
Towards Specification of Medical Processes According to International
Standards and Semantic Interoperability Needs
Tanel S
˜
oerd
1
, Kristian Kankainen
2 a
, Gunnar Piho
1 b
, Toomas Klementi
1 c
and Peeter Ross
2 d
1
Department of Software Science, TalTech, Akadeemia Str. 15A, Tallinn, Estonia
2
Department of Health Technologies, TalTech, Akadeemia Str. 15A, Tallinn, Estonia
Keywords:
Process Meta-Model, Federated Interoperability, Clinical Knowledge Modelling, Electronic Health Record,
Healthcare Workflow.
Abstract:
Models of healthcare processes and workflows to support the continuity of health care are an essential research
topic in medical informatics. This research topic is driven by the necessity to enable systems (including se-
mantic) interoperability, to see the consistency of clinical data recorded in electronic health records (EHR)
and to understand retrospectively the clinical pathways that led to these data. We propose a process meta-
model and evaluate its usability by modelling the healthcare concepts and models from the ISO 13940 (system
of concepts to support continuity of care) standard. Our meta-model is developed according to the software
design patterns principles, enabling the formal specification of knowledge in a machine-readable format and
preserving the history of these specifications. Our work contributes to the federated interoperability of health-
care information systems (healthcare enterprise applications), utilising executable meta-models that can map
healthcare data at the semantic (medical knowledge) level, even at run-time.
1 INTRODUCTION
Health care is evolving from episodic (symptom-
triggered) health care towards a continuous, preven-
tive healthcare approach (EIC, 2022). There is a need
for continuous and unified access to health data not
limited to a particular episode of a specific health case
at a particular health institution (health data silos).
A significant effort has been made to store medical
records electronically (EHR). However, the stored in-
formation does not always reveal the context or the
reason behind taking a blood sample, administering a
drug or using a particular treatment.
The current practice of EHR makes it difficult for
healthcare workers to determine clinical data consis-
tency and understand clinical pathways, especially in
secondary use cases (e.g. medical science and clin-
ical research) of EHRs, where data users know nei-
ther the patient nor the context, as physicians do in
EHR primary use cases (diagnosis and clinical care).
While governments and society constantly push hos-
a
https://orcid.org/0000-0002-0551-927X
b
https://orcid.org/0000-0003-4488-3389
c
https://orcid.org/0000-0002-8260-526X
d
https://orcid.org/0000-0003-1072-7249
pitals to reduce costs and improve efficiency, health-
care costs rise yearly. One possible cost-reducing
strategy is wise health data digitalization towards
beneficial secondary usage (PWC, 2009). However,
this task is complicated because information systems
in healthcare institutions have semantically heteroge-
neous data models and approximately 80% of medical
data are unstructured (Negro-Calduch et al., 2021).
According to Chen et al., three architectural ap-
proaches to enterprising interoperability exist: inte-
grated (based on a common format), unified (based
on a common standard) and federated (no common
format; instead, parties accommodate each other on
the fly) (Chen et al., 2008). We rule out integrated
and unified approaches because of historical soft-
ware development; most medical institutions use their
in-house-specific standards or at least in-house ver-
sions of national and international standards. It is
common knowledge that software systems developed
by independent parties tend to be semantically het-
erogeneous even when based on the same standards
(Halevy, 2005; Mocan et al., 2009). This heterogene-
ity is because standards always have room for inter-
pretation. The redesign and redevelopment of these
systems is too risky and costly. Instead, we strive
for the federated approach, where (semantic) interop-
160
Sõerd, T., Kankainen, K., Piho, G., Klementi, T. and Ross, P.
Towards Specification of Medical Processes According to International Standards and Semantic Interoperability Needs.
DOI: 10.5220/0011687900003402
In Proceedings of the 11th International Conference on Model-Based Software and Systems Engineering (MODELSWARD 2023), pages 160-167
ISBN: 978-989-758-633-0; ISSN: 2184-4348
Copyright
c
2023 by SCITEPRESS – Science and Technology Publications, Lda. Under CC license (CC BY-NC-ND 4.0)

erability of systems (Ciampi et al., 2013; Tu et al.,
2016) is achieved by adjudicating each party’s seman-
tic inconsistencies continuously. For this, we are de-
veloping ABC4HEDA (Archetype-based Computing
for Health Data), which is a Single Underlying Model
(Meier et al., 2019) and software that enables Elec-
tronic Health Record (EHR) management in a trans-
parent, secure and semantically coherent way. By
archetype, we mean a business archetype that “is a
primordial thing that occurs consistently and univer-
sally in business domains and business software sys-
tems” (Arlow and Neustadt, 2003), not the archetype
term as utilized by the openEHR (Beale, 2002) and
ISO13606 (ISO, 2019) standards.
ABC4HEDA aims to contribute to more interop-
erable and consistent healthcare data. It is developed
based on software engineering best practices and pro-
poses a theoretically ”standard-ignorant” approach
to the federated semantic interoperability of clini-
cal data models. By “standard-ignorant”, we mean
an approach similar to computing, infrastructure and
platform-ignorant (independent) approaches, where
no unified standard is defined and third parties can
specify the standards, taxonomies or terminologies
they use declaratively. This paper evaluates whether
the process meta-model in ABC4HEDA is applicable
in the healthcare domain by testing whether it can be
used to declaratively specify the healthcare process of
the ISO 13940 (system of concepts to support conti-
nuity of care) standard (ISO, 2015).
Our approach has been explained in (Piho et al.,
2010a; Piho et al., 2010c; Piho et al., 2011; Piho
et al., 2012; Piho et al., 2014), evaluated in real-life
applications (Piho et al., 2010b) and analysed on the
basis of HL7 RIM (reference information model) and
openEHR RM (reference model) (Piho et al., 2015) as
well as LOINC (Raavel et al., 2022) and HL7 FHIR
(Randmaa et al., 2022) interoperability tests.
The rest of this paper is structured as follows. In
Section 2, we explain the methodology we have uti-
lized. Sections 3 and 4 briefly overview the ISO
13940 standard and Process Archetype Pattern, re-
spectively. Section 5 specifies the healthcare pro-
cess from the ISO 13940 standard in the domain-
specific language based on the Process Archetype Pat-
tern meta-model of ABC4HEDA. We analyse and dis-
cuss the presented results in Section 6 and conclude
the paper in Section 7.
