
Living on Video: Insights on the User Perspective of Video-Based AAL
Technology
Caterina Maidhof
a
, Julia Offermann
b
and Martina Ziefle
c
Chair of Communication Science, RWTH Aachen University, Campus Boulevard 57, Aachen, Germany
{maidhof, offermann, ziefle}@comm.rwth-aachen.de
Keywords:
Video-Based AAL Technology, Acceptance, Privacy, Older Adults, Quantitative Study.
Abstract:
Research on video-based Ambient Assisted Living (AAL) technologies is increasing due to their potential of
providing abundant sensory information about a person in need of support. Acceptance of these visual sensors
is limited among potential users as perceptions of barriers persist, most importantly privacy concerns. The
current study aimed to investigate potential users’ behavioural intention to use video-based AAL and their
evaluations of relevant benefits and barriers during activities of daily living in their own homes. Special focus
was on exploring the influences of individual differences (demographics and psychometrics) on evaluation
patterns. In total, evaluations of 122 participants (age range: 17-81 years) were assessed through an online
survey. The results are in line with previous findings on perceived benefits and barriers and their relevance to
the acceptance of AAL technology. Beyond that, the results revealed significant relationships and impacts of
individual differences, i.e., privacy perception, self-consciousness, and body consciousness, on the perceived
barriers and indirectly also on the acceptance of video-based AAL technology. Further, three clusters of
potential users were identified, differing significantly in their evaluation of video-based AAL technology as
well as in their individual characteristics, i.e., privacy perception and self-consciousness. The findings of this
study are useful to derive recommendations for user-tailored development and communication of video-based
AAL technology.
1 INTRODUCTION
Ambient Assisted Living (AAL) technology is em-
bedded through various environmental and wearable
sensors into a person’s daily living environment to
provide support for activities of daily living and pre-
vent risky incidents for people in need of assistance.
Among others, vital signs and changes in mobility
and activity patterns can be monitored with AAL con-
tributing to more safety, well-being, and autonomy
(Choukou et al., 2021; Blackman et al., 2016; Cal-
varesi et al., 2017). Visual sensors such as RGB or
depth cameras are increasingly included among the
AAL set-up as these video-based technologies have
the advantage of providing abundant sensory infor-
mation (Climent-P
´
erez et al., 2020). This way, other
sensors may even become redundant because any ac-
tivity in a specific room can be monitored by one sin-
gle camera (Cardinaux et al., 2011). While the trend
towards visual sensors may be reasonable from a tech-
a
https://orcid.org/0000-0002-0573-4498
b
https://orcid.org/0000-0003-1870-2775
c
https://orcid.org/0000-0002-6105-4729
nological perspective, studies depicting the user per-
spective suggest an instead rejecting attitude towards
video-based monitoring mentioning privacy issues as
one main concern in the process of technology accep-
tance (e.g., (Beach et al., 2009; Arning and Ziefle,
2015; Offermann-van Heek et al., 2019)).
1.1 AAL Acceptance and Privacy
Robust models such as the Technology Acceptance
Model (TAM) (Davis, 1987) and the Unified The-
ory of Acceptance and Use of Technology (UTAUT)
(Venkatesh et al., 2012) with their main variables Per-
ceived Usefulness (PU) and Perceived Ease of Use
(PEOU) prevail in research on technology acceptance
but lack possibilities for context-specific evaluations
(Chen and Chan, 2011). To specifically understand
AAL acceptance, (Jaschinski et al., 2021) highlighted
relevant belief antecedents for AAL acceptance in-
cluding Attitude towards using AAL, Social Norm,
Personal Norm and Perceived behaviour control as
decisive multidimensional belief constructs in their
conceptual model. The latter model succeeded to ex-
28
Maidhof, C., Offermann, J. and Ziefle, M.
Living on Video: Insights on the User Perspective of Video-Based AAL Technology.
DOI: 10.5220/0011759800003476
In Proceedings of the 9th International Conference on Information and Communication Technologies for Ageing Well and e-Health (ICT4AWE 2023), pages 28-39
ISBN: 978-989-758-645-3; ISSN: 2184-4984
Copyright
c
2023 by SCITEPRESS – Science and Technology Publications, Lda. Under CC license (CC BY-NC-ND 4.0)

plain 69% of the variance in behavioural intention to
use AAL technology and depicts the relative impor-
tance of various acceptance factors including benefits
and barriers of such technology use.
Indeed, previous research on assistive technol-
ogy has identified that acceptance is considerably im-
pacted by the evaluation of several barriers (privacy
implications, lack of control over technology, false
alarms, obtrusiveness, low ease of use, high costs,
stigmatization) and benefits (increased safety, per-
ceived usefulness, increased independence, reduced
burden for family caregivers, mobility and support
with daily activities) (e.g., (Jaschinski and Allouch,
2015; Jaschinski and Allouch, 2019; Zander et al.,
2021; Peek et al., 2014; Yusif et al., 2016; Garg
et al., 2014; G
¨
overcin et al., 2010; Wild et al., 2008)).
Findings suggest that benefits and barriers are typi-
cally traded-off against each other when it comes to
a decision whether to adopt this technology or not
(Offermann-van Heek and Ziefle, 2019; Jaschinski
et al., 2021; Ehrari et al., 2020). While increased
safety is most often a decisive driver of AAL tech-
nology acceptance (Schomakers and Ziefle, 2022),
concerns regarding privacy and related aspects like
the feeling of permanent surveillance, (unauthorized)
data access and misuse of personal information, infor-
mation sensitivity, invasion of personal space, and ob-
trusiveness are the most relevant barriers in that trade-
off process (Garg et al., 2014; Schomakers and Ziefle,
2019; Lorenzen-Huber et al., 2011).
Especially in contexts where visual sensors such
as video-based AAL are installed in the daily living
environment for constant monitoring, privacy con-
cerns are paramount (Arning and Ziefle, 2015; Mul-
venna et al., 2017; Berridge et al., 2019; Maidhof
et al., 2022a). In fact, actions, situations, (mental)
states, places and objects can all be labelled as pri-
vate (R
¨
ossler, 2001) which at the same time can all
be captured and easily interpreted by a visual sen-
sor. In this manner, the preservation of privacy in
such an intimate place as the own home (e.g., (Wiles
et al., 2012)) is challenged on different levels. (Bur-
goon, 1982) provides a privacy framework that ad-
equately covers the multidimensionality of studying
privacy perceptions in video-based AAL and has al-
ready been applied previously in the field (Schomak-
ers and Ziefle, 2019; Maidhof et al., 2022b). The
author (Burgoon, 1982) divides between four dimen-
sions of privacy, namely, dimensions of social privacy
(control over social contacts, interaction, and commu-
nication), of physical privacy (degree of physical in-
accessibility) as well as of psychological privacy (de-
gree of inaccessibility to thoughts, feelings, and inti-
mate information), and of informational privacy (con-
trol over personal information). To adequately ad-
here to these concerns raised by potential users, their
subjective privacy perceptions in all these dimensions
have to be considered.
1.2 Individual Differences
Several individual differences among a variety of po-
tential AAL users have been identified to influence
the trade-off process of benefits and barriers and with
that the behavioural intention of adopting AAL. As
such, age has been reported to play a role. For in-
stance, (Arning and Ziefle, 2009) reported that utiliza-
tion barriers are perceived as higher for older adults
who also expressed more concerns about data safety
issues. Focusing on both age and gender, findings
from (Wilkowska et al., 2010) suggested a decreasing
trust and motivation to use medical technology with
age among females and a varying trust and motivation
to use these technologies among males throughout the
age. Disability or the perceived need for care has also
been identified as a relevant motivator for technology
acceptance with disabled people being more accep-
tant of sharing and recording information captured by
a monitoring device compared to non-disabled per-
sons (Beach et al., 2009). Indeed, (Offermann-van
Heek et al., 2019), showed that the perception of
benefits, barriers, and general acceptance of assisting
technologies is influenced by personal care needs. If
care needs are higher, the benefits of technology are
more acknowledged and barriers are partly more re-
jected.
