
A Mobile Application for Milano Ventilatore Meccanico:
A First Prototype
Silvia Bonfanti
1 a
, Angelo Gargantini
1 b
and Luca Novelli
2 c
1
University of Bergamo, Bergamo, Italy
2
Pulmonary medicine Unit, ASST Papa Giovanni XXIII, Bergamo, Italy
Keywords:
Mobile Application, Milano Ventilatore Meccanico, Telemedicine, Mechanical Ventilator, Application
Prototype.
Abstract:
In hospitals the need to have devices connected and accessible remotely is increasing, in order to continuously
monitor patients. This need also arose for mechanical ventilators. In this paper, we introduce the first pro-
totype of a mobile application to connect remotely to Milano Ventilatore Meccanico, a mechanical ventilator
developed during COVID-19 pandemic. We show the process adopted to design and develop the first proto-
type in Android.
1 INTRODUCTION
Nowadays, the use of applications to remotely con-
trol patients’ health is increasing. During COVID-19
pandemic, a group of researchers has developed an
open source ventilator called Milano Ventilatore Mec-
canico (MVM)
1
. The MVM project started from the
idea of the physicist Cristiano Galbiati, who was also
the leader. In only 42 days from the initial prototype
production to the demonstration of performances, the
FDA (Food and Drug Administration) declared that
the MVM falls within the scope of the Emergency Use
Authorization (EUA) for ventilators and, during the
following months, it has obtained the Health Canada
and the CE marking as well. Thanks to these achieve-
ments, the MVM can be sold and used in the USA,
Canada, and Europe. One disadvantage of this venti-
lator is that the patient connected cannot be monitored
and controlled remotely. This functionality has been
omitted because, based on international regulations,
the ventilator must guarantee a cybersecurity standard
that was not possible to satisfy during its develop-
ment due to time constraints related to the pandemic.
Before the COVID-19 pandemic, remote control of
ventilators was limited; however, changes caused by
the COVID-19 crisis and the limited amount of physi-
a
https://orcid.org/0000-0001-9679-4551
b
https://orcid.org/0000-0002-4035-0131
c
https://orcid.org/0000-0002-2705-248X
1
http://mvm.care
cians, motivated new designs of remote-control ven-
tilators, despite system setup complexity and strict
government regulation requirements (Barrow et al.,
2022).
In this paper, we show how we have implemented
a prototype of remote controller for the MVM. In par-
ticular, after having introduced the basic functional-
ities of MVM (see Sect. 2), we explain the method-
ology adopted in order to develop the prototype by
applying an Agile approach (see Sect. 3). In Sect. 4
we have collected the existing applications related to
mechanical ventilators, and in Sect. 5 we have listed
the MVM mobile application requirements. The pro-
totypes are presented in Sect. 6, while the Android
prototype is shown in Sect. 7. Sect. 8 concludes the
paper and we list some future improvements to the
application.
2 MILANO VENTILATORE
MECCANICO
MVM is an electro-mechanical ventilator and it is in-
tended to provide pressure-regulated ventilation sup-
port for patients that are in the Intensive Care Unit
(ICU). The ventilation is controlled by the pressure
and both compressed oxygen and medical air are
required for its operation (Bombarda et al., 2022).
Before starting the ventilation the MVM controller
passed through three phases: start-up in which the
314
Bonfanti, S., Gargantini, A. and Novelli, L.
A Mobile Application for Milano Ventilatore Meccanico: A First Prototype.
DOI: 10.5220/0011668400003414
In Proceedings of the 16th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2023) - Volume 5: HEALTHINF, pages 314-321
ISBN: 978-989-758-631-6; ISSN: 2184-4305
Copyright
c
2023 by SCITEPRESS – Science and Technology Publications, Lda. Under CC license (CC BY-NC-ND 4.0)

Controller GUI
Supervisor
User
Sensors
Actuators
Serial
Communication
Serial
Communication
I2C
Communication
Figure 1: Current high-level software architecture.
controller is initialized with default parameters; self-
test which ensures that the hardware is fully func-
tional; and ventilation off in which the controller is
ready for ventilation when requested. MVM pro-
vides two types of ventilation: Pressure Controlled
Ventilation (PCV) and Pressure Support Ventilation
(PSV). PCV is used when the patient is not able to
start breathing on his own. The respiratory cycle
is set by the physician and kept constant during the
ventilation, while the pressure changes between tar-
get inspiratory pressure and positive end-expiratory
pressure. A new breath starts after a breathing cy-
cle is over, and it is controlled by the respiratory rate
(RR) and the ratio between inspiratory and expira-
tory (I/E). Sometimes the user can spontaneously ini-
tiate a breath when a sudden drop in pressure is de-
tected within the trigger window during expiration.
