
Trust in and Acceptance of Video-based AAL Technologies
Sophia Otten
a
, Wiktoria Wilkowska
b
, Julia Offermann
c
and Martina Ziefle
d
Chair of Communication Science, Human-Computer Interaction Centre, RWTH Aachen University, Campus-Boulevard 57,
Aachen, Germany
Keywords: Trust, Video-based AAL Technology (VAAL), Technology Acceptance.
Abstract: Due to a growing demand and need for solutions that alleviate the strain on the overburdened healthcare
system, video-based ambient assisted living (VAAL) technologies offer a good alternative to support
individuals in need of help. In order to successfully implement such technologies into the living spaces of
individuals with care needs, factors that determine their trust in, and acceptance of, such technology need to
be examined in more detail. This study investigates perceptions on trust and its relationship with the
acceptance criteria of VAAL technologies. In a mixed-methods design approach using focus groups and a
questionnaire study, participants evaluated their trust and acceptance perceptions of VAAL technology and
assessed its benefits and barriers. Results revealed significant relationships between the variables, signalling
the relevance of understanding of how trust may influence the overall acceptance of VAAL technologies.
Recommendations for future studies as well as applications of the findings are made.
1 INTRODUCTION
As of this moment, there is both a shortage of
healthcare personnel that is expected to increase and
a growing demand of people with care needs (Michel
& Ercanot, 2020). These issues have been further
exacerbated by the ongoing Covid-19 pandemic and
will bring about multiple serious societal issues, such
as maintaining the relationship with physicians in
people with chronic diseases (Erquicia et al., 2020).
In order to combat these challenges, there are several
approaches to go about it. One of them, in an attempt
of digitalising processes in all sectors of the public,
are assistive technologies. These kinds of devices and
systems are designed to enable people with care needs
to live a more autonomous life and keep their quality
of life while still having support for their
requirements (Peek et al., 2014, Wahezi et al., 2021).
Specifically, ambient and assisted living (AAL)
technologies are a type of technology that is typically
used for monitoring health status and behaviours,
such as detecting falls or recognising movement
patterns. These include wearable or ambient-installed
a
https://orcid.org/0000-0002-4027-5362
b
https://orcid.org/0000-0002-7163-3492
c
https://orcid.org/0000-0003-1870-2775
d
https://orcid.org/0000-0002-6105-4729
sensors that are used in people’s homes or permanent
care facilities (Climent-Perez et al., 2020; Steinke et
al., 2012). More precisely, video-based AAL
technologies (VAAL) can be used to monitor
people’s behaviours and alert medical personnel
and/or family members in case of a medical
emergency without having to interact with the users.
However, many of these solutions are still under
construction and more information about their
potential is needed. While studies often focus on
technological or legal obstacles, the perspective of
potential users is often missing. It is therefore
important to investigate people’s acceptance of AAL
technologies and what plays into their decisions to
use them, conducting studies from a user-centred
perspective (Offermann-van Heek & Ziefle, 2019).
Perceived benefits and barriers are proven to make
it more or less likely for people to accept such
technologies (Jaschinski & Allouch, 2015;
Wilkowska et al., 2021). Some examples of potential
benefits are the (re)gained independence and health-
related security of immediate help, while some
examples of potential barriers include data
management, usability, and trust issues (Schomakers
126
Otten, S., Wilkowska, W., Offermann, J. and Ziefle, M.
Trust in and Acceptance of Video-based AAL Technologies.
DOI: 10.5220/0011785500003476
In Proceedings of the 9th International Conference on Information and Communication Technologies for Ageing Well and e-Health (ICT4AWE 2023), pages 126-134
ISBN: 978-989-758-645-3; ISSN: 2184-4984
Copyright
c
2023 by SCITEPRESS – Science and Technology Publications, Lda. Under CC license (CC BY-NC-ND 4.0)

et al., 2021). In addition, other factors shape the AAL
acceptance by potential users, like privacy, perceived
control, attitudes towards AAL, medical necessity, as
well as the added value to their daily life (Jaschinski
et al., 2021; Offermann-van Heek et al., 2019).
The Technology Acceptance Model (TAM; Davis,
1989) has been widely used in technology acceptance
research. This model assumes that two key
components significantly influence the attitude
towards its use: 1) perceived ease of use a given
technology, and 2) perceived usefulness that relates
to the idea of how useful the technology is. These
components are closely related to the behavioural
intention to use and the actual use of this technology.
Current research on health-related technologies
applied TAM in different contexts, confirming the
predictive power and determining role of these
criteria for innovative technologies (Rahimi et al.,
2018; Alshammari & Rosli, 2020).
In line with trading off the benefits and barriers,
potential users consider trust in these systems to be
vital. Throughout the literature, trust has been
conceptualised a human belief and expectancy and is
considered and interplay of a trustors and a trustee
(McKnight & Chervany, 2001). For trust in medical
technology, three main dimensions are relevant: user,
technology, and context factors (Xu et al., 2014; Bova
et al., 2006). However, as the development and use of
technologies is rapidly advancing, a more nuanced
distinction of how people form trust in VAAL
technology is necessary. Research shows that whether
and how people trust a particular technology is
dependent on both factors relating directly to the
technology but also context-related influences, such
as trust in their physician (Qiao et al., 2015). This
suggests that trust is influenced by multiple aspects,
and the way how people form trust in technology is
complex. Specifically, trust in technology has been
shown to be crucial for later acceptance (Wilkowska
& Ziefle, 2019). Due to the different measurements
of acceptance and trust in (V)AAL technology across
studies, results might differ (Wilkowska et al., 2015).
