
Intelligent Provision of Tailored, Easily Understood, and Trusted
Health Information for Patient Empowerment
Marco Alfano
1,4 a
, John Kellett
2b
, Biagio Lenzitti
3c
and Markus Helfert
1,4 d
1
Innovation Value Institute, Maynooth University, Maynooth, Co. Kildare, Ireland
2
Department of Emergency Medicine, Hospital of South West Jutland, Esbjerg, Denmark
3
Dipartimento di Matematica e Informatica, Università di Palermo, Palermo, Italy
4
Lero, Science Foundation Ireland Research Centre for Software, Ireland
Keywords: Digital Health, Patient Empowerment, Intelligent Agent, Tailored Health Communication, Artificial
Intelligence, Responsible AI, Big Data, Machine Learning.
Abstract: Although digital transformation in healthcare is accelerating, there is still a disconnect between current
healthcare, focused on disease management, and a more holistic approach that looks at the health and
wellbeing of the whole person. The latter approach aims at empowering patients and other health information
seekers by improving their comprehension of their health so that they can manage it better. Currently, few
stand-alone applications for patient empowerment exist and they seldom help users to understand health
information. Thus, health information seekers often interact with the Web through generic search engines,
which often produce results that are overwhelming, too generic, and of poor quality. This paper shows how
the use of Artificial Intelligence (AI) in a responsible way may provide patients and others with health higher
quality information that empowers them to improve their health and wellbeing. It presents an AI engine that
extracts health content from the Web and provides the user with health information that is relevant,
trustworthy, and easy to understand. The AI engine has been used to create an Intelligent Empowering Agent
(IEA) that dialogues with users in simple language to provide customised information on symptoms and
diseases, which helps them form their own evidence-based opinion on health matters that concern them.
1 INTRODUCTION
Although digital transformation in healthcare is
accelerating, “the existing care pathways and care
models rely on prescriptive approaches of health
professionals who assess and direct care and
treatment for patients, rather than creating care
models designed and informed by patients to achieve
personal goals and health outcomes” (Snowdon,
2020; Snowdon et al., 2014). The latter approach aims
at empowering patients by improving their
comprehension of their health so that they can
manage it better (Alfano et al., 2019; European
Health Parliament, 2017; WHO, 2016). Patient's
health literacy, information-seeking behaviour, sense
of meaning, shared decision-making, and self-
a
https://orcid.org/0000-0001-7200-9547
b
https://orcid.org/0000-0002-4741-9242
c
https://orcid.org/0000-0003-2664-7788
d
https://orcid.org/0000-0001-6546-6408
care/self-management are among the most important
elements that characterise person/patient
empowerment (Bodolica and Spraggon, 2019; Cerezo
et al., 2016; Fumagalli et al., 2015). To be empowered
a person/patient must:
1. have the necessary knowledge and self-
awareness to understand health conditions and
treatment options;
2. be able to make informed and conscious health
choices (i.e., decide);
3. actively manage, with or without advice from
medical professionals, their health and well-
being (i.e., act).
Currently, few stand-alone applications for patient
empowerment exist (Snowdon, 2020; Bodolica and
384
Alfano, M., Kellett, J., Lenzitti, B. and Helfert, M.
Intelligent Provision of Tailored, Easily Understood, and Trusted Health Information for Patient Empowerment.
DOI: 10.5220/0011694300003414
In Proceedings of the 16th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2023) - Volume 5: HEALTHINF, pages 384-391
ISBN: 978-989-758-631-6; ISSN: 2184-4305
Copyright
c
2023 by SCITEPRESS – Science and Technology Publications, Lda. Under CC license (CC BY-NC-ND 4.0)

Spraggon, 2019) and patients and other users often go
on the Web to search for health information (Alfano
et al., 2019; Finney Rutten et al., 2019). However,
Web information is mainly obtained through generic
search engines and is often overwhelming, too
generic, outdated and of poor quality (Finney Rutten
et al., 2020; Alfano et al., 2019). Although Artificial
Intelligence (AI) could play an important role in
health empowerment (Iatraki et al., 2018; Kondyalkis
et al., 2013), it often empowers machines rather than
people (i.e., self-diagnosis apps tend to be substitute
doctors and keep patients as passive recipients;
Davenport and Kalakota, 2019; Fast and Horvitz,
2017; Jiang et al., 2017).
This paper presents the principles of the
responsible use of AI for person/patient
empowerment and describes an AI engine that can be
used to extract and process health content from the
Web. It provides the user with health information
tailored to their specific needs, which is simple to
understand and trustworthy. This AI engine powers
an Intelligent Empowering Agent (IEA) that
dialogues with users in simple language and provides
customized information on symptoms and diseases,
which helps them form their own evidence-based
opinions on whatever health matters concern them.
