
Classification of Respiratory Diseases Using the NAO Robot
Rafael Andrade Rodriguez, Jireh Ferroa-Guzman and Willy Ugarte
a
Universidad Peruana de Ciencias Aplicadas, Lima, Peru
Keywords:
Classification, NLP, NAO, Respiratory.
Abstract:
This work proposes an interface that connects the NAO robot with a development environment in Azure Ma-
chine Learning Classic for the prediction of respiratory diseases. The developed code uses Machine Learning
algorithms trained for the prediction of diseases and fatal symptoms in order to provide the user with a scope
of his health status and the possible conditions associated with his age, sex, symptoms and severity. During
this process, a brief discard of COVID-19 is made with the symptoms obtained, which indicates if they cor-
respond to those of this disease. Additionally, we offer a friendly interaction with the NAO robot to facilitate
the exchange of information and, at the end of the algorithm flow, it is always suggested to use a professional
doctor to provide users with more details about their current status based on the overall results obtained. The
tests carried out on the work show that it is possible to speed up the time of care in medical care centers in Peru
through the Nao Robot. Additionally, it has been possible to predict respiratory diseases, which also helps the
doctor to have a notion of the patient prognosis.
1 INTRODUCTION
On March 11, 2020, the World Health Organisation
(WHO) declared SARS-Cov-2 a pandemic, due to
its far-reaching, affecting millions of people in sev-
eral countries around the world
1
. In Peru, COVID-
19 was officially reported on March 6, 2020; Faced
with this, the Peruvian state declared on March 15 of
the same year, a state of Emergency, considering the
speed of progression of the disease and ruled manda-
tory quarantine at the national level (Miyahira, 2020).
On the 25th of the same month, the Peruvian Gov-
ernment established the measures that would lead cit-
izens towards a new social coexistence and the state
of emergency was extended due to the serious circum-
stances that affected the nation as a result of SARS-
Cov-2 (Barrutia-Barreto et al., 2021)
Despite the measures taken, the numbers of deaths
in Peru continued to grow. For the month of August
2020, Peru reached 613,378 infections, which made
it the sixth country with the most reported cases. At
that time, we reached 28 thousand deaths due to the
pandemic with a mortality rate of 85.8 per thousand
inhabitants
2
. During this period, there was evidence
a
https://orcid.org/0000-0002-7510-618X
1
WHO - https://covid19.who.int/
2
“Peru has the world’s highest COVID death rate.
Here’s why” - NPR - https://n.pr/3EBRukh
of a deficient response by the public health system of
Peru, taking into account the number of deaths over
the number of infections (Gianella et al., 2021). How-
ever, this deficiency did not begin with the COVID-19
pandemic.
In the public sector of the Peruvian health system,
the government offers health services to uninsured
people in exchange for the payment of a fee through
the Integral Health System (SIS), with EsSalud be-
ing the entity that offers the services (Gianella et al.,
2021). During previous years, complaints and even
denunciations have been expressed by patients who
have health insurance within this center. Problems
such as speed of care, lack of medication and medical
malpractice are part of the large list of claims against
EsSalud. For example, in 2016, more than 111,000
claims for medical malpractice were filed in EsSalud
for poor provision of services, which shows the dis-
satisfaction of users about the care provided
3
.
According to the National Institute of Statistics
and Informatics (INEI) of Peru, 25% of patients
treated at EsSalud have to wait between 15 to 30 days
to be able to schedule a simple medical consultation
3
,
while for surgical interventions, the time between the
date of programming and the date of intervention rises
to 2 months. On the other hand, for outpatient med-
3
“Complaints for lack of medical care and negligence
persist in EsSalud” (in spanish) - https://bit.ly/2XAjVby
940
Andrade Rodriguez, R., Ferroa-Guzman, J. and Ugarte, W.
Classification of Respiratory Diseases Using the NAO Robot.
DOI: 10.5220/0011782700003411
In Proceedings of the 12th International Conference on Pattern Recognition Applications and Methods (ICPRAM 2023), pages 940-947
ISBN: 978-989-758-626-2; ISSN: 2184-4313
Copyright
c
2023 by SCITEPRESS – Science and Technology Publications, Lda. Under CC license (CC BY-NC-ND 4.0)

ical care, the waiting time in a Peruvian clinic is 42
minutes on average, a figure that for Essalud rises to
81 minutes. Therefore, many people are discouraged
from carrying out medical consultations in the public
health sector, also considering other problems such as
the level of distrust in medical personnel that still pre-
vails to date. Synthesizing the main problems during
consultations, it has been identified: insufficient at-
tention time, high workload, patient anxiety or fear,
fear of physical and verbal abuse, unrealistic expecta-
tions of patients, fear of demands, patient resistance to
change and lack of training in this area. For all these
reasons, there are still barriers between doctors and
patients, which hinder the efficient exchange of infor-
mation, which can have an impact on misdiagnoses,
which currently cover 11% of cases in the country
4
.