2 METHODOLOGY
Consider a situation where a clinical guideline speci-
fies how and in which order the particular healthcare
activities should be performed. And consider that
medical science is evolving and the guideline is re-
vised. Based on this revision, the healthcare institu-
tion has to change its practices; therefore, it is neces-
sary to also change the information system to support
the new guideline. However, as the historical data are
based on the old guidelines, the new system must now
support both versions.
Instead of convening a team of developers to
implement such changes to the information system,
in the ABC4HEDA approach, changes are speci-
fied declaratively while the application is running.
Changes can be rolled back, updating the source code
is not required and the application does not need to
be restarted for healthcare providers to proceed with
work and utilise the new guideline.
ABC4HEDA makes use of syntax, semantics
and pragmatics-based three-level modelling (Bjørner,
2006). All data and knowledge are stored in an
archetype and archetype pattern(A&AP)-based model
(syntax – what we write) (Piho, 2011). These
archetypes and archetype patterns have been designed
(Piho et al., 2010c) according to the Zachman Frame-
work (Zachman, 1987) by asking (and answering)
who (involved actors and their roles), what (products
and services), when (date and time), where (location),
why (rules) and how (processes) questions. This paper
evaluates the business process (how) meta-model.
The A&AP model forms a domain-specific lan-
guage (DSL) (Fowler, 2010) for specifying (not pro-
gramming) all existing and future developed medical
knowledge (taxonomies, ontologies, standards, pro-
tocols, etc.) declaratively (even at run-time) in an un-
ambiguous and machine-readable format (semantics
– what we mean). This DSL is to be applied in a par-
ticular healthcare information system for specifying
(pragmatics – how we use) the healthcare terms and
concepts in use in that particular healthcare organisa-
tion.
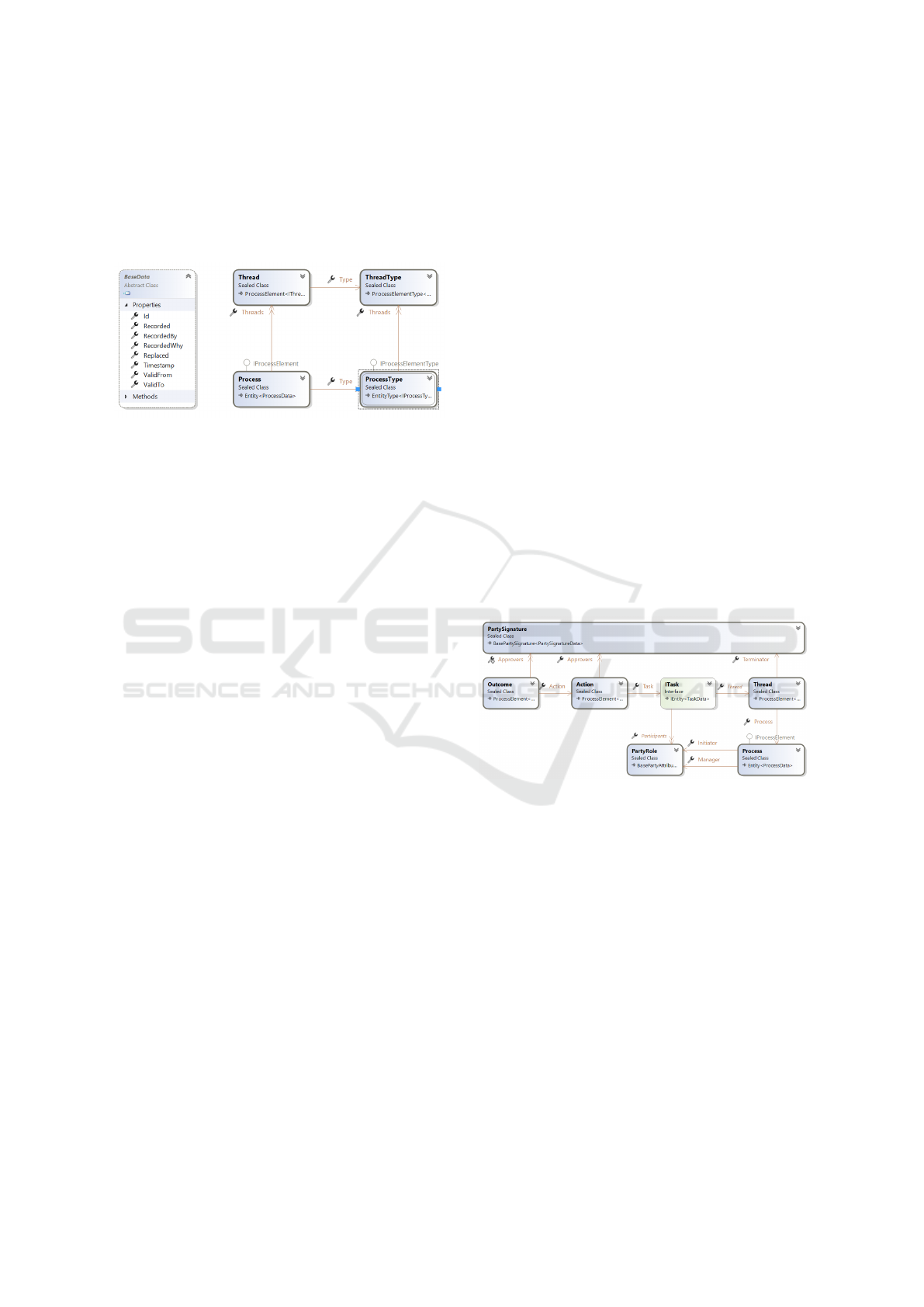
The two principal patterns in use – the item de-
scription pattern (Coad, 1992) and the evolving sys-
tems pattern (Oei et al., 1994) – make our meta-model
dynamically evolvable and semantically interopera-
ble despite model changes. In line with the first pat-
tern, every concept in the ABC4HEDA meta-model
has a type that is specifiable during run-time (Fig-
ure 1, right). And in accordance with the second
pattern, meta-data is stored for the transparency and
history preservation purposes of the items (Figure 1,
left). So, in case of a mistake or an error during a
change in requirements, it is possible to trace and roll
back the system. Consequently, ABC4HEDA sup-
ports second-order evolution (Oei et al., 1994) in such
a way that changes in semantics (meaning of data,
Towards Specification of Medical Processes According to International Standards and Semantic Interoperability Needs
161
knowledge about data), which would generally re-
quire a change in meta-models (e.g. database layout,
classes in software), are converted to first-order evo-
lution of data because both the data and their seman-
tics (meaning, knowledge) are presented in the same
manner.