2 RESPONSIBLE AI FOR
PATIENT EMPOWERMENT
Responsible Artificial Intelligence is the “practice of
designing, building, deploying, operationalizing and
monitoring AI systems in a manner that empowers
people and businesses, and fairly impacts customers
and society – allowing companies to engender trust
and scale AI with confidence” (Responsible Artificial
Intelligence Institute, 2021). Although Responsible
AI, Ethical AI, and Trustworthy AI are often used
interchangeably (Responsible Artificial Intelligence
Institute, 2021), in the context of our research to
enhance patient empowerment, we prefer the term
Responsible AI.
The basic principles of Responsible AI in health
are analysed in the WHO guidance on “Ethics &
Governance of Artificial Intelligence for Health”
(2021). It shows that new technologies that use AI
hold great promise to improve diagnosis, treatment,
health research and drug development. AI
technologies can also support government run public
health functions, such as disease surveillance and
outbreak control, provided ethics and human rights
are at the heart of their design, deployment, and use.
The “Ethics guidelines for trustworthy AI” by the EU
High-Level Expert Group on Artificial Intelligence
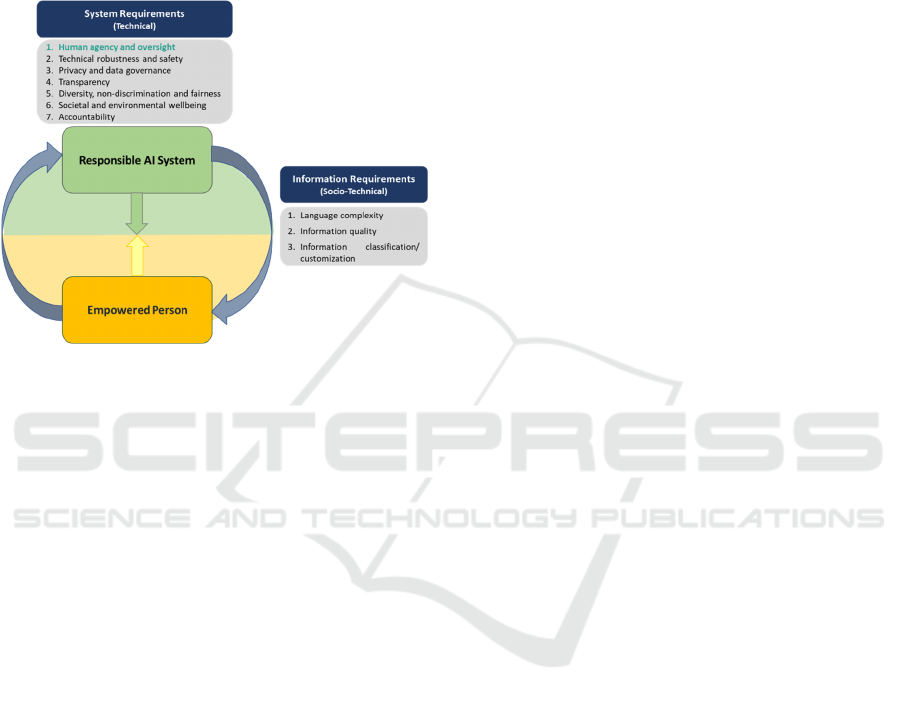
(HLEG, 2019), sets out a list of seven key
requirements on the AI systems:
• Human agency and oversight;
• Technical robustness and safety;
• Privacy and data governance;
• Transparency;
• Diversity, non-discrimination, and fairness;
• Societal and environmental wellbeing;
• Accountability Trustworthy.
Responsible AI requires a holistic and systemic
approach, encompassing the trustworthiness of all
actors and processes that are part of the technical and
socio-technical context. The most important actors
are human beings, and they must be able to interact
with AI systems at any stage. In particular, the first
requirement, “Human agency and oversight”, states
that AI systems should empower human beings by
allowing them to make informed decisions and
safeguarding their fundamental rights. Users should
be given the knowledge and tools to comprehend and
interact with AI systems to a satisfactory degree and,
where possible, be enabled to reasonably self-assess
or challenge them. AI systems should support
individuals in making better, more informed choices,
in accordance with their goals (HLEG, 2019).