Within this context, it is important to consider
these shortcomings in the health system, maintain an
adequate doctor-patient relationship through patient
training and information, encourage health prevention
and promote adherence to treatments. For this, Peru-
vians need a source of information that serves as an
assistant and allows them to foresee the presence of
certain diseases based on probabilities. To meet these
needs, an interface capable of delivering results with
suggested illnesses and feedback on symptom sever-
ity to patients was developed through brief interaction
with the robotic assistant, NAO. The algorithm that is
handled in the interface was rigorously selected after
performing a comparative analysis with other classi-
fication algorithms prioritizing accuracy and avoiding
overtraining.
This paper is organized as follows. Therefor, in
Section 2, an analysis of the state of the art consid-
ered for this work will be made. Section 3, first, in-
troduces the technologies used for the development of
the proposed solution.
Finally, Section 4 shows the experimental proto-
col, the results obtained, and the discussion. To con-
clude with Section 5
2 RELATED WORKS
The work of Fale (Fale and Gital, 2022) proposes
a hybrid of Mamdani type and Fuzzy Sugeno type
models by means of a fuzzy controller, follow a se-
quence of three steps: fuzzification; inference; and
defuzzification. Yuan’s work (Rozo et al., 2021) fo-
cuses on qualitatively detecting normal breathing and
Cheyne-Stokes breathing in patients with non-contact
4
“Medical error rate is around 11% in hospitals
and technology could change this figure” - https://bit.ly/
3V0PWHi
heart failure using orthogonal frequency division and
multiplexing technology (OFDM). On the other hand,
Mubashir’s work (Rehman et al., 2021) develops a
machine learning (ML) classification model that is in-
telligent, secure, reliable and contributes to current
health systems by exploiting several Machine Learn-
ing algorithms to classify eight respiratory anomalies:
eupnea, bradypnea, tachypnea, Biot, sighs, Kussmaul,
Cheyne-Stokes and central sleep apnea (CSA). All
these works are oriented to respiratory diseases, just
like ours. However, we use Multiclass Decision Jun-
gle and Two Class Decision Forest as algorithms for
prediction, unlike the other methods mentioned.
In (Romero-Garc
´
ıa et al., 2021) evaluates the per-
formance of symptoms as a diagnostic tool for SARS-
CoV-2 infection using Mantel-Haenszel logistic re-
gression. In this area, in (Arslan, 2021), the authors
develop a prediction method based on the similarity of
the genome of human SARS-CoV-2 and a coronavirus
similar to bat SARS-CoV to predict this same disease.
Also, in (Brunese et al., 2020), the authors develop a
supervised machine learning model that discriminates
between COVID-19 and other lung diseases. These
three works are based on the detection or prediction
of COVID-19 and obtained the accuracies of 83.45%,
99.8% and 96.5% respectively according to the tests
performed. Unlike them, our work simply performs
a quick discard considering the symptoms mentioned
by the user, without additional analysis.
In (Yoon et al., 2019), a deep learning system is
developed using a recurrent neural network capable
of encoding and deciphering people’s postures in im-
ages and videos, and then being able to imitate them.
Similar to this, in (Filippini et al., 2021), the authors
design a CNN-based FER (Facial Expression Recog-
nition) model for facial expression recognition in real-
life situations. Both works handle neural networks
and employ computer vision, unlike us, who mainly
use the Audio service of the NAOqi library.
In (Burns et al., 2022), the authors attempt to
prove that the walking speed of the humanoid NAO
can be improved without modifying its physical con-
figuration using decision trees and the ANN and
NAive Bayes models. On the other hand, in (Hoff-
mann et al., 2021), the authors develop a process
model with the components that are required to pass
the recognition test in front of a mirror. Regarding
our work, instead of working with decision trees, we
manage multiple DAG’s for disease prediction.
Classification of Respiratory Diseases Using the NAO Robot
941

3 CLASSIFICATION TASK
3.1 Preliminary Concepts
3.1.1 Human-Robot Interaction
The study of human-robot interactions (also called
HRI) represents a multidisciplinary field with contri-
butions from human-computer interaction, artificial
intelligence, robotics, natural language understand-
ing, design, and social sciences.
1. Robot NAO: Nao is a programmable and au-
tonomous humanoid robot developed by Alde-
baran Robotics. Nao is 4.3 kg in weight and has
a height of 58 centimeters. It is relatively light
and small, which makes it an ideal solution to
live with humans. Thanks to its prehensile finger
hands with tactile sensors, it is capable of lifting
objects of up to 600 grams. The different elements
of NAO, such as sensors, motors and software are
controlled by a powerful operating system called
NAOqi. All versions have an inertial measure-
ment unit with gyrometer, accelerometer and 4
ultrasound sensors, which provide the robot with
stability, while the leg versions include 8 force de-
tection resistors and 2 stops. The collaborative
robot includes 4 microphones, 2 speakers and 2
high-definition cameras. Also, it presents inter-
esting attributes and features such as a 25-degree
movement, 2 HD cameras, 2 speakers, Wi-fi con-
nection and an Intel Atom 1.6 GHz processor
5
.
2. The robot has functionalities that the programmer
can use as resources to automate processes with
the NAO robot. In the interaction with the NAO
robot, it is necessary to have a copy connected
to a local IP of the home so that it can be con-
nected to a remote computer in which it is going
to be programmed. This process of connecting to
a network and synchronizing in the working envi-
ronment of the Python programming language is
understood as “AlProxy”.