When the patient is able to control his breathing, but
still needs support, PSV mode is the most appropriate
mode because MVM partially takes over the work of
breathing. A new breath starts when the ventilator de-
tects a sudden drop in pressure, while the expiration
starts when the patient’s inspiratory flow drops below
a set fraction of the peak flow. If a new breath is not
detected within the apnea delay (a time window set
by the physician), the ventilator automatically moves
to PCV mode because it is assumed that the patient
is not able to breathe alone. Two valves allow the air
to enter/exit from the patient, i.e., an input valve and
an output valve. When the ventilator is in the inspi-
ration phase, the input valve is opened and the output
valve is closed, while in the expiration phase the input
valve is closed and the output valve is opened. When
the ventilator is not running, or in case of emergen-
cies, valves are set to safe mode: the input valve is
closed and the output valve is opened. During ventila-
tion, three special operations can be performed by the
physician: inspiratory pause, expiratory pause, and
recruitment maneuver.
Current high-level software architecture is shown
in Fig. 1. It is composed of three components: GUI
(Graphical User Interface), controller, and supervisor.
The GUI (see Fig. 2), a touch screen, allows the physi-
cian to control patient parameters and interact with
the ventilator to set ventilation parameters; the con-
troller receives input from the GUI and interacts di-
rectly with the hardware reading patient’s data and is-
suing commands; the supervisor monitors the overall
Figure 2: MVM Graphical User Interface on board.
behavior of the ventilator and intervenes in case of er-
rors.
3 METHODOLOGY
In order to develop the MVM mobile application, we
have adopted an Agile approach to keep development
cycles small and incremental. Moreover, since the ap-
plication is new, and we did not find any similar appli-
cation to monitor and manage the ventilator remotely,
we use a prototyping approach. Instead of directly de-
veloping the final application, we build several proto-
types. Here, we describe how we have designed and
developed the final Android prototype by following
these steps:
1. analysis of existing applications for ventilation;
2. analysis of the existing GUI;
3. writing of the requirements specification docu-
ment for the mobile application;
4. prototyping on paper (POP);
5. prototyping using a software: Justinmind;
6. working prototype implemented in Android;
During all these steps, a pulmonologist has been con-
sulted to discuss the functionalities that the MVM ap-
plication should provide and to get suggestions for
improvement.
The main goal of the first step is to extract the ad-
vantages and disadvantages of existing applications,
in order to identify those functionalities that should
be provided by the MVM application. The obtained
results are shown in Sect. 4.
The second step consists in analyzing the GUI cur-
rently used to interact with the ventilator. We have
analyzed the user manual and the requirements spec-
ification from which we have extracted the function-
alities that can be performed also from the mobile ap-
plication to allow the physician to interact remotely.
In the third step, we formally defined the mo-
bile application requirements by integrating the func-
tionalities available in the GUI and the tips from the
physician. In particular, the physician helped us to
A Mobile Application for Milano Ventilatore Meccanico: A First Prototype
315

improve the application security in order to avoid pa-
tient harm and the usability of the application. The
application requirements are explained in Sect. 5.
Then, the prototyping design started. The pro-
totype has been designed following the prototyping
on paper (POP) approach, which consists in drawing
on paper shapes representing screens, buttons, text
boxes, and other items of the user interface. This is
the simplest method to prototype applications and al-
lows the designer to have a general view of what will
be the final result. The second approach adopted to
prototype is using dedicated software: Justinmind
2
.
Justinmind allows us to prototype mobile and web ap-
plications analogous to realistic applications. After
that, we started the implementation on Android Stu-
dio to get a working prototype. It does not have all the
functionalities as defined in the requirements specifi-
cation document, but it is a starting point to develop
the complete MVM mobile application.