Figure 1: Evolving systems (left) and item description.
3 ISO 13940:2015
The ISO 13940:2015 standard “defines a system of
concepts for different aspects of the provision of
health care” (ISO, 2015, p. 1). It states that the
core business of health care is the interaction be-
tween the patient and healthcare actors. The stan-
dard uses UML (Unified Modelling Language) dia-
grams to define around 150 concepts and their in-
terrelations across eight domains: healthcare actors,
healthcare matters, activities, processes, healthcare
planning, time, responsibilities, and information man-
agement. The standard does not have any regulatory
impact on care delivery, but rather gives a conceptual
basis for describing both the content and the context
of healthcare services. We use the standard as a com-
mon healthcare domain model, which, according to
the software triptych principle, “from domain model
via requirements to the software” (Bjørner, 2006) is
wise to use whenever the requirements for informa-
tion systems are analysed. A review (Kankainen,
2021) analysing how the ISO 13940 concepts have
been understood and applied in literature found two
relevant use cases of the standard. The first use case
(Oniki et al., 2014) collected information contexts
(discharge diagnosis, cause of death, complication of
surgery, problem list, etc.) from the standard and used
them in data transformation; the same assertive in-
formation is displayed differently in individual con-
texts. The work discusses the importance of having
an ‘implementation layer’, which means that the logi-
cal models are not compiled directly into the artefacts
used in an implemented system; instead, ‘implemen-
tation models’ are used as a buffer between the logi-
cal models and system implementation. Such a tech-
nique allows context-dependent transformations of
the assertive information and implementation-specific
transformations for performance optimisation. The
second use case (Garc
´
ıa-de Le
´
on-Chocano et al.,
2015) exploited the fact that the contexts enumerated
in the ISO 13940 standard hold universally across cul-
tural, national and organisational borders. Contextu-
alising their data quality metrics with the ISO 13940
standard enabled them to replicate their methodology
at a cross-organisational level.
4 BUSINESS PROCESS
ARCHETYPE PATTERN
A large part of the ABC4HEDA model is based
on business archetypes (Arlow and Neustadt, 2003),
which allow us to respond to all the questions in
the Zachman framework. While Arlow & Neustadt
do not define an archetype pattern for business pro-
cesses explicitly, they describe how to manage re-
lationships between parties through a customer rela-
tionship management archetype. With some amend-
ments to their pattern, we have created the business
process archetype pattern (Figure 2) by generalising
their party relationship archetype (Piho, 2011).
Figure 2: Business process archetype pattern.
In a similar fashion to a film being a series of static
pictures, the process archetype pattern specifies the
processes’ dynamics through an ordered set of reports
and feedback from the process. More reports and/or
feedback give a better overview of the entire process
as a dynamic phenomenon. The same pattern can
be used for business process planning by replacing
actual reports and/or feedback with expected reports
and/or feedback. By comparing the actual with the
expected, we can monitor the adequacy of the plans.
The central part of our business process archetype
pattern is the task archetype (Figure.3). A task is a
party relationship between two party roles and allows
us to model multiple simultaneous roles, e.g. in terms
of a family member, a person can simultaneously be
a parent and a spouse, or a daughter and a sister.
This modelling approach combined with the afore-
MODELSWARD 2023 - 11th International Conference on Model-Based Software and Systems Engineering
162
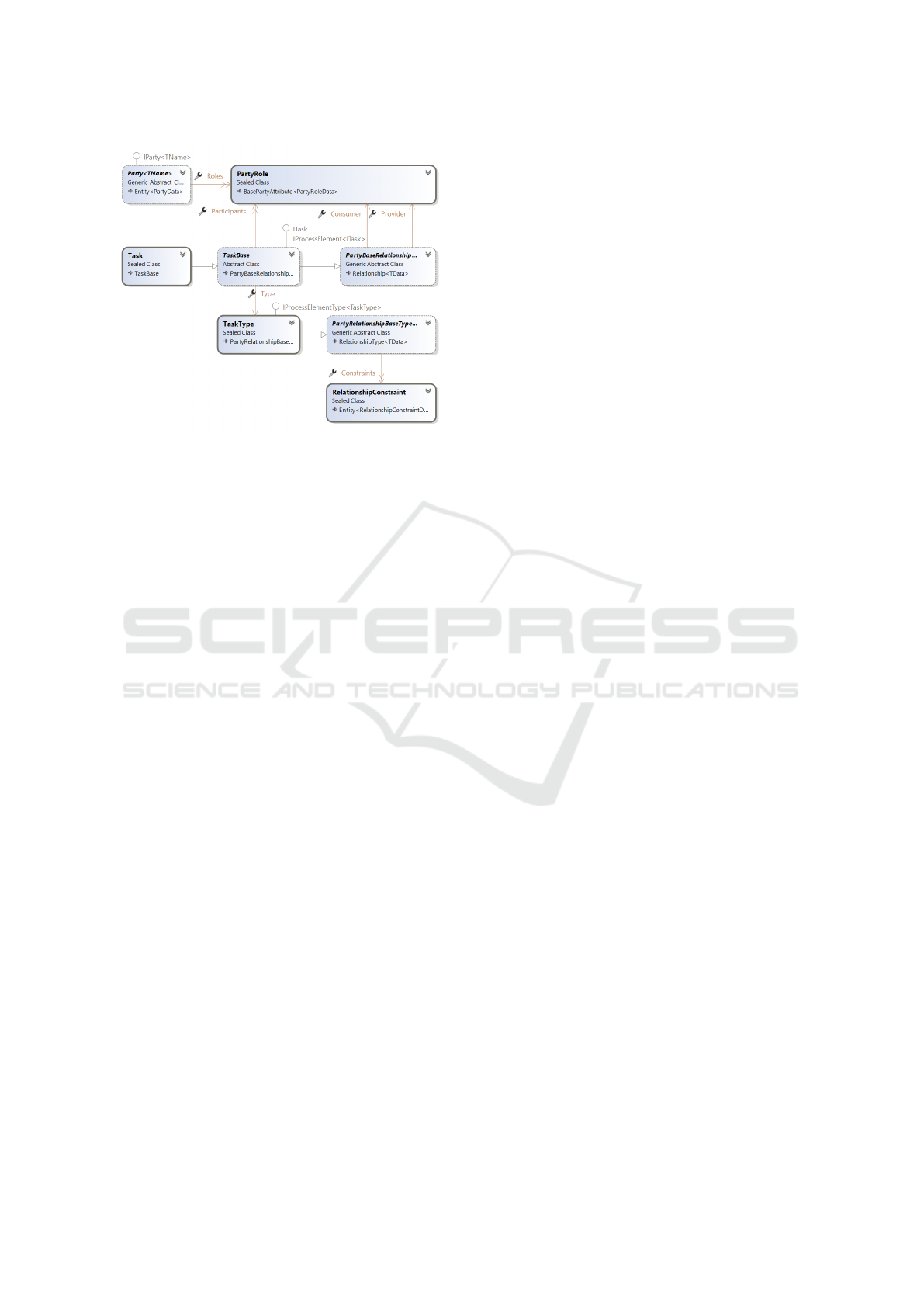
Figure 3: Task archetype.
mentioned patterns for item description and systems
evolution makes it possible to define new role and re-
lationship types at run-time. Additionally, it allows
us to keep information consistent in ABC4HEDA,
which, according to Lagos et al. (Lagos et al., 2018),
is a crucial aspect of information models and systems.
