
Neonatal Video Database and Annotations for Vital Sign Extraction and
Monitoring
Hussein Sharafeddin
1
, Lama Charafeddine
2
, Jamila Khalaf
1
, Ibrahim Kanj
1
and Fadi A Zaraket
2
1
Lebanese University, Beirut, Lebanon
2
American University of Beirut, Beirut, Lebanon
Keywords:
Video Database, Neonatal Monitoring Data Set, Noninvasive Monitoring.
Abstract:
Background: The end goal of this project is to detect early signs of physiological disorders in term and
preterm babies at the Neonatal Intensive Care Unit using real time camera-based non-contact vital signs mon-
itoring technology. The contact sensors technology currently in use might cause stress, pain, and damage to
the fragile skin of extremely preterm infants. Realization of the proposed camera based method might com-
plement and eventually replace current technology. Non-invasive early detection of heart rate variability might
allow earlier intervention, improve outcome, and decrease hospital stay. This study constructed a curated set
of videos annotated with accurate and reliable measurements of the monitored vital parameters such as heart
and respiratory rates so that further analysis of the curated data set lead towards the end goal. Body: The
data collection process included 56 total hours of recording in 127 videos of 27 enlisted neonates. The video
annotations include (1) vital signs acquired from bedside patient monitors at second based intervals, (2) the
neonate state of health entered and manually reviewed by a healthcare provider, (3) region of interest in video
frames for heart rate detection extracted semi-automatically, and (4) the anonymized and clipped region of
interest videos. Conclusion: The paper presents a curated data set of 127 video recordings of deidentified
neonate foreheads annotated with vital signs, and health state in XML format. The paper also presents a utility
study that shows accurate results in estimating the heart rate of term and preterm neonates. We hypothesize
that the data set we collected is beneficial for improving state of the art monitoring techniques. Its timely
dissemination may help lead to techniques that detect anomalies earlier, hence, leading to earlier treatment
and improved outcome.
1 INTRODUCTION
Current medical and technological advancements are
increasingly leading to higher survival rates of term
and premature neonates. Of all live births at least
ten percent need some intervention after birth to help
them adapt to the extra-uterine life and close to one
percent will need further management because of dif-
ferent conditions and illnesses. Typically, all in-
fants admitted to the neonatal intensive care unit
(NICU) require continuous cardiopulmonary moni-
toring which is essential for early detection of signs
of illness and for tracking changes in physiologic
state (Liu et al., 2012; Lozano et al., 2012). Since the
earliest sign of physiologic disturbances in neonates
is a change in heart rate (HR) followed by the res-
piratory rate (RR), it is important to have a reliable
continuous monitoring system that permits early de-
tection and prompt intervention as early as possible to
prevent treatment delay and avoid potential morbidity
or mortality (Group, 2008).
In neonates, watchful waiting until more obvious
signs are revealed may already be too late to achieve
a complete recovery. On the other hand, over treat-
ment may be detrimental as it is the case of excessive
use of antibiotics that increases the likelihood of se-
lecting resistant bacteria hence rendering future treat-
ments more difficult (Edmond and Zaidi, 2010). Cur-
rent monitoring tools used in the NICU require direct
contact with the patient which might cause harm at
times or, at least, might interfere with patient care or
parent-infant bonding. This is particularly true for ex-
tremely premature infants who have thin gelatinous
skin that is prone to sloughing in case of strong bond
or erroneous signal due to poor adherence.
For the above reasons, minimally invasive moni-
toring tools using “non-contact” electrodes have been
the subject of extensive analytical and data oriented
research (Wu et al., 2012; Poh et al., 2010; Alghoul
et al., 2017; Christinaki et al., 2014) that requires
Sharafeddin, H., Charafeddine, L., Khalaf, J., Kanj, I. and Zaraket, F.
Neonatal Video Database and Annotations for Vital Sign Extraction and Monitoring.
DOI: 10.5220/0011637800003411
In Proceedings of the 12th International Conference on Pattern Recognition Applications and Methods (ICPRAM 2023), pages 767-774
ISBN: 978-989-758-626-2; ISSN: 2184-4313
Copyright
c
2023 by SCITEPRESS – Science and Technology Publications, Lda. Under CC license (CC BY-NC-ND 4.0)
767
collecting data sets for training, learning and evalu-
ation. We review these techniques and others in the
Related Work section 3. In this work, we present a
video database annotated with vital signs for neonate
infants. The work makes the database available to
the research community aims to advance research and
development efforts towards non-invasive monitoring
techniques for neonates.