4 EXISTING APPLICATIONS
FOR VENTILATION
Before starting the design of the MVM mobile ap-
plication, we analyzed existing applications related to
mechanical ventilators (Agudelo and S
´
anchez, 2020).
We have found seven applications.
Four of them are for educational purposes, they
provide ventilator setting parameters based on patient
data given as input by the expert: Basics of Mechan-
ical Ventilation (Unknown, 2014), VentilO (IUCPQ,
2020), VentICalc (van Beukering et al., 2020) and
Mechanical Ventilation Expert (Streltsov, 2022). The
other three applications simulate or are connected to
the ventilator, for each of them we have extracted ad-
vantages and disadvantages as summarized in Table 1.
MyVenus (Lab, 2022; Battista, 2016) is used for pa-
tients that suffer from chronic respiratory failure or
acute respiratory diseases and are mechanically ven-
tilated at home. Using this device the physician can
remotely monitor, using a web interface, the ventila-
tion parameters e.g. respiratory rate, inspiration time,
peak flow, and tidal volume. Moreover, it is able
to detect apnea and patient tube disconnection. Tru-
Vent App (Trucorp, 2022) is a training application.
The trainer sets patient characteristics and the learner
monitor and performs actions based on patient status,
which can be modified continuously by the trainer in
order to test different clinical conditions. Hamilton
Connect App (medical, 2022) allows the physician to
access selected ventilation data in order to monitor
2
https://www.justinmind.com/
patients remotely. Moreover, it offers a demo mode
that allows exploring all the application functional-
ities. None of the presented applications is able to
control remotely the ventilator in order to monitor and
also control patient clinical status.
5 APPLICATION
REQUIREMENTS
The possibility of remote management that this appli-
cation allows, reduces the response time of special-
ized personnel given the high demand for ventilators
and specifically in the cases of patients who totally de-
pend on the use of this equipment and require greater
attention and care by intensive care physician (Mi
˜
no
et al., 2021).
To provide safe care to ventilated patients, the
number of healthcare professionals who are allowed
to adjust the ventilator should be limited. Inform-
ing the clinician early about potential complications
or patient tolerance of ventilator changes can pro-
vide coordinated care and improve patient outcomes.
Every time an adjustment is made on the ventilator,
there must be a notification to the critical care nurse
in charge in order that the settings can be reviewed,
and an appropriate clinical observation is guaranteed
for the safety of the patient. It is crucial a local con-
trol and careful verification of remote prescriptions by
qualified health professionals. Furthermore, any pa-
rameter and alarm prescription change on ventilatory
devices should be clearly recorded, documented, and
communicated to the entire healthcare team. A mul-
tiparameter monitoring of the patient and a collabora-
tive and trained interprofessional team are necessary
conditions for safe and effective mechanical ventila-
tion. It might be reasonable to define shared protocols
and algorithms in individual ICUs to avoid potential
confusion from competing loci of control and infor-
mation, including alarm signals, introduced by the
remote-control system. A careful study of the man-
agement of the clinical risk deriving from the remote
control of mechanical ventilation and related cyberse-
curity will be necessary to define the possible clini-
cal implications and obtain the authorizations of the
Healthcare regulatory Agencies (Williams LM, 2022;
Branson et al., 2016; AAMI, 2020). An accurate eval-
uation of risks associated with a medical device re-
mote control in the tele-critical care context is strictly
recommended.