Considering this gap, this empirical study aims at
identifying relevant trust factors for the use of VAAL
technology, applying a mixed method approach.
2 QUALITATIVE APPROACH
First, an interview study was run with the purpose of
identifying trust factors that are considered relevant
for trusting VAAL technology.
2.1 Procedure
Both interview groups were recruited in the social
network of the researchers and volunteered to take
part. Informed consent and permission to record was
obtained prior to the beginning. During the interview,
first, trust perceptions in the healthcare system were
explored. Secondly, AAL technologies with a focus
on video-based systems were explained. Next, trust
perceptions, requirements for trust, and benefits and
barriers about trusting VAAL technology were
discussed and participants were asked about how trust
changes and develops in health decisions. Lastly,
demographic variables (e.g., age, gender, health
status), but also, technical affinity, and experience
with medical technology were assessed.
2.2 Sample
Two focus groups were held on two occasions with
each five participants (50% female). Both interview
groups lasted roughly one hour, were audiotaped and
transcribed later on. The age range was 22 to 55 years
(M=30.2; SD=12.39). On a scale from 1 to 6,
technical affinity ranged at M=4.2 (SD=1.48). Seven
participants completed vocational training, two of
them are students. Four participants work in the
medical and four in a technical field. Eight of them
have experience with medical technology and two
have professional care experience. None of them
neither dependent on care by others nor have acute
diseases, but four of them reported chronic diseases.
2.3 Results
There were two key topics in users’ argumentation
lines that were relevant for trust in the VAAL
technology: data protection and information and
communication flow. Also, several trust-associated
criteria were found and are discussed below.
2.3.1 Data Protection
In this category, participants mostly referred to their
data being sealed from third parties. While they
reckoned that any technology can theoretically be
hacked, they did agree that in order for them to trust
the VAAL system, access to their data should have
the highest possible protection mechanism.
“Just as important is the issue of data protection,
because of course no one wants to be filmed in their
own four walls or have any sound recordings of
them published for whatever purpose. There are
enough crazy people who abuse data like that [...].
Trust in and Acceptance of Video-based AAL Technologies
127

So data protection is a very important point for
me.” (male, 24 y)
Data protection was also an important aspect for
trust in VAAL technologies. In addition, participants
felt more comfortable if they could decide who has
access to their data and how it is shared.
“In any case, data will be stored somehow if the
[VAAL system] is installed in my bedroom and if I
knew that someone could access it, of course I
wouldn't like it at all.” (male, 26 y)
The key component was knowledge about the
technology brought to the users in a truthful way.
According to them, the topic receives growing
interest over the last years (relevance). For this
factor, five items were constructed in the
questionnaire (data access and relevance).
2.3.2 Information and Communication Flow
This category was defined as the context in which the
technology was introduced, monitored, and used.
Participants mentioned that they would more likely
trust a VAAL system in their home if their physician
explained it to them well. Moreover, they felt more
secure in trusting if the person monitoring their
activity, e.g., in case of a fall, was someone with a
professional medical background. Conversely, they
would not trust a VAAL system if they felt that the
systems did not understand the severity of the
incident. Participants agreed that an overall
professional appearance mattered for their trust
development (professionalism).
“I would then, if something like that [a detected
incident]is checked again by another person, then I
would like to have the experienced person and not
the one who was maybe a gardener before and says,
"oh, let's have a look" and then sends someone off.
[...] It would be important to me that it is checked
again by competent people who have medical
experience.” (female, 52 y)
Another aspect of this was that participants
referred to understanding the mechanisms both
behind the actual technology, i.e. the source code, and
behind the bureaucracy, i.e. the financing of it. One
participant, working as a computer scientist, said that
his only condition for trust in VAAL technology
required an open-source code. Other participants
argued that this would not affect them as much seeing
as they lacked the technical know-how. They did,
agree that they wanted to be able to retrace how
VAAL systems end up with the user. Moreover, they
worried about financing these systems and who
would pay for the usage. They also referred to trusting
the systems more if the costs were covered by their
insurance companies.
“If the source code behind it is open source, i.e. if I
can see it, modify it and, as a computer scientist, I
can understand exactly what is happening there,
then for me trust is already given because I can
identify that for myself.” (male, 25 y)
“I have also written down transparency. So how
does the system work, how does it recognise that
there is a problem. Of course, people have to be
taught this, made aware of it, and older people in
particular understand it even less than we do
now..” (female, 24 y)
“Who finances this? Does the health insurance or
the long-term care insurance cover part of it, or do
you have to pay the whole cost yourself? Of course,
not everyone can afford that.” (male, 24 y)
Participants mentioned that information should not
only consider the technology, but also about the
processes and involved parties behind and around it
(information transparency). Participants also
agreed that whether or not the system worked well
was relevant to trusting it.
"I would also say competence, so it doesn't set off a
false alarm twenty times. That it works reliably and
doesn't notify someone when really only a pen fell
down. I mean once or twice is no problem, but if it's
all the time, I’m thinking 'Why do I have the thing
in the first place?'" (female, 22 y)
Regarding the technical competence of the
system, it was agreed that this was one of the most
important predictors of trust in the VAAL system.
Taken together, this factor consisted of
information transparency about and around the
technology, professionalism toward the potential
users, and technical competence. For this factor,
seven items were constructed in the questionnaire.