2 CONSTRUCTION AND
CONTENT
The following describes our work to collect video
recordings of neonates while in care and curate them
with heart rate, respiratory rate and other health care
relevant annotations. The data collection process pro-
ceeded as follows.
• We designed our video capture environment with
the help of the NICU staff and director. Our target
was to allow studying the possibility of establish-
ing norms for each neonate population and to es-
tablish research data resources for public access.
• Simultaneously, we designed a method to collect
synchronized data from bedside monitors con-
nected to the neonates through electrodes. We
used the bedside monitors to obtain automatic
heart rate and respiratory rate annotations. We
bridged and synchronized the existing bedside
monitoring sensory devices with the same ma-
chine capturing the video recordings. We were in-
terested in capturing the change in heart rate and
heart rate variability (Task Force of the European
Society of Cardiology the North American Soci-
ety of Pacing Electrophysiology, 1996; Sztajzel,
2004) as we would like to study their correlation
with skin color variations.
• We constructed our annotation terms and notes
based on discussions with the NICU healthcare
team. The terms concern (i) medical state of
the neonate, and (2) technical conditions such as
reasons for obstructions to recordings or lighting
conditions.
• We drafted a consent form to collect consent from
the parents. The form describe to parents the aims
of the study and the possible risks involved in-
cluding how we planned to preserve privacy and
anonymity.
• We drafted our design as proposal to the Institu-
tional Review Board (IRB) of the American Uni-
versity of Beirut and obtained their approval to be-
gin the study. Institutional Review Board (IRB)
Table 1: Sample demographics.
Variables Value
Number of infants enrolled 27
Birth weight (g) Mean (±sd) 1302(576)
Gestational age (wk) Mean (±sd) 32.33(4.98)
Total hours recorded 55:34:28
Number of videos 127
Infants with bradycardia events 11
Infants with apnea events 2
who also approved the sharing of the anonymised
videos as an open access repository for further re-
search in this area.
• We trained our research assistants on how to ap-
proach parents for consent, and how to setup the
video recording environment to be compliant with
the objective of the studies.
• The research assistants approached the parents for
consent and once they received written informed
consent from the parents, they started the video
recordings.
• To date, we recorded, annotated and analyzed
over 55 hours of videos from 27 term and preterm
neonates.
We evaluated the utility of our collected data set
by running existing techniques (Wu et al., 2012; Al-
ghoul et al., 2017) on the data. Knowing that one
of the first signs of physiologic disturbances in new-
born is the change in heart rate and heart rate variabil-
ity (Task Force of the European Society of Cardiology
the North American Society of Pacing Electrophysi-
ology, 1996; Sztajzel, 2004), we focused on correlat-
ing heart rate with skin color changes. The results we
obtained are promising and we discuss them further
in Section 4.
2.1 Video Database Content
Table 1 shows that the data set contains 56 hours in
127 recordings of 27 enrolled infants. Eleven infants
had bradycardia events and two infants had Apnea
events.
Table 3 shows the detailed schematic of the an-
notations. We implemented the annotations in XML
format and associated one XML file with each video.
The published video files capture the forehead region
of interest (ROI) that is instrumental in determining
the vital signs. Table 2 illustrated statistics of the
video recordings.
ICPRAM 2023 - 12th International Conference on Pattern Recognition Applications and Methods
768

Table 2: Recording Statistics.
Recording Time
(minutes)
Total all videos 3334
Overall Average(SD) 26.2(14.1)
Average per patient (SD) 120.5(131)
Age at first recording (days) Min - Max 1 - 185
Recording Place
( % time)
Open incubator 61%
Closed incubator 39%
Infant status
(average % time)
Awake 31%
Deep Sleep 8%
Light Sleep 61%
Infant motion
(average % time)
At rest 8%
Minimal 63%
Agitated 25%
Agitated & Crying 5%
Detection
(average % time)
Detected 81%
Not detected 19%
Figure 1: RECORDING SETUP: Tripod with camera
mounted near incubator.