3. Naoqi: NAOqi is an interpreter between the Nao
robot and Python programming that will allow us
to interact with the robot. It consists of a frame-
work that will allow to use the functionalities of
the robot and implement the Machine Learning al-
gorithm to the robot to process the received input
data.
• “ALProxy” command: This command is used
as a means of communication between the pro-
5
“Programming NAO robot with Python” - Softbank
Robotics Europe (2015) -https://www.youtube.com/watch?
v=iAeis7j5LmE
gramming interface and the NAO robot. Previ-
ously, the robot must be connected to the inter-
net so that it can be recognized by the program.
Its syntax consists of: an action to perform, the
IP address where the robot is connected and the
port where the NAO robot is connected.
• Action Name: NAOqi’s own SDK comes
with pre-programmed actions. All these pre-
programmed actions can help the program-
mer perform processes or automations with
the robot. From simple commands like say-
ing something by voice to taking pictures
and interpreting symbols. According to Soft-
Bank Robotics (2022), these are separated by
groups
5
.
(a) NAOQi core: Contains a list of functions that
allows you to interact with the NAO robot to
perform complex actions.
(b) NAOqi sensors and led: Contains the action
codes of the NAO robot with which it can in-
teract and program.
(c) NaoQi vision: Contains a library responsible
for managing video cameras, stereo cameras
and 2D cameras of the NAOqi robot.
(d) NAOqi Audio: Contains modules for record-
ing and playing audio, as well as for handling
the robot’s language.
(e) NAOqi people perception: Contains com-
mands are used to analyze human behavior
around the robot.
(f) Naoqi Motion: Contains the commands that
allow the movement of the NAO robot.
From these functionalities of the NAOqi library,
we take advantage of ALSpeechRecognition, a
NAOqi Audio command, which allows to inter-
pret the sounds or words that a human can make.
In this way, the NAO robot is able to capture the
input data necessary for symptom processing and
also, the user information that will be used to send
the results.
3.1.2 Basic Notions About Health and
Symptomatology
1. Symptomatology: Set of symptoms characteristic
of a given disease or grouping of symptoms that
occur in a patient.
2. Comorbidity: The presence of two or more asso-
ciated disorders or diseases in the same person,
occurring at the same time or one after the other
6
.
6
Co-morbidities - WHO - https://www.who.int/
southeastasia/activities/co-morbidities-tb
ICPRAM 2023 - 12th International Conference on Pattern Recognition Applications and Methods
942
3. Interconsultation: Occurs when a doctor refers the
patient to another specialist doctor to handle com-
munication with different areas of expertise.
3.1.3 Classification Models
1. Multiclass Decision Jungle: Represents an exten-
sion or modification of the Decision Forest algo-