2.3.3 Associated Trust Criteria
This category pertained to individual perceptions of
benefits of VAAL systems bringing a surplus value to
their life, coded as health aspects. They also brought
up examples of having less strain on medical
personnel as well as more independence with the
VAAL system, i.e. relief in care.
“It [the VAAL system] would have to be a good
added value somehow. When I see that I am limited, I
would like to be able to try it out and be told that if I
ICT4AWE 2023 - 9th International Conference on Information and Communication Technologies for Ageing Well and e-Health
128

really fall down or hit the corner and hit my head and
can't press a button any more, that someone will
come. So if I could recognise an added value, that it
would make me more independent of other people, I
would trust it more.” (female, 52 y)
“So, of course, for the people who rely on the system,
it must be ensured that the system works well, because
normally you save a caregiver who is with you 24/7
and who watches over you, or relatives who make
sure that nothing happens to you, that you are well
and that you don't lie in your flat for two days and
can't move.” (male, 25 y)
Some aspects were highly individual, respecting
the need of empathy (i.e., emotional aspects) of the
system as a relevant trust considerations. Seven items
were constructed in the questionnaire (emotional
aspects, relief in care, and health aspects).
3 QUANTITATIVE APPROACH
On the basis of the focus group study, trust factors
were identified and classified in three categories.
Considering other variables in literature, i.e.,
acceptance measures, the following research
questions emerged:
RQ1: How are the identified trust factors evaluated?
RQ2: Which role do the associated trust criteria play?
RQ3: Are trust and associated trust criteria related to
the evaluations of VAAL technology?
RQ4: Which role do the trust categories play for the
evaluation of VAAL technology?
3.1 Methods
Data was collected by an online survey in summer
2022. Participants were recruited mostly via social
networks and the participation was voluntary.
3.1.1 Design of the Survey & Care Scenario
We first introduced participants to the main purpose
of the study, i.e. trust in, and acceptance of, VAAL
technology. We assured participants of a high
standard of data protection and informed that none of
their answers can be referred to them personally.
The online survey was divided into four parts.
First, participants indicated their demographic data
(i.e., age, gender, education, and professional
background). We also surveyed the respondents’
perceived health condition (1=”very bad” to 6=”very
good”), the health status as well as need for nursing
care. We also surveyed the usage of health-related
digital technologies as well as the purpose of the use.
In the third part, using a scenario-based method,
participants were introduced into the following
situation: “(…) You are 85 years old and live alone in
your house (...). Because you have several chronic
diseases, including hypertension and inflamed joints,
you take daily regulating medication. Recently, you
have been experiencing additional coordination
difficulties and you are increasingly unsteady on your
feet, especially at night. However, moving into a
retirement home is unthinkable for you, as you would
like to remain in your familiar surroundings. You
decide to install a VAAL system in your home.
Decisive for you is the technology for the fall
prevention, intervention, and the control of the daily
routine as well as the analysis of your mobility
behaviour. You are free to decide who you share the
data with (e.g., doctor, nursing service, relatives). If
changes in your health condition and activity status
are detected, these persons receive a notification.”
Thereafter, participants assessed the acceptance of the
use of assistive technologies for health reasons. They
responded to statements referring to benefits (e.g.,
sense of security, emergency notification) and
barriers for the use (e.g., invasion of privacy, concern
about surveillance). Respondents also evaluated
technology acceptance criteria according to TAM
(Davis, 1989), i.e., perceived ease of use, usefulness,
and the intention to use such technologies (7 items;
=.86) which were adapted to VAAL technology.
Finally, participants shared their opinions on trust
in VAAL technology. The trust items were related to
Data Protection (5 items; =.89), Information &
Communication Flow (7 items; =.69), and
Associated Trust Criteria (7 items; =.75). All items
were evaluated on six-point Likert scales.
3.1.2 Sample
After data cleaning, N=101 participants were
considered for the statistical analyses. The age of the
participants ranged from 18 to 83 (M=35.7 years,
SD=10); 64% of respondents were females. Most of
the respondents (50%) held a university degree, 22%
indicated general university entrance qualification
(22%). Of all participants, 12.9% had a vocational
baccalaureate diploma and 10.9% held a secondary
school degree as their highest educational
qualification, whereas 3% reported to hold a PhD.
