this process by using multimedia and smartphone to
make the activity more enjoyable for the target users
is quite widespread (Jesus et al., 2019a; Pentiuc et al.,
2010; Rossano et al., 2020). Thus, considering the
ever-evolving and ever-growing ICT in the medical
field, the idea is to develop a system that simplifies
the process of administering therapies to children, be-
cause it enables them to carry out exercises from their
homes, having their caregiver’s supervision and the
therapists’ remote monitoring (Desolda et al., 2021;
Butcher et al., 1987). This can be possible if therapies
are delivered through mobile and ”smart” computing
devices. This results in the development of mobile ap-
plications or, even better, the introduction of systems
that can be accessed from mobile devices, and with
the introduction of new concepts and principles, such
as ”gamification” and ”game-based learning” (Saeedi
et al., 2022) for a more effective employement in fol-
lowing the therapies.
The paper presents a web-based system to sup-
port speech therapists in administering and monitor-
ing therapies that aim at solving problems involv-
ing phonology, morphology, content, and structure of
speech. It represents a concrete application of princi-
ples, such as e-health, telemedicine, gamification, and
game-based learning. The system targets are children
as patients, from 4 to 6 years old, speech therapists,
and caregivers.
The goals are to help therapists to manage and to
monitor their patients in a quicker and more structured
way; patients carry out the exercises without the need
to physically go to a facility. In addition, the plan of a
usability study and a longitudinal study is presented,
which will be performed in the next future to test the
system’s usability and medical efficacy.
2 SYSTEM DESCRIPTION
e-SpeechT is a system that offers different function-
alities and graphical interfaces for each type of user
will be shown. On the welcome page of e-SpeechT,
users can select their role, log in or create a new ac-
count. Therapists, caregivers, and patients play three
distinctive roles, according to which the system dis-
plays and enables different functionalities. In order to
be consistent with its diverse audience, when children
use the application, the graphical interface becomes
more playful.
2.1 Speech Therapist
The speech therapist’s perspective of e-SpeechT al-
lows to create and to monitor therapies for each child.
More specifically, as shown in Figure 1, the main
actions that the system allows speech therapists to
perform are listed below: view current and previ-
ous diagnoses; create new therapies and view previ-
ous ones; view the results and their statistics of the
exercises carried out by the patient; check and per-
form corrections on the previously-mentioned exer-
cises; view patients’ personal data.
Figure 1: An example of the patient’s web-page from the
therapists point of view.
The menu section in the upper-central part of Fig-
ure 1 is composed of four sections:
1. add a new patient;
2. monitor and create exercises for therapies;
3. open a calendar where the schedule of appoint-
ments for each patient is shown;
4. receive miscellaneous notifications.
In addition, speech therapists can create a series,
that is a predefined sequence of exercises that will
be administered each time in the same order. It is
crucial to adapt the level of difficulty of exercises
to the patient’s needs, age, and diagnosis in order
to make a balanced and proper evaluation (Pagano
and Marengo, 2021). e-SpeechT allows therapists to
set an error tolerance threshold that plays an impor-
tant role in the automatic correction of exercises per-
formed by the system. This functionality was imple-
mented by training a classification model using the
voice recordings of fifteen children. In Figure 2, an
example of threshold setting is shown.