rithm. However, this consists of a set of acyclic
graphs that are driven by a decision (DAG). Mu-
ticlass Decision Jungle has the following advan-
tages:
(a) By allowing tree branches to merge, a deci-
sion DAG typically takes up less memory space
and has better generalization performance than
a decision tree, albeit at the cost of somewhat
longer training time.
(b) Decision jungles are nonparametric models that
can represent nonlinear decision boundaries.
(c) They perform a selection and classification of
built-in features and are resistant in the pres-
ence of noisy features.
The algorithm has many advantages in terms of
machine learning and has had considerable suc-
cess when testing. However, this also has a fun-
damental limitation that, with a lot of data, the
number of nodes in decision trees will grow ex-
ponentially with depth, limiting their use to only
certain platforms that can support this amount of
processing.
Figure 1: DAG visualization (Shotton et al., 2013).
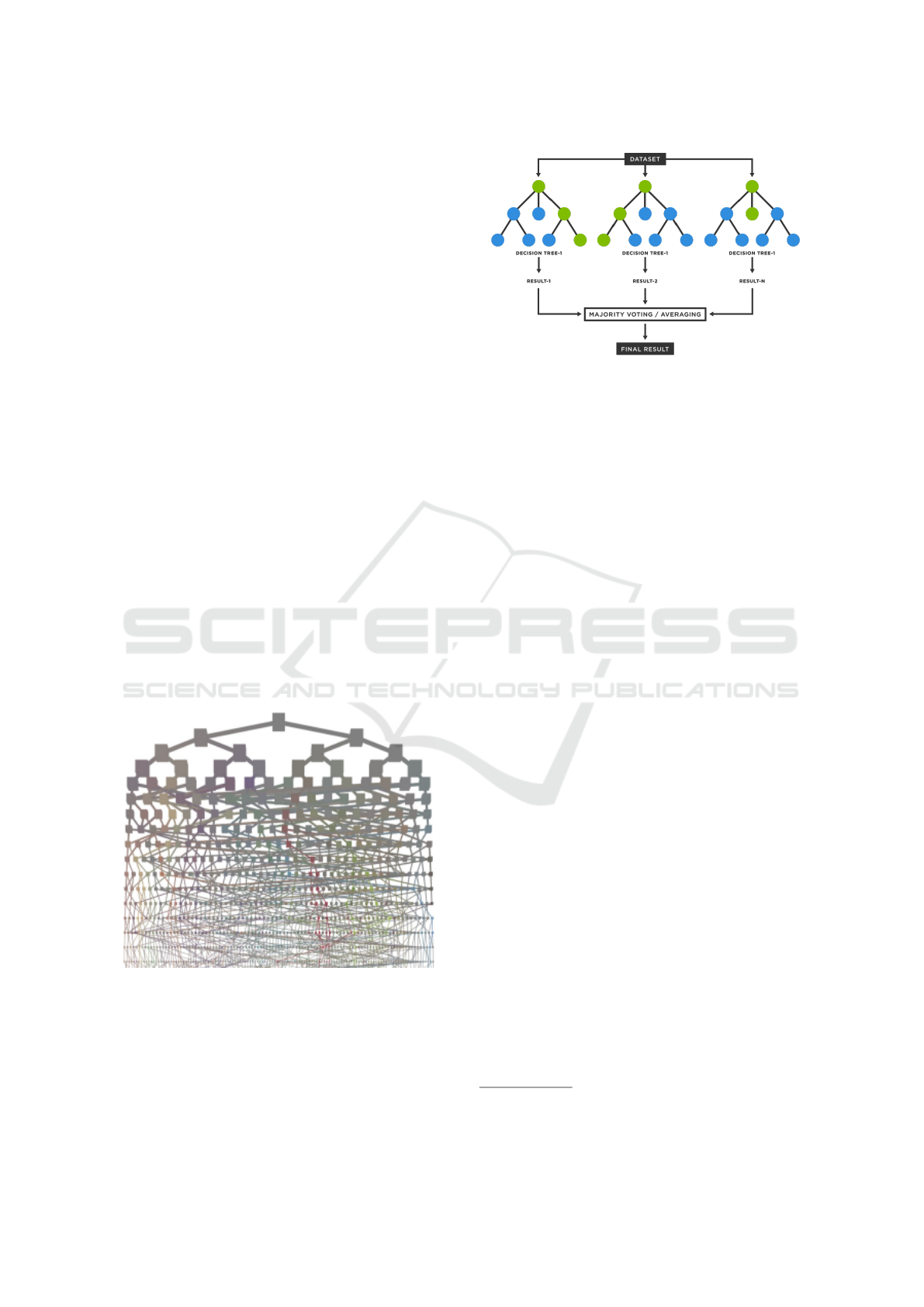
2. Two Class Decision Forest: A decision forest de-
scribes a model made of multiple decision trees.
The prediction of a decision forest is the aggrega-
tion of the predictions of each decision tree.
Figure 2: Decision Forest flow. (H
¨
ansch, 2021).
3.2 Method
Our main contribution is the prediction of diseases
based on symptoms using a Multiclass Decision Jun-
gle. This algorithm is powered by a dataset published
on the Kaggle platform by American Health Info
7
.
For its adaptation in the Azure environment, we have
made some improvements such as data normaliza-
tion; That is, those symptoms that were written dif-
ferently, but corresponded to the same, were unified
into one. Also, because the dataset was unbalanced;
in other words, with unrepresented classes, we aggre-
gate records with missing severities (high, medium,
or low) for each symptom of each disease; so that the
code can predict diseases with any level of severity of
their symptoms. To exemplify this idea, if there are
no records of people with disease: asthma and symp-
tom: chest tightness, specifically with severity: low,
it is assumed that no user with these last two charac-
teristics can have asthma.
From the dataset handled, we use “Diseases”, as a
column to predict, and the columns of: “symptom”,
“sex”, “age” and “severity” as predictive variables.
We also use this dataset with an additional column of
Mortality, which indicates whether a symptom con-
sidering age and severity, can become fatal. To do
this, the code sends the data to another development
environment and tells the user if it detects several
deadly symptoms.
On the Azure Machine Learning Classic plat-
form, we first load the normalized dataset and sec-
tion the columns relevant to our algorithm. Then,
we use 88% of the dataset for processing and 12%
for testing. Records for both proportions are random.
