
Low Profiled Angiographic Catheter with Enhanced Pushability and
Flexibility: A Novel Design, Fabrication, and in-Vitro Analysis
Hafsa Inam, Murtaza Najabat Ali and Aimen Arshad
Biomedical Engineering and Sciences Department, School of Mechanical and Manufacturing Engineering (SMME),
National University of Sciences and Technology (NUST), Islamabad, Pakistan
Keywords: Laser-Cut Reinforced Shaft, Laser-Cut Torque Transfer Layer, Angiographic Catheter, Corrosion-Resistant,
Burst Test, Leak Test, Tensile Strength, Flow Rate, Performance Testing.
Abstract: The diagnostic angiographic catheter (DAC) available in the market have improved the survival rate and are
the result of extensive R&D, but there’s still room for improvement in terms of catheter profile, enhanced
pushability, and trackability therefore, the current research focuses on the development of laser-cut reinforced
shaft catheters in an attempt to design a low-profile DAC with enhanced pushability and trackability. A new
‘I’ hollow geometry has been used to fabricate reinforced shafts. Stainless Steel 304 was selected as a material
to fabricate a laser-cut reinforced shaft and PTFE and PEBAX
®
for inner lumen and catheter jacketing. This
study analyzes and reports the design, performance, and behavior of laser-cut reinforced shaft catheters. The
‘I’ geometry of laser-cut reinforced shaft catheter differed from braided catheters based on ovality retention,
enhanced flexural rigidity, and pushability; the pushability force analysis results prove that laser-cut
reinforced shaft catheter exerts a minimal resistive force which is approximately 1/3
rd
times less than the
braided catheter. This study also endeavored to manufacture a significantly lower wall thickness for reinforced
angiographic catheters. Based on this extensive in-vitro assessment, it has been concluded that laser-cut
reinforced shaft catheter performed better in advancement force and flexibility than the braided catheter. In
performance evaluation, the laser-cut reinforced shaft catheter has outperformed 16 and 32 wires braided
catheters, exhibiting an exceptionally minimal pushability force of 6.25 N.
1
INTRODUCTION
Atherosclerosis is the buildup of plaque inside
coronary arteries; as plaque continues to accumulate
in artery walls, arteries tend to stiffen, causing
narrowing and blockage of arteries, and not getting
enough blood supply to the heart muscle can lead to
chest pain (Mozaffarian D, 2016) (Roth, 2017)
(Prabhakaran D, 2018) (Moran AE, 2014) (Sampasa-
Kanyinga H, 2015) (Heart, 2022), (Lappegård,
Kjellmo, & Hovland, 2021), (Lorkowski & Smith,
2022), (Kostromina, et al., 2022).
The major advantage of coronary angiography is
precisely identifying the narrowed artery leading to
the instantaneous decision of requirement of coronary
angioplasty or stent implantation. Angiography has
evolved into a safe and frequently used component of
cardiac catheterization due to advancements in
catheter design, radiographic imaging, contrast
media, and the introduction of therapeutic choices for
the treatment of coronary artery disease. (Baim,
1986), (Ghelfi et al., 2022).
Immediate complications during coronary
angiography include problems with an angiographic
catheter such as catheter advancement, pushability,
kinking trackability, torqueability, vascular damage,
perforation site pain, and discomfort; later
complication includes vascular spasm, tissue damage
caused by X-ray radiation if the procedure is
prolonged, damage to the kidneys caused by the
contrast dye, and heart attack. (NHS, 2021), (Liao, et
al., 2022). Laser-cut tubing (LCT) uses a focused
laser to ablate through a metal or polymer tube wall
before removing the deteriorated material using a
high-pressure coaxial gas nozzle. For more than 30
years, the method has been employed in medical
device manufacture, with substantial breakthroughs
following the push for miniaturization for minimally
invasive treatments (Kevin Hartke, 2020). A
mechanism to achieve a laser-cut catheter-reinforced
shaft was theoretically introduced by Liam (Liam
Inam, H., Ali, M. and Arshad, A.
Low Profiled Angiographic Catheter with Enhanced Pushability and Flexibility: A Novel Design, Fabrication, and in-Vitro Analysis.