2.2 Video Acquisition
Video acquisition started November 2016 and contin-
ued until April 2018. The videos feature infants ad-
mitted to the NICU at the AUBMC after parental writ-
ten and informed consent. A total of 160 videos were
captured using the LogitecC920 high definition cam-
era with 1920 × 1080 pixel resolution at 30 frames
per second. The camera was mounted on a tripod 40
to 60cm away from the baby incubator as depicted in
Figure 1 showing the camera mounted facing the baby
incubator in the NICU. We excluded 33 out of the 160
videos due to technical issues or to failure of forehead
detection. The forehead regions extracted from the
remaining 127 videos are all admitted to the database
with their annotations.
2.3 Data De-Identification
We performed data anonymization to clear patient
names, dates of birth and identifying facial features.
We replaced patient names and dates of birth with
a unique patient ID number and a day index while
preserving order, respectively. We only publish the
detected forehead region of the videos that is instru-
mental for vital sign extraction. Consequently, this
removes identifying facial features such as the eyes,
nose and lips. We reviewed the automatically detected
ROI videos and made sure no identifying facial fea-
Figure 2: CHALLENGES IN FACE DETECTION AND
TRACKING. FRAMES A-C: (a) Patient ID 08, sleeping at
rest. Medical equipment occluding face and challenging
face detection. (b) Baby moving and turning; challenging
continuous ROI localization. (c) face detection and fore-
head (ROI) localization (note green superimposed box). .
Figure 3: TWO PATIENT SAMPLES EACH REQUIRING
ITS SPECIALIZED INITIAL TEMPLATE FOR MATCHING.
FRAMES A-D: (a) Patient P09 in video1. (b) Patient P08
in video2. (c) Template for video1. (d) template for video2.
tures exist in them.
2.4 Forehead Detection
Typically, forehead detection proceeds by face de-
tection followed by facial feature tracking, and then
segmenting the forehead portion. However, inter-
and intra- video variability in patient appearance and
state complicated this task. For example, the pres-
ence of medical tape and nasal tubes affected the qual-
ity of features necessary for automatic face detection.
Hence, forehead detection robustness suffered and we
needed semi-automatic detection. Figure 2 shows an
example of such challenges for one baby. The baby
face is continuously partially occluded with medical
dressing. Occasionally more occlusion occurs due to
baby face or hand motion. This sometimes leads to
lost detection.
We created several image templates that cover dif-
ferent scenarios, and for each video, we manually
identified the specific template that best matches the
nose and surrounding area. Once there is a match,
the forehead region to be extracted is the rectangular
region above the template. Figure 3 shows two differ-
Neonatal Video Database and Annotations for Vital Sign Extraction and Monitoring
769

ent patient presentations together with their identified
templates and extracted regions.
The forehead tracking proceeded frame-by-frame.
Once we matched the template in an initial frame,
we automatically track the region across subsequent
frames measuring similarity mostly with no need
for human intervention. When a significant scene
change occurs such as nurse intervention or heavy
baby movement, the tracking fails. We remedy this by
restarting the forehead detection and skipping frames
where detection fails. We manually inspected the
videos to make sure that forehead tracking failure did
not result in identifying facial features leaking into the
published videos.
2.5 Video Organization and Annotation
We organized the videos of each patient into a sepa-
rate directory. The videos of patient 01 and the as-
sociated annotation files go into directory P01. Each
patient directory contains a number of videos with an
associated annotation file in XML format.
File RecodingList includes metadata records
about all patient videos. Each record has the name
of the video file, the number of frames per second,
the day of the recording in preserved order, the length
of the video, the age of the baby at recording since
inception, and the status of the incubator.
It might also have temporal annotations indicating
when the baby was in states such as deep sleep, light
sleep, agitated, bradycardia, apnea and rest. Other
temporal annotations indicate when the region of in-
terest was detected, re-detected or lost.
Each video in a patient directory comes with an
associated xml video annotation file. The video anno-
tation file includes two sections. The first section pro-
vides metadata about the file including its name, dura-
tion, number of frames per second, width and height
of the captured region of interest, the status of the in-
cubator, feeding method, whether an event happened
during the recording and whether a nutritive feed hap-
pened during the recording.
The second section provides a time stamp from
the start of recording, the heart and respiratory rates.