After having analyzed existing applications and
the existing MVM GUI, we have defined the MVM
application requirements by writing the Software Re-
quirement Specification document. Fig. 3 shows an
HEALTHINF 2023 - 16th International Conference on Health Informatics
316
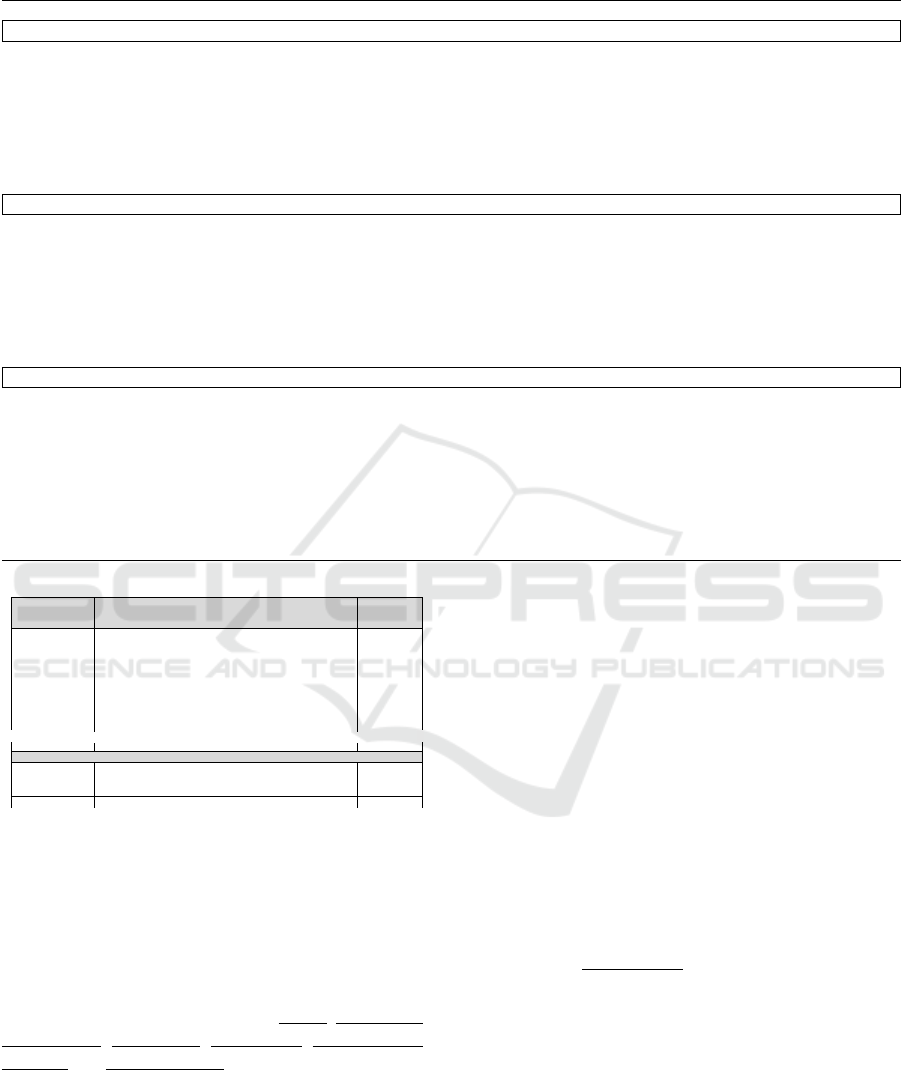
Table 1: Existing applications for ventilation.
Advantages Disadvantages
MyVenus
• continuous monitoring of home mechanical ventilation
• visualization of treatment at the patient’s home via web
interface for caregivers
• web interface optimized for different devices with nu-
merical parameters and waveforms
• apnea detection and patient tube disconnections
• dark and basic layouts
• only a web interface
• not connected directly to the ventilator, but a specific
device is required
• not yet on the market
TruVent App
• performs realistic medical simulation training without
the need for expensive/high-fidelity mannequins
• the instructor can adjust patient characteristics
• intuitive interface
• complex scenarios can be run
• shows ventilation alarms
• not connected to ventilators, it is an interactive remote
learning ventilation app
• concentration of information on one single screen
• needs clinical judgment
Hamilton Connect App
• test the app even without the ventilator when in demo
mode
• management of connected devices
• respiratory data wherever you want
• freeze and change the time scale for a closer view
• customizable view: layouts that suit the physician’s
needs
• not intended to replace the real-time display of data on
the ventilator
• dark layouts
ID
Requirement / Rationale
Input
Reference
APP.1
APP.1.1
APP.1.2
APP.1.3
…
APP shall implement the following screens:
Login: in the login screen, the user shall sign into his/her account.
Homepage: in the homepage screen, the APP shall visualize the
main criticalities and statistics about ventilators and pathologies.