DOI: 10.5220/0011633700003414
In Proceedings of the 16th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2023) - Volume 1: BIODEVICES, pages 29-36
ISBN: 978-989-758-631-6; ISSN: 2184-4305
Copyright
c
2023 by SCITEPRESS – Science and Technology Publications, Lda. Under CC license (CC BY-NC-ND 4.0)
29
Farrissey, 2004) previously, based on the variable
pitch of the proximal and distal end of the catheter’s
shaft as the proximal end requires more stiffness and
enhanced pushability, whereas distal end requires
flexibility.
This research work, laser-cut angiographic
catheter, was inspired by the laser-cut hypotubes,
which are being used in angioplasty catheters, as first
mentioned by Liam Farrissey in 2004, who explained
the requirement of variable flexibility and stiffness
throughout the length of the catheter. Therefore, this
research work aims to develop a novel manufacturing
approach comprising disruptive manufacturing and
additive manufacturing techniques to produce a laser-
cut reinforced layer, also known as torque transfer
layer and laser-cut reinforced angiographic catheter.
This study also endeavored to manufacture a
significantly thin-walled angiographic catheter.
The structural parameters of the catheter of this
research are critical in achieving kink-free,
pushability, and flexibility. Higher values for the ‘I’
slotted pattern and higher pitch between rows of
slotted ‘I’ can provide more flexibility and, therefore,
better torque response to rotating the distal end of the
catheter as per the cardiologist’s need. The use of
lumen and jacket polymer coatings (which may
extend into and interface with each other through the
laser-cut lines) allows the ‘I’ slotted pattern to flex
without plastic deformation. Thus, a closer pitch in
the distal end will enhance flexibility which is
desirable while moving through tortuous anatomy.
2
MATERIAL AND METHODS
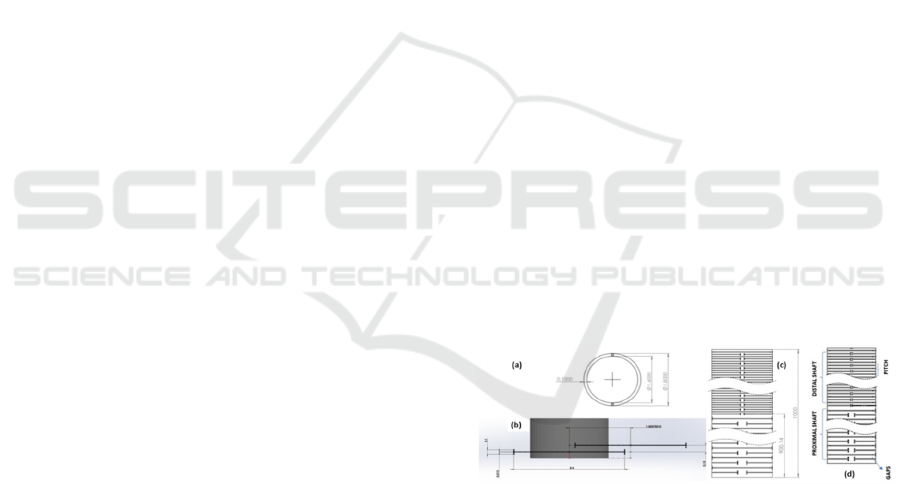
2.1 Design Considerations of the
Catheter shaft
The design of catheter geometry of the present laser-
cut catheter reinforced shaft is built with a plurality of
unit cells shown in Figure 1(b), interconnected with
the help of horizontal and vertical edges to form an
‘I’ pattern and gaps. The design width (DW) and
design length (DL) of the ‘I’ pattern remain the same;
however, the pitch varies from proximal to the distal
end. The proximal and distal shaft dimensions are 900
mm and 100mm, respectively. The tube has a 1.8mm
outer diameter having a wall thickness of 0.1mm
(Hafsa Inam, 2022).
To develop a hollow ‘I’ patterned geometry and
configure it into a tubular reinforced layer form,
Stainless Steel 304 was selected as a material.
PEBAX
®
and PTFE hollow tubes were acquired to
construct ‘I’ patterned reinforced shaft geometry into
a laser-cut reinforced catheter configuration. The
inner lumen of the catheter was lined with thin-walled
polytetrafluoroethylene (PTFE), as it has a lower
coefficient of friction to reduce the advancement
resistance when going through the mock vascular
system. Flouropeels heat shrink extruded tube was
acquired to fuse all polymeric layers to the laser-cut
reinforced shaft for the development of the catheter.