Besides these demographic markers, psycholog-
ical differences may be relevant in the acceptance
processes but have not been studied extensively so
far in relation to video-based AAL. Especially, in a
setting where visual sensors are involved, it might
be interesting how potential users frame their per-
ceptions of benefits and barriers including their sub-
jective privacy perceptions based on the unfolding
of a specific their specific aspect of their person-
ality, namely their dispositional tendencies towards
self-awareness. This disposition, conceptualized as
self-consciousness, is a relatively stable individual
difference concerning the tendency to direct atten-
tion and thought toward oneself (Fenigstein et al.,
1975; Fenigstein, 2009). Research has consistently
shown that self-consciousness is composed of two,
largely independent dimensions: public and private
self-consciousness. Private self-consciousness com-
prises ”the tendency to be aware of and attentive to
the covert, internal aspects of oneself, such as one’s
thoughts and feelings and aspirations” ((Fenigstein,
2009); p.496). Public self-consciousness, on the other
Living on Video: Insights on the User Perspective of Video-Based AAL Technology
29

hand, concerns ”an awareness of and interest in the
external manifestations of the person, such as appear-
ance, social behaviour and the impression made on
others” ((Fenigstein, 2009); p.496). Privately and
publicly self-conscious people differ in the identities
they try to create for themselves. Whereas public
self-conscious people portray themselves as cooper-
ative team players trying to adapt their behaviour to
conform expectations and preferences of others, pri-
vate self-conscious people present themselves as be-
ing autonomous and independent and trying to convey
these conceptions in social interactions (Schlenker
and Weigold, 1990). It is important to note that self-
consciousness is not value-loaded (neither positive
nor negative) but is considered as a relatively pure at-
tentional tendency (Fenigstein, 2009). These psycho-
logical factors of self-consciousness are also associ-
ated with an interest in the bodily aspects of oneself.
Analogous to self-consciousness, it includes private
body consciousness, the attentional focus on inter-
nal bodily sensations (e.g., heartbeat, pain) and pub-
lic body consciousness meaning a chronic tendency to
focus on and be concerned with the external appear-
ance of the body (e.g. hairstyle, body shape), which
is essentially the same personality trait as public self-
consciousness (Miller et al., 1981a).
While these dispositional constructs have not been
studied in relation to video-based monitoring of ac-
tivities in the own home, self-consciousness has been
explored within research on consumer acceptance
behaviour. For instance, self-consciousness is re-
ported to affect consumer adoption of online shop-
ping (L
´
opez-Bonilla et al., 2021) and the consumer
decision-making process of fashion items (Lee and
Workman, 2020).
In this study, the behavioural intention to use
video-based AAL technology during activities of
daily living in the own home is assessed includ-
ing evaluations of perceived benefits, perceived gen-
eral barriers and perceived privacy barriers. Fur-
thermore, the influences of public and private self-
consciousness as well as body consciousness in the
acceptance process of video-based AAL are explored.
2 METHOD AND MATERIALS
In this chapter, the empirical approach of the study is
presented. First, the design of the online survey and
its subsequent data analysis are explained. Second,
the participants of the study are described.
Figure 1: Empirical Design.
2.1 Online Questionnaire
Based on the previously described literature and a pre-
ceding qualitative study, a questionnaire was devel-
oped and delivered online through the social media
channels of one of the researchers. It addressed par-
ticipants of all ages. The questionnaire was divided
into two main parts.
The first part of the questionnaire started with de-
mographics, such as age, gender, educational level, as
well as living situation and place of living. Then, in-
formation about participants’ health (i.e., if they suf-
fered from a chronic illness and if they needed care),
as well as information about having experience in car-
ing for another person was asked. Subsequently, ad-
ditional user factors such as working field, techni-
cal understanding (four items) (Beier, 1999; Beier,
2003), and psychometrics were assessed. For the lat-
ter, user factors relevant in the context of video-based
AAL were chosen, such as body consciousness (three
items) (Miller et al., 1981b), private and public self-
consciousness (three items each) (Fenigstein et al.,
1975; Scheier and Carver, 1985). In addition, gen-
eral privacy attitudes (16 items) (partly based on (Bur-
goon, 1982)) were assessed to evaluate participants’
understanding of the meaning of privacy in daily life.
The second part of the questionnaire introduced
video-based AAL with a detailed explanation. Partic-
ipants were then asked to evaluate their overall accep-
tance (partly based on (Davis, 1987; Venkatesh et al.,
2012; Jaschinski et al., 2021)) of imagining them-
selves living with such a technology. Specific refer-
ICT4AWE 2023 - 9th International Conference on Information and Communication Technologies for Ageing Well and e-Health
30

ence was made to several activities of daily living in
the own home. Participants had to indicate their over-
all acceptance (three items) and their evaluation of
benefits (five items) and barriers (six items). Among
the barriers, three items dealt with privacy invasion,
which later in the analysis became one construct. For
further analyses of the general acceptance of video-
based analyses the respective constructs (Perceived
Benefits, General Perceived Barriers, Perceived Pri-
vacy Barriers, and Behavioral Intention to Use video-
based AAL technology) were summarized and not in-
vestigated separately for each type of activity.
In conclusion, participants were given the oppor-
tunity to share their thoughts or critiques about the
questionnaire. All scales were rated on six-point Lik-
ert scales (1 = completely disagree, 6 = completely
agree). An overview of the empirical approach of the
study is given in Figure 1.
2.2 Data Analysis
Reliability analysis ensured the measurement quality
of all constructs (Cronbach’s α > .7). The measured
constructs are reported by means of descriptive statis-
tics such as means (M) and Standard Deviations (SD)
and percentages (%) of the examined sample.
To analyze potential relationships between the ac-
ceptance and perception of video-based AAL technol-
ogy on the one hand and user factors like body con-
sciousness, and private- and public-self conscious-
ness, on the other hand, Pearson Correlation coef-
ficients (r) were calculated for continuous variables.
Based on the results of the correlation analysis, linear
regression analysis was conducted in order to analyze
which type of benefits and barriers was most decisive
for the acceptance of video-based technology. Linear
regression analyses were also conducted to analyze
the effects of the above-mentioned user factors on the
perception of the two types of barriers in more detail.
Beyond analyses of the whole sample, cluster
analyses were used to identify segments or groups
of participants according to their similarities in their
evaluation patterns (Hair, 2011). Thereby, a two-step
cluster analysis approach (Hierarchical and K- means
cluster analysis) was applied based on the constructs
Perceived Benefits, General Perceived Barriers, Per-
ceived Privacy Barriers, and Behavioral Intention to
Use video-based AAL technology. ANOVAs corrob-
orated the validity of the cluster segmentation, as the
three clusters significantly differed regarding specific
user factors and the respective construct scores.
The level of statistical significance (p) was set at
the conventional level of 5%(∗p < .05;∗ ∗ p < .01),
thus values above the significance level of p > 0.05
were interpreted as not significant (n.s.).