A Protocol to Assess Usability and Feasibility of e-SpeechT, a Web-based System Supporting Speech Therapies
547
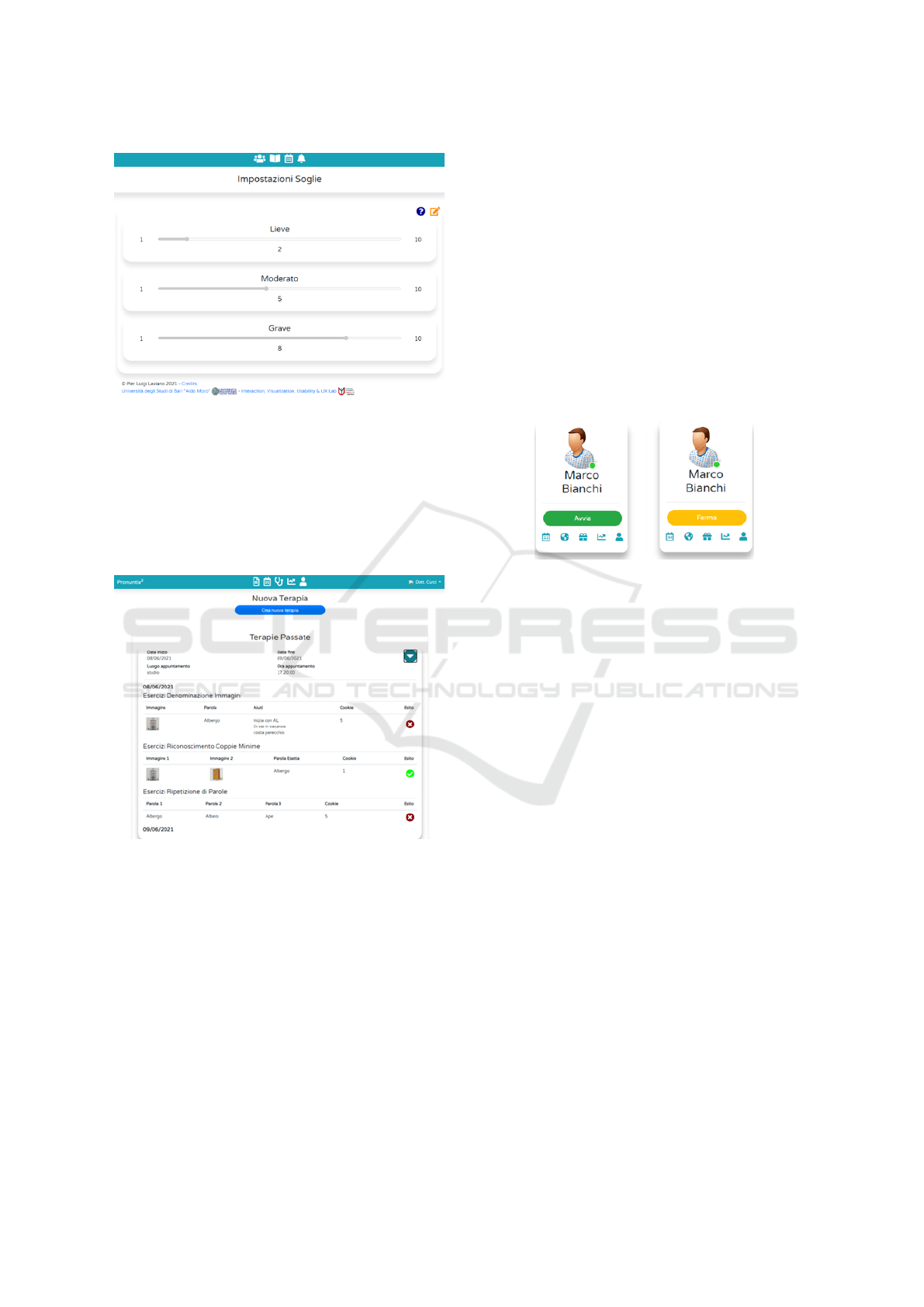
Figure 2: Setting of the error tolerance threshold.
The visualization and the automatic exercise cor-
rections provided by the system to the therapist are
shown in Figure 3. However, therapists are allowed
to change these corrections manually.
On the top right, a drop-down menu allows to
change their personal data, view the screening page,
and log out of the system.
Figure 3: Therapy and patient overview.
2.2 Caregiver
Similarly to speech therapists, the first page shown
to caregivers is an overview of all the children that
they are associated with, because there might be mul-
tiple patients in the same family. The following
functionalities are offered to the caregiver: accessing
the calendar section where all the appointments and
medical examinations available; accessing the gifts
and rewards section; viewing reports and statistics
of the exercises performed by the child; viewing the
child’s personal information; changing the aspect of
the child’s personal area by setting a playful wallpa-
per, called ”scenario”.
Through their caregiver’s account, children can set
the password to log into their personal area. Since
this system targets children aged from 4 to 6 years
old, their reading and writing skills are at a very early
stage or not present at all, therefore, a graphical pass-
word has been opted for. In order to let children feel
comfortable and welcomed, the graphical password
consists of a cartoon character to be chosen from a
list proposed by the system.