Tasks (e.g. an appointment) are grouped into
threads (e.g. patient’s clinical examinations to deter-
mine a possible diagnosis), and threads are grouped
into processes (e.g. a patient’s stay in hospital). A
task contains one or many actions (e.g. measuring
blood pressure), and each action may have one or
many outcomes (e.g. both systolic and diastolic value
of a blood pressure). All the process archetype el-
ements (process, thread, task, action and outcome)
have declaratively specifiable types that can be added
during run-time. For certain activities, business pro-
cesses often require approval that can only be given
by authorised parties. For example, Estonia has five
licences for providing various medical services under
the Health Care Services Organisation Act. Legal co-
ordination must take place between the parties, which
is made possible using the party signature archetype
(PartySignature). Finally, TaskRouting allows tasks
to be transferred between parties (e.g. a change in
treating physician).
5 SPECIFYING THE ISO 13940
SYSTEM OF CONCEPTS
In this section, we specify the concepts and relation-
ships from the ISO 13940 standard using the domain-
specific language of the ABC4HEDA meta-model de-
scribed above. Unified Modelling Language (UML)
object diagrams are used for visualisation. In the ob-
ject diagrams, the ABC4HEDA meta-model terms are
pictured as classes (types), and the ISO 13940 stan-
dard concepts are pictured as objects (type instances).
5.1 Specifying the Care Plan
The core of a patient’s healthcare process in ISO
13940 is the dynamic, personalised care plan that
encompasses the activities, goals and objectives re-
lated to a health issue (Figure 4). The ’care plan’
is modelled as a Task in the ABC4HEDA business
process meta-model (domain-specific language). In
ISO 13940, multiple ’care plans’ can address multi-
ple ’health threads’, where a health thread is a defined
association between healthcare matters as determined
by one or more healthcare actors. In ABC4HEDA, we
model health threads as Thread. The ’care plan’ and
’health thread’ are organised by adding health threads
to the healthcare process and adding care plans to the
health thread. According to ISO 13940, the care plan
is the result of ’healthcare planning’ and it is ’health-
care activity management’ that changes the statuses of
healthcare activities in the care plan. In ABC4HEDA,
healthcare planning is a Process and a change in the
status of activities is modelled using the ActionSta-
tus. Care plans are applied by ’healthcare actors’ –
either organisations or persons participating in health
care. In ABC4HEDA, healthcare actors are defined
in terms of their roles (PartyRole) or signatures (Par-
tySignature). The healthcare process is set in motion
by a health issue identified by one or more health-
care actors. An example of a healthcare process is
a patient’s stay at a hospital until discharged. Dur-
ing the stay, the patient can undergo many ’health
threads’ (Thread). Each Thread is related to a spe-
cific problem that will be dealt with in hospital clinics
and centres. A ’referral’ in the ISO 13940 standard is
the movement of a ’healthcare commitment’ between
’healthcare professionals’. The same is accomplished
by TaskRouting in ABC4HEDA.
Activities in a care plan can be arranged to com-
ply with a ’clinical guideline’. The ISO 13940 stan-
dard describes a clinical guideline as a systemati-
cally developed statement designed to assist health-
care actors in making decisions about healthcare ac-
tivity related to specified health issues. Just like other
tasks (healthcare appointments), clinical guidelines
are modelled by specific types of activity (Action-
Type). These guidelines make up checklists for the