For this purpose, we configured a dual MIB/RS232
serial cord to extract realtime vital signs from the
MP40-70 Philips Intellivue monitor. The second sec-
tion also has the status of the baby, whether an action
happened, and the location of the captured ROI with
respect to the video frame. It might also have some
notes taken by the healthcare providers. Table 3 de-
scribes the entire annotation scheme with examples
for each field.
3 RELATED WORK
Recently, several methods for extracting HR data
from video recordings of adult subjects have been
published. Eulerian Video Magnification (Wu et al.,
2012) (EVM) utilizes minute skin color variations and
low amplitude motion that are magnified to reveal sig-
nals of interest which reflect physiologic changes at
the cellular level such as changes in skin perfusion,
temperature and heart rate. Poh et al. (Poh et al.,
2010) used Blind Source Separation (BSS) based on
independent component analysis (ICA) of the red,
green, and blue (RGB) intensity channels in facial
videos for HR measurement. Alghoul et al. (Alghoul
et al., 2017) compared between EVM and ICA and
found approaches based on ICA to deal better with
lighting-related noise; however, approaches based on
EVM performed better with motion-related noise. A
comparison of three BSS-ICA based methods is found
in (Christinaki et al., 2014) where different statistical
transformations aimed at enhancing component sepa-
rability for extracting the HR.
EVM and BSS only require video recordings from
a close distance without any close contact with the pa-
tient hence they are non-invasive. In (Wu et al., 2012),
colour changes are tracked over time, thus permit-
ting analysis of physiological state changes such as
heart rate and subsequently perfusion. Those changes
would then be correlated with particular condition or
disease states for the purpose of automatic diagnosis
and alarm issuance.
4 UTILITY AND DISCUSSION
We performed video analysis to extract vital signs us-
ing two methods reported in the literature to validate
the sanity of our data set and establish its utility. The
video analysis proceeds in two steps: face detection
and heart rate extraction.
Face Detection: Baby faces maybe often partially
covered with medical equipment and dressing while
in the incubator. That led to failure of off-the-shelf
face detection algorithms. Thus for each video, and
in the first frame, we selected an initial region of in-
terest (ROI) containing the face. We set this as a face
template and used ROI tracking to capture it in the
rest of the video. This resulted in successful detection
throughout the recordings.
HR Extraction: We tested two methods to recover
the PPG signal from the detected faces. One is based
on analyzing the frequency content of the green chan-
nel(Wu et al., 2012), and the other is based on in-
dependent component analysis (ICA)(Alghoul et al.,
ICPRAM 2023 - 12th International Conference on Pattern Recognition Applications and Methods
770
Table 3: Description of annotation scheme.
Label Description Examples
Patient ID The code given to the patient in chronological order P15
VideoName combination of patient ID, date index and video sequence num-
ber
P25-Day0505-V25-1.avi
Video porperties recording parameters
Frame rate how many image frames are captured per second (fps) of
recording
30 fps
Duration the video length in h:m:s 1:18:49
Width frame width in pixels 90
Height frame height in pixels 50
Recording Info environment-related information
Incubator incubator status being open or closed Closed
Position the baby’s position being supine or prone Supine
Non-nutritive feed whether non-nutritive feeding (pacifier) is being used at record-
ing time
yes
Recording Annotations Instantaneous heart rate, Status, Action, Detection, Coordi-
nates, Notes
HR Instantaneous heart rate extracted from the Intellivue Philips
Monitor every second
167
Status baby’s status in three states :
• deep sleep (absolutely no motion except for breathing re-
lated)
• light sleep (possible slow movement of hand, face, etc..)
• awake (open eyes, possible movements or interaction with
environment)
deep sleep
Action We identified four states :
• rest (usually coinciding with deep sleep)
• minimal (light or slow movement of face, limbs, etc.)
• agitated (heavy / fast movements)
• agitated with crying
agitated
Detection whether detection has occured at this second which means fore-
head availability
Detected
X,Y coordinates of the forehead in the initial frame
• x is the top left corner
• y is the bottom right corner
759,250
Notes Any activity observed during recording such as nurse care,
changes in ambient light, etc.
nurse care
2017). Both methods aim to extract rate of the car-
diovascular pulse wave which circulates throughout
the body when the heart beats.