2.3 Participants
Overall, 122 participants completed the question-
naire. Their age ranged from 17 to 81 (M=38.39;
SD=16.69) with 63.9% females (N=78), and 32.1%
males (N=44) (no participant indicated being divers
or disclosed information). Asked for participants’
highest educational degree, 5.7% (N=7) participants
had at least a secondary school diploma or 29.5%
(N=36) a high school diploma/A-Level degree. The
remaining 64.7% either had a university degree
(N=75) or a promotion/doctoral degree (N=4). 34.4%
(N=42) indicated working in a technical environment
compared to 65.6% (N=80) not having a technical
profession. The general technical understanding was
quite decent (M= 4.14; SD= 1.07; Cronbach’s α =
.74). The majority (64.2%; N=70.5%) were living in
the city, only 10.7% (N=13) in the suburbs and 18.9%
(N=23) indicated living in the countryside. Some par-
ticipants (19.7%; N=24) lived alone, 42.6% shared
their living space with another person such as a part-
ner and the remaining 37.7% (N=46) stated to live
together with more than one person such as a fam-
ily or flatmates. Participants’ privacy understanding
was quite good (16 items; M= 4.80; SD= 0.60; Cron-
bach’s α = .76). On average, scores for private self-
consciousness were higher (three items; M= 4.40;
SD= 1.08; Cronbach’s α = .70) than scores for pub-
lic self-consciousness (three items; M= 4.10; SD=
1.10; Cronbach’s α = .78). Scores of (Private) Body-
Consciousness were on average rather balanced (three
items; M= 3.88; SD= 1.00; Cronbach’s α = .70).
3 RESULTS
This section presents the results of the empirical
study. First, the evaluations of video-based AAL tech-
nology are descriptively presented for the whole sam-
ple of participants. Then, the relationships between
acceptance and perception of AAL technology as well
as relevant user factors in this context are described.
Finally, the results of a cluster analysis are introduced.
3.1 Acceptance of Video-Based AAL
Technology
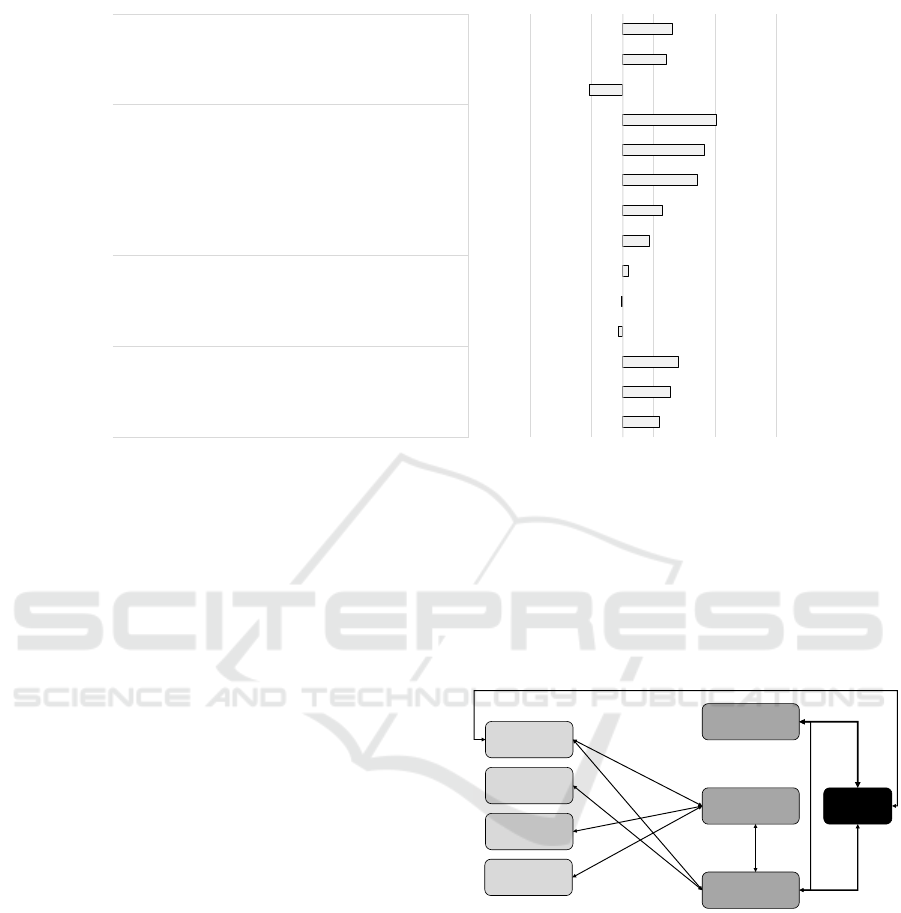
Figure 2 shows the descriptive results for the whole
sample of participants, indicating the evaluation of
all single items referring to the constructs Perceived
Benefits, General Perceived Barriers, Perceived Pri-
Living on Video: Insights on the User Perspective of Video-Based AAL Technology
31
4.10
4.27
4.40
3.43
3.48
3.59
3.92
4.14
4.72
4.82
5.02
2.95
4.22
4.31
1 2 3 4 5 6
Fear of data misuse
Invasion of privacy
Feeling of surveillance
Fear of false alarms
Fear of technical problems
Feeling of incapacitation
Increased comfort and convenience
Increased independence and autonomy
Gain in security
Relief for family caregivers
Faster reactions in emergencies
Video-based technology does not come into my house.
I would like to use video-based technology.
I can well imagine the use of video-based technology.
Privacy Barriers
General
Barriers Perceived Benefits
Behavioural
Intention to Use
Evaluation (min = 1; max = 6)
rejection agreement
Figure 2: Evaluation of video-based AAL technology (N = 122).
vacy Barriers, and Behavioral Intention to Use video-
based AAL technology.
The overall Behavioral Intention to Use video-
based AAL technology was rather high (M=4.06;
SD=.72). In this regard, the participants confirmed
both positive statements (e.g., ”I can well imagine the
use of video-based technology” (M=4.31; SD=.96))
and slightly rejected the negative statement: ”Video-
based technology does not come into my house for
this purpose” (M=2.95; SD=1.12).
Moving to the Perceived Benefits, the participants
generally acknowledged and confirmed the poten-
tial benefits of using video-based AAL technology
(M=4.52; SD=.76). This was also true for all five sin-
gle items, but to a different extent. The benefits re-
lated to ”Faster reactions in emergencies”, ”Relief for
family caregivers”, and ”Gain in security” received
the highest agreement and were thus most relevant.
The benefits ”Increased independence and autonomy”
and ”Increased comfort and convenience” received
lower, but still confirming evaluations.
Further, the General Perceived Barriers (M=3.50;
SD=.92) were evaluated neutrally, reaching the mean
of the scale. This was also true for all three single
items, which all circulated closely around the mean
of the scale (see Figure 2). Finally, the Perceived
Privacy Barriers received a clearly higher evaluation
and were confirmed to be relevant barriers of using
video-based AAL technology (M=4.26; SD=1.00).
Here, the ”Feeling of surveillance” received the high-
est agreement, followed by ”Invasion of Privacy” and
”Fear of data misuse”.
3.2 Relationships and Interactions
Acceptance
Perceived
Benefits
General Perceived
Barriers
Perceived Privacy
Barriers
r = .646**
r = -.489**
r = -.291**
r=.426**
Privacy
Perception
Private Self
Consciousness
Public Self
Consciousness
Body
Consciousness
r =.317**
r = .268**
r = .335**
r =.202**
r = .213**
r = .213**
Figure 3: Correlations between constructs and user factors
(N = 122) (r: correlation coefficient).