Menu: the app shall allow the user to select 5 different options:
…
…
Login: in the login screen, the user shall sign into his/her account.
APP.2
The transition from login to homepage shall occur when the user
(physician or nurse) enters correctly e-mail and password and then
presses the “Login” button.
…
…
…
Figure 3: Excerpt of Software Requirement Specification
document.
excerpt of the requirements document, we have de-
fined each requirement and assigned an identifier in
order to track it through all the documents produced
during the application development (like e.g. in test-
ing documentation).
We have identified nine views: Login, Homepage,
New patient, PSV mode, PCV mode, Ventilator list,
Monitor and Alarms setting.
Login. After logging in using the username and
password provided, the system allows different oper-
ations based on user type: the nurse/medical assis-
tant can monitor the connected ventilators and check
if alarms have been raised by the ventilator; the physi-
cian, in addition to the features provided for the nurse,
can connect/disconnect new patients and set ventila-
tion parameters.
Homepage. From the homepage the user can view
the list of ventilators alarms based on their criticality.
By clicking on the single alarm he/she is automati-
cally redirected to the monitor screen. On the home
page, some statistics related to the state of ventilators
(available or connected) and patients’ pathologies are
shown. The following screens are reachable from the
menu on the homepage: New patient, Ventilator list,
and Monitor.
New Patient. The user can insert patient informa-
tion through New patient screen. The required in-
formation is an ID (usually the fiscal code), name,
surname, date of birth, height (in cm), gender, and
patient disease. Then, based on these data, the ap-
plication automatically computes the predicted body
weight (PBW), the required parameters for the venti-
lation. All the data are stored in a database by clicking
the save button. Then the physician (this function is
not available for nurse/medical assistant) selects the
ventilator through a drop-down menu showing all the
available ventilators. Then by clicking on the corre-
sponding button, the physician inserts the ventilator
A Mobile Application for Milano Ventilatore Meccanico: A First Prototype
317
parameters for both PCV and PSV modes.
PCV Mode. The physician inserts all the param-
eters required for running the ventilator in PCV
mode: respiratory rate (RR), inspiratory/expiratory
ratio (I:E), target inspiratory pressure (P
insp
) and in-
hale trigger sensitivity (ITS). Then all the parameters
are stored in a database. To start and stop the venti-
lation, the physician can use the appropriate buttons.
For security purposes, these operations must be au-
thorized through an authorization code displayed on
the ventilator. This guarantee that someone is close to
the patient when performing these critical operations,
nevertheless the physician can do them remotely.
PSV Mode. The physician inserts all the parameters
required for running the ventilator in PSV mode: tar-
get inspiratory pressure (P
insp
), inhale trigger sensitiv-
ity (ITS), expiratory trigger sensitivity (ETS), apnea
delay and the apnea backup parameters (RR, I:E and
P
insp
) when automatically the ventilator moves from
PSV to PCV because the patient is not able to breathe
on his/her own. As required for PCV mode, start and
stop operations must be authorized through an autho-
rization code displayed on the ventilator.
Ventilator List. This screen shows all the ventila-
tors registered in the application. For each of them,
the application shows if it is connected to the patient
or not, if it is ventilating or not, and if alarms are
present. By clicking on the ventilator, the user is redi-
rected to the monitor screen.
Monitor. The monitor screen shows the real-time
measured parameters and waveforms. The wave-
forms displayed on the screen are pressure in the air-
ways (PAW), tidal volume (V
tidal
), and the instanta-
neous flow. Then the following real-time parameters
are shown: RR, PEEP, measured minute volume V
e
,
P
insp
, V
tidal
, the measured fraction of inspired oxygen
(FiO
2
). Then, only for the physician, it is possible to
perform inspiratory and expiratory pauses and recruit-
ment maneuver, which must be authorized by a code
displayed on the ventilator.
Alarms Setting. The physician inserts the alarm
parameters ranges: minimum and maximum RR,
minimum and maximum P
insp
, minimum and maxi-
mum V
tidal
, minimum and maximum PEEP. All these
values are stored in the database and used during the
ventilation to raise alarms when measured parameters
are out of range.
Figure 4: State machine.
Figure 5: New high-level software architecture.
An overview of the transition between application
screens is given in Fig. 4.