Then, we generate the training model, which connects
with the multiclass decision jungle algorithm. This
has at the beginning of 16 DAG’s (directed acyclic
graphs), with a maximum depth of 156 DAG’s and
7
https://www.kaggle.com/datasets/abbotpatcher/
respiratory-symptoms-and-treatment
Classification of Respiratory Diseases Using the NAO Robot
943
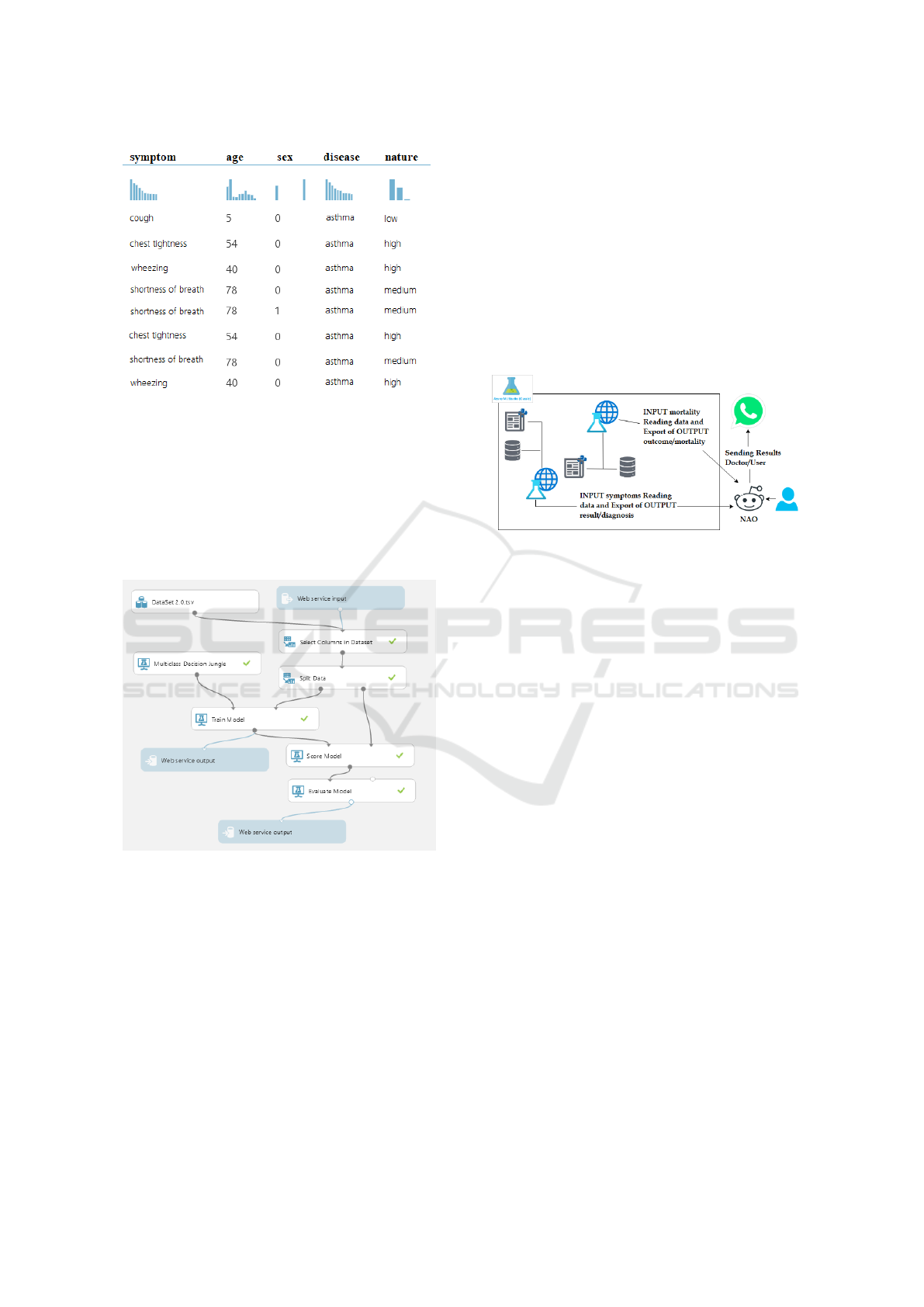
Figure 3: Image of the updated Dataset.
width of 140 DAG’s. Subsequently, we create the
Score Model, which contains the percentages calcu-
lated with each test record selected for the testing pro-
cess and is part of the basis for knowing the accu-
racy of the algorithm in general. Finally, the Evaluate
model shows us the metrics calculated on the same
platform and we connect the input and output services
to make our architecture functional.
Figure 4: Architecture in Azure Machine Learning.
According to the flow, in the first instance, the user
indicates his personal data to the robot: Name, Age,
Sex, Symptoms and Severities; for the latter variables,
an iterative flow is traversed that detects when there
are 3 or more symptoms of COVID-19. In case the
detection is positive, the user is consulted if a discard
test was done; If so, continue with the code and other-
wise, the flow is cut off indicating that a test is carried
out as soon as possible. After completion of symp-
tom and mortality uptake; The NAO robot sends the
captured symptoms to the first development environ-
ment in Azure, which will process one by one and
save the individual results, to then be averaged and
thus, calculate those diseases with more probability.
After this process, it connects with the second devel-
opmental environment and comments are issued re-
garding the mortality of the symptoms. Finally, the
user is queried for their WhatsApp number and, after
having captured it, the overall results are sent. During
the entire process of connection to the development
environments, it is necessary to execute a reconnec-
tion script with the NAO robot to connect to a net-
work that has access to the internet; which is required
to receive results from Azure. Subsequently, we link
again with the robot so that it continues its flow.
Figure 5: Connection Flow with the environments.
This developed flow has allowed us to speed up
and have a shorter attention time, thanks to the fluid
conversation facilitated by the humanoid robot. Addi-
tionally, during the development and tests carried out,
we have been able to observe certain characteristics of
the robot that allow the correct reception of the input
data. These are as follows:
1. When talking to the NAO: We have to position
ourselves at a considerable height (higher than
that of the robot), because the microphones are
located on the upper front of the robot (Fig. 1)
2. Response time: When the robot makes a query,
you have to wait approximately 3 seconds to re-
spond to it.
3. Detection of the person: As seen in Fig. 1, the
sensors are located in the chest of the robot, which
means that it will detect the person in front of it,
therefore, it is recommended that, when talking to
the robot, the patient is in front of it, Not on the
sides.