patient’s care path, similarly to Nan (Nan et al., 2015).
Additionally, a ’care plan’ can be based on a ’core
care plan’, which provides reusable content and struc-
ture for a specific set of circumstances. We model
core care plans as Threads specified by ThreadType in
Towards Specification of Medical Processes According to International Standards and Semantic Interoperability Needs
163
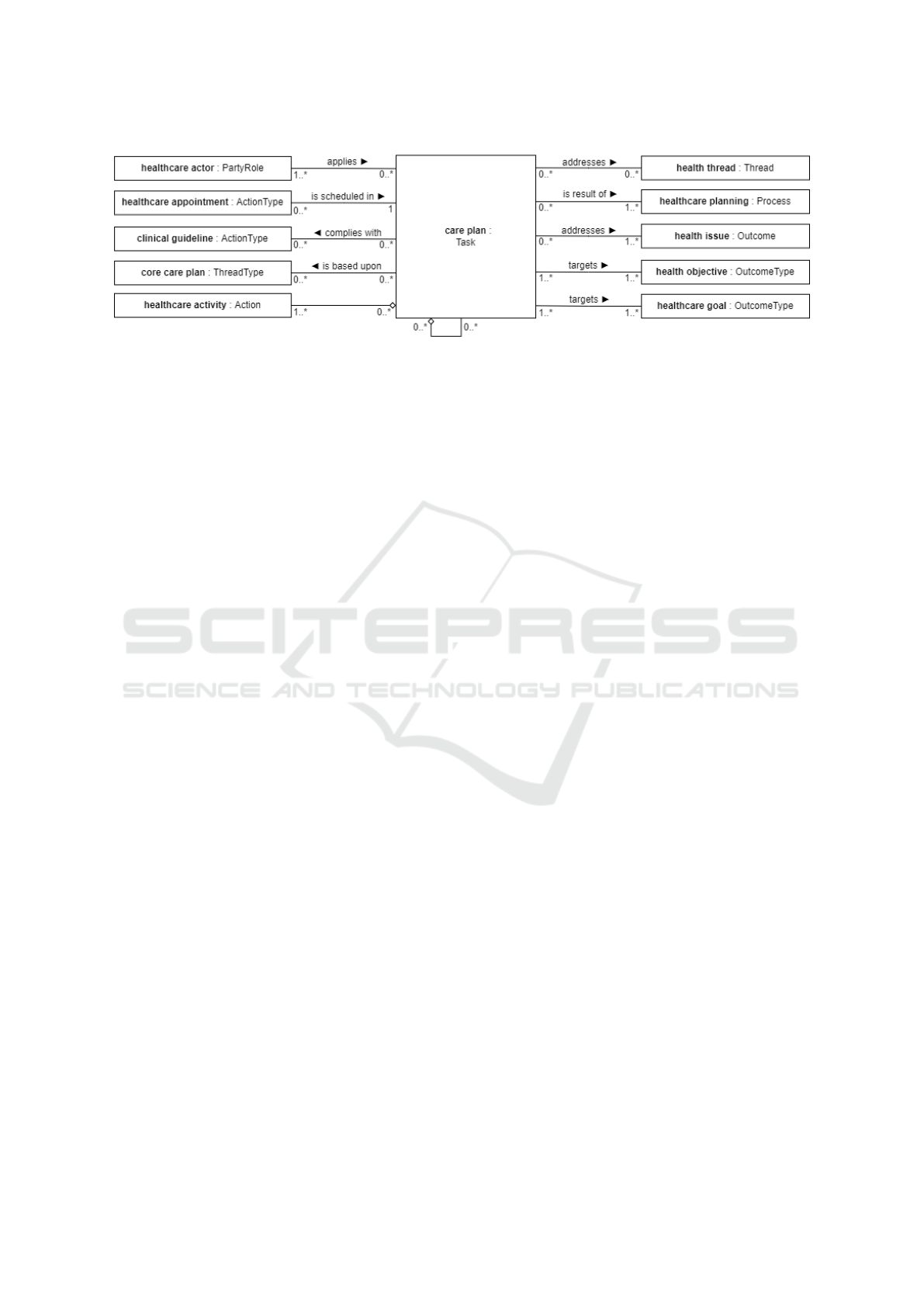
Figure 4: ISO 13940 care plan in ABC4HEDA domain-specific language.
the ABC4HEDA process model. A care plan aims to
fulfil a ’health objective’, and the activities it carries
out target ’healthcare goals’ that contribute to the ob-
jective. How the goals and objectives can be used for
evaluation is described below in the section on health-
care activities.
5.2 Modelling the Healthcare Process
ISO 13940 defines the ’healthcare process’ (Figure 5)
as transforming the patient’s health. It has an input
health state and an output health state. How the health
state can be observed and assessed is described in the
section on healthcare activities. The healthcare pro-
cess can be evaluated by ’healthcare process evalua-
tion’, where requirements are systematically assessed
against the healthcare processes. The ABC4HEDA
meta-models evaluate the compliance of the process
using RuleContext.
For each healthcare process, a ’healthcare man-
date’ is required. ISO 13940 defines this as a directive
based on either ’informed consent’ or ’legal authori-
sation’ and a ’healthcare actor’ accepting ’healthcare
commitment’. In the ABC4HEDA meta-models, par-
ties have legal capacity (PartyCapacity) to perform
specific activities.
The entire process model yields a holistic health
record, which is a data repository regarding both the
health and the health care of the patient. This health
record consists of entity types, along with entities.
Entity types are the planned treatment activities with
the expected results and entities are (immutable) pro-
tocols of correct Action and the associated Outcomes.
5.3 Modelling the Healthcare Activity
The healthcare activity model is shown in Figure 6.
The management of activities within the care plan
was detailed in the above care plan section and not
repeated here. In the ISO 13940 standard, a ’health-
care activity’ targets a ’healthcare goal’, just like the
care plan aims to meet the overall ’health objective’.
A healthcare activity is assessed by the healthcare
evaluation, which refers to the process of evaluat-
ing various aspects of healthcare operations. In our
ABC4HEDA meta-model, when there is a need to re-
view external evaluations or contracts, the rules can
indicate what is needed, and the context of the rules
(RuleContext) indicates what meets the desired goals
and what does not.
Previously, it was pointed out that different man-
dates are needed for the healthcare activities outlined
in the care plan. In this sense, a healthcare activity is
connected to a healthcare commitment. According to
ISO 13940, this refers to the party’s acceptance of a
healthcare mandate to which the healthcare mandate
is assigned. In order to begin any activity and to meet
that condition, the activities included in the Task re-
quire the approval (PartySignature) of both the origi-
nator and the recipient.
ISO 13940 also outlines ’automated health care’,
which is one type of Action (ActionType) initiated by
a responsible healthcare actor and thereafter delivered
by an automatic medical device. The actor as well
as the medical device both represent ’healthcare re-
sources’, as detailed in the next section. The health-
care activities provided to the patient require at least
one of these resources, and at least two parties are in-
volved in a patient’s health-related Task at any given
time.