There cannot be truly Responsible AI in health
without the direct intervention of “empowered”
human beings (health professionals and patients) who
must be able to understand both the AI-system
process and its outcome, and directly participate in
the decisions and actions that originate. For
person/patient empowerment, the first step is
understanding health information. A previously
published research and a literature review (Alfano et
al., 2019, 2021) identified the following metrics of
health-information comprehension for empowerment
purposes:
• language complexity;
• information quality
• information classification/customization
(tailoring).
Thus, person empowerment becomes both a
requisite and an outcome of Responsible AI
(Fig. 1) and to have Responsible AI in health:
• AI systems must behave responsibly by
applying ethical principles such as the ones
discussed above (technical requirements);
• AI systems must help people to become
empowered by providing health information
Intelligent Provision of Tailored, Easily Understood, and Trusted Health Information for Patient Empowerment
385
that presents characteristics that facilitate its
comprehension (socio-technical requirements).
The application of these principles leads to the
“virtuous circle” shown in Fig. 1. A Responsible AI
system facilitates person empowerment and an
empowered person exerts “human agency and
oversight” on the AI system.
Figure 1: “Virtuous” interaction between Responsible AI
and an empowered person.
3 USING AI FOR EXTRACTING
AND CLASSIFYING WEB
HEALTH INFORMATION
As shown in Alfano et al. (2020) and in Fox et al.
(2013), the most searched type of health information
on the Web is about medical problems and diseases.
Therefore, we decided to provide the user with web
information on symptoms and diseases organised in
sections. This is similar to what many other health
web sites do, but in a more structured,
comprehensive, and interactive way. Initially, we
made a visual analysis of fifty health web pages of
symptoms and diseases to understand what kind of
information is provided and how it could be best
divided into sections. The headings of each web page,
their semantic equivalents and themes were analysed
to determine those which were most frequently
provided; these were then grouped together into the
following initial classification:
• Overview (summary, what is it, what are the
types, definition, description, consideration,
types, types of, deeper types of, basics, basic
information).
• Alternative name (synonyms, substitutes).
• Symptoms (what are the symptoms, clinical
presentation, what you feel, related complaints,
what you cannot do anymore).
• Causes (what is main cause, it is hereditary,
causes, possible causes, most common causes,
most serious causes, what causes, other causes,
culprit, causes of, health conditions).
• Diagnosis and test (how is it evaluated and
diagnosed, what test will be done to diagnose
it, diagnosing, what to expect at a medical visit,
location of your pain, type and intensity,
history of your pain, other medical history,
other types of diagnosis, how is it diagnosed).
• Risk factor (who gets it, what are the risk
factors, who’s at risk, who does it affect).
• When to see a doctor (when to contact
professionals, when to contact a medical
professional, when should I call my healthcare
provider, when to see a doctor, what symptoms
require medical care, when to worry, symptoms
that require urgent care, when should I see my
healthcare provider).
• Management and treatment (how is it
treated, medication for it, treating the
underlying condition, how can I get rid of it,
home care, care and treatment, medication,
medications, how to ease it yourself, treatment
for, medical treatment, home treatment,
surgery).
• Prevention (how can I prevent it, beware of,
can it be prevented).
• Outlook and prognosis (can it be cured, what
happen after I start treatment, what should I
expect in the long term, complications, what is
the outlook if you have it, what’s the outlook,
living with).
Next, we created a list of 474 symptoms derived
from a classic textbook on signs and symptoms
(MacBryde, R.S. Blacklow, 1970), review of the
literature, and expert opinion, and a list of 801
diseases derived by the commonest diagnoses
encountered in primary care (Finley et al., 2018) and
the diseases most often associated with in-hospital
death (Kellett and Deane, 2007).
Machine learning was then applied to
automatically classify the headings of web pages
related to the symptoms and diseases to the classes
seen above. This was done by using the following
functions:
• Url_Generator (k, n) uses a Google
TM
API to
retrieve n URLs of keyword k (e.g., a
symptom). For each symptom and disease, 40
URLs were retrieved.
HEALTHINF 2023 - 16th International Conference on Health Informatics
386

• BaseScraper (URL) takes each URL and
extracts all <h> headings.
• MachineLearner uses a TensorFlow
1
algorithm to create an AI model that allocates
headings to classes. TensorFlow is an open
source library for numerical computation and
large-scale machine learning. It allows to create
dataflow graphs—structures that describe how
data moves through a graph, or a series of
processing nodes. Each node in the graph
represents a mathematical operation, and each
connection or edge between nodes is a
multidimensional data array, or tensor (Abadi
et al., 2016). The AI model has been trained
with 1500 headings manually allocated to
different classes, reaching a ~ 85% precision.