Likewise, the symptoms have been classified in
order to simplify the process of receiving input data
so that the user can mention those symptoms recorded
that fit their own during the consultation. The classi-
fications are as follows:
1. Cough Related
2. Related to breathing
3. Pains
ICPRAM 2023 - 12th International Conference on Pattern Recognition Applications and Methods
944

4. Weight loss
5. Fatigue related
6. General discomfort
On the limitations and scope of our proposal, we
have the following:
1. Our model recognizes a total of 65 symptoms and
18 different respiratory diseases.
2. Our model is limited to respiratory diseases.
3. We must consider a waiting time to be able to give
an answer to each question asked by the robot.
This time is 5 seconds.
4. The flow does not include adding new symptoms
or diseases (conditioned by the dataset).
The use of the NAO robot for our proposal, unlike
any other technological solution, is justified by rely-
ing on one of the causes of our main problem: the
level of distrust that exists towards medical person-
nel, which hinders an efficient exchange of informa-
tion with patients. Faced with this, a study entitled
“Making eye contact with a robot: Psychophysiologi-
cal responses to eye contact with a human and with
a humanoid robot” concludes, after an experimen-
tal process, that in human-robot and human-human
condition, eye contact in front of the deviated gaze
caused a greater conductance of the skin, responses
associated with positive affect and deceleration of the
heart, that index attention allocation. In conclusion,
eye contact provokes affective and attentional reac-
tions when shared with a humanoid robot as well as
with another human.
4 EXPERIMENTATION
In this section, we present the experimental analysis
to demonstrate the feasibility of the proposal. We will
outline our experimental process and explain all the
considerations that were fundamental to obtain the fi-
nal results.
4.1 Experimental Protocol
To carry out the experiments, various tools have been
used, both hardware and software. First, the NAO v.6
humanoid robot enabled interaction with users as well
as data capture in the experimental process. The pro-
gramming language of Python 2.7 and 3.10 has been
handled, along with the Naoqi framework. Regarding
our algorithms in Azure Machine Learning classic,
we have made use of the web service. On the other
hand, the computer that was responsible for execut-
ing the developed code has an AMD Ryzen 5 2500U
processor with 2.00 GHz and 24.0 GB of RAM.
Within our experimentation we have also tested
with different algorithms to be able to know which of
them would be better to be able to predict the diseases
that we are going to enter. Among these algorithms
are the Multiclass Decision Jungle, Multiclass Deci-
sion Forest, Multiclass Logitic Regression and Multi-
class Neural Network. Additionally, these algorithms
have internal parameters that we have been modify-
ing in order to find the most appropriate model for the
prediction we want. In Table 1, we can find the re-
sults of the algorithms with the default values given
by the Azure Machine Learning Classic; and in Ta-
ble 1b you can find the results of the same algorithms
with the modified values. In Table 1c you can find
the experimentation that has been carried out for the
part of the algorithm that predicts the mortality of the
disease.
Our code is currently available at https://github.
com/gareia/Dr Nao.git.
4.2 Results
In this section, we will detail the results of the tests
performed and show some videos in which the work-
flow and each functionality mentioned below are vi-
sualized. The complete flow of our proposal can be
visualized in our video
8
.
Reception Input Data. The reception of name is
conditioned by a dataset, which initially overloaded
the vocabulary allowed by Naoqi. Other input values
such as Age and Sex are received without major prob-
lems; However, in the symptoms section, at times the
mentioned symptom is not recognized. Here, several
factors such as ambient noise or similarity in the name
of different symptoms can influence.
Connection to Development Environment. The
API Key and URL generated by Azure Machine
Learning classic allow us to connect with the devel-
opment environment. This is functional at all times
and the disconnection/reconnection script with NAO,
as well as the network with defined internet access,
works properly without errors.
Discard COVID-19: The flow is properly met. When
symptoms related to COVID-19 are detected, the user
is asked if the COVID-19 test was performed to end
the flow in case of responding negatively.
Reception and Sending of Results. It was possible
to send results through a WhatsApp account linked
to the selected browser. It is recommended that it is
8
https://youtu.be/sw7LpUie2TA
Classification of Respiratory Diseases Using the NAO Robot
945
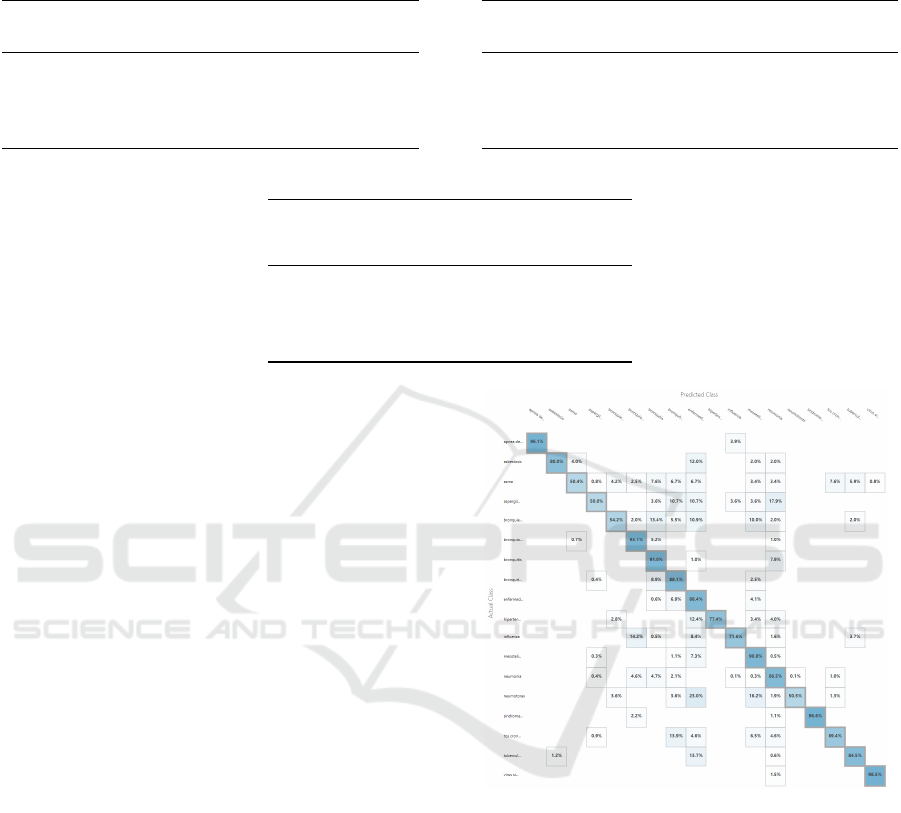
Table 1: Machine Learning Algorithms Metrics Charts.