Figure 3 shows all results of the conducted correla-
tion analyses. The strongest correlations between the
perception and the Acceptance of video-based AAL
technology (here operationalized as behavioural in-
tention to use) are presented. Thereby, Acceptance
was strongly connected with the Perceived Benefits
(r=.646; p < .01) and moderately negatively related
with the Perceived Privacy Barriers (r=-.489; p <
.01). Interestingly, there was no significant direct cor-
relation with the General Perceived Barriers, which
in turn were moderately related with the Perceived
Privacy Barriers (r=.426; p < .01). In addition, the
ICT4AWE 2023 - 9th International Conference on Information and Communication Technologies for Ageing Well and e-Health
32
Perceived Privacy Barriers were negatively related
with the Perceived Benefits (r=-.291; p < .01).
Beyond these relationships, it was also analyzed
to what extent attitudinal characteristics and user fac-
tors of the participants are related to the percep-
tion and acceptance of video-based AAL technology.
Here, the participants’ Privacy Perception was the
own user factor that was directly related to the Ac-
ceptance of video-based AAL technology (r=.213;
p < .01). In addition, the Privacy Perception was
also connected with the General Perceived Barriers
(r=.268; p < .01) as well as with the Perceived Pri-
vacy Barriers (r=.335; p < .01). Further, the partic-
ipants’ Private Self-Consciousness showed a moder-
ate relationship with the Perceived Privacy Barriers
(r=.317; p < .01), while the participants’ Public Self-
Consciousness (r=.202; p < .01) as well as their Body
Consciousness (r=.213; p < .01) were both related
with the General Perceived Barriers.
Acceptance
(r
2
=.504)
Perceived
Benefits
General Perceived
Barriers
(r
2
=.234)
Perceived
Privacy Barriers
(r
2
=.335)
β = .551**
β = -.323**
Privacy
Perception
Private Self
Consciousness
Body
Consciousness
β = -.255**
β =.370**
β =.197*
β =.255**
β =.233**
β =.426**
Figure 4: Results of regression analysis: constructs and user
factors (N = 122) (β : standardized regression coefficient).
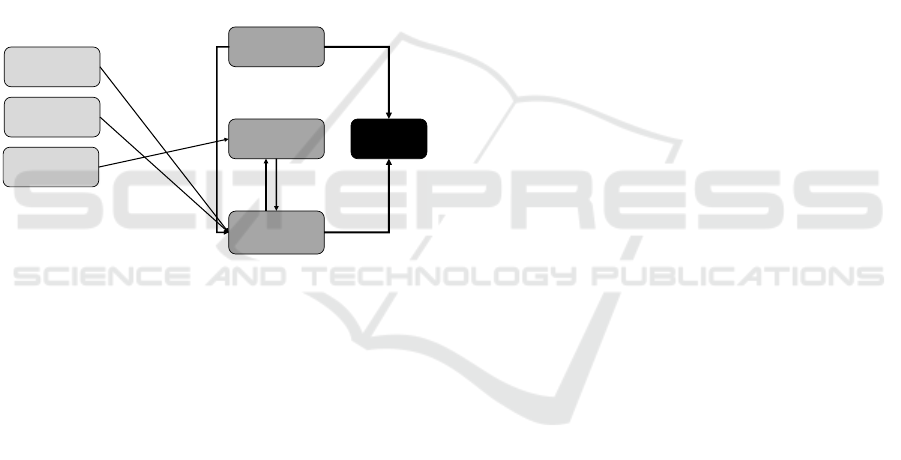
Based on the results of the correlation analysis,
linear regression analyses were conducted (see Fig-
ure 4). In the first step, the Acceptance of video-based
AAL technology was focused. The results show that
50.4% of variance of the Acceptance of video-based
AAL technology (adj. r
2
=.504) can be explained by
the constructs Perceived Benefits (β =.551; p < .01)
and Perceived Privacy Barriers (β =-.323; p < .01).
Furthermore, the results of the correlation analyses
suggested analyzing the Perceived Privacy Barriers
and the General Perceived Barriers in more detail.
Starting with the Perceived Privacy Barriers the lin-
ear regression analysis revealed that 33.5% of its vari-
ance (adj. r
2
=.335) can be explained by the constructs
General Perceived Barriers (β =.370; p < .01) and
the user factors Privacy Perception (β =.197; p < .05)
as well as Private Self-Consciousness (β =.255; p <
.01). With regard to the General Perceived Barriers,
still 23.4% of its variance (adj. r
2
=.234) can be ex-
plained by the Perceived Privacy Barriers (β =.426;
p < .01) as well as the user factor Body Conscious-
ness (β =.233; p < .01).
3.3 Acceptance, Privacy Concerns and
the Self: A Cluster Analysis
Beyond the results for the whole sample of partici-
pants, we conducted a two-step cluster analysis ap-
proach to identify user groups with specific evalua-
tion patterns of video-based AAL technology. Based
on the previous results, we assumed that these clusters
will also differ with regard to individual user factors.
According to the hierarchical cluster analysis,
three clusters were identified as optimal cluster so-
lution in the data set. The first cluster included
n=26 (21.3%) participants, the second cluster n=45
(36.9%), and the third cluster n=51 (41.8%) respon-
dents. Based on that, a K-means Cluster analysis
was conducted to segment respondents into three dis-
tinct groups based on the four construct scores (Hair,
2011): Perceived Benefits, General Perceived Barri-
ers, Perceived Privacy Barriers, and Behavioral In-
tention to Use video-based AAL technology. Con-
firming the assumption, ANOVAs corroborated the
validity of the cluster segmentation, as the three
clusters significantly differed regarding the construct
scores (see Figure 5 and user factors (see Table 1).
The presentation of the cluster analysis results is
structured as follows: First, the findings regarding
differences between the three clusters (demographic
characteristics and the factors scores) are reported.
Second, the clusters are characterized by their eval-
uations of the items of the respective constructs.