The majority of the sample reported (very) good
health (58%) and 10% as mostly bad. Additionally,
42% respondents reported to suffer from a chronic
illness or physical impairment and 23% indicated to
Trust in and Acceptance of Video-based AAL Technologies
129
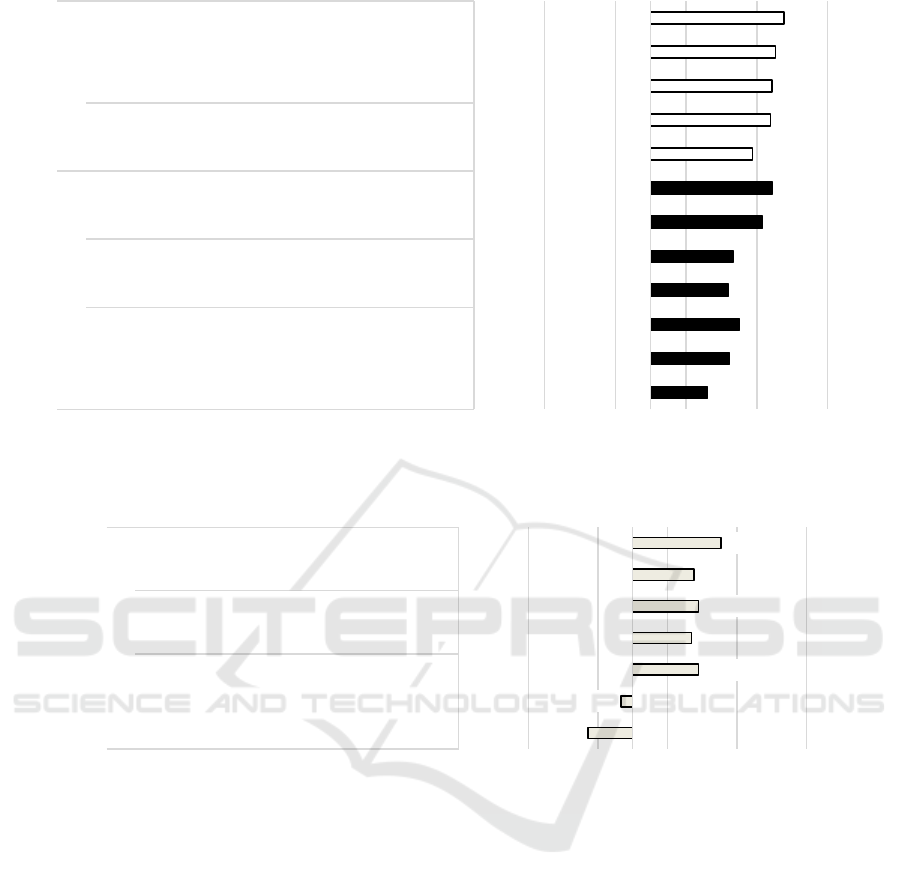
Figure 1: Evaluation of trust in VAAL technology (N = 101).
Figure 2: Evaluation of associated trust criteria (N = 101).
be affected by an acute physical or mental illness. 4%
needed care assistance (professional nursing or family
support). 53% of the respondents are actively using
health-assisting technologies (e.g., documentation of
vital parameters, monitoring of physical activities,
control of sleeping patterns, or weight control.)
3.2 Results
The quantitative results are described based on the
research questions. We used descriptive statistics for
the analysis of acceptance and trust statements
(M=means, SD=standard deviations). To examine
relations between the constructs we calculated
correlation analyses and examined the internal
consistency of the scales using Cronbach’s Alpha (
>.7). The significance level (p) was set at 5%.
3.2.1 Trust in Technology (RQ1)
Starting with Data Protection, all five items received
confirming evaluations. For the participants, it was of
major importance that they can decide “…who may
share…” (M=5.38; SD=.81), “…who sees…”
(M=5.26; SD=.91), and “…who may store…”
(M=5.21; SD=.92) their data. Further, they showed
strong agreements referring to the statements that
their “…privacy…” (M=5.08; SD=.95) and their
“…data security…” (M=4.94; SD=.97) are of highest
priority. Moving to the category Information &
Communication Flow, the results showed a more
differentiated evaluation pattern. Here, the statements
referring to Information Transparency (i.e., “…if I
4,30
4,61
4,75
4,60
4,66
5,08
5,22
4,94
5,19
5,21
5,26
5,38
123456
... if it is ready for the market.
... if it has been thoroughly researched.
... if it has a low error rate.
... if my doctor is well experienced with the technology.
... if my doctor has a good command of the technology.
... if I am well informed about it.
... if I can inform myself well about it.
... if my data security is of the highest priority.
... if my privacy is of highest priority.
... if I can decide who may store my data.
... if I can decide who sees my data.
... if I can decide who may share my data.
Technical
Competence
Professio-
nalism
Information
Transpa-
rency Relevance Data Access
Information & Communication Flow Data Protection
Evaluation (min = 1; max = 6)
rejection agreement
2,86
3,33
4,45
4,35
4,45
4,38
4,77
123456
... if it shows me warmth.
... if it shows me empathy.
... if it is individually tailored to me.
... if it relieves professional caregivers.
... if it relieves my relatives.
... if it improves my health situation.
... if it helps me with activities in everyday life.
Emotional
Aspects
Relief in
Care
Health
Aspects
Evaluation (min = 1; max = 6)
rejection agreement
Associated Trust Criteria
ICT4AWE 2023 - 9th International Conference on Information and Communication Technologies for Ageing Well and e-Health
130
can inform myself…” (M=5.22; SD=.84) and “…if I
am well informed…” (M=5.08; SD=.91) received the
highest agreement and thus represent relevant factors
for trust in VAAL technology. Further, the statements
referring to Professionalism received agreement, but
at a lower level: “…my doctor has a good command
of…” (M=4.66; SD=1.03) and “…my doctor is well
experienced with…” (M=4.60; SD=1.10) the
technology. Finally, also the items referring to
Technical Competence received agreeing
evaluations: here, participants confirmed statements
referring to “…a low error rate…” (M=4.75; SD=.89)
and “…it has been thoroughly researched” (M=4.61;
SD=1.10)), while the item “…if it is ready for the
market” (M=4.30; SD=1.15) received the lowest, but
still positive evaluations (Figure 1).