(a) Default Values.
Multiclass
Decision
Jungle
Multiclass
Decision
Forest
Multiclass
Logitic
Regression
Multiclass
Neural
Network
Overall accuracy .820627 .805957 .914870 .907313
Average accuracy .980070 .978440 .990541 .989701
Micro-averaged precision .820627 .805957 .914870 .907313
Macro-averaged precision .861564 .838173 .934235 .918068
Micro-averaged recall .820627 .805957 .914870 .918068
Macro-averaged recall .760552 .768652 .896562 .903236
(b) Modified values.
Multiclass
Decision
Jungle
Multiclass
Decision
Forest
Multiclass
Logitic
Regression
Multiclass
Neural
Network
Overall accuracy .817070 .805957 .918649 .907535
Average accuracy .979674 .978440 .990961 .989726
Micro-averaged precision .817070 .805957 .918649 .907535
Macro-averaged precision .862696 .838173 .937841 .918490
Micro-averaged recall ,817070 .805957 .918649 .907535
Macro-averaged recall .755444 .768652 .899862 .901638
(c) Mortality prediction models.
Two Class
Bayes
Point
Machine
Two Class
Averaged
Perceptron
Two Class
Boosted
Decision
Tree
Two Class
Decision
Forest
Accuracy .962 .273 .273 .988
Precision .951 .273 .273 .984
Recall precision .907 1.000 1.000 .972
F1 Score .929 .430 .430 .978
Threshold .500 .500 .500 .500
AUC .992 .164 .000 .999
already open and that it has synchronized correctly to
avoid unnecessary delays.
According to Tables 1 and 1b, and an analysis car-
ried out, for the detection of diseases, we have cho-
sen the Multiclass Decision Jungle as an algorithm
for the detection and diagnosis of diseases. On the
other hand, according to Table 1c, for the detection
of mortality we have selected the Two Class Decision
Forest.
4.3 Discussions
The reason we chose the Multiclass Decision Jungle
over the other classification algorithms is justified in
the precision matrix. The matrix, as shown in Figure
7, with the lowest amount of empty blocks is benefi-
cial for the proposal, since it rules out fewer diseases
during detection and favors obtaining more real re-
sults. In addition to that, it is the one that has the best
parameters and results at the time of experimentation,
not having an overtraining or having too low values.
The reason we chose the Two Class Decision For-
est is that, over the other classification algorithms we
have tested, this is the one that has returned us bet-
ter results. This, because it has a better Accuracy
and Precision that will help to obtain better results
from our algorithm. Additionally, it is better than
the Two Class Averaged Perceptron and Two Class
Boosted Decision Tree algorithms, as these return
very low values to be selected. Regarding the Two
Class Decision Forest, it obtained metrics quite simi-
lar to the Two Class Bayes Point Machine, so any of
these would have been useful.
Initially, we want to recognize the user’s name by
assigning a Dataset of names; However, the number
Figure 6: Multiclass Decision Jungle Precision Matrix.
of records exceeded 40,000 names, which overloaded
the vocabulary of the robot and began to present errors
and slowness during testing. From there, we limit the
number of names to recognize and avoid overloading
the vocabulary with a lot of data. Among those that
occupy the most space are combinations of numbers
and names. Subsequently, we make improvements so
that, before receiving each input data, the vocabulary
is configured to be more limited and less overloaded.
5 CONCLUSIONS
First, the Nao has technical tools that have very been
useful, however, it has limitations in terms of Speech
ICPRAM 2023 - 12th International Conference on Pattern Recognition Applications and Methods
946

Recognition. Additionally, it has sensitivity to noise,
that is, if in the place where we are there is too much
noise around, the Nao will not be able to detect the
voice of the person or may have difficulties. Testing
the code was difficult at this stage because it’s not pos-
sible to test with Choreography if input data in audio
format is needed. Also, the person cannot be at a great
distance from the microphones of the Robot (which
are in his head), otherwise, the listening of this will
be low and may have problems to understand the mes-
sage. According to this, we noticed that the Nao robot
has a greater facility to capture numbers when listen-
ing to them, than large words. You are more likely to
ask to repeat the word than to ask to repeat the dic-
tated number. Another limitation is related to Internet
access, because if it were possible to access the In-
ternet connected to the Nao robot, our full flow time
will be severely reduced. Finally, special care must
be taken when training with the classification algo-
rithms, because some datasets can generate overtrain-
ing, which would generate irregular results (Burga-
Gutierrez et al., 2020).