Starting with differences regarding user factors
(see Table 1), Cluster 2 was significantly older than
Cluster 1 and 3, while those two clusters did not dif-
fer significantly with regard to age. Related to other
demographic characteristics, the three clusters did not
reveal any significant differences (i.e., gender, edu-
cational level, health status, care needs, experiences
in care, and living situation). Taking other user fac-
tors, such as attitudinal characteristics, into account,
the private and public self-consciousness, as well as
individual privacy perception, characterized the three
clusters differed significantly. With regard to each of
the mentioned variables, Cluster 3 showed the high-
est, Cluster 1 the lowest, and Cluster 2 medium eval-
uations. To sum up, Cluster 2 can be characterized
as the oldest user group with a medium evaluated
private and public self-consciousness and a medium
level of individual privacy perception. Cluster 1 is
clearly younger and can be distinguished by the in
comparison lowest evaluations of private and public
self-consciousness as well as a comparably low in-
dividual privacy perception. Cluster 3 is almost as
young as Cluster 1, but in contrast, the participants
are characterized by the highest evaluations in private
Living on Video: Insights on the User Perspective of Video-Based AAL Technology
33
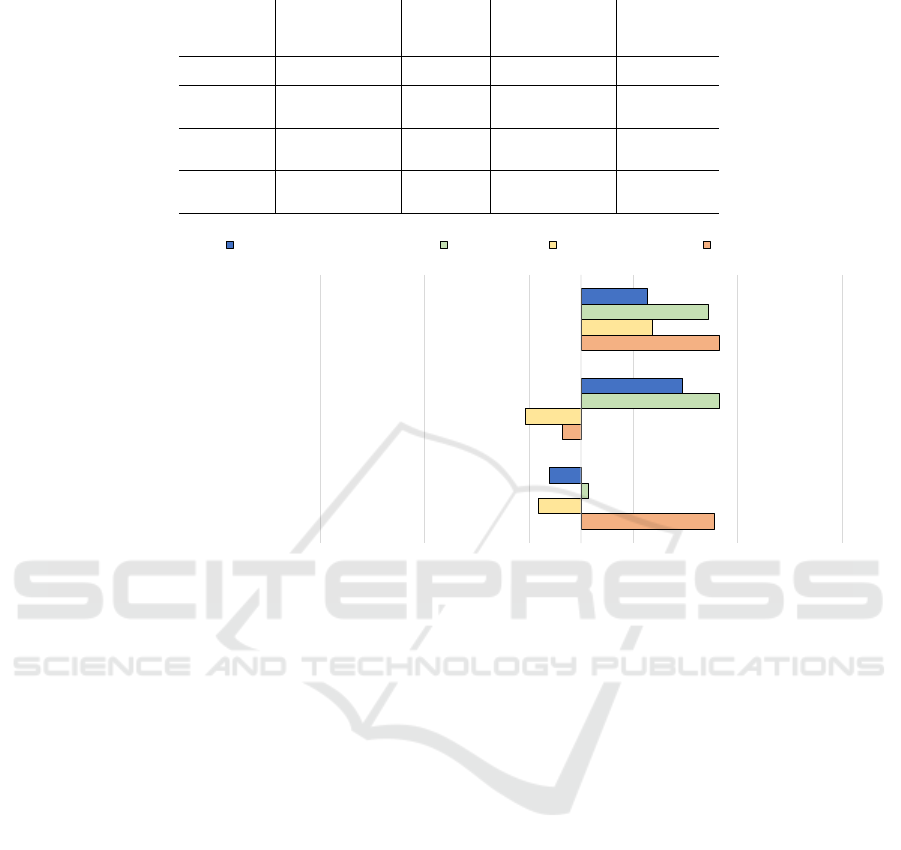
Table 1: Influences of user factors on the cluster segmentation.
Cluster 1
(n = 26)
”Privacy-Conscious
rejecters”
Cluster 2
(n = 45)
”adopters”
Cluster 3
(n = 51)
”Privacy-Conscious
adopters”
Inference
Statistics
Age
(M, SD)
34.24 ( 15.18) 45.00 (17.71) 34.71 (14.90)
F(2,116)=5.770;
p <.01
Private Self-
Consciousness
(M, SD)
4.54 (0.90) 3.97 (0.94) 4.72 (0.87)
F(2,121)=8.586;
p <.01
Public Self-
Consciousness
(M, SD)
3.99 (1.09) 3.75 (1.03) 4.45 (1.03)
F(2,121)=5.589;
p <.01
Privacy
Perception
(M, SD)
4.67 (0.68) 4.57 (0.55) 5.01 (0.52)
F(2,121)=7.760;
p <.01
4.78
3.32
4.83
3.09
2.96
4.19
3.57
4.83
4.72
3.19
4.47
4.13
1 2 3 4 5 6
Cluster 1: Privacy-Conscious Rejecters (n = 26)
Cluster 2: Adopters (n = 45)
Cluster 3: Privacy-Conscious Adopters (n = 51)
Evaluation (min = 1; max = 6)
rejection agreement
Behavioral Intention to Use Benefits General Barriers Privacy Barriers
Figure 5: Cluster identification based on constructs (N = 122).
and public self-consciousness as well as the compara-
bly highest individual privacy perception.
Moving to the basis of the cluster segmentation,
the evaluation of the constructs (Figure 5) is now pre-
sented. The Behavioral Intention to Use video-based
AAL technology varied distinctly for the three clus-
ters (F(2,121) = 45.619; p < .01): Cluster 2 showed
the highest confirming evaluation (M=4.47; SD=.45),
while Cluster 3 showed a lower, still positive inten-
tion to use this type of AAL technology (M=4.13;
SD=.54); in contrast, Cluster 1 showed a slightly re-
jecting, clearly lower evaluation of the intention to
use video-based AAL technology (M=3.19; SD=.70).
All differences between the three groups were on a
significant level. Considering the Perceived Benefits
(F(2,121) = 43.511; p < .01), Cluster 2 (M=4.83;
SD=.54) and Cluster 3 (M=4.72; SD=.47) showed
strong confirmations of the potential benefits of us-
ing video-based AAl technology and did not differ
in their evaluations significantly. However, Cluster
1 (M=3.57; SD=.82) expressed a completely neutral,
and significantly lower evaluation of the Perceived
Benefits. Related to the General Perceived Barriers
(F(2,121) = 40.752; p < .01), distinct evaluation pat-
terns were found as well. While Cluster 3 (M=4.19;
SD=.65) was the only Cluster confirming the poten-
tial general barriers, Cluster 2 (M=2.96; SD=.65) and
Cluster 1 (M=3.09; SD=.91) showed similar slightly
rejecting evaluations. Finally, the strongest differ-
ences were identified for the evaluations of Perceived
Privacy Barriers (F(2,121) = 64.909; p < .01): while
Cluster 1 (M=4.78; SD=.85) and Cluster 3 (M=4.83;
SD=.57) showed strong agreements of the Perceived
Privacy Barriers, they were evaluated with slightly
rejecting values by Cluster 2 (M=3.32; SD=.73).
Based on these results, it was possible to charac-
terize, understand and label the three identified Clus-
ters in more detail. Starting with Cluster 1, this group
was characterized by a very high evaluation of Per-
ceived Privacy Barriers, a low evaluation of General
Perceived Barriers, the comparably lowest evaluation
of Perceived Benefits as well as the lowest, slightly
negative Behavioral intention to use and thus low-
est acceptance of using video-based AAL technol-
ogy. We labelled this group ”Privacy-Conscious re-
jecters” as they do not want to use video-based AAL
technology based on a high perception of privacy-
related barriers. Cluster 2 represents almost the op-
posite of Cluster 1 and is characterized by slightly re-
jecting evaluations of Perceived Privacy Barriers and
ICT4AWE 2023 - 9th International Conference on Information and Communication Technologies for Ageing Well and e-Health
34

4.59
4.86
4.88
2.93
3.46
2.88
2.79
3.32
3.69
3.96
4.28
3.85
3.26
3.00
3.12
3.35
3.49
2.88
3.00
3.02
4.23
4.43
5.06
5.19
5.26
2.32
4.75
4.75
4.72
4.79
4.97
4.18
4.18
4.20
4.24
4.31
4.95
4.93
5.18
3.06
4.46
4.37
1 2 3 4 5 6
Fear of data misuse
Invasion of privacy
Feeling of surveillance
Fear of false alarms
Feeling of incapacitation
Fear of technical problems
Increased comfort and convenience
Increased independence and autonomy
Gain in security
Relief for family caregivers
Faster reactions in emergencies
Video-based technology does not come into my house for this purpose.
I can well imagine the use of video-based technology here.
I would like to use video-based technology in this context.
Privacy Barriers General Barriers Perceived Benefits
Behavioural Intention to
Use
Evaluation (min = 1; max = 6)
rejection agreement
Privacy-Conscious
Adopters (n = 51)
Adopters (n = 45)
Privacy-Conscious
Rejecters (n = 26)
Figure 6: Evaluation patterns of identified clusters (N = 122).
General Perceived Barriers. In addition, this clus-
ter showed the highest evaluation of Perceived Ben-
efits and the highest evaluations of the Behavioral in-
tention to use video-based AAL technology. As this
group acknowledges the benefits and shows a positive
usage intention, we labelled this group ”adopters”.