2.1.1 Development of Laser Cut Shaft for
Angiographic Catheter
Laser Cutting of the Catheter’s Reinforced Shaft
The thermo-mechanical cutting method by
computerized numerical control (CNC) guided laser
was adopted to fabricate a laser-cut reinforced
catheter shaft (Silvio Genna, 2020). The laser cutting
method employed in this study was further optimized,
and the fabrication of the catheter reinforced shaft
was conducted on a realistic size of 6 French
angiographic catheters. Medical grade stainless steel
304 tube, commercially known as “18-8 stainless
steel,” was procured from Hechuang Hitech China
based on its highly anti-corrosive and durable
properties (Medical Grade & Surgical Stainless Steel,
2022); these hollow ‘I’ patterned geometry was
manufactured specifically for medical applications.
The stainless steel 304 tube was 0.1mm thick, as
illustrated in Figure 1 (c), and the overall length of the
reinforced tube was 1000mm, as illustrated in Figure
1 (d).
Figure 1: (a) Outer Diameter, Inner Diameter and Wall
Thickness of Metallic tubing (b) The unit cell is hollow ‘I’
pattern (b) ‘I’ hollow pattern measurements (c) The
geometry for the proximal and distal end of the
angiographic catheter’s reinforced shaft (d) Illustration of
'I' pattern drawing from proximal to the distal end of
catheter reinforced tubing. To fabricate an ‘I,’ pattern laser-
cut catheter reinforced shaft, a Star Cut CNC guided laser
system was used; the in-process image is shown in fig.2 (a).
The 2D hollow ‘I’ geometry DXF design was fed into
high precision fiber laser cutting machine’s software,
Preco RT1000, and the laser system emitted optical
energy in an invisible infrared beam. The laser system
BIODEVICES 2023 - 16th International Conference on Biomedical Electronics and Devices
30
used a laser power of around 150W to cut the
workpiece material.
Process of Acid Pickling
Acid pickling solution (150 mL) for the laser-cut
reinforced tube was prepared using pickling solutions
consisting of hydrofluoric acid and nitric acid. The
catheter tubing was immersed in 150 mL of pickling
solution and ultrasonicated for 15 mins.
Subsequently, the laser-cut catheter tubing was rinsed
with warm water and air-dried. The whole process is
shown in Figure 2(b, c, d).
Passivation Process
The passivation solution consisted of nitric acid as it
is an oxidizing acid and is always used. Acid-pickled
laser-cut tubing was dipped in the nitric acid solution
for 5 minutes to create a passivated layer; catheter
tubing was removed, washed with DI water, and dried
with air, as shown in Figure 2(e, f, g).
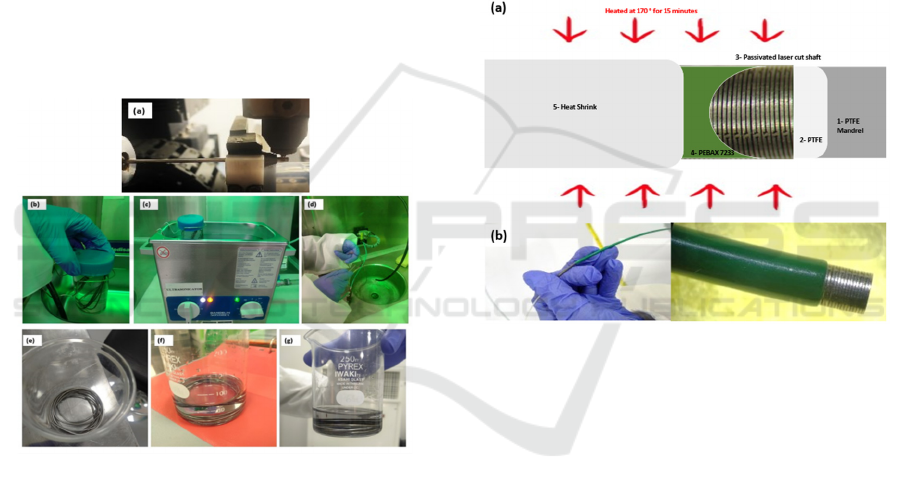
Figure 2: (a) Laser-cutting of catheter reinforced shaft (b, c,
d) Acid Pickling processes & (c, d, and f) passivation
processes of the laser-cut reinforced shaft.