The green channel method proceeds as follows.
a. R=Select ROI
b. Obtain raw signal s from each frame of selection
R
c. Extract hgi the green channel from s
d. Compute discrete signal hd
g
i = zero-mean, win-
dowed hgi.
e. Select the best component d
best
=
MAXPEAK
240
60
FFT(d
g
) by applying Fast Fourier
Transform (FFT) on on hd
g
i and choose the
resulting FFT component with the highest peak
within the range of 60 and 240 beats per minute
(bpm).
The ICA method follows the (a,b) steps from
above and proceeds as follows.
c. Extract hr, g, bi the red, green and blue (RGB)
channels from s
d. Compute zero-mean, unit-variance normalized
discrete signals hd
r
, d
g
, d
b
i from hr, g, bi.
e. Apply ICA to compute three independent source
signals hi
1
, i
2
, i
3
i = JADE(s, r, g, b). The signals
break up the raw elements hr, g, bi into three in-
dependent source signals (i
1
, i
2
, i
3
) using the joint
approximate diagonalization of Eigen matrices
(JADE) algorithm.
f. Apply FFT on i
1
, i
2
, and i
3
.
g. Compute the best FFT component with the high-
est peak within the 40 and 240 bpm range.
Neonatal Video Database and Annotations for Vital Sign Extraction and Monitoring
771
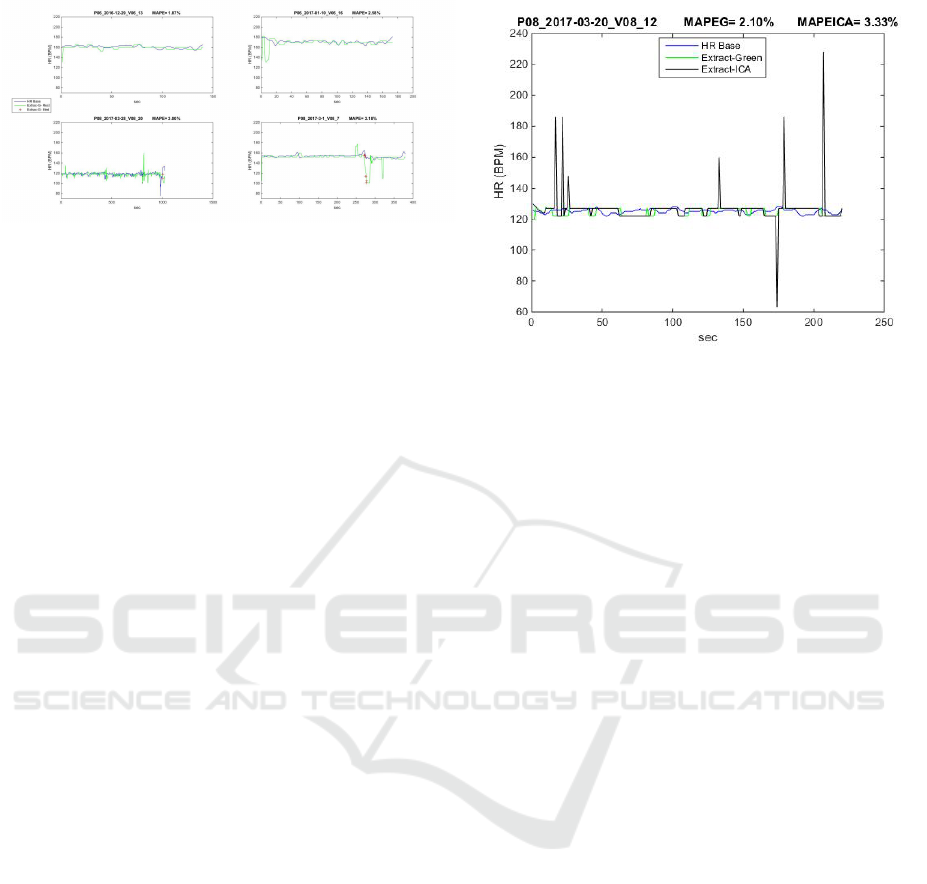
Figure 4: HEART RATE EXTRACTION EXAMPLES: Four
examples of HR extraction by the Green Channel method.