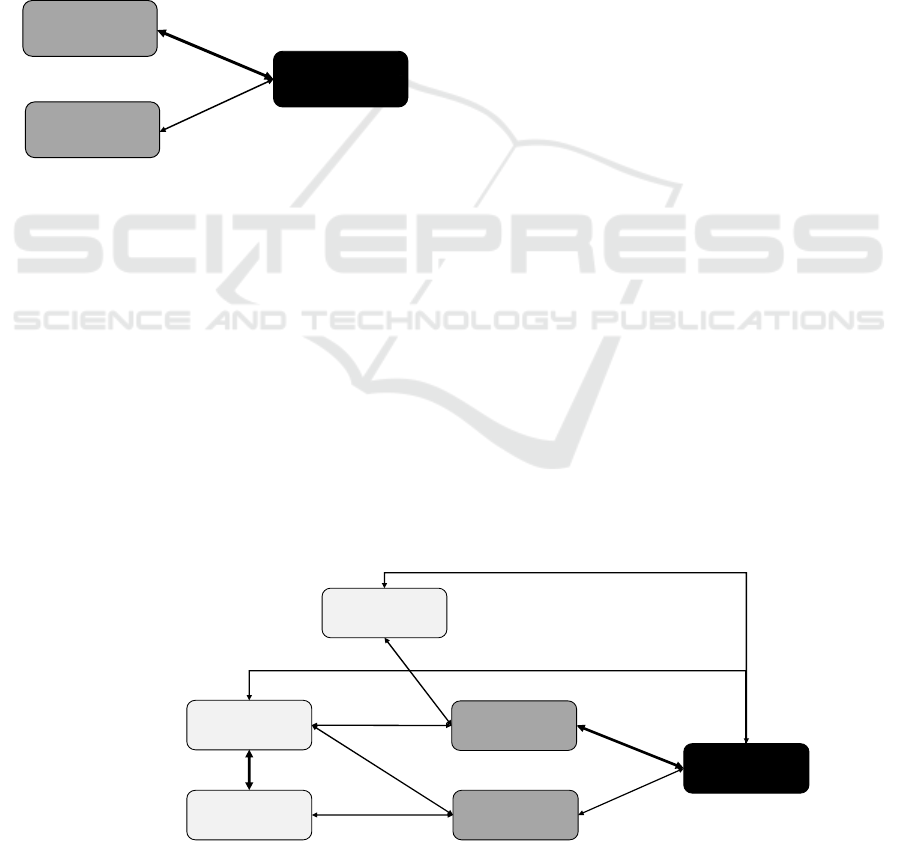
Figure 3: Correlations between technology perception and
acceptance (N = 101).
3.2.2 Associated Trust Criteria (RQ2)
The participants also assessed criteria relevant for
trust related to the interaction with VAAL technology
(7 items, Figure 2). Participants evaluated Health
Aspects to be relevant trust criteria when interacting
with VAAL technology. Here, help and support
“…with activities in everyday life” (M=4.77;
SD=1.03) as well as an improvement of the “…health
situation” (M=4.38; SD=1.22) received confirming
evaluations. Likewise, statements referring to Relief
in Care (i.e., relief of “relatives” (M=4.45; SD=1.13)
and “professional caregivers” (M=4.34; SD=1.18)
obtained approval. Regarding Emotional Aspects the
most divergent evaluation patterns were found: the
participants confirmed that if technology “…is
individually tailored” (M=4.45; SD=1.22)
represented a relevant trust criterion for them. In
contrast, the participants tended to reject showing
“empathy” (M=3.33; SD=1.56) and showing
“warmth” (M=2.86; SD=1.46) to be relevant factors
for trust in interacting with VAAL technology.
3.2.3 Relationships Between Technology
Perception & Acceptance (RQ3)
Regarding the relations between technology
perception and the acceptance of VAAL technology
(Figure 3), correlation analyses identified a strong
relationship between the Perceived Benefits and
Acceptance of VAAL technology (ρ=.552; p<.001)
and a moderate negative correlation between
Perceived Barriers and Acceptance (ρ=-.371;
p<.001). A correlation analysis was also run to
uncover relations between Information &
Communication Flow, Data Protection, and
Associated Trust Criteria (Figure 4). The results
showed a direct moderate relationship between
Associated Trust Criteria and the Acceptance of
VAAL technology (ρ=.379; p<.001). Further,
acceptance correlated with the Perceived Benefits of
VAAL technology as well (ρ=.263; p<.001).
However, Trust Criteria were not related with the
other trust constructs (n.s.). Information &
Communication Flow was related with the
Perceived Benefits (ρ=.331; p<.001) and the
Perceived Barriers (ρ=.295; p<.001). Also,
Information & Communication Flow and the
Acceptance of VAAL technology (ρ=.238; p<.001)
were related. Focusing on Data Protection, a
relationship with the Perceived Barriers (ρ=.461;
p<.001) was found. Data Protection was neither
related with the other trust constructs nor with the
Perceived Benefits and Acceptance of VAAL (n.s.).
Figure 4: Correlations between trust and technology acceptance (N = 101).