Caregivers are allowed to start or stop the admin-
istration of therapy in order to choose a specific and
dedicated period of time in which a child has to carry
out the designated exercises. This functionality is
shown in Figure 4.
Figure 4: Therapy options: on the left the button that allows
to start a therapy and on the right the one that allows to stop
a therapy.
On the top right, a drop-down menu can be opened
in which caregivers can view their personal informa-
tion and log out of the system.
2.3 Patient
Patients use the system to carry out exercises pre-
scribed by the therapist by playing serious games. Ex-
amples of exercises are shown, described, and ana-
lyzed in the next section.
3 THE GAME-BASED LEARNING
APPROACH
The e-SpeechT system embodies principles like gam-
ification and game-based learning. Every aspect of
the system that involves interaction with children is
in the form of games or contains playful aspects
(Di Bitonto et al., 2014). In the following sections,
the patient area will be illustrated.
3.1 Login-Method
The login phase is composed of two steps: speech
therapist choice and password selection; each patient
can access their personal area by choosing among the
HEALTHINF 2023 - 16th International Conference on Health Informatics
548

list of speech therapists in the system by recogniz-
ing their profile picture; then, they will need to select
the password image chosen together with her/his care-
giver, as shown in Figure 5.
Figure 5: Child Login page: therapist and password selec-
tion.
Once the child has successfully logged in to the
system, a home screen is shown and both a textual
and audio welcome message is given.
3.2 Exercises
Three categories of exercises can be identified in e-
SpeechT:
1. Naming images;
2. Minimum pair recognition
3. Repetition of Words.
For the first type of exercise, Naming Images, the
system will show on the left the image associated with
the word to pronounce and on the right an orange but-
ton with the icon of a microphone. Under this button,
hints are provided for the execution of the exercise in
the form of buttons representing a loudspeaker; press-
ing on them, the system will reproduce vocally the
selected hint. See, as an example, Figure 6.
Figure 6: Naming Images exercise.
In the Minimum Pair Recognition exercise, the
graphic interface will consist of two images corre-
sponding to the words placed on the sides of the
screen, and a button with a speaker icon between
them: by pressing this button, the system will repro-
duce the name of the correct word. The position of
the correct image will be randomly generated each
time a user accesses the execution of the exercise. To
perform the exercise correctly, the patient must repro-
duce the name of the word, and associate it with one
of the two images by pressing on the possibly correct
one (see, for example, Figure 7).
Figure 7: Minimun Pair Recognition exercise.
For the last type of exercise, Repetition of Words,
two buttons are shown in the center of the screen.
The first one represents the icon of a microphone and
the second one that of a speaker; below, one next to
the other, there will be the three words that the child
will have to pronounce. By clicking on them, the im-
age associated with the words will appear as an ad-
ditional hint for the exercise. To carry out the exer-
cise correctly, the child can reproduce the sequence
of words spoken by the system by pressing the button
with the speaker icon and use the hints by pressing
on the words he is uncertain about; in any case, he
needs to press the button with the microphone icon,
pronounce the sequence of words in the correct order,
and press the same button again (see Figure 8).
3.2.1 Exercise Execution
Depending on the type of exercise the child is doing,
the proposed interface changes. Each time the child
completes the execution of an exercise, the system
will show him/her a window with a message, either
written or spoken, congratulating him/her on complet-
ing the exercise, regardless of the outcome. In case
the exercise is performed correctly, the message will
also indicate the earned cookies, which act as a re-
ward.
A Protocol to Assess Usability and Feasibility of e-SpeechT, a Web-based System Supporting Speech Therapies
549

Figure 8: Repetition of Words exercise.
4 EVALUATION PLAN
In order to plan an evaluation of the system’s usability
and medical efficiency, we involved two speech ther-
apists from the hospital of Bari ”Papa Giovanni Paolo
XXIII”, with whom we already collaborated in the de-
veloping process of the system. A series of meetings
and discussions were carried out with speech thera-
pists in order to get an insight into the medical aspects
to consider and the appropriate features to evaluate;
their expertise was fundamental during this phase.