To mitigate risks associated to remote control, we
have included in the application some procedures that
require an authorization code shown on the GUI of
the ventilator. This is necessary to guarantee that dur-
ing critical operations, like start/stop ventilation and
pauses, nevertheless the physician performs them re-
motely, a qualified person is close to the patient to
monitor his/her health state. Moreover, an authoriza-
tion code is required whenever connecting to the ven-
tilator in case the physician wants to update ventila-
tion parameters or connect a new patient. It is not re-
quired only if the physician intends to view measured
parameters without performing any action.
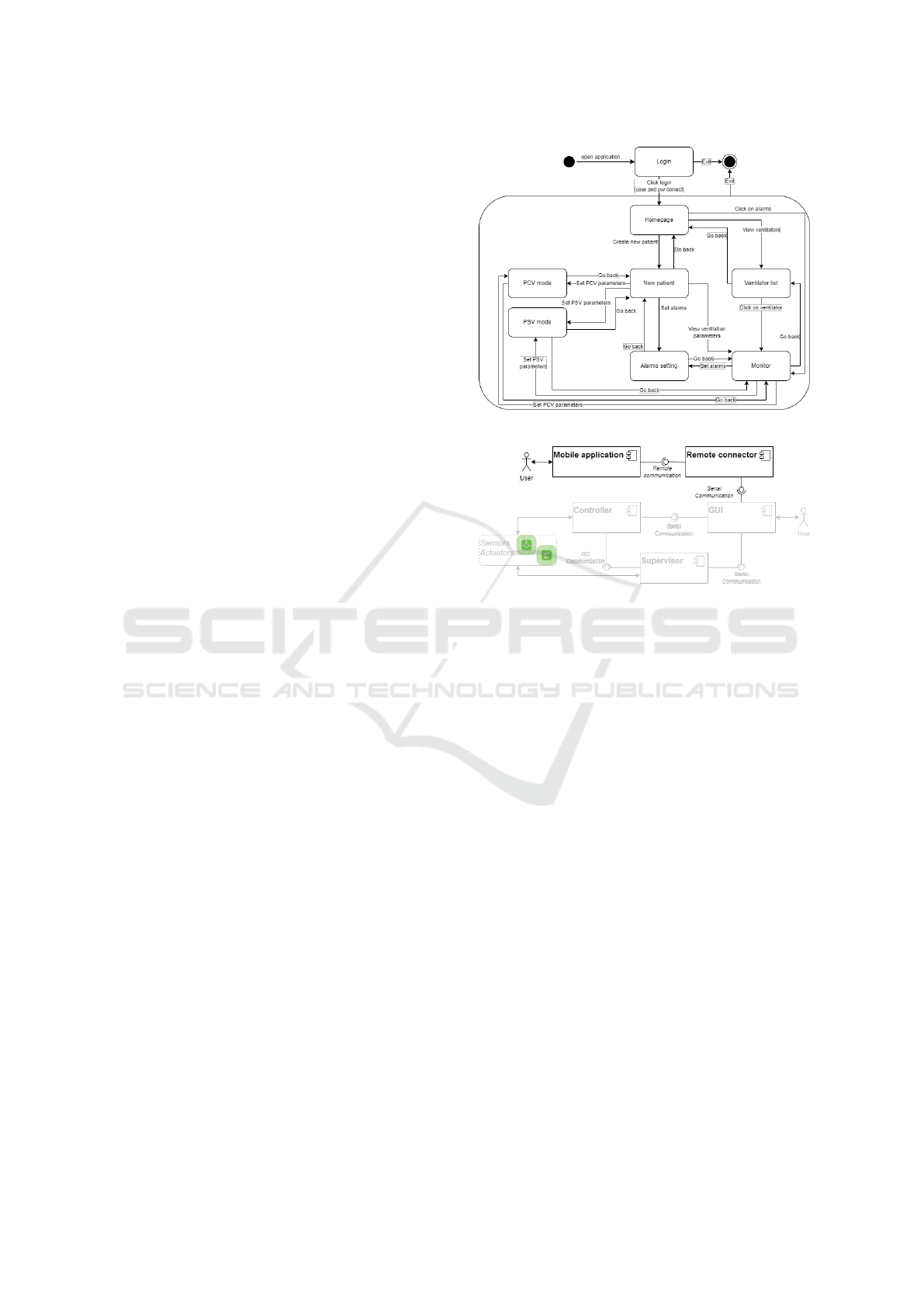
5.1 Architecture
The existing MVM architecture (see Fig. 1) does
not support mobile application integration because,
for cybersecurity problems, all the remote connection
modules have been removed. Fig. 5 shows the new
architecture in which new components are added in
order to allow communication between the ventilator
and the mobile application.