Acceptance of VAAL
(TAM, 7 Items)
Perceived Barriers
(8 Items)
Perceived Benefits
(7 Items)
.552**
-.371**
Acceptance of VAAL
(TAM, 7 Items)
Perceived Barriers
(8 Items)
Perceived Benefits
(7 Items)
.552**
-.371**
Data Protection
(5 Items)
Information &
Communication Flow
(7 Items)
Trust in AAL Technology
Trust related to
Interaction with
AAL Technology
.238*
.295**
.461**
.331**
.616**
Associated Trust
Criteria
(7 Items)
.379**
.263**
Trust in and Acceptance of Video-based AAL Technologies
131
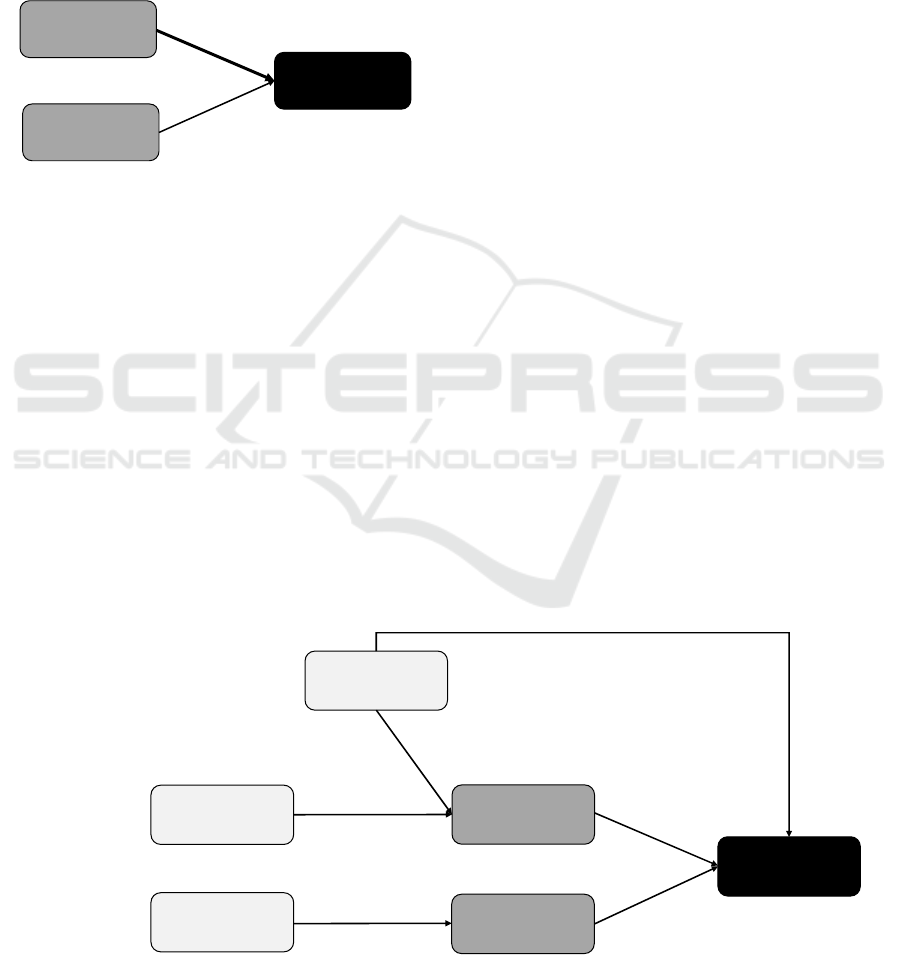
3.2.4 Role of Trust for Technology
Perception & Acceptance (RQ4)
To answer the underlying research question, linear
regression analyses were run to reveal the role the
technology perception for its acceptance (Figure 5).
39.6% variance of the Acceptance of VAAL
technology (adj. r
2
=.396; F(2,100)=33.77; p<.001)
can be explained by the Perceived Benefits (β=.490;
p<.001) and Perceived Barriers (β=-.350; p<.001).
Figure 5: Regression analysis: Role of technology
perception for acceptance (N = 101).
Next, the three identified trust constructs were
considered in regression analyses as well. Based on
the results of the correlation analysis, linear
regression analyses were conducted. Starting with the
Acceptance of VAAL technology, the regression
model predicted 47.9% (adj. r
2
=.479;
F(2,100)=23.96; p<.001) variance of Acceptance
based on Perceived Benefits (β=.364; p<.001),
Perceived Barriers (β=-.382; p<.001) and the trust
construct Associated Trust Criteria (β=.269;
p<.001). Information & Communication Flow
(β=.146; p=.082; n.s.) was not a predictor for the
Acceptance of VAAL technology. Based on the
results of the correlation analysis, the role of the trust
constructs for the perception of VAAL technology
was analysed (Figure 6: significant results).
For the Perceived Benefits, the regression model
predicts 13.1% variance (adj. r
2
=.131; F(2,100)=8.56;
p<.001) based on the two trust constructs
Information & Communication Flow (β=.260;
p<.01) and Associated Trust Criteria (β=.244;
p<.05). For the Perceived Barriers, the regression
model explained 18.5% variance (adj. r
2
=.185;
F(2,100)=12.32; p<.001) based on the trust construct
Data Protection (β=.391; p<.01). In contrast,
Information & Communication Flow (β=.073;
p=.54; n.s.) was not proven to be a significant
predictor of the perceived barriers of VAAL
technology.
4 DISCUSSION
In this study, a mixed-methods approach was used to
explore the perceptions of VAAL technology on trust
and acceptance.
From the interview study, two main themes
emerged, data protection and information and
communication flow. The category “Data
protection” included relevance and data access.