2.1.2 Development of Laser Cut
Angiographic Catheter
PEBAX
®
7233 extruded jacket tubing and the PTFE
inner lumen were sourced from Zeus (USA). PTFE
monofilament mandrel having an outer diameter of
1.57mm was used as the inner lumen. A peelable
heat-shrink tubing was used as an external layer to
facilitate polymer fusion to laser-cut catheter-
reinforced shaft.
Thermal Fusion of Polymeric Jacket and PTFE
Extruded Tubing
In this process, PTFE, as the inner lining of the
catheter-reinforced shaft, mounted on a PTFE
mandrel, was inserted in passivated laser-cut catheter-
reinforced shaft. An extruded PEBAX
®
jacketing,
7233 (72D durometer), was used to cover the
reinforced shaft. A heat shrink, having an inner
diameter of 2.10mm, was used as an external layer to
combine the whole material. The arrangement is
illustrated in Figure 3(a). The whole shaft was then
exposed to 170°C for 15 minutes in a pre-heated
forming oven. After completing the process, the
catheter tubing was cooled down, and heat shrink was
removed. The polymer-fused catheter-reinforced
shaft is shown in Figure 3(b).
Figure 3: Illustration of the polymeric and metallic layer
layering, depicting heat fusion process (b) Polymeric jacket
fusion on the laser-cut reinforced shaft after removal of
heat-shrink tubing.
Soft Tip and Distal Tube Shaping of Novel
Angiographic Catheter Shaft Using a
Thermoforming Process
The preparation of a novel angiographic catheter was
conducted by welding a soft tip, PEBAX® 35D
durometer (CUUMED Taiwan), and tapering. A
female luer lock, polycarbonate, was attached at the
proximal end using Loctite, a medical-grade glue. To
shape the distal end of the catheter, the catheter shaft
is assembled in Judkins right die Figure 4 (a); the
whole shaft was then placed in a pre-heated
longitudinal oven at 150°C for 15 minutes using
assembling mandrels, Figure 4 (b, c). After
completing the distal shaping process, the catheter
was removed from the thermoforming machine and
eventually from forming die.
Low Profiled Angiographic Catheter with Enhanced Pushability and Flexibility: A Novel Design, Fabrication, and in-Vitro Analysis
31

Figure 4: (a); the whole shaft was then placed in a pre-
heated longitudinal oven at 150°C for 15 minutes using
assembling mandrels, (b, c). After completing the distal
shaping process, the catheter was removed from the
thermoforming machine and eventually from die.
3
RESULTS
3.1 Characterization, in Vitro
Mechanical and Performance
Testing
The novel reinforced DAC was characterized, and its
performance was evaluated in comparison with a
commercially available catheter. In vitro mechanical
testing was carried out to analyze and evaluate the
mechanical performance of the laser-cut reinforced
shaft and laser-cut reinforced angiographic catheter.
A hemolysis test was carried out as per ASTM F756,
physical tests were carried out as per ISO 10555-
1:2013+A1:2017, and pushability testing was carried
out on a mock arterial system developed on ASTM
F2394.
3.2 Statistical Analysis
All experimental approaches were executed in
triplicates. Results are represented as mean ± standard
deviation, n ≥ 3. Statistical analysis was done to
analyze the differences between the experimental
results, and a value of p < 0.05 was considered
significant.
3.3 Analysis of Laser-Cut Metallic
Shaft Fabrication
Formation of ‘I’ Geometry Pattern
The laser-cut reinforced shaft design pattern
comprising a hollow ‘I’ pattern was cut by
interpolating 304 stainless steel tubing movements in
both linear and rotational directions. A thin stainless-
steel tubing of 0.1mm thickness with hollow ‘I’
geometry is shown in
Figure
Figure 5(a). The
reinforced shaft has wider gaps in the proximal end
whereas tighter gaps in distal end making distal end
of reinforced metallic shaft more flexible.
Effect of Pickling on the Laser-Cut Reinforced
Shaft Design
Acid pickling is the smoothest method to remove slag
and impurities from metallic surfaces. Slag was
removed from the laser-cut metallic reinforced shaft
during the acid pickling process as the smoother
surface of the acid pickled shaft is shown in Figure 5
(b). After acid pickling, the unit cells (hollow I
pattern) and laser-cut metallic reinforced shaft
geometry were visible.