The new architecture requires a new module inte-
grated into the hardware where GUI is implemented.
This module read and sends data from the ventilator
HEALTHINF 2023 - 16th International Conference on Health Informatics
318

Figure 6: Prototyping on paper.
to the mobile application and vice versa. When imple-
menting this module, the cyber security risk must be
considered in order to avoid systems vulnerabilities
(e.g. ventilator parameters are changed by an external
application not authorized).
6 APPLICATION PROTOTYPE
As written in Section 3, we have followed two steps
for the application prototype: prototyping on paper
(POP) and prototyping using the software.
Fig. 6 shows the POP result. This initial proto-
type helped us to have an immediate overview of the
entire application, by understanding the information
displayed by the application and the information re-
quired to the user.
The second prototype has been implemented us-
ing Justinmind tool (see Fig. 7). The obtained proto-
type is clickable and fully-functional, without writing
a single line of code. This step required less effort
than implementing in Android, but allowed us to have
a usable application showable to the physician from
which we started to analyze the characteristics, ad-
vantages, and disadvantages of the implemented pro-
totype.
Given the prototype, we got important feedback
from the physician. The most important and criti-
cal was the lack of direct control of the ventilator
when performing critical operations like start and stop
ventilation. For this reason, as already explained in
Sect. 5, we have decided to introduce an authoriza-
tion code shown on the ventilator, that must be com-
municated to the physician and used by him/her to
confirm critical operations. This procedure guarantee
that someone belonging to the medical staff is close
to the ventilator and monitors the patient’s status.
Another suggestion was about the functionalities
available based on the role of the app user. In the
prototype implemented in Justinmind, there was no
difference between the app interface used by a physi-
cian or by a nurse/medical assistant, all the operations
were allowed to everyone. This was not safe for pa-
tients because the competencies of medical staff are
different, and not everybody is able to correctly con-
figure the ventilator and start/stop patient ventilation.
Given this, we have associated a role to each user, and
based on it different operations are allowed.
Performing different operations on the ventilator
can be critical, and for safety purposes, it is very im-
portant to track who performs and when operations
are performed. At the moment this functionality is
not expected to be implemented in the first version of
the application, but it will be taken into consideration
for the next.
7 ANDROID IMPLEMENTATION
After having implemented the prototype using the two
approaches presented above, we have implemented
the first prototype in Android Studio as shown in
Fig. 8. The first screen is for authentication (see
Fig. 8a). At the moment, in this prototype, we have
not distinguished between two roles as explained in
the requirements section. The home page (see Fig. 8b)
shows all the alarms raised by connected ventilators,
and clicking on each alarm it is possible to directly ac-
cess the ventilation screen in order to check measured
parameters. At the bottom of the screen are shown
how many ventilators are free and the type of disease
for which patients need ventilator support. The main
menu, different from the prototype implemented us-
ing Justinmind tool, is accessible from a drop-down
menu, from where the user can access the following
main functionalities: connect a new patient to the ven-
tilator and see all the ventilators. When connecting a
new patient (see Fig. 8c), some personal data are re-
quired, then the physician must specify the type of
disease and select the ventilator to which the patient
is connected among the free ones. Then the physician
must set the PSV and PCV parameters (see Fig. 8f
and Fig. 8e) to start the ventilation. In order to guar-
antee patient safety when performing a start and stop
ventilation, an authorization code is required to au-
thorize the activity. Moreover, alarms threshold are
set using the alarms interface (see Fig. 8g). When the
physician opens the screen to see all the ventilators
(see Fig. 8d) is it possible to see for each a colored
led: gray if the ventilator is disconnected, green if
there are no alarms, yellow if there are warnings on
the ventilator, red if there are critical alarm raised by
the ventilator. In this prototype, all the connections
with the real ventilators are omitted, because the ven-
tilator does not have a module to interact remotely.