Information and communication flow consisted of
information transparency, professionalism, and
technical competence. These categories suggest an
interplay of aspects pertaining to the technology itself
and providers that are involved in its usage. In
addition, a separate category covered aspects of
associated trust criteria, consisting of health
aspects, relief in care, and emotional aspects. These
results suggest that there are multiple facets relevant
for trust in VAAL technology. In the subsequent
survey, four research questions in the context of trust
components in VAAL technology and its relation
to acceptance and, specifically, to the benefit and
Figure 6: Regression analysis: Role of trust for technology perception and acceptance (N = 101).
Acceptance of VAAL
(adj. r
2
=.396)
Perceived Barriers
(8 Items)
Perceived Benefits
(7 Items)
.490**
-.350**
Acceptance of VAAL
(adj. r
2
=.479)
Perceived Barriers
(adj. r
2
=.195)
Perceived Benefits
(adj. r
2
=.135)
Data Protection
(5 Items)
Information &
Communication Flow
(7 Items)
Trust in AAL Technology
Trust related to
Interaction with
AAL Technology
.397**
.260**
Associated Trust
Criteria
(7 Items)
.269**
.244**
.364**
-.382**
ICT4AWE 2023 - 9th International Conference on Information and Communication Technologies for Ageing Well and e-Health
132

barriers perceptions. The role that the trust
dimensions played in the perception and acceptance
of VAAL was identified with regression analyses.
The findings revealed multiple significant
relationships that are discussed in the next section.
Data protection in line with data access and
security was highlighted as extremely trust-relevant
by participants. Regarding information and
communication flow, information transparency was
the most important predictor of trust, followed by
professionalism and technical competence. This
means that there are clear rankings of which factors
are important for trusting VAAL. When it comes to
the question of which trust criteria are applied, there
were more diverse answers. While relief in care and
health aspects are undisputedly trust relevant,
emotional aspects received contradicting evaluations.
Apparently, associated trust criteria vary more among
participants and seem to be more individual.
In line with previous research on the acceptance of
AAL technologies (Peek et al., 2014; Offermann et
al., 2022), the evaluations of the technology are
significantly associated with the overall VAAL
acceptance. The higher benefits were perceived, the
higher was the resulting VAAL acceptance, and also,
higher assessments of perceived barriers lowered this
overall acceptance. Associated trust criteria directly
correlated with perceived benefits and overall
acceptance of VAAL technology. Moreover, data
protection significantly correlated with perceived
barriers, while information and communication flow
was significantly associated with perceived benefits.
Both of these relationships are also associated with
overall acceptance which signals an indirect effect of
trust in VAAL technology through perceptions of
VAAL technology.
With respect to the identified trust constructs, one
trust construct directly and two indirectly correlated
with the acceptance of VAAL technology. In line
with previous research (e.g., Jaschinski, 2018;
Wilkowska & Ziefle, 2019), these results confirm
trust to be a decisive factor for the acceptance of
medical assisting technologies. Beyond that, the
study identified different facets of trust suggesting a
network of influences relating to different constructs.
There are not many studies combining the knowledge
from qualitative and quantitative approaches as
outlined by a review from Peek et al. (2014).
Summarizing the approach and the methodology, we
can say that the mixed-methods design provides a
solid foundation for scientific practice, but also
allows for flexibility and opportunity to extract in-
depth knowledge.
When it comes to the limitations of the study, a
first issue regards the use of “only” scenario-based
evaluations of trust and the acceptance of VAAL. We
cannot exclude that scenario-evaluations differ from
the agreements or rejections and usage behaviours in
real-life contexts, representing the well-known gap
between (reported) attitudes and the (real) behaviour
(Ajzen & Fishbein, 1980). Future studies might
incorporate some sort of scenario comparison that
would allow for an experimental manipulation of the
targeted VAAL systems. It is further relevant to
outline how trust perceptions alter the evaluations of
acceptance as it represents one of the key predictors
of the perception and acceptance including the
intention to use VAAL technology.
Reflecting the sample of the quantitative study, the
size was relatively small, and not very representative
for the majority of people which are in need of care.
Thus, we cannot exclude a sample selection bias,
which reduces the generalizability of our findings to
the whole population of care.
5 CONCLUSIONS
This study used two methodological approaches in
order to investigate trust in VAAL technology and its
relationship with the acceptance of such technologies.
Several dimensions of trust revealed to be relevant in
understanding how people evaluate potential benefits
and barriers, but also, whether the users are more or
less likely to accept such technologies. When
designing these technologies, it becomes evident that
not only the technological features are important to
think about but also the context. Specifically the
interactions of the people involved, such as
technicians, physicians, and healthcare providers, are
important to prepare and honour. It is important to
remember that people still place their trust to a large
extent in humans and by extension, on their
recommendations of said technologies.
Understanding these mechanisms can help in
educating developers, computer scientists, healthcare
professionals and even policy makers about the
priorities of the potential users.
ACKNOWLEDGEMENTS
Authors thank Verena Grouls for research support.
This project has received funding from the European
Union’s Horizon 2020 research and innovation
Trust in and Acceptance of Video-based AAL Technologies
133

programme under the Marie Skłodowska-Curie grant
agreement No 861091.
REFERENCES
Ajzen I, Fishbein M. Understanding Attitudes and
Predicting Social Behavior. 1st ed. Englewood Cliffs,
NJ: Prentice-Hall (1980).
Alshammari, S. H., Rosli, M. S. (2020). A review of
technology acceptance models and theories. Innovative
Teaching and Learning Journal (ITLJ), 4(2), 12-22.
Beier, G. (1999). Kontrollüberzeugungen im Umgang mit
Technik [Locus of control when interacting with
technology]. Report Psychologie, 24(9):684–693.