Two types of studies have been planned: Usability
and Longitudinal study (Razak et al., 2010; Lazar
et al., 2017). Therefore, the usability study has the
goal of analysing the users’ overall experience with
the system and its features, while the Longitudinal
study is related to the system’s medical effectiveness
and efficacy and the impact on the children’s speech
impairments. Before planning the study, to obtain an
insightful opinion about the system, a pilot study was
conducted involving two speech therapists. The prob-
lems reported in this phase were resolved in advance
to avoid evaluating an already-known faulty system.
This plan involves, in both cases, 10-13 speech
therapists and 20-23 caregivers and 20-23 patients
(because each child is associated with one caregiver).
The group of therapists has also supported the process
of drafting questionnaires, tasks choice, and the dura-
tion of the longitudinal study. In order to guarantee
participants’ privacy, it has been established to assign
to each of them an identification code.
4.1 Usability Study
The usability study consists of the execution of tasks
and filling out questionnaires. This study is planned
to be conducted in a remote way by using the plat-
form ”eGLU-BOX”, a software to support usability
testing based on the eGLU LG 2018.1 protocol (Fed-
erici et al., 2021)
1
. The tasks have been chosen care-
fully by considering all the main functionalities of the
system and the domain requisites. The creation of the
testers’ accounts on eGLU-BOX will be carried out
before the administration of the test in order to speed
up the process. Two different studies have been cre-
ated: one for speech therapists and one for caregivers,
called respectively “Test iniziale e-SpeechT – Logo-
pedisti” and “Test iniziale e-SpeechT – Caregiver”,
respectively. Each task will be evaluated taking into
account the stress factor that often alters the behavior
of participants. Therefore, two additional steps will
be taken before starting the test. The first is an expla-
nation of the study and its goal will have to be carried
out before starting the test. This evaluation plan also
includes an introductory questionnaire in which each
participant is asked to provide personal information
in order to profile them and evaluate their experience
in relation to their age, experience with technology,
and systems supporting health. The second step is
a video demos of e-SpeechT, in which they will be
provided with a first overview of the system and its
main functionalities, in order to let them gain comfort
and reduce the stress factor for novice users. The de-
mos at hand bring attention to possible malfunctions
and anomalies that might be encountered, explaining
how to recover from them. The maximum duration
planned for each task is 5 minutes.
4.1.1 Study with Speech Therapists
This study involves 10-13 therapists and the execu-
tion of 6 tasks; for each task, the participant will have
5 minutes to carry it out. The title and the instructions
for each task has a title and instructions are listed be-
low:
1. ”Create a therapy”: fill out the form with the re-
quested information and add some exercises to as-
sign to the patient.
2. ”Monitor statistics”: correct and mark exercises
from the therapies section for a patient.
3. ”Create exercises”: create an exercise for each
category (Naming Images, Repetition of Words,
and Minimum Pair Recognition).
4. ”Create a new word”: create a new word, fill out
the form with the requested information and add
its image.
5. ”Modify thresholds”: change the thresholds and
make some trials to check if the system’s behavior
has actually been affected.
1
https://egluboxpa.ddns.net/public/
HEALTHINF 2023 - 16th International Conference on Health Informatics
550

4.1.2 Study with Caregivers
The designated number for this part of the study is
from 10 to 13 caregivers. Analogously to speech ther-
apists, caregivers will be asked to carry out the follow-
ing tasks:
1. ”Set a password for a new child”: set a password
by choosing among one of the cartoon characters.
2. ”Start a therapy”: start the therapy for a child for
which the button is enabled.
3. ”Monitor statistics”: view the statistics and results
of the exercises carried out by a child.
4. ”Stop a therapy”: Stop a therapy for the child
whose therapy has been previously started.