Cluster 3 shows the most indifferent evaluation pat-
tern, as the participants acknowledged the Perceived
Benefits, showed a positive Behavioral intention to
use video-based AAL technology, but simultaneously
they also evaluated Perceived Privacy Barriers and
General Perceived Barriers to be relevant factors. As
they showed a positive usage intention and the trade-
off between potential barriers and benefits are rele-
vant for this group, we labelled this group as ”Privacy-
Conscious adopters”.
Beyond the construct evaluations and based on the
understanding of the three clusters, the evaluations
within the constructs are now focused (see Figure 6).
Since the differences in all 14 items are highly signif-
icant overall, in the following, only the general evalu-
ation patterns are described. Starting with the Behav-
ioral intention to use video-based AAL technology,
”adopters” and ”Privacy-Conscious adopters” showed
similar positive evaluations of the two positive state-
ments, while these statements were slightly rejected
by the ”Privacy-Conscious rejecters”. Consider-
ing the negative statement, the ”Privacy-Conscious
rejecters” showed a slight agreement, while the
”Privacy-Conscious adopters” showed slight and the
”adopters” even clearer rejecting evaluations. Look-
ing at the emphPerceived Benefits, ”adopters” and
”Privacy-Conscious adopters” showed similar pos-
itive evaluations of the benefits ”Fast reactions in
emergencies”, ”Relief for family caregivers”, and
”Gain in security”, while the evaluations of the
”Privacy-Conscious rejecters” successively decrease.
Lower, but still positive evaluations of the benefits of
”Increased independence and autonomy” and of ”in-
creased comfort and convenience” by the ”adopters”
and ”Privacy-Conscious adopters” contrast with re-
jecting evaluations of the ”Privacy-Conscious re-
jecters”.
Considering the General Perceived Barriers, all
single items were confirmed to be relevant barriers
by the group of ”Privacy-Conscious adopters”. In-
stead, all three items were rejected to be relevant
barriers by the group of ”adopters”. The ”Privacy-
Conscious rejecters” rejected the barriers of ”Fear of
technical problems” and of ”Fear of alarms”, while
they evaluated the barrier of ”Feeling of incapacita-
tion” neutrally. The results for the Perceived Privacy
Living on Video: Insights on the User Perspective of Video-Based AAL Technology
35

Barriers showed strong confirmations of all three
items by the ”Privacy-Conscious adopters” as well
as the ”Privacy-Conscious rejecters”. In contrast, the
”adopters” showed neutral (”Feeling of surveillance”)
up to slightly rejecting evaluations (”Fear of data mis-
use”).
Within the next section, the results for the whole
sample, but also the cluster-specific results are sum-
marized, discussed, and used to derive recommenda-
tions with respect to the development of user-centred
video-based AAL technology.
4 DISCUSSION
This study explored and quantified potential users’
perceptions and evaluations of being supported with
video-based AAL in their own homes during activi-
ties of daily living. In particular, the behavioural in-
tention was assessed including the evaluation of the
benefits and barriers of installing video-based AAL.
In a second step, potential influences of general pri-
vacy perception, self - and body consciousness on ac-
ceptance of video-based AAL were explored through
correlation, regression and cluster analysis.
4.1 Interpretation of the Key Findings
Generally, the behavioural intention to use video-
based AAL was rather high among all participants.
This positive trend is further enhanced by overall
higher evaluations of benefits compared to the evalua-
tions of barriers and is in line with literature reporting
a positive perception of AAL technology (e.g., (Garg
et al., 2014; G
¨
overcin et al., 2010; Wild et al., 2008)).
With regard to the here evaluated video-based AAL
technology, the results contradict the so far rather
negative evaluations of and attitudes towards video-
based AAL technology (Beach et al., 2009; Arning
and Ziefle, 2015; Offermann-van Heek et al., 2019),
which could be due to the rather generic description
within the scenario-based approach (see section 4.3).
Regarding benefits, potential users particularly ap-
preciated faster reactions in case of an emergency, re-
lief for family caregivers and increased safety. Pre-
vious findings have already highlighted safety as an
important contributor to technology acceptance and
a suitable incentive to negotiate benefits and barriers
(Schomakers and Ziefle, 2022; Ehrari et al., 2020). In
this trade-off process, usually, the most relevant coun-
terpart is privacy concerns (Garg et al., 2014; Ehrari
et al., 2020; Peek et al., 2014; Offermann-van Heek
and Ziefle, 2019) which were confirmed to be the
higher barriers in this study compared to perceived
general barriers regarding technical issues or feelings
of incapacitation. Furthermore, correlational and re-
gression analysis revealed that perceived benefits and
perceived privacy barriers are explaining factors of
technology acceptance suggesting that acceptance in-
creases with higher evaluated benefits and lower rat-
ings of privacy barriers. General perceived barriers
do not seem to influence acceptance decisively as no
direct statistical relationship could be found. Hence,
these results suggest the idea that in a scenario where
video-based AAL is applied, it is mostly privacy that
evokes hesitation or denial of AAL use.
To gain a better understanding of potential users,
influences of relevant attitudinal and dispositional
user factors were explored. Among them, general pri-
vacy perception was directly related to video-based
AAL acceptance as well as both, general barriers and
privacy barriers. This suggests that potential users
with an elaborate understanding of the meaning of
privacy in daily life tend to accept the technology
with or despite an elevated awareness of the poten-
tial barriers at stake. Public self-consciousness and
body consciousness were related to perceived gen-
eral barriers but only body consciousness could ex-
plain some variance of perceived barriers. In turn,
private self-consciousness influenced ratings of pri-
vacy barriers and could explain some variance of the
latter construct. This leads to suggest that persons
focusing more on the internal aspects of themselves
are more concerned about privacy issues. It remains
unclear whether these privately self-conscious users
perceived privacy barriers as more important because
they are more concerned about the privacy of their
thoughts and feelings or whether privacy is one read-
ily available thought in this trade-off process which is
even more easily retrievable for people with a chronic
tendency to focus on their thoughts. Another expla-
nation of this influence of private self-consciousness
may be that being able to act autonomously is consid-
ered as one function of privacy (R
¨
ossler, 2001) and
autonomy is crucial in the identity of privately self-
conscious persons (Schlenker and Weigold, 1990). In
fact, private self-conscious people attempt to portray
an autonomous identity which as a consequence may
lead to more acknowledgement of privacy and its re-
lated concerns in cases where it is threatened.
4.2 User-Specific Findings and
Recommendations
In addition, the present study identified three distinc-
tive preference profiles of potential users of video-
based AAL, namely, privacy-conscious rejecters,
adopters and privacy conscious-rejecters.
ICT4AWE 2023 - 9th International Conference on Information and Communication Technologies for Ageing Well and e-Health
36

Starting with the privacy-conscious rejecters, this
group was characterized by the highest perception of
privacy-related barriers, leading to the lowest inten-
tion to use video-based AAL technology and a neu-
tral evaluation of potential barriers. Other potential
barriers were not relevant for this group.
In line with their name, the adopters showed the
highest intention to use and also the highest evalua-
tion of potential benefits of video-based AAL tech-
nology. Neither general barriers nor privacy-related
barriers played a decisive role for this group. Con-
sidering individual differences, this group was signif-
icantly older than the other two clusters and hold the
lowest ratings regarding self-consciousness and pri-
vacy perception. Especially the latter explains and fits
perfectly with the evaluation patterns of this group.
The privacy-conscious adopters showed the most
complex evaluation patterns. They showed high per-
ceptions of both, the privacy-related barriers as well
as potential benefits of using video-based AAL tech-
nology. Further, they had a rather positive intention to
use video-based AAL technology and confirmed also
general barriers to be relevant. Looking at the indi-
vidual characteristics, this group was characterized by
the highest evaluations of self-consciousness and pri-
vacy perception. These characteristics in turn fit and
explain the evaluation patterns of this group of poten-
tial users of video-based AAL technology.