• Sorter uses the AI model to classify headings
by indicating the probability a heading belongs
to a class. It uses the TextVectorization()
function, provided by the Keras framework
2
,
to transform text into a vector by also removing
capital letters and punctuation to avoid similar
words counted as different vectors.
As a last step, for each symptom or disease, the 40
web pages indicated by Url_Generator were
downloaded. The HTML contents, related to the
various headings, were extracted, using the DOM
3
of
the HTML page, and stored in a DB. The most fitting
web information, for each symptom/disease section,
is chosen based on:
• Information Relevance
The proximity of the symptom/disease with
the title of the page, S
c
, is computed as the
maximum of the cosine of similarity between the
symptom/disease and its synonyms (A) and the
title of the page (T), as follows:
𝑆
(
𝐴,𝑇
)
=𝑚𝑎𝑥
∑
∙
∑
∑
(1)
where A
i
and T
i
are the occurrences of the
same word present in the two texts and n is the
number of words present in A and T.
The symptom/disease occurrence index,
I
occ
, is computed as the maximum of the ratio
between the average occurrences of the
symptom/disease and its synonyms (A) and the
number of occurrences of the most frequent word
1
https://www.tensorflow.org/
2
https://keras.io/
in the page (P), as follows:
𝐼
(
𝐴,𝑃
)
=𝑚𝑎𝑥
(
∑
)
(
)
(2)
For improved results, we have applied a
stemming process to all words and we have
evaluated the similarities between words by
using the normalized Levenshtein distance
(Yujian and Bo, 2007).
• Information Quality
The quality of a web page P is computed by
counting the meta data of the page that can be
associated to the information quality (Alfano et
al., 2021; WHO, 2003; Eysenbach, 2002) and
grouping them in four categories:
o Temporal indicators T(P) (Last-Modified,
revised, PublishDate, ...);
o Spatial indicators S(P) (og:email,
og:phone_number, og:street-address, ...);
o Descriptive indicators D(P) (abstract,
summary, description, og:description, …);
o Author indicators A(P) (author,
citation_author, …).
o A fifth indicator O(P) refers to the most
popular health web sites.
The Information Quality, Iq, is then computed as
follows:
𝐼
(
𝑃
)
=
()∙()∙()∙()∙()
(3)
• Language Complexity
The Language Complexity, L
c
of a web page P, is
computed with the following formula:
𝐿
(
𝑃
)
=
∑
(
)∙
∑
(4)
where W
i
are the words of a text P, WF(W
i
) is
the Word Familiarity, i.e., the number of Google
results of W
i
(Alfano et al., 2021; Kloehn et al.,
2018, Leroy et al., 2016), and A
i
are the occurrences
of W
i
.
The most fitting information is computed by using
the following weighted formula:
𝐹𝑖𝑡𝐼𝑛𝑓𝑜 = 𝛼 ∙ 𝑆
+ 𝛽∙𝐼
+𝛾∙𝐼
+ 𝛿∙𝐿
(5)
Where α + β + γ + δ = 1 and allow to differently
weigh the information relevance, information quality
3
https://en.wikipedia.org/wiki/Document_Object_Model
Intelligent Provision of Tailored, Easily Understood, and Trusted Health Information for Patient Empowerment
387
and language complexity. A Support Vector Machine
(SVM, Cortes and Vapnik, 1995) has been trained
with human classified web pages to provide the best
combination of the weights and then the most
appropriate information for each section.