The title of each subplot has the source video name and
the MAPE. The HR monitor output (considered the ground
truth) is the blue line. The extracted HR is shown in green
when the baby is at ”rest” and in red plus when the baby is
”agitated” - as defined in Table 3.
Results: Both methods were tested on a sample of 10
recordings and gave acceptable heart rate estimates.
We compared the estimated heart rate with that of
the baby monitor, considered as ground truth, on a
second-by-second basis. The sample had a mean ab-
solute percentage error (MAPE) range of 3% to 8%
and standard deviation of 6% to 8% with increased
error during agitated (medium) baby motion. When-
ever our algorithm could not detect the baby face, we
considered that the signal has been lost. This usually
happens when the baby turns more than 45 degrees
away from the camera or when there is total occlu-
sion.
Figure 4 shows four sample results from the green
channel method with MAPE between 1.87% and
3.18%. The red crosses are the estimated HR at in-
stances when the baby is mildly agitated. The blue
and the green lines show the heart rates from the HR
monitor (the ground truth) and from the green channel
method respectively.
Figure 5 shows a sample comparison between the
green channel and the ICA methods. The mean ab-
solute percentage error for the green channel method
(MAPEG) is 2.1%, slightly less that that of the ICA
method (MAPEICA), 3.33%. We note that the chal-
lenge in the green channel method is its sensitivity to
the bandwidth selection to which the green signal
5 CONCLUSION
Automated early detection of physiological distur-
bances in newborns is essential for initiating therapy
as soon as possible. A contactless and non-invasive
system would be particularly helpful in vulnerable
populations such as sick neonates. This is a cross
sectional, observational study where all infants ad-
Figure 5: GREEN CHANNEL VS ICA HR EXTRACTION:
An example juxtaposing the ground truth HR (blue line)
from the attached monitor with both HR extraction meth-
ods, the Green Channel (green line) and the ICA method
(black line). The mean absolute percentage error for the
green channel method (MAPEG) is slightly less that that of
the ICA method (MAPEICA). In this recording of abour 3
minutes the baby is at ”rest” (see Table 3).
mitted to the NICU are eligible. After parent con-
sent, 127 video recordings of infants (total of 56hours
of recording) were obtained and analyzed. To estab-
lish the utility of the data set, the study performed
blind source separation (BSS) for detecting HR and
HR variability of infants admitted to the intensive
care unit. The estimated HR was compared to the
“ground truth” values of the regular monitors used in
the NICU. The testing results showed feasible heart
rate measurements on premature babies. There was
an average absolute error range of 3% to 8% and
standard deviation of 6% to 8% with increased error
during baby motion. As a conclusion, the proposed
method proves the utility of the dataset for vital sign
extraction. This technique proved beneficial for pa-
tient monitoring and we hope further work presents
techniques for early detection of diseases, leading to
earlier treatment and possibly improved outcome.
6 LIST OF ABBREVIATIONS
• NICU: Neonatal intensive care unit
• HR: Heart rate
• BSS: Blind source separation
• AUBMC American University of Beirut Medical
Center
• ROI: Region of interest
ICPRAM 2023 - 12th International Conference on Pattern Recognition Applications and Methods
772

7 DECLARATIONS
Ethics Approval and Consent to
Participate
All research procedures have been reviewed and ap-
proved by the institutional review board (IRB) at
the American University of Beirut Medical Center
(AUBMC). We obtained written consent statements
from the investigators and the participants. The in-
vestigator and participant consent statements follow.
Investigator’s Statement
I have reviewed and explained in detail, the informed
consent document for this research study with [name
of participant, legal representative or guardian/ parent
if the participant is a minor or is unable to sign] the
nature and purpose of the study and its risks and ben-
efits. I have answered to all his/her questions clearly
to the best of my ability. I will inform the participant
in case of any changes of this study or its negative
impacts or benefits in the event of their occurrence.
Consent to Participate
I have read this consent form and understood its con-
tent. All my questions have been answered. Accord-
ingly, I agree, with my own free will, to be part of
this research study, and I know that I can contact Dr.
Lama Charafeddine at 01-350000 Ext: 5874 or any
of her designee/assistant involved in the study in case
of any questions. If I feel that my questions have not
been answered or need further clarification I can con-
tact one of the members of the Institutional Review
Board for human rights or its chair Dr. Fouad Zyadeh
at 01-350000 Ext: 5445.