For future improvements, more diseases can be
added to the dataset so that it can cover a larger field
and can be run again with the same algorithm. Al-
though our premise is that the input data is said aloud,
our flow time can decrease if the patient, instead of
dictating the symptoms one by one, can have a table
with the total symptom numbers and tell the numbers
to the robot. Similar to this, the reception of the tele-
phone number generates that the time flow increases
considerably. We suggest that this data can be typed
and the results can be sent to the doctor if applica-
ble. Additionally, by skipping this step, we can avoid
scaring the patient, because we do not know how sen-
sitive he may be and may even misinterpret the robot’s
comments on the results. Furthermore, combining our
approach with other kinds of smart health allocation
systems (Ugarte, 2022).
REFERENCES
Arslan, H. (2021). COVID-19 prediction based on genome
similarity of human sars-cov-2 and bat sars-cov-like
coronavirus. Comput. Ind. Eng., 161.
Barrutia-Barreto, I., S
´
anchez-S
´
anchez, R. M., and Silva-
Marchan, H. A. (2021). Consecuencias econ
´
omicas
y sociales de la inamovilidad humana bajo covid – 19
caso de estudio per
´
u. Lecturas de Econom
´
ıa, 1(94).
Brunese, L., Martinelli, F., Mercaldo, F., and Santone, A.
(2020). Machine learning for coronavirus covid-19
detection from chest x-rays. Procedia Computer Sci-
ence, 176.
Burga-Gutierrez, E., Vasquez-Chauca, B., and Ugarte, W.
(2020). Comparative analysis of question answering
models for HRI tasks with NAO in spanish. In SIM-
Big.
Burns, R. B., Lee, H., Seifi, H., Faulkner, R., and Kuchen-
becker, K. J. (2022). Endowing a NAO robot with
practical social-touch perception. Frontiers Robotics
AI, 9.
Fale, M. I. and Gital, A. Y. (2022). Dr. flynxz - A first aid
mamdani-sugeno-type fuzzy expert system for differ-
ential symptoms-based diagnosis. J. King Saud Univ.
Comput. Inf. Sci., 34(4).
Filippini, C., Perpetuini, D., Cardone, D., and Merla, A.
(2021). Improving human-robot interaction by en-
hancing NAO robot awareness of human facial expres-
sion. Sensors, 21(19).
Gianella, C., Gideon, J., and Romero, M. J. (2021). What
does covid-19 tell us about the peruvian health sys-
tem? Canadian Journal of Development Studies / Re-
vue canadienne d’
´
etudes du d
´
eveloppement, 42(1-2).
H
¨
ansch, R. (2021). Handbook of Random Forests - Theory
and Applications for Remote Sensing. Series in Com-
puter Vision. WorldScientific.
Hoffmann, M., Wang, S., Outrata, V., Alzueta, E., and
Lanillos, P. (2021). Robot in the mirror: Toward
an embodied computational model of mirror self-
recognition. K
¨
unstliche Intell., 35(1).
Miyahira, J. (2020). Lo que nos puede traer la pandemia.
Revista Medica Herediana, 31(2).
Rehman, M., Shah, R. A., Khan, M. B., Shah, S. A., Abuali,
N. A., Yang, X., Alomainy, A., Imran, M. A., and
Abbasi, Q. H. (2021). Improving machine learning
classification accuracy for breathing abnormalities by
enhancing dataset. Sensors, 21(20).
Romero-Garc
´
ıa, R., Mart
´
ınez-Tom
´
as, R., Pozo, P., de la
Paz, F., and Sarri
´
a, E. (2021). Q-CHAT-NAO: A
robotic approach to autism screening in toddlers. J.
Biomed. Informatics, 118.
Rozo, A., Buil, J., Moeyersons, J., Morales, J. F., van der
Westen, R. G., Lijnen, L., Smeets, C., Jantzen, S.,
Monpellier, V., Ruttens, D., Hoof, C. V., Huffel, S. V.,
Groenendaal, W., and Varon, C. (2021). Controlled
breathing effect on respiration quality assessment us-
ing machine learning approaches. In IEEE CinC.
Shotton, J., Sharp, T., Kohli, P., Nowozin, S., Winn, J. M.,
and Criminisi, A. (2013). Decision jungles: Compact
and rich models for classification. In NIPS.
Ugarte, W. (2022). Vaccination planning in peru using con-
straint programming. In ICAART.
Yoon, Y., Ko, W., Jang, M., Lee, J., Kim, J., and Lee, G.
(2019). Robots learn social skills: End-to-end learn-
ing of co-speech gesture generation for humanoid
robots. In IEEE ICRA.
Classification of Respiratory Diseases Using the NAO Robot
947