Bova, C., Fennie, K. P., Watrous, E., Dieckhaus, K., &
Williams, A. B. (2006). The health care relationship
(HCR) trust scale: Development and psychometric
evaluation. Res Nurs Health, 29(5), 477-488.
Climent-Perez, P., Spinsante, S., Mihailidis, A., & Florez-
Revuelta, F. (2020). A review on video-based active
and assisted living technologies for automated
lifelogging. Expert Systems with Applications, 139.
Davis, F. D., 1989. Perceived Usefulness, Perceived Ease
of Use, and User Acceptance of Information
Technology. MIS Quarterly, 13(3), 319–340.
Erquicia, J., Valls, L., Barja, A., Gil, S., Miquel, J., Leal-
Blanquet, J., ... & Vega, D. (2020). Emotional impact
of the Covid-19 pandemic on healthcare workers in one
of the most important infection outbreaks in Europe.
Medicina Clínica,, 155(10), 434-440.
Jaschinski, C. (2018). Independent Aging with the Help of
Smart Technology: Investigating the Acceptance of
Ambient Assisted Living Technologies. Dissertation.
University of Twente.
Jaschinski, C., & Allouch, S. B. (2015). An extended view
on benefits and barriers of ambient assisted living
solutions. International Journal on Advances in Life
Sciences 7(1-2). 40-53.
Jaschinski, C., Allouch, S. B., Peters, O., Cachucho, R., &
Van Dijk, J. A. (2021). Acceptance of technologies
foraging in place: A conceptual model. Journal of
medical Internet research, 23(3),
McKnight, D. H., & Chervany, N. L. (2001). What trust
means in e-commerce customer relationships: An
interdisciplinary conceptual typology. International
Journal of Electronic Commerce, 6(2), 35-59.
Michel, J. P., & Ecarnot, F. (2020). The shortage of skilled
workers in Europe: Its impact on geriatric medicine.
European Geriatric Medicine, 11(3), 345-347.
Offermann-van Heek, J., Schomakers, E. M., & Ziefle, M.
(2019). Bare necessities? How the need for care
modulates the acceptance of ambient assisted living
technologies. International Journal of Medical
Informatics, 127, 147-156.
Offermann, J., Wilkowska, W., Ziefle, M. (2022). Interplay
of Perceptions of Aging, Care, and Technology
Acceptance in Older Age. International Journal of
Human–Computer Interaction, 1-13.
Offermann-van Heek, J., & Ziefle, M. (2019). Nothing else
matters! Trade-offs between perceived benefits and
barriers of AAL technology usage. Frontiers in Public
Health, 7, 134.
Peek, S. T., Wouters, E. J., Van Hoof, J., Luijkx, K. G.,
Boeije, H. R., & Vrijhoef, H. J. (2014). Factors
influencing acceptance of technology for aging in
place: a systematic review. International journal of
medical informatics, 83(4), 235-248.
Qiao, Y., Asan, O., & Montague, E. (2015). Factors
associated with patient trust in electronic health records
used in primary care settings. Health Policy and
Technology, 4(4), 357-363.
Rahimi, B., Nadri, H., Afshar, H. L., Timpka, T., (2018). A
systematic review of the technology acceptance model
in health informatics. Applied clinical informatics, 9(3),
Schomakers, E. M., Biermann, H., & Ziefle, M. (2021).
Users’ Preferences for Smart Home Automation–
Investigating Aspects of Privacy and Trust. Telematics
and Informatics, 64, 101689.
Steinke, F., Fritsch, T., Brem, D., & Simonsen, S. (2012).
Requirement of AAL systems: Older persons' trust in
sensors and characteristics of AAL technologies. In
Proceedings of the 5th International Conference on
Pervasive Technologies Related to Assistive
Environments (pp. 1-6).
Wahezi, S. E., Kohan, L. R., Spektor, B., Brancolini, S.,
Emerick, T., Fronterhouse, J. M., ... & Kaye, A. D.
(2021). Telemedicine and current clinical practice
trends in the COVID-19 pandemic. Best Practice &
Research Clinical Anaesthesiology, 35(3), 307-319.
Wilkowska, W., Offermann-van Heek, J., Florez-Revuelta,
F., & Ziefle, M. (2021). Video cameras for lifelogging
at home: Preferred visualization modes, acceptance,
and privacy perceptions among german and turkish
participants. International Journal of Human–
Computer Interaction 37(15), 1436-1454.
Wilkowska, W., Ziefle, M. (2019). Determinants of Trust
in Acceptance of Medical Assistive Technologies. In:
Bamidis, P., Ziefle, M., Maciaszek, L. (eds). ICT4AWE
2018. Communications in Computer and Information
Science, vol 982. Springer, Cham.
Wilkowska, W., Ziefle, M., & Himmel, S. (2015).
Perceptions of personal privacy in smart home
technologies: Do user assessments vary depending on
the research method?. In International Conference on
Human Aspects of Information Security, Privacy, and
Trust (pp. 592-603). Springer, Cham.
Xu, J., Le, K., Deitermann, A., & Montague, E. (2014).
How different types of users develop trust in
technology: A qualitative analysis of the antecedents of
active and passive user trust in a shared technology.
Applied Ergonomics, 45(6), 1495-1503.
ICT4AWE 2023 - 9th International Conference on Information and Communication Technologies for Ageing Well and e-Health
134