Communication strategies informing potential
users about video-based AAL should be specifi-
cally tailored and targeted depending on the vary-
ing evaluation patterns of the different user groups.
Based on the theoretical framework of the elabora-
tion likelihood model (Petty and Cacioppo, 1986),
a central route of communication may be adequate
for both, privacy-conscious rejecters and privacy-
conscious adopters who seem to grasp the whole sce-
nario including the advantages and disadvantages of
adopting video-based AAL and are well aware of
the pitfalls regarding privacy. Indeed, messages for
these groups should be based on technological evi-
dence and logical arguments connecting to their cur-
rent beliefs uncovered through the evaluation pat-
terns. For privacy-conscious rejecters, this means ad-
hering primarily to their huge concern about privacy
infringements. Perhaps technical privacy preservation
techniques such as filters or privacy-by-design and
privacy-by-context approaches should be highlighted
(Climent-P
´
erez et al., 2020; Ravi et al., 2021). Fur-
ther, the legal basis including, for instance, regula-
tions of the GDPR should be mentioned (He, 2022).
Their evaluation patterns seem to suggest that pri-
vacy concerns and low perceptions of benefits are
the reason why they reject the use of video-based
AAL. Therefore, the benefits of using such a tech-
nology should be included perhaps depicting realistic
and reasonable use cases where video-based AAL is
particularly efficient. For privacy-conscious adopters,
benefits are very clear and important, and their be-
havioural intention is given despite high privacy con-
cerns. These concerns should be tackled in a similar
way as for privacy-conscious rejecters and in general
messages should show facts with evidence-based ex-
planations. Contrarily, for adopters with lower scores
for self-consciousness, lower perceived barriers and
with a comparatively high behavioural intention to
use video-based AAL a peripheral route of communi-
cation may be most adequate. Perhaps a suitable tes-
timonial could be part of the communication strategy
and the focus should be more on evoking emotions.
4.3 Limitations and Future Work
The present study successfully replicated findings on
the evaluations of benefits and barriers in the accep-
tance process of video-based AAL. However, partic-
ipants for the study were recruited via convenience
sampling which resulted in a relatively small sam-
ple size. Furthermore, in terms of gender, the sam-
ple consisted of a slightly higher proportion of female
participants. Overall, participants of this study were
rather young, comparably highly educated and either
German or Bulgarian. Ideally, future work should an-
alyze behavioural intention and influences of dispo-
sitional user differences with a larger sample which
is more evenly distributed in terms of demographics.
Also, cultural influences should be considered in the
analysis and different cultural backgrounds should be
compared. The examined technology - video-based
AAL - has not been widely adopted as described
in the scenario in this online survey. In fact, the
scenario used in this online survey was fictitious to
project a possible future scenario and did not provide
a detailed explanation of the technological function-
ing. Here, it has to be considered that especially the
positive evaluations (e.g., intention to use) of video-
based AAL technology could be due to the scenario-
based evaluation and could thus differ from evalua-
tions in real contexts enabling hands-on experience.
As this gap between reported attitudes and real be-
haviour is well-known (Ajzen and Fishbein, 2000),
future work should provide more details and ideally
show the technology either during workshop sessions
or video clips. Furthermore, participants were asked
to imagine that they were the ones needing care. It
would also be interesting to replicate this study for
other contexts such as professional care environments
(i.e., nursing homes) or from an informal carers per-
spective.
Living on Video: Insights on the User Perspective of Video-Based AAL Technology
37

5 CONCLUSION
This quantitative study provided detailed insights into
the perception and acceptance of video-based AAL
technology taking privacy-related barriers as well as
individual characteristics of the participants (i.e., pri-
vacy perception, self- and body consciousness) into
account. Beyond that, three user groups were seg-
mented differing in their evaluation patterns of video-
based AAL technology as well as in their individual
characteristics. The results may be used as a basis
for recommendations and guidelines for user-tailored
development and communication of innovative video-
based AAL technology.
ACKNOWLEDGEMENTS
The authors would like to thank all survey partici-
pants for sharing their opinions, wishes, and needs in
the context of privacy and acceptance of video-based
AAL technologies. We also thank Ivanina Buchkova,
Sophia Otten, and Alexander Hick for their research
support. This work resulted from the project Vi-
suAAL “Privacy-Aware and Acceptable Video-Based
Technologies and Services for Active and Assisted
Living” and was funded by the European Union’s
Horizon 2020 research and innovation programme
under the Marie Skłodowska-Curie grant agreement
No 861091.
REFERENCES
Ajzen, I. and Fishbein, M. (2000). Attitudes and the
attitude-behavior relation: Reasoned and automatic
processes. European review of social psychology,
11(1):1–33.
Arning, K. and Ziefle, M. (2009). Different perspectives on
technology acceptance: The role of technology type
and age. In Symp. of the Austrian HCI & usability
engineering group, pages 20–41. Springer.
Arning, K. and Ziefle, M. (2015). “get that camera out of
my house!” conjoint measurement of preferences for
video-based healthcare monitoring systems in private
and public places. In Int. Conf. on Smart Homes and
Health Telematics, pages 152–164. Springer.
Beach, S., Schulz, R., Downs, J., Matthews, J., Barron, B.,
and Seelman, K. (2009). Disability, age, and infor-
mational privacy attitudes in quality of life technol-
ogy applications: Results from a national web survey.
Transactions on Accessible Computing, 2(1):1–21.
Beier, G. (1999). Kontroll
¨
uberzeugung im umgang mit
technik. Report Psychologie, 9:684–693.
Beier, G. (2003). Control beliefs in dealing with technology.
Humboldt-University Berlin.
Berridge, C., Halpern, J., and Levy, K. (2019). Cameras
on beds: The ethics of surveillance in nursing home
rooms. AJOB empirical bioethics, 10(1):55–62.
Blackman, S., Matlo, C., Bobrovitskiy, C., Waldoch, A.,
Fang, M. L., Jackson, P., Mihailidis, A., Nyg
˚
ard, L.,
Astell, A., and Sixsmith, A. (2016). Ambient assisted
living technologies for aging well: a scoping review.
J. of Intelligent Systems, 25(1):55–69.
Burgoon, J. K. (1982). Privacy and communication. Annals
of the Int. Communication Association, 6(1):206–249.
Calvaresi, D., Cesarini, D., Sernani, P., Marinoni, M., Drag-
oni, A. F., and Sturm, A. (2017). Exploring the am-
bient assisted living domain: a systematic review. J.
of Ambient Intelligence and Humanized Computing,
8(2):239–257.
Cardinaux, F., Bhowmik, D., Abhayaratne, C., and Hawley,
M. S. (2011). Video based technology for ambient
assisted living: A review of the literature. J. of Amb.
Intelligence and Smart Environments, 3(3):253–269.
Chen, K. and Chan, A. H. (2011). A review of technology
acceptance by older adults. Gerontechnology.
Choukou, M., Polyvyana, A., Sakamoto, Y., and Osterre-
icher, A. (2021). Ambient assisted living technologies
to support older adults’ health and wellness: a system-
atic mapping review. European Review for Medical
and Pharmacological Sciences, 25(12):4289–4307.
Climent-P
´
erez, P., Spinsante, S., Mihailidis, A., and Florez-
Revuelta, F. (2020). A review on video-based active
and assisted living technologies for automated lifelog-
ging. Expert Systems with Applications, 139:112847.