4.2 Longitudinal Study
The longitudinal study has been planned with the goal
of measuring the effectiveness, the ease of familiar-
ization with the system, and the differences between
the traditional and experimental approaches of the
system. In order to perform a proper evaluation, the
between-subject design technique has been chosen,
which consists in forming a control and an experi-
mental group. The planning phase was carried out
after an accurate literature analysis of the use of di-
aries and data gathering in longitudinal studies (Lazar
et al., 2017); in this case, diaries are in the form of
questionnaires that are filled out periodically to un-
derstand how the interaction with the system evolves
over time. The recruitment of children and their care-
givers is delegated to the speech therapists, who are
in charge of creating two homogeneous groups in or-
der to balance out potential individual differences that
could ruin the end results. After many meetings and
an in-depth discussion, it was concluded that since
the smallest period of time necessary to obtain med-
ically relevant results and to check the impacts of
therapies on children is 6 weeks, the estimated dura-
tion of the study is 6-8 weeks. The effectiveness and
relevancy of continuous communication with thera-
pists during longitudinal studies can be observed in
the literature, too; an example is the ”Tablet-to-Tablet
(T2T) Speech and Language Therapy Software De-
velopment Roadmap” (Jesus et al., 2019b), in which
the testing phase of systems that support speech ther-
apies focuses on real end-users and lasts around 6
weeks. It is worth to underline that the medical re-
sults of the study will be evaluated by the speech ther-
apists, while computer scientists will take care of only
the technical aspects.
In the following two sections, the activities of each
group will be described in more detail.
4.2.1 Experimental Group
The experimental group will be formed by 10-13 pa-
tients with their caregivers and they will carry out
the therapies with the support of e-SpeechT. The plan
consists of the periodical administration of a ques-
tionnaire, through Google Form, that consists of ques-
tions about the main services that participants avail of,
according to the type of participant. Two question-
naires have been created, and both of them contain
questions about the experience of the patient in order
to get an insight from two different points of view.
The questionnaire for the speech therapists includes
questions that concern the used device, the ease of
use when creating a therapy, the automatic correc-
tion tool for exercises, and a section for possible other
weaknesses or problems that emerged. The question-
naire for caregivers includes questions that concern
the process of starting/stopping the therapy, the expe-
rience while flanking their child while using the sys-
tem, monitoring the statistics, and a section for other
miscellaneous observations.
For caregivers, the questionnaire is administered
right after the child’s completion of the series of ex-
ercises planned for the day, implemented into the sys-
tem.
The section of the questionnaire concerning the
patient’s experience remains unchanged regardless of
whether it is administered to a caregiver or a therapist.
They are asked about the time taken to complete ex-
ercises, the process of logging in their personal area,
the emotions expressed by the child while playing and
how they are adjusting to the system as time passes.
Some questions are:
• ”If the child encountered problems while logging
into e-SpeechT, please specify them”.
• ”Did the child have fun while playing?”
• ”Did the child want to quit the game before its
end?”
The type of response varies among Likert scale,
multi-options, and open text.
Emotional reactions are crucial when it comes to
evaluating children’s experiences because they are of-
ten raw and unfiltered, letting the most relevant as-
pects emerge. Since the target patients are children,
asking them to fill out a questionnaire would be in-
feasible for two main reasons: the playful atmosphere
would get ruined and some of them are not old enough
to read and comprehend their content. Hence, care-
givers and therapists will have to answer in their
place. Nevertheless, a prototype of a pop-up has been
designed and implemented in order to administer a
rating scale question directly to the patient through a
A Protocol to Assess Usability and Feasibility of e-SpeechT, a Web-based System Supporting Speech Therapies
551
smileyometer, shown in Figure 9, in which the scale
is in the shape of smileys (Bell, 2007; Jesus et al.,
2019b).
Figure 9: Pop-up with smileyometer.
The data obtained through these questionnaires
will be analyzed at the end of the study to understand
its outcomes and results; they will be compared with
those obtained from the control group to draw conclu-
sions.
4.2.2 The Control Group
The control group will be formed by 10-13 patients
with their caregivers and they will carry out the ther-
apies in a traditional way, without the help of e-
SpeechT. They will not have to answer periodic ques-
tionnaires, since traditional protocols and methods do
not need to be further proven as effective. The com-
parison will only involve the results and the impact
that the therapies have had on the children.
5 CONCLUSIONS AND FUTURE
WORKS
Systems that support medicine, health, and well-
being are spreading more and more in today’s world.