I understand that I am free to withdraw my con-
sent from this study and discontinue my participation
at any time, even after signing this form without prej-
udice to the medical care provided to me. I know that
I will receive a copy of this signed informed consent.
• I agree to participate in this study and authorize
the investigator and her designee the access to my
child’s AUBMC medical records
• I authorize the investigator and her designee to
contact me at a later stage for future follow-up if
needed.
Consent for Publication
We have obtained consent to publish de-identified and
anonymized versions of the data. We are only sharing
publicly areas of foreheads which do not include any
identification features.
Availability of Data and Material
The dataset supporting the conclusions of this arti-
cle is available in the American University of Beirut
research repository via the link: http://research-fadi.
aub.edu.lb/neonates/home.html.
Funding
Authors (LC, HS, and FZ) used Lebanese National
Council for Scientific Research Awards and Lebanese
Univeristy Research Funding Awards to hire research
assistants to complete the work. The funders did not
intervene in the process of the research work.
Authors’ Contributions
Authors JK and IK helped define and implement the
curation process. Authors HS and FZ helped define
and implement the curation process and the signal
processing process. Author LC defined and imple-
mented the clinical aspects and processes. All authors
contributed equally to the ideation and organization of
the manuscript, revised and approved the final version
of the manuscript.
ACKNOWLEDGEMENTS
We would like to thank the baby parents for their con-
sents in recording their newborns and recording them
on video, the engineers at the AUBMC for their co-
operation and help in setting up the medical monitor
equipment for data extraction and the nurses for their
patience and cooperation in the data collection pro-
cess.
REFERENCES
Alghoul, K., Alharthi, S., Al Osman, H., and El Sad-
dik, A. (2017). Heart rate variability extraction from
videos signals: Ica vs. evm comparison. IEEE Access,
5:4711–4719.
Christinaki, E., Giannakakis, G., Chiarugi, F., Pediaditis,
M., Iatraki, G., Manousos, D., Marias, K., and Tsik-
nakis, M. (2014). Comparison of blind source sepa-
ration algorithms for optical heart rate monitoring. In
2014 4th International Conference on Wireless Mo-
bile Communication and Healthcare - Transforming
Healthcare Through Innovations in Mobile and Wire-
less Technologies (MOBIHEALTH), pages 339–342.
Neonatal Video Database and Annotations for Vital Sign Extraction and Monitoring
773

Edmond, K. and Zaidi, A. (2010). New approaches to
preventing, diagnosing, and treating neonatal sepsis.
PLOS Medicine, 7(3):1–8.
Group, Y. I. C. S. S. (2008). Clinical signs that predict se-
vere illness in children under age 2 months: a multi-
centre study. The Lancet, 371(9607):135–142.
Liu, L., Johnson, H. L., et al. (2012). Global, regional, and
national causes of child mortality: an updated system-
atic analysis for 2010 with time trends since 2000. The
Lancet, 379(9832):2151–2161.
Lozano, R., Naghavi, M., et al. (2012). Global and re-
gional mortality from 235 causes of death for 20 age
groups in 1990 and 2010: a systematic analysis for
the global burden of disease study 2010. The Lancet,
380(9859):2095–2128.
Poh, M.-Z., McDuff, D. J., and Picard, R. W. (2010). Non-
contact, automated cardiac pulse measurements using
video imaging and blind source separation. Opt. Ex-
press, 18(10):10762–10774.
Sztajzel, J. (2004). Heart rate variability: A noninva-
sive electrocardiographic method to measure the auto-
nomic nervous system. Swiss Medical Weekly, pages
514–522.
Task Force of the European Society of Cardiology the
North American Society of Pacing Electrophysiology
(1996). Heart rate variability. task force of the euro-
pean society of cardiology the north american society
of pacing electrophysiology. Circulation, 93(5):1043–
1065.
Wu, H.-Y., Rubinstein, M., Shih, E., Guttag, J., Durand, F.,
and Freeman, W. (2012). Eulerian video magnifica-
tion for revealing subtle changes in the world. ACM
Trans. Graph., 31(4):65:1–65:8.
ICPRAM 2023 - 12th International Conference on Pattern Recognition Applications and Methods
774