5.4 Modelling the Healthcare Resource
Health care and its activities need resources (Figure
7). ’Healthcare personnel’ is modelled as Person and
the ’point of care’, i.e. the location at which direct
healthcare activities are performed, is an Organisa-
tionUnit. One shortcoming in the party archetype pat-
tern is that a Party can also be considered a resource
that is consumed or used during the process. As such,
it is likely that the addition of an abstract device to
meta-models will be necessary in the future in order
MODELSWARD 2023 - 11th International Conference on Model-Based Software and Systems Engineering
164
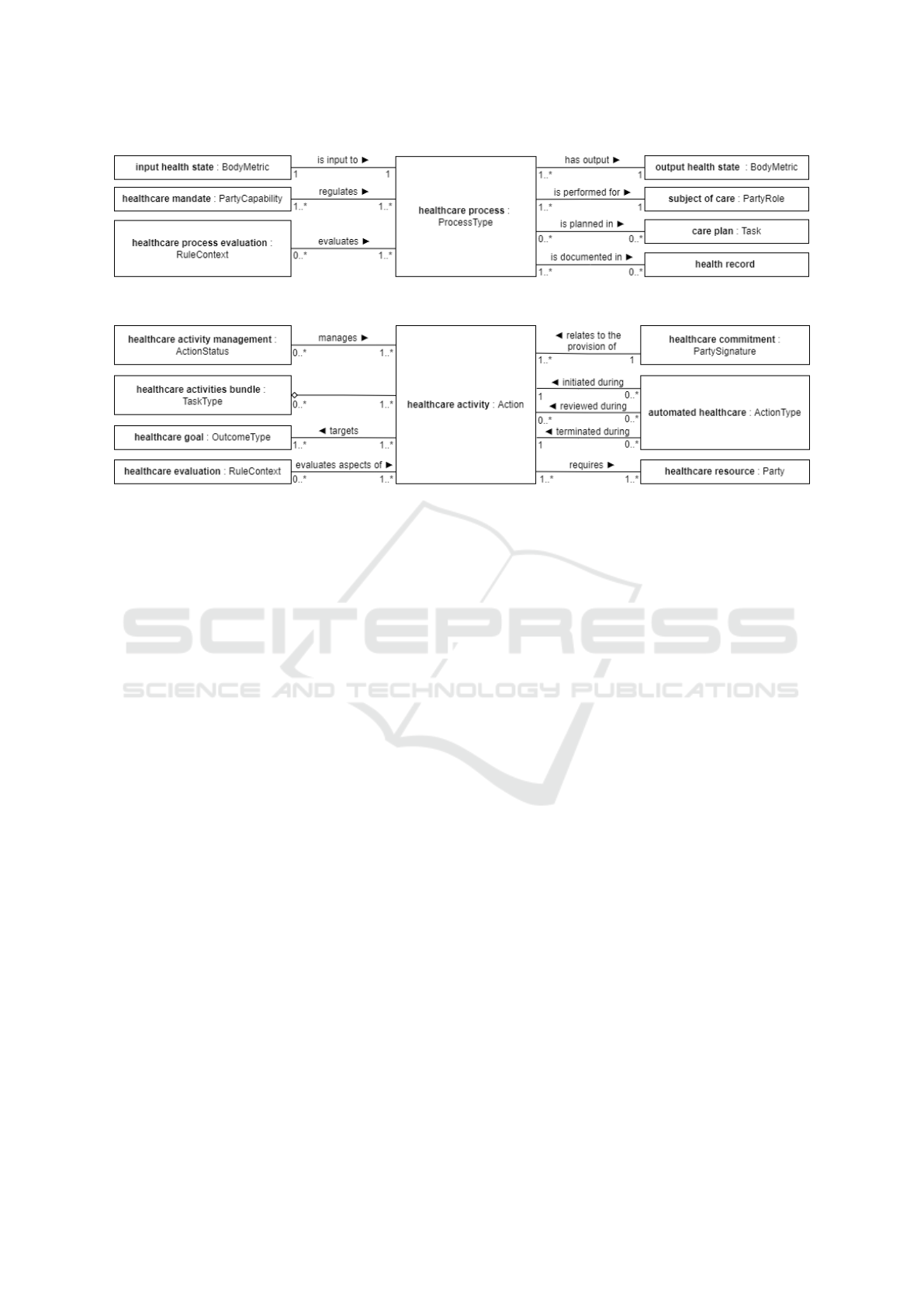
Figure 5: Model of healthcare process using ISO 13940 terms and ABC4HEDA entities.
Figure 6: Model of healthcare activity using ISO 13940 terms and ABC4HEDA entities.
to describe, for instance, automated medical devices.
Resource management and funding for health care
are shown in Figure 7, and both items needed to de-
scribe them are available in the meta-models. For ex-
ample, a Party is needed to fund healthcare resources,
and said Party may have a role in funding (PartyRo-
leType). In addition, the management of healthcare
resources can be performed by a specific type of Task
(TaskType).
6 DISCUSSIONS AND
CONCLUSION
In ABC4HEDA, around 120K lines of source code
have been written in C# programming language, and
45% of this code consists of automated unit and ac-
ceptance tests to ensure 100% code coverage. The ar-
chitecture and coding practices are clean and approx-
imately 12% of the code is pure POCO (Plain Old
CLR Object), which forms the computable domain
model for the A&AP. Approximately 3% of the code
implements a repository and unit of work patterns
for the platform-independent data-persistent infras-
tructure. The Entity Framework Core as an object-
relational mapper is in use. However, due to clean
code and a clean architecture approach, the mapping
can easily be replaced by another mapper, if neces-
sary. Approximately 40% of the code uses the latest
ASP.NET Core (also replaceable) and provides infras-
tructure and UI features for management and opera-
tion by allowing medical knowledge specifications to
be written in a declarative manner, therefore enabling
specification of medical standards & other commonly
used or custom-made specifications.
ABC4HEDA follows the federated approach to
the interoperability of systems without establishing
rules and protocols. This standard’s ignorance is
achieved by separating data and knowledge. Rather
than enforcing standards, ABC4HEDA allows clin-
ical knowledge to be specified declaratively at run-
time. By preserving the history of both data and
knowledge, the integrated systems may evolve inde-
pendently and safely.
We described how the ABC4HEDA meta-
model is capable of encoding terms from the ISO
13940:2015 (system of concepts to support continu-
ity of care) standard. The terms covered all domains:
healthcare actors, matters, activities, processes, plan-
ning, time, responsibilities, and information manage-
ment.
The necessary work behind the meta-model was
done by selecting the clinical guideline for a stroke
patient’s journey created during a design sprint at
North Estonia Medical Centre and devised by the
master’s students of Tallinn University of Technol-
ogy. Several treatment plans were outlined on the
patient’s journey, and the Estonian Health Insurance
Fund provided us with a more detailed description of
the treatment plans. Throughout the research, the pro-
cess model was validated by experts.