Speech therapy is a field in which technology can
be extremely helpful since patients’ perseverance and
time consistency is crucial for the successful outcome
of treatments. e-SpeechT is a web-based system de-
signed for speech therapists who oversee young pa-
tients with primary language disorders, followed in
their therapies by a Caregiver, who can be a parent
or a figure close to the child who assists her/him in
the execution of therapies. Dealing with systems that
are accurately designed and carefully tested is funda-
mental in order for them to be effective, efficient, and
satisfactory.
The initial pilot study with speech therapists
brought up some interesting points that highlighted
the problems and strengths of the system, which re-
sulted to be very useful to plan the usability and lon-
gitudinal studies. This study researched the most con-
venient and appropriate ways to evaluate e-SpeechT
in question by creating an evaluation plan both for
usability and longitudinal studies can be the tool to
portray an analysis of the most relevant aspects of
e-SpeechT. The evaluation plan also involved initial
research of the potential participants to recruit. The
study was not conducted right after the planning phase
because of the COVID-19 pandemic. It resulted that
parents and caregivers were not enticed by the idea of
letting their children follow therapies on digital plat-
forms because of the long period of forced distance
learning that had just passed. Therefore, it is intended
to conduct the planned studies at a later time. Gaining
familiarity with new applications and systems might
be demanding for some; nevertheless, the advantages
that come after that first phase are highly beneficial
to all parties involved. In addition, speech therapists
appreciated e-SpeechT during the pilot studies and
seemed to grasp its potential; they have shown interest
to extend the use of the system also to children with
more serious issues, such as Down syndrome.
As future works, it would be interesting to use
the Medical Research Framework (Craig et al., 2008;
Shahsavari et al., 2020) to understand the differences
between assessing feasibility and assessing effective-
ness of the system; this framework emphasizes that
any intervention should be presented to the patients
tailored to the context and culture of the society they
live in, considering political, social, and geographi-
cal aspects (Huang et al., 2021). In conclusion, it is
intended to improve the implementation of the login
method for children by adding a geolocalization fea-
ture, in order to improve the systems’ security and
preserve users’ privacy (Baldassarre et al., 2021).
ACKNOWLEDGEMENTS
The support of University of Bari through grant
“Horizon Europe Seeds 2021” is acknowledged. We
would also thank the student Pier Luigi Laviano
who re-engineered the system during his master the-
sis work, the speech therapists Isabella Roppa and
Roberta Cassano from the “Giovanni XXIII” Pedi-
atric Hospital of Bari for their collaboration in the
system requirements collection, analysis, and study
planning.
HEALTHINF 2023 - 16th International Conference on Health Informatics
552

REFERENCES
Adams, C., Lockton, E., Freed, J., Gaile, J., Earl, G.,
McBean, K., Nash, M., Green, J., Vail, A., and Law,
J. (2012). The social communication intervention
project: A randomized controlled trial of the effective-
ness of speech and language therapy for school-age
children who have pragmatic and social communica-
tion problems with or without autism spectrum disor-
der. International journal of language & communica-
tion disorders / Royal College of Speech & Language
Therapists, 47:233–44.
Baldassarre, M. T., Barletta, V. S., Caivano, D., and Pic-
cinno, A. (2021). Integrating security and privacy in
hcd-scrum. In CHItaly 2021: 14th Biannual Con-
ference of the Italian SIGCHI Chapter, CHItaly ’21,
New York, NY, USA. Association for Computing Ma-
chinery.
Barletta, V. S., Cassano, F., Pagano, A., and Piccinno, A.
(2022). A collaborative ai dataset creation for speech
therapies. volume 3136, page 81 – 85.
Bell, A. (2007). Designing and testing questionnaires for
children. Journal of research in nursing, page 462.
Butcher, P., Elias, A., Raven, R., Yeatman, J., and Little-
johns, D. (1987). Psychogenic voice disorder unre-
sponsive to speech therapy: Psychological character-
istics and cognitive-behaviour therapy in children: A
systematic review of features and challenges. Interna-
tional Journal of language and speech disorders.
Cassano, F., Pagano, A., and Piccinno, A. (2022). Support-
ing speech therapies at (smart) home through voice
assistance. In Novais, P., Carneiro, J., and Chamoso,
P., editors, Ambient Intelligence – Software and Appli-
cations – 12th International Symposium on Ambient
Intelligence, pages 105–113, Cham. Springer Interna-
tional Publishing.