A Mobile Application for Milano Ventilatore Meccanico: A First Prototype
319

(a) Home. (b) New Patient. (c) Ventilator List. (d) PCV mode.
(e) PSV mode. (f) Alarms settings. (g) Ventilator monitor.
Figure 7: Prototype implemented using Justinmind tool.
(a) Login. (b) Home. (c) New Patient. (d) Ventilator List.
(e) PCV mode. (f) PSV mode. (g) Alarms settings.
Figure 8: First prototype in Android.
8 CONCLUSIONS AND FUTURE
WORK
In this paper, we have shown the methodology
adopted in order to develop a first prototype of the
mobile application to monitor and control patients
connected to the ventilator. Starting from the GUI,
already integrated into MVM, we have defined re-
quirements and we have implemented two prototypes,
HEALTHINF 2023 - 16th International Conference on Health Informatics
320

the first using the approach of prototyping on paper
and the second prototype having been developed us-
ing Justinmind tool. Starting from the prototype, we
have integrated physician comments, especially we
have included that critical operations must be con-
firmed by a code displayed on the device (this im-
plies that someone is near the ventilator, but at the
same time the physician can perform actions in order
to treat the patient). This work is just preliminary,
and it has been performed in order to check the fea-
sibility. Many other features must be implemented as
future work to get the final working application. For
example, depending on the role of the user only pa-
tient monitoring is available, or also ventilator con-
trol. The most critical part is to connect the applica-
tion with the ventilator because this requires changes
also on the MVM as shown in the new architecture.
While, in order to make the application available to
the largest number of users, it should be developed
using a cross-platform development environment.
ACKNOWLEDGEMENTS
We would like to thank Alice Lucchini, Dounia Ah-
bar, Tatiana Vasilache, and Martina Brambilla for the
preliminary work done for this project.
REFERENCES
AAMI (2020). Emergency use guidance for remote control
of medical devices.
Agudelo, J. C. M. and S
´
anchez, M. B. S. (2020). Medical
learning tool for ventilator weaning protocols. Revista
EIA, 17(34).
Barrow, M., Restuccia, F., Gobulukoglu, M., Rossi, E., and
Kastner, R. (2022). A remote control system for emer-
gency ventilators during SARS-CoV-2. IEEE Embed-
ded Systems Letters, 14(1):43–46.
Battista, L. (2016). A new system for continuous and
remote monitoring of patients receiving home me-
chanical ventilation. Review of Scientific Instruments,
87(9):095105.
Bombarda, A., Bonfanti, S., Galbiati, C., Gargantini, A.,
Pelliccione, P., Riccobene, E., and Wada, M. (2022).
Guidelines for the development of a critical software
under emergency. Information and Software Technol-
ogy, 152:107061.
Branson, R., Godwin, T., Hargett, J., Papadakos, P., Ro-
driquez, D., Stampor, L., and Strickland, S. (2016).
Safe initiation and managementof mechanical ventila-
tion. American Association for Respiratory Care and
UniversityHealthSystem Consortium’s.
IUCPQ (2020). VentilO.
Lab, B. (2022). MyVenus.
medical, H. (2022). Hamilton Connect App.
Mi
˜
no, C., Flor, O., Quiroga, J., and Cuaycal, A. (2021).
Remote variable monitoring app for mechanical ven-
tilators used in COVID-19. In Artificial Intelligence,
Computer and Software Engineering Advances, pages
303–315. Springer International Publishing.
Streltsov, V. (2022). Mechanical Ventilation Expert.
Trucorp (2022). TruVent App.
Unknown (2014). Basics of Mechanical Ventilation.
van Beukering, S., de Ruijter, P., Sreekantan, S., der Ho-
even, J. V., and Workum, J. (2020). VentICalc.
Williams LM, S. S. (2022). Ventilator Safety. StatPearls [In-
ternet]. Treasure Island (FL): StatPearls Publishing.
A Mobile Application for Milano Ventilatore Meccanico: A First Prototype
321