We evaluated the usability of the ABC4HEDA
meta-models and software using its domain-specific
language to specify the ISO 13940 terminology
declaratively. The ISO 13940 standard takes a
Towards Specification of Medical Processes According to International Standards and Semantic Interoperability Needs
165
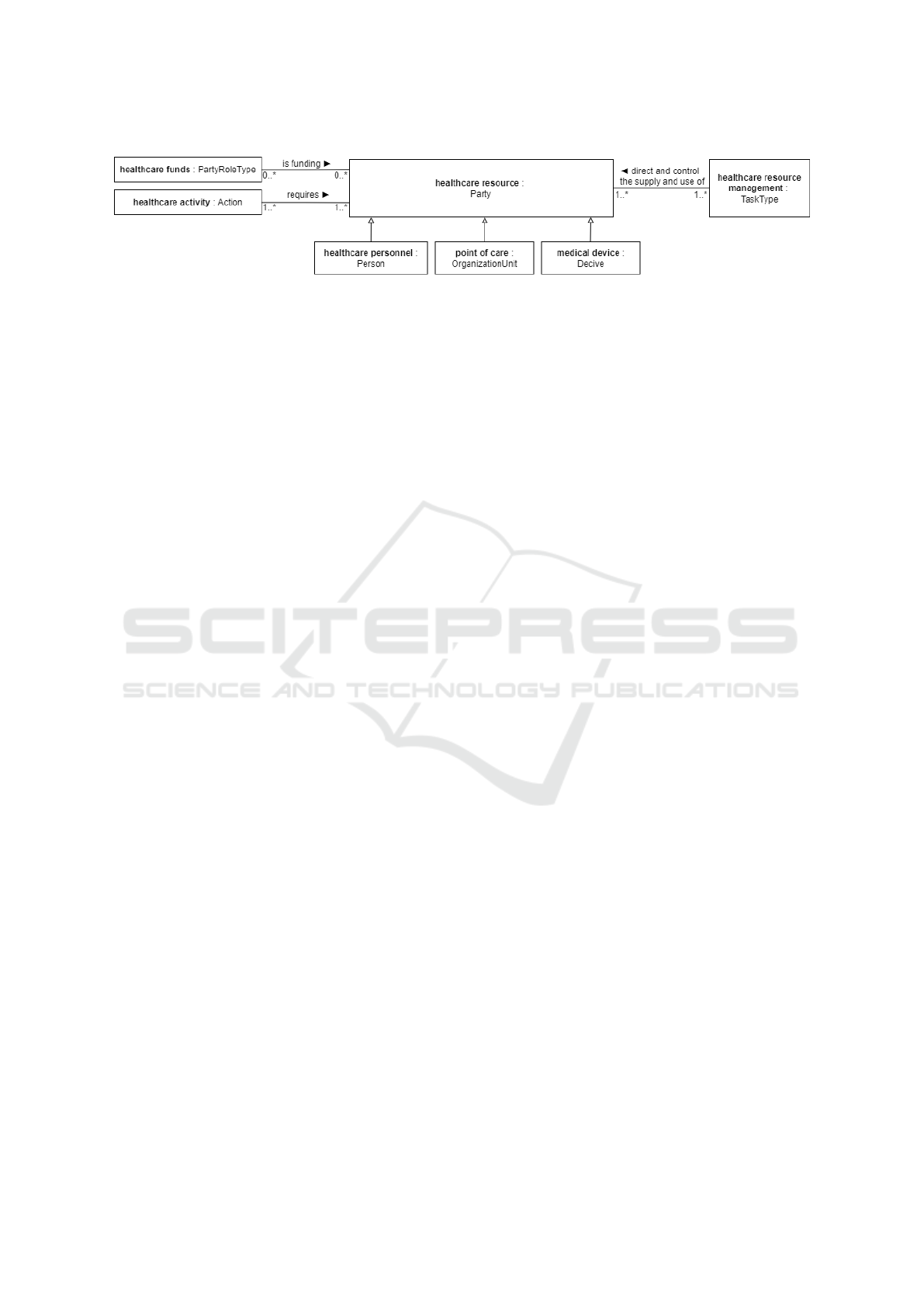
Figure 7: Model of healthcare resource using ISO 13940 terms and ABC4HEDA entities.
process-oriented approach and postulates the inter-
action between patients and healthcare professionals
as the essential aspect of healthcare processes. The
system requirements based on ISO 13940 were visu-
alised and validated using object diagrams.
Our proposed process meta-model contributes to
the semantic interoperability of federated systems and
the inclusion of more quality healthcare data in pri-
mary (care and diagnoses) and secondary (medical
science and research) use cases. Notably, the con-
textualisation dimension of data quality (Aerts et al.,
2021) is increased, as all clinical data in ABC4HEDA
are modelled as process outcomes, which keeps the
content of data (e.g. blood pressure) linked to its con-
text (e.g. the activity of measuring blood pressure and
the reason for performing the activity).
Our process meta-model describes the dynamics
of business processes as a series of conducted and re-
ported tasks as relationships between parties. Process
planning follows the same pattern and allows us to
evaluate the planned with the achieved.
Future work involves validating the order and
party role archetype patterns. The integration of
ABC4HEDA with more healthcare standards and
clinical research standards must also be proven before
the entire business logic can be validated.
AUTHORS’ CONTRIBUTION
TS wrote the manuscript with support from KK,
GP and TK. GP designed ABC4HEDA. TS and two
other bachelor’s students (Rainer Randmaa and Kaur
Matthias Ravel) under the supervision of KK, TK
and GP implemented ABC4HEDA. GP and PR su-
pervised the project and paper writing.
ACKNOWLEDGEMENTS
This work in the project ‘ICT programme’ was sup-
ported by the European Union through the European
Social Fund.
REFERENCES
Aerts, H., Kalra, D., Saez, C., Ram
´
ırez-Anguita, J. M.,
Mayer, M.-A., Garcia-Gomez, J. M., Dur
´
a Hern
´
andez,
M., Thienpont, G., and Coorevits, P. (2021). Is the
quality of hospital EHR data sufficient to evidence its
ICHOM outcomes performance in heart failure? A pi-
lot evaluation. preprint, Health Informatics.
Arlow, J. and Neustadt, I. (2003). Enterprise patterns and
MDA: building better software with archetype pat-
terns and UML. Addison-Wesley, Object Technology
series, Boston, ...
Beale, T. (2002). Archetypes: Constraint-based domain
models for future-proof information systems. In
OOPSLA 2002 workshop on behavioural semantics,
November 4–8, Washington State Convention and
Trade Center, volume 105, pages 1–69, Seattle, Wash-
ington, USA. Citeseer.
Bjørner, D. (2006). Software engineering 1: Abstraction
and modelling. Springer Science & Business Media,
Berlin Heidelberg.
Chen, D., Doumeingts, G., and Vernadat, F. (2008). Archi-
tectures for enterprise integration and interoperabil-
ity: Past, present and future. Computers in industry,
59(7):647–659.
Ciampi, M., De Pietro, G., Esposito, C., Sicuranza, M., and
Donzelli, P. (2013). A federated interoperability archi-
tecture for health information systems. Int. J. Internet
Protoc. Technol., 7(4):189–202.
Coad, P. (1992). Object-oriented patterns. Communications
of the ACM, 35(9):152–159.
EIC (2022). Eic pathfinder challenge: Towards the health-
care continuum: technologies to support a radical shift
from episodic to continuous healthcare. Accessed:
2022-03-24.
Fowler, M. (2010). Domain-specific languages. Addison-
Wesley Professiona, New Tork.