Craig, P., Dieppe, P., Macintyre, S., Michie, S., Nazareth,
I., and Petticrew, M. (2008). Developing and evaluat-
ing complex interventions: the new medical research
council guidance. British Medical Journal.
Desolda, G., Lanzilotti, R., Piccinno, A., and Rossano, V.
(2021). A system to support children in speech ther-
apies at home. In CHItaly 2021: 14th Biannual Con-
ference of the Italian SIGCHI Chapter, CHItaly ’21,
New York, NY, USA. Association for Computing Ma-
chinery.
Di Bitonto, P., Corriero, N., Pesare, E., Rossano, V., and
Roselli, T. (2014). Training and learning in e-health
using the gamification approach: The trainer interac-
tion. Lecture Notes in Computer Science (including
subseries Lecture Notes in Artificial Intelligence and
Lecture Notes in Bioinformatics), 8515 LNCS(PART
3):228 – 237.
Federici, S., Mele, M. L., Bracalenti, M., De Filippis, M. L.,
Lanzilotti, R., Desolda, G., Borsci, S., Gaudino, G.,
Cocco, A., Amendola, M., and Simonetti, E. (2021).
A Chatbot Solution for eGLU-Box Pro: The Usabil-
ity Evaluation Platform for Italian Public Administra-
tions, pages 268–279.
Hourcade, J. P. (2015). Child-computer interaction. The
publishing company, 1st edition.
Huang, R. X., Pagano, A., and Marengo, A. (2021). Build-
ing a pedagogical framework for the education of sus-
tainable development using a values-based education
approach. page 78 – 82.
Jesus, L., Martinez, J., Santos, J., Hall, A., and Joffe, V.
(2019a). Comparing traditional and tablet-based in-
tervention for children with speech sound disorders:
A randomized controlled trial. Journal of Speech Lan-
guage and Hearing Research, 62:4045–4061.
Jesus, L., Santos, J., and Martinez, J. (2019b). The table
to tablet (t2t) speech and language therapy software
development roadmap. JMIR Research Protocols, 8.
Law, J., Garrett, Z., and Nye, C. (2003). ‘speech and lan-
guage therapy intervention for children with primary
speech and language delay or disorder: Cochrane
developmental, psychosocial and learning problems
group.’. Cochrane database of systematic reviews
(Online), 3:CD004110.
Lazar, J., Feng, J. H., and Hochheiser, H. (2017). Chapter
6 - diaries. In Lazar, J., Feng, J. H., and Hochheiser,
H., editors, Research Methods in Human Computer
Interaction (Second Edition), pages 135–152. Morgan
Kaufmann, Boston, second edition edition.
Pagano, A. and Marengo, A. (2021). Training time opti-
mization through adaptive learning strategy. page 563
– 567.
Pentiuc, S. G., Tobolcea, I., Schipor, O. A., Danubianu, M.,
and Schipor, D. M. (2010). Translation of the speech
therapy programs in the logomon assisted therapy sys-
tem. Advances in Electrical and Computer Engineer-
ing, 10:48–52.
Razak, F. H. A., Hafit, H., Sedi, N., Zubaidi, N. A.,
and Haron, H. (2010). Usability testing with chil-
dren: Laboratory vs field studies. In 2010 Interna-
tional Conference on User Science and Engineering
(i-USEr), pages 104–109.
Rossano, V., Lanzilotti, R., Cazzolla, A., and Roselli, T.
(2020). Augmented reality to support geometry learn-
ing. IEEE Access, 8:107772–107780.
Saeedi, S., Bouraghi, H., Seifpanahi, M.-S., and
Ghazisaeedi, M. (2022). Application of digital games
for speech therapy in children: A systematic re-
view of features and challenges. National Library of
Medicine.
Shahsavari, H., Matourypour, P., Ghyasvandian, S., and Ne-
jad, M. (2020). Medical research council framework
for development and evaluation of complex interven-
tions: A comprehensive guidance. Journal of Educa-
tion and Health Promotion, 9:88.
A Protocol to Assess Usability and Feasibility of e-SpeechT, a Web-based System Supporting Speech Therapies
553