4 INTELLIGENT EMPOWERING
AGENT
The AI engine, presented in the previous section, has
been implemented as part of an Intelligent
Empowering Agent (IEA) that provides health
information tailored to the users’ needs, which is
intelligible, current, accurate, trustworthy, valuable,
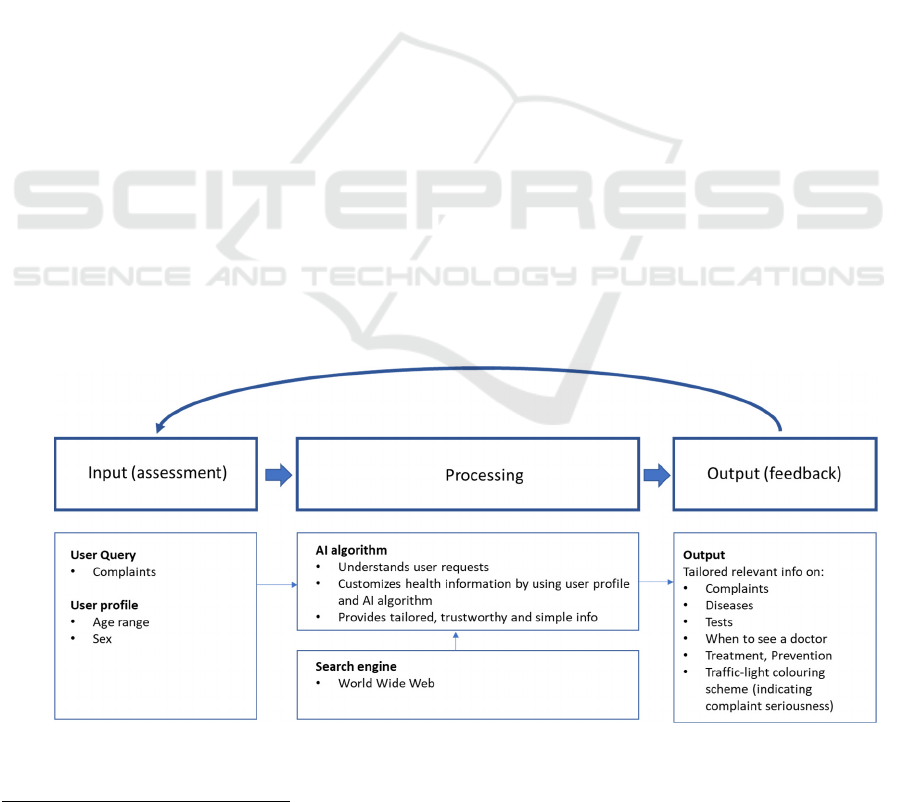
and usable. The IEA model is shown in Fig. 2. Its
components have been described in detail (Alfano et
al., 2022) and can be summarized as follows:
a. User Query. The user selects a complaint from a
list or directly enters it as free text.
b. User Profile. The user provides some
information about him/her (currently age range
and sex).
c. Search Engine. The search engine retrieves the
top 40 Google results for each symptom/disease.
d. AI Algorithm. The AI algorithm uses the AI
model shown above to select the health
information according to following criteria:
o Custom Information, to provide users with
tailored content for the symptom/disease of
interest, organized in sections.
o Information Quality, to provide users with
current, accurate, trustworthy, and
unambiguous information.
o Language Complexity, to provide users
with information that they can easily
understand.
e. Output Presentation. Tailored relevant health
information is provided on complaints, diseases,
medical tests, when to see a doctor, treatment,
prevention, and scientific articles according to
the section headings presented above. The
scientific-articles section uses a PubMed
TM4
API
to retrieve the most relevant articles on the topic
of interest.
A “traffic-light” colouring coding (i.e., red,
amber, or green), that implies the need for an
urgent consultation with a healthcare
professional, is also provided.
In an IEA prototype, the Conversational Health
Agent for Person Empowerment (CHAPE -
http://cohealth.ivi.ie/chape/), users input their age and
sex; CHAPE then provides a list of possible
complaints that can be easily understood, such as pain
or discomfort, breathlessness, and weakness or
fatigue. Depending on the complaint selected and the
user’s profile characteristics, a further sub-list of
possibly related complaints is presented, to help
define the primary complaint more precisely (Fig. 3).
Alternatively, the user can directly type in any
complaint in a free text area.
Figure 2: IEA model.
4
https://pubmed.ncbi.nlm.nih.gov/
HEALTHINF 2023 - 16th International Conference on Health Informatics
388
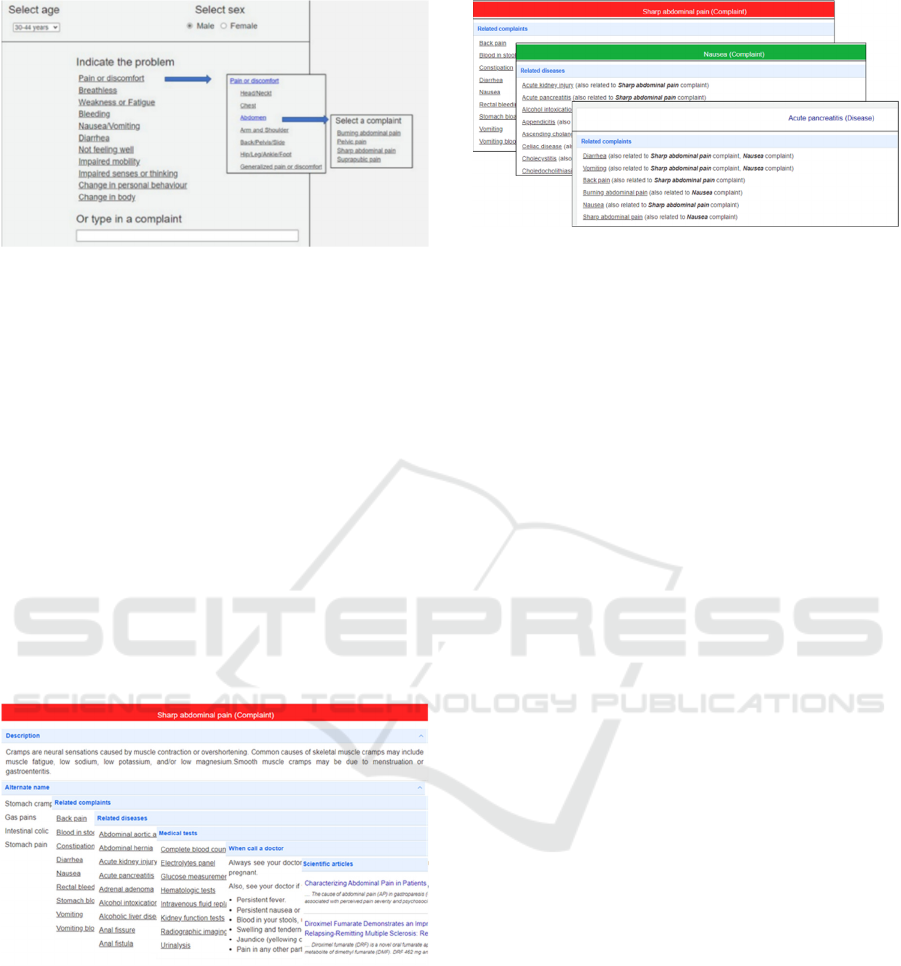
Figure 3: CHAPE interface allows users to specify their
complaints in an easy and natural way.
An information window is then displayed (Fig. 4)
and it contains:
• Complaint name with a background colour
(red, amber, or green), which indicates the
health risk.
• Complaint description.
• Alternate names of the complaint.
• Related complaints.
• Disease(s) associated with the complaint.
• Tests commonly used to further define the
complaint.
• When to see a doctor
• Treatment.
• Prevention.
• Scientific articles.
Figure 4: Output window containing information about the
searched element.