Garc
´
ıa-de Le
´
on-Chocano, R., S
´
aez, C., Mu
˜
noz-Soler, V.,
Garc
´
ıa-de Le
´
on-Gonz
´
alez, R., and Garc
´
ıa-G
´
omez,
J. M. (2015). Construction of quality-assured in-
fant feeding process of care data repositories: defini-
tion and design (part 1). Computers in Biology and
Medicine, 67:95–103.
Halevy, A. (2005). Why your data won’t mix: New tools
and techniques can help ease the pain of reconciling
schemas. Queue, 3(8):50–58.
ISO (2015). 13940:2015 Health informatics - system of
concepts to support. International Organization for
Standardization, Geneva. Switzerland.
MODELSWARD 2023 - 11th International Conference on Model-Based Software and Systems Engineering
166

ISO (2019). ISO 13606-1:2019 Health informatics — Elec-
tronic health record communication — Part 1: Refer-
ence model. International Organization for Standard-
ization, Geneva. Switzerland.
Kankainen, K. J. I. (2021). Usages of the contsys stan-
dard: a position paper. In Bellatreche, L., Chernishev,
G., Corral, A., Ouchani, S., and Vain, J., editors, Ad-
vances in model and data engineering in the digitali-
sation Era, MEDI 2021, 21-23 June 2021, Tallinn, Es-
tonia, volume 1481 of Communications in Computer
and Information Science, pages 314–324, Dordrecht
Heidelberg New York London. Springer Nature.
Lagos, N., Mos, A., and Cornax, M. C. (2018). Towards
semantically-aided domain specific business process
modeling. Data Technol. Appl., 52:463–481.
Meier, J., Klare, H., Tunjic, C., Atkinson, C., Burger, E.,
Reussner, R. H., and Winter, A. (2019). Single un-
derlying models for projectional, multi-view environ-
ments. In Hammoudi, S., Pires, L. F., and Seli
´
c, B.,
editors, Model-Driven Engineering and Software De-
velopment: 7th International Conference, MODEL-
SWARD 2019, pages 117–128, Prague, Czech Repub-
lic, February 20–22, 2019, Revised Selected Papers.
Springer Nature.
Mocan, A., Facca, F. M., Loutas, N., Peristeras, V., and
Goudos, S. K. (2009). Solving semantic interoperabil-
ity conflicts in cross-border e-government services.
International Journal on Semantic Web and Informa-
tion Systems (IJSWIS), 5(1):1–47.
Nan, S., Van Gorp, P., Korsten, H. H., Kaymak, U.,
Vdovjak, R., Lu, X., and Duan, H. (2015). Dccss:
A meta-model for dynamic clinical checklist sup-
port systems. In 2015 3rd International Conference
on Model-Driven Engineering and Software Develop-
ment (MODELSWARD), ESEO, Angers, Loire Valley
France February 9 - 11, 2015, pages 272–279, Se-
tubal. Portugal. SCITEPRESS - Science and Technol-
ogy Publications.
Negro-Calduch, E., Azzopardi-Muscat, N., Krishnamurthy,
R. S., and Novillo-Ortiz, D. (2021). Technological
progress in electronic health record system optimiza-
tion: Systematic review of systematic literature re-
views. International journal of medical informatics,
152:104507.
Oei, J. H., Proper, H. A., and Falkenberg, E. D. (1994).
Evolving information systems: meeting the ever-
changing environment. Information Systems Journal,
4(3):213–233.
Oniki, T. A., Coyle, J. F., Parker, C. G., and Huff, S. M.
(2014). Lessons learned in detailed clinical mod-
eling at intermountain healthcare. Journal of the
American Medical Informatics Association: JAMIA,
21(6):1076–1081.
Piho, G. (2011). Archetypes based techniques for develop-
ment of domains, requirements and software: towards
LIMS software factory. PhD thesis, Tallinn University
of Technology, Tallinn.
Piho, G., Roost, M., Perkins, D., and Tepandi, J. (2010a).
Towards archetypes-based software development. In
Sobh, T. and Elleithy, K., editors, Innovations in
Computing Sciences and Software Engineering, pages
561–566, Dordrecht. Springer.
Piho, G., Tepandi, J., Parman, M., and Perkins, D. (2010b).
From archetypes-based domain model of clinical lab-
oratory to lims software. In The 33rd International
Convention MIPRO, pages 1179–1184, New York.
IEEE.
Piho, G., Tepandi, J., and Roost, M. (2010c). Domain analy-
sis with archetype patterns based zachman framework
for enterprise architecture. In 2010 International Sym-
posium on Information Technology, volume 3, pages
1351–1356, New York. IEEE.
Piho, G., Tepandi, J., and Roost, M. (2011). Evaluation of
the archetypes based development. In Databases and
Information Systems VI, pages 283–295. IOS Press,
Amsterdam.
Piho, G., Tepandi, J., and Roost, M. (2012). Archetypes
based techniques for modelling of business domains,
requirements and software. In Information Modelling
and Knowledge Bases XXIII, pages 219–238. IOS
Press, Amsterdam.
Piho, G., Tepandi, J., Thompson, D., Tammer, T., Parman,
M., and Puusep, V. (2014). Archetypes based meta-
modeling towards evolutionary, dependable and inter-
operable healthcare information systems. Procedia
Computer Science, 37:457–464.
Piho, G., Tepandi, J., Thompson, D., Woerner, A., and Par-
man, M. (2015). Business archetypes and archetype
patterns from the hl7 rim and openehr rm perspectives:
Towards interoperability and evolution of healthcare
models and software systems. Procedia Computer
Science, 63:553–560.
PWC (2009). Transforming healthcare through secondary
use of health data. PriceWaterhouseCoopers.
Raavel, K. M., Kankainen (supervisor), K., and Piho (super-
visor), G. (2022). Introduction of loinc terminology to
archetype patterns based abc4heda base model. BSc
thesis, in Estonian.
Randmaa, R., Bossenko, I., Klementi, T., Piho, G., and
Ross, P. (2022). Evaluating business meta-models
for semantic interoperability with fhir resources. In
HEDA-2022: The International Health Data Work-
shop, June 19-24, 2022, Bergen. CEURAT, Norway.
Tu, Z., Zacharewicz, G., and Chen, D. (2016). A federated
approach to develop enterprise interoperability. Jour-
nal of Intelligent Manufacturing, 27(1):11–31.
Zachman, J. A. (1987). A framework for information sys-
tems architecture. IBM systems journal, 26(3):276–
292.
Towards Specification of Medical Processes According to International Standards and Semantic Interoperability Needs
167