Davis, F. (1987). User Acceptance of Information Systems:
The Technology Acceptance Model (TAM). University
of Michigan School of Business Administration.
Ehrari, H., Ulrich, F., and Andersen, H. B. (2020). Concerns
and trade-offs in information technology acceptance:
The balance between the requirement for privacy and
the desire for safety. Communications of the Associa-
tion for Information Systems, 47(1):46.
Fenigstein, A. (2009). Private and public self-
consciousness. In Leary, M. R. and Hoyle, R. H.,
editors, Handbook of individual differences in social
behavior, page 459. The Guilford Press.
Fenigstein, A., Scheier, M. F., Buss, A. H., and Buss, H.
(1975). Public and private self-consciousness: As-
sessment and theory. J. of Consulting and Clinical
Psychology, 43:522–527.
Garg, V., Camp, L. J., Lorenzen-Huber, L., Shankar, K.,
and Connelly, K. (2014). Privacy concerns in assisted
living technologies. annals of telecommunications,
69(1):75–88.
G
¨
overcin, M., K
¨
oltzsch, Y., Meis, M., Wegel, S., Gietzelt,
M., Spehr, J., Winkelbach, S., Marschollek, M., and
Steinhagen-Thiessen, E. (2010). Defining the user
requirements for wearable and optical fall prediction
and fall detection devices for home use. Infor. for
health and social care, 35(3-4):177–187.
Hair, J. (2011). Multivariate data analysis: an overview.
In Int. Encyclopedia of Statistical Science, page pp.
904e907. Springer.
ICT4AWE 2023 - 9th International Conference on Information and Communication Technologies for Ageing Well and e-Health
38

He, Z. (2022). Privacy-enhancing technologies for active
and assisted living: What does the gdpr say? In Pro-
ceedings of the 15th Int. PETRA Conference, pages
430–433.
Jaschinski, C. and Allouch, S. B. (2015). An extended view
on benefits and barriers of ambient assisted living so-
lutions. Int. J. Adv. Life Sci, 7(2).
Jaschinski, C. and Allouch, S. B. (2019). Listening to
the ones who care: exploring the perceptions of in-
formal caregivers towards ambient assisted living ap-
plications. J. of ambient intelligence and humanized
computing, 10(2):761–778.
Jaschinski, C., Allouch, S. B., Peters, O., Cachucho, R.,
Van Dijk, J. A., et al. (2021). Acceptance of tech-
nologies for aging in place: A conceptual model. J. of
medical Internet research, 23(3):e22613.
Lee, S.-H. and Workman, J. (2020). How do face con-
sciousness and public self-consciousness affect con-
sumer decision-making? J. of Open Innovation: Tech-
nology, Market, and Complexity, 6(4):144.
L
´
opez-Bonilla, L. M., Sanz-Altamira, B., and L
´
opez-
Bonilla, J. M. (2021). Self-consciousness in online
shopping behavior. Mathematics, 9(7):729.
Lorenzen-Huber, L., Boutain, M., Camp, L. J., Shankar, K.,
and Connelly, K. H. (2011). Privacy, technology, and
aging: A proposed framework. Ageing International,
36(2):232–252.
Maidhof, C., Hashemifard, K., Offermann, J., Ziefle, M.,
and Florez-Revuelta, F. (2022a). Underneath your
clothes: A social and technological perspective on nu-
dity in the context of aal technology. In Proceedings
of the 15th Int. PETRA Conference, pages 439–445.
Maidhof, C., Ziefle, M., and Offermann, J. (2022b). Ex-
ploring privacy: Mental models of potential users of
aal technology. In ICT4AWE, pages 93–104.
Miller, L. C., Murphy, R., and Buss, A. H. (1981a). Con-
sciousness of body: Private and public. J. of person-
ality and social psychology, 41(2):397.
Miller, L. C., Murphy, R., and Buss, A. H. (1981b). Con-
sciousness of body: Private and public. Journal of
Personality and Social Psychology, 41:397–406.
Mulvenna, M., Hutton, A., Coates, V., Martin, S., Todd,
S., Bond, R., and Moorhead, A. (2017). Views of
caregivers on the ethics of assistive technology used
for home surveillance of people living with dementia.
Neuroethics, 10(2):255–266.
Offermann-van Heek, J., Schomakers, E.-M., and Ziefle, M.
(2019). Bare necessities? how the need for care mod-
ulates the acceptance of ambient assisted living tech-
nologies. Int. j. of medical informatics, 127:147–156.
Offermann-van Heek, J. and Ziefle, M. (2019). Nothing
else matters! trade-offs between perceived benefits
and barriers of aal technology usage. Frontiers in pub-
lic health, 7:134.
Peek, S. T., Wouters, E. J., Van Hoof, J., Luijkx, K. G.,
Boeije, H. R., and Vrijhoef, H. J. (2014). Factors in-
fluencing acceptance of technology for aging in place:
a systematic review. Int. j. of medical informatics,
83(4):235–248.
Petty, R. E. and Cacioppo, J. T. (1986). The elaboration
likelihood model of persuasion. In Communication
and persuasion, pages 1–24. Springer.
Ravi, S., Climent-P
´
erez, P., and Florez-Revuelta, F.
(2021). A review on visual privacy preservation tech-
niques for active and assisted living. arXiv preprint
arXiv:2112.09422.
R
¨
ossler, B. (2001). Der Wert des Privaten. Suhrkamp
Frankfurt am Main.
Scheier, M. F. and Carver, C. S. (1985). The self-
consciousness scale: A revised version for use with
general populations’. Journal of Applied Social Psy-
chology, 15:687–699.
Schlenker, B. R. and Weigold, M. F. (1990). Self-
consciousness and self-presentation: Being au-
tonomous versus appearing autonomous. J. of person-
ality and soc. psychology, 59(4):820.
Schomakers, E.-M. and Ziefle, M. (2019). Privacy percep-
tions in ambient assisted living. In ICT4AWE, pages
205–212.
Schomakers, E.-M. and Ziefle, M. (2022). Privacy vs. secu-
rity: Trade-offs in the acceptance of smart technolo-
gies for aging-in-place. Int. J. of Human-Computer
Interaction, pages 1–16.
Venkatesh, V., Thong, J. Y., and Xu, X. (2012). Consumer
acceptance and use of information technology: ex-
tending the unified theory of acceptance and use of
technology. MIS quarterly, pages 157–178.
Wild, K., Boise, L., Lundell, J., and Foucek, A. (2008). Un-
obtrusive in-home monitoring of cognitive and physi-
cal health: Reactions and perceptions of older adults.
J. of appl. gerontology, 27(2):181–200.
Wiles, J. L., Leibing, A., Guberman, N., Reeve, J., and
Allen, R. E. (2012). The meaning of “aging in place”
to older people. The gerontologist, 52(3):357–366.
Wilkowska, W., Gaul, S., and Ziefle, M. (2010). A small
but significant difference–the role of gender on ac-
ceptance of medical assistive technologies. In Symp.
of the Austrian HCI & Usability Engineering Group,
pages 82–100. Springer.
Yusif, S., Soar, J., and Hafeez-Baig, A. (2016). Older peo-
ple, assistive technologies, and the barriers to adop-
tion: A systematic review. Int. j. of medical informat-
ics, 94:112–116.
Zander, V., Gustafsson, C., Landerdahl Stridsberg, S., and
Borg, J. (2021). Implementation of welfare technol-
ogy: a systematic review of barriers and facilitators.
Disability and Rehabilitation: Assistive Technology,
pages 1–16.
Living on Video: Insights on the User Perspective of Video-Based AAL Technology
39