When a related complaint, disease, or test is clicked
on, a new information window for that element is
opened. The list of related complaints, diseases and
tests of the new window is ordered so that the
elements that are in common with the previous
searches are shown first (Fig. 5). This further
customizes the provided information by following the
user search path.
Figure 5: Related complaints and diseases are ordered by
their correlation with previous searched elements.
Some subjective tests have been carried out to
assess the effectiveness of the IEA in terms of
usability, user experience and perceived value
(Alfano et al., 2022). In terms of usability, most
respondents found CHAPE interface clear and helpful
in identifying health information about complaints,
diseases, and tests. In terms of user experience, most
respondents could better understand their complaints
and related diseases and tests. In terms of perceived
value, the majority of respondents found that CHAPE
would improve communication with their doctors.
Expanding the user profile and improving the
system’s interaction interface were the main
recommendations.
5 CONCLUSIONS
This paper shows how the use of AI in a responsible
way may help empower a person/patient better
manage their health and wellbeing. It presents an AI
engine that extracts health content from the Web to
provide the user with health information that is
relevant, trustworthy, and easy to understand. The AI
engine powers a prototype Intelligent Empowering
Agent (IEA) that dialogues with user in simple
language and provides tailored, trustworthy
information on symptoms and diseases, which help
users to form evidence-based opinions on health
matters that concern them. To our best knowledge,
this is the first attempt to create an intelligent
empowering agent that exploits the potential of AI
and the vast amount of health information available
on the Web to facilitate comprehension and action on
general complaints/diseases.
Intelligent Provision of Tailored, Easily Understood, and Trusted Health Information for Patient Empowerment
389

6 FUTURE
RESEARCH/DIRECTIONS
Although third party subjective assessments are
encouraging, the user profile and the system
interaction need to be improved. To this end, the user
interface is being provided with a graphical
representation of the body, for complaint
identification and location, and more user profile
information, such as gait, body type, nutritional
status, comorbidities, are being added. Complaints
and diseases are being associated with Concept
Unique Identifiers (CUI) of the Unified Medical
Language System (UMLS)
9
to map them to standard
terms taken from medical-term classifications such as
ICD-9
10
, ICD-10
11
, or SNOMED
12
. How information
is gathered and filtered out will be improved and
explicitly explained to improve trustworthiness.
Although user input is anonymous, users will be
provided with an option to grant or withdraw
informed consent to use their data. Finally, the agent
is going to be tested on a wider demographic.
ACKNOWLEDGEMENTS
This work was supported, in part, by Science
Foundation Ireland grant 13/RC/2094_P2 and co-
funded under the European Regional Development
Fund through the Southern & Eastern Regional
Operational Programme to Lero - the Science
Foundation Ireland Research Centre for Software
(www.lero.ie). Thanks to Yvan Pannefieu, from
ESEO Grand École d'Ingénieurs, for his contribution
on the machine learning algorithm for the extraction
and classification of HTML headings.
REFERENCES
Abadi, M. et al. (2016). TensorFlow: A System for Large-
Scale Machine Learning. Proc. of 2th USENIX
Symposium on Operating Systems Design and
Implementation (OSDI ’16). https://doi.org/
10.5555/3026877.3026899.
Alfano, M., Kellett, J., Lenzitti, B., Helfert, M. (2022).
Characteristics and Subjective Evaluation of an
Intelligent Empowering Agent for Health Person
Empowerment. Studies in health technology and
informatics, 299, 177–182. https://doi.org/10.3233/
SHTI220979.
9
https://www.nlm.nih.gov/research/umls/index.html
10
https://www.cdc.gov/nchs/icd/icd9cm.htm
Alfano, M., Lenzitti, B., Taibi, D., Helfert, M. (2021). On-
Line Retrieval of Health Information Based on
Language Complexity, Information Customization and
Information Quality. In Ziefle M., Guldemond N.,
Maciaszek L.A. (eds) Information and Communication
Technologies for Ageing Well and e-Health.
ICT4AWE 2020. Communications in Computer and
Information Science, vol 1387. Springer, Cham, 2021.
https://doi.org/10.1007/978-3-030-70807-8_1.
Alfano, M., Lenzitti, B., Taibi, D., Helfert. (2020).
Language Complexity in On-line Health Information
Retrieval. In: Ziefle M., Maciaszek L. (eds) Information
and Communication Technologies for Ageing Well and
e-Health. ICT4AWE 2019. Communications in
Computer and Information Science, vol 1219, 2020,
Springer, Cham. https://doi.org/10.1007/978-3-030-
52677-1_5
Alfano, M., Lenzitti, B., Taibi, D., Helfert, M. (2019).
Provision of Tailored Health Information for Patient
Empowerment: An Initial Study. In Proceedings of the
20th International Conference on Computer Systems
and Technologies (CompSysTech ’19). Association for
Computing Machinery, New York, NY, USA, 213–
220. https://doi.org/10.1145/3345252.3345301.
Bodolica, V., Spraggon, M., (2019). Toward patient-
centered care and inclusive health-care governance: a
review of patient empowerment in the UAE. Public
Health, 169(971), 114–124. https://doi.org/10.1016/
j.puhe.2019.01.017
Cerezo, P. G., Juvé-Udina, M. E., Delgado-Hito, P. (2016).
Concepts and measures of patient empowerment: A
comprehensive review. Revista Da Escola de
Enfermagem. https://doi.org/10.1590/S0080-6234201
60000500018
Cortes, C. and Vapnik, V. (1995). Support-Vector
Networks. Machine Learning, 20, 273-297.
http://dx.doi.org/10.1007/BF00994018
Davenport T, Kalakota R. (2019). The potential for
artificial intelligence in healthcare. Future Healthc J.
6(2):94-98. https://doi.org/10.7861/futurehosp.6-2-94.
European Health Parliament. (2017). Patient empowerment
and centredness. https://www.healthparliament.eu/
patient-empowerment-centredness/#:~:text=There%
20is%20a%20widespread%20consensus,expanding%2
0burden%20of%20chronic%20diseases.
Eysenbach G., Powell, J., Kuss, O., Sa, E.R. (2002).
Empirical studies assessing the quality of health
information for consumers on the world wide web: a
systematic review. JAMA J. Am. Med. Assoc,.
287(20), pp. 2691–2700, 2002. https://doi.org/
10.1001/jama.287.20.2691.
Fast E., Horvitz, E. (2017). Long-term trends in the public
perception of artificial intelligence. In Proceedings of
31st AAAI Conference on Artificial Intelligence, AAAI
2017, pp. 963–969, January 2017. https://doi.org/
10.48550/arXiv.1609.04904
11
https://www.cdc.gov/nchs/icd/icd-10-cm.htm
12
https://www.snomed.org/
HEALTHINF 2023 - 16th International Conference on Health Informatics
390

Finley C.R., Chan D.S., Garrison S., Korownyk C., Kolber
M.R., Campbell S., Eurich D.T., Lindblad A.J.,
Vandermeer B., Allan G.M. (2018). What are the most
common conditions in primary care? Systematic
review. Canadian Family Physician 2018;64:832-840.
Finney Rutten L.J., Blake, K.D., Greenberg-Worisek, A.J.,
Allen, S.V., Moser, R.P., Hesse, B.W. (2019). Online
Health Information Seeking Among US Adults:
Measuring Progress Toward a Healthy People 2020
Objective. Public Health Reports. 2019;134(6):617-
625. https://doi.org/10.1177/0033354919874074.
Fox, S., Duggan, M.: Health Online 2013, Pew, Research
Center’s Internet & American Life
Project (2013). http://www.pewinternet.org/2013/01/15/
health-online-2013/
Fumagalli, L. P., Radaelli, G., Lettieri, E., Bertele’, P.,
Masella, C. (2015). Patient Empowerment and its
neighbours: Clarifying the boundaries and their mutual
relationships. Health Policy. 119(3), 384–394.
https://doi.org/10.1016/j.healthpol.2014.10.017
AI HLEG. (2019). Ethics guidelines for trustworthy AI.
Retrived 22 September 2022 from https://digital-
strategy.ec.europa.eu/en/library/ethics-guidelines-trust
worthy-ai.
Iatraki, G., Kondylakis, H., Koumakis, L., Chatzimina, M.,
Kazantzaki, E., Marias, K., & Tsiknakis, M. (2018).
Personal Health Information Recommender:
implementing a tool for the empowerment of cancer
patients. Ecancermedicalscience, 12, 1–11.
https://doi.org/10.3332/ecancer.2018.851.
Jiang F, Jiang Y, Zhi H, et al. (2017). Artificial intelligence
in healthcare: past, present and future. Stroke and
Vascular Neurology 2017;2: e000101. https://doi.org/
10.1136/svn-2017-000101.
Kellett, J., & Deane, B. (2007). The diagnoses and co-
morbidity encountered in the hospital practice of acute
internal medicine. European Journal of Internal
Medicine, 18(6), 467–473. https://doi.org/10.1016
/j.ejim.2007.02.019.
Kloehn N. et al. (2018). Improving consumer understanding
of medical text: development and validation of a new
subsimplify algorithm to automatically generate term
explanations in English and Spanish. J. Med. Internet
Res. 20(8), e10779. https://doi.org/10.2196/10779
Kondyalkis, H., Koumakis, L., Tsiknakis, M. (2013). Smart
Recommendation Services in Support of Patient
Empowerment and Personalized Medicine. In
Multimedia Services in Intelligent Environments.
Smart Innovation, Systems and Technologies (Vol. 24).
Springer Cham. https://doi.org/10.1007/978-3-319-
00372-6.
Leroy G. et al. (2012). Improving perceived and actual text
difficulty for health information consumers using semi-
automated methods. In: AMIA Annual Symposium
Proceedings, pp. 522–531
MacBryde CM, Blacklow RS, eds. (1970). Signs and
Symptoms: Applied Pathologic Physiology and
Clinical Interpretation. 5th edn. Philadelphia:
Lippincott, 1970. 27.
Responsible Artificial Intelligence Institute. https://
www.responsible.ai/faq (accessed on 10th September
2022).
Snowdon, A. (2020). Digital health: A Framework for
Healthcare Transformation. HIMSS. Retrieved
September 2022 from https://www.himss.org/resour
ces/digital-health-framework-healthcare-transformati
on-white-paper.
Snowdon, A., Schnarr K., Alessi, C. (2014). It’s All About
Me : The Personalization of Health Systems. Retrieved
April 2022 from https://www.ivey.uwo.ca/media/
3467873/its-all-about-me-the-personalization-of-heal
th-systems.pdf.
World Health Organization. (2021). Ethics and governance
of artificial intelligence for health: WHO guidance.
Geneva, 2021.
World Health Organization. (2016). Framework on
integrated, people-centred health services: Report by
the Secretariat. World Health Assembly, (A69/39),
April 2016, pp. 1–12. https://apps.who.int/g
b/ebwha/pdf_files/WHA69/A69_39-en.pdf.
World Health Organization. (2003). Improving Data
Quality: A Guide for Developing Countries. 2003. pp.
1–74.
Yujian, L., Bo, L. (2007). A Normalized Levenshtein
Distance Metric," in IEEE Transactions on Pattern
Analysis and Machine Intelligence, vol. 29, no. 6, pp.
1091-1095, June 2007. https://doi.org/10.1109/T
PAMI.2007.1078.
Intelligent Provision of Tailored, Easily Understood, and Trusted Health Information for Patient Empowerment
391