Achievement of Passivation
The surface peaks and valleys (i.e., surface
roughness) were removed, and material reduction and
surface smoothness were obtained by dipping the
laser-cut metallic shaft in passivation solution
consisting of nitric acid. As depicted below in Figure
5 (c), the surface definition and characteristics were
significantly improved after passivation.
Figure 5: (a) 'I' patterned geometry of Laser Cut Metal Shaft
(Proximal and Distal End of Angiographic Catheter) (b and
c) Effect of pickling on the laser-cut reinforced shaft design
(slags were removed) (d and e) Effect of passivation on the
laser-cut reinforced shaft design (the shaft surface was
passivated).
Quantitative analysis was conducted by Ultraviolet
(UV) Spectrophotometry at 550nm wavelength of the
supernatant as the absorbance range of hemoglobin is
520-550nm. As shown in Figure 6, the quantitative
analysis results revealed that the laser-cut reinforced
shaft showed 1.27%. The laser-cut reinforced catheter
showed 1.48% hemolysis while negative control with
0% hemolysis. The laser-cut reinforced shaft and
laser-cut reinforced catheter cause <2% hemolysis
BIODEVICES 2023 - 16th International Conference on Biomedical Electronics and Devices
32

when directly encountering blood, as presented in
Figure , categorizing them as non-hemolytic (ASTM
F756, 2017).
Figure 6: Hemolysis Testing of Laser Cut Reinforced Shaft
& Catheter. The laser-cut reinforced shaft and laser-cut
reinforced catheter cause <2% hemolysis when directly
encountering blood, categorizing them as non-hemolytic.
Initially, a laser-cut metallic reinforced shaft was
used to prepare the tubing from the proximal and
distal end to measure the baseline tensile data of the
laser-cut metallic reinforced shaft material as per ISO
10555-1. Therefore, two catheter specimens,
proximal and distal end, were prepared by carefully
cutting the catheter tubing, 10.0mm long, having an
outer diameter of 2.00mm. A SHIMADZU AG-X
plus series tensile tester was used in this study. The
equipment was initially calibrated, and the laser-cut
metallic reinforced shafts specimen from the
proximal and distal ends were then evaluated. The
same test was repeated twice, and the mean of the
baseline stress-strain data for the proximal and distal
end of laser-cut metallic tubing was taken. After
getting the baseline data, the proximal and distal end
of the catheter specimen was tested. The proximal end
of catheter tubing exhibits a higher stress/strain ratio
than the distal end, as shown in Figure 7.
Figure 7: Stress/Strain Curve of Laser Cut Reinforced shaft,
laser-cut reinforced catheter, and hollow PEBAX tubing.
Tensile strength of laser-cut reinforced catheter along
with laser-cut metallic reinforced shaft was carried
out, and optimal results were received, compared with
Dxterity
™
Medtronic (Medtronic, 2016), a fully
braided catheter, having round-wire braid
configuration of 2x1 (32 wires). Infiniti Cordis
®
and
Angiodyn
®
BBraun consist of the non-braided distal
end. Upon comparison with the fully reinforced laser-
cut angiographic catheter, Infiniti
®
Cordis and
Angiodyn
®
BBraun, Dxterity
™
(Figure 8) exhibited a
tensile strength of 16.24g, Angiodyn
®
experienced
33.8g, and Infiniti
®
experienced 22.7g. The laser-cut
reinforced catheter exhibits 37.4g stress which is
most significant compared to commercial catheters.
Figure 8: Stress/Strain of Commercial Catheters (Infiniti
Cordis, Angiodyn BBraun, Dxterity Medtronic).
The laser-cut reinforced catheter yielded an average
flow rate of 63.17mL/minute, as shown in Figure 9 as
per ISO 10555-1 standard requirement.
Figure 9: Laser cut Catheter - Flowrate (ml/min).
Figure 10 (a) exhibits the flexural rigidity of the
proximal and distal end of the laser-cut metallic shaft,
where the distal end experienced a maximum force of
5.0g when moved to 90-0°. In contrast, the proximal
end experienced a maximum force of 15.0g.
63,17
60,5
58
59
60
61
62
63
64
Laser Cut Reinforced
Catheter
DxTerity, Medtronic
Flowrate (mL/min)
Samples
Flowrate (mL/min)
Low Profiled Angiographic Catheter with Enhanced Pushability and Flexibility: A Novel Design, Fabrication, and in-Vitro Analysis
33
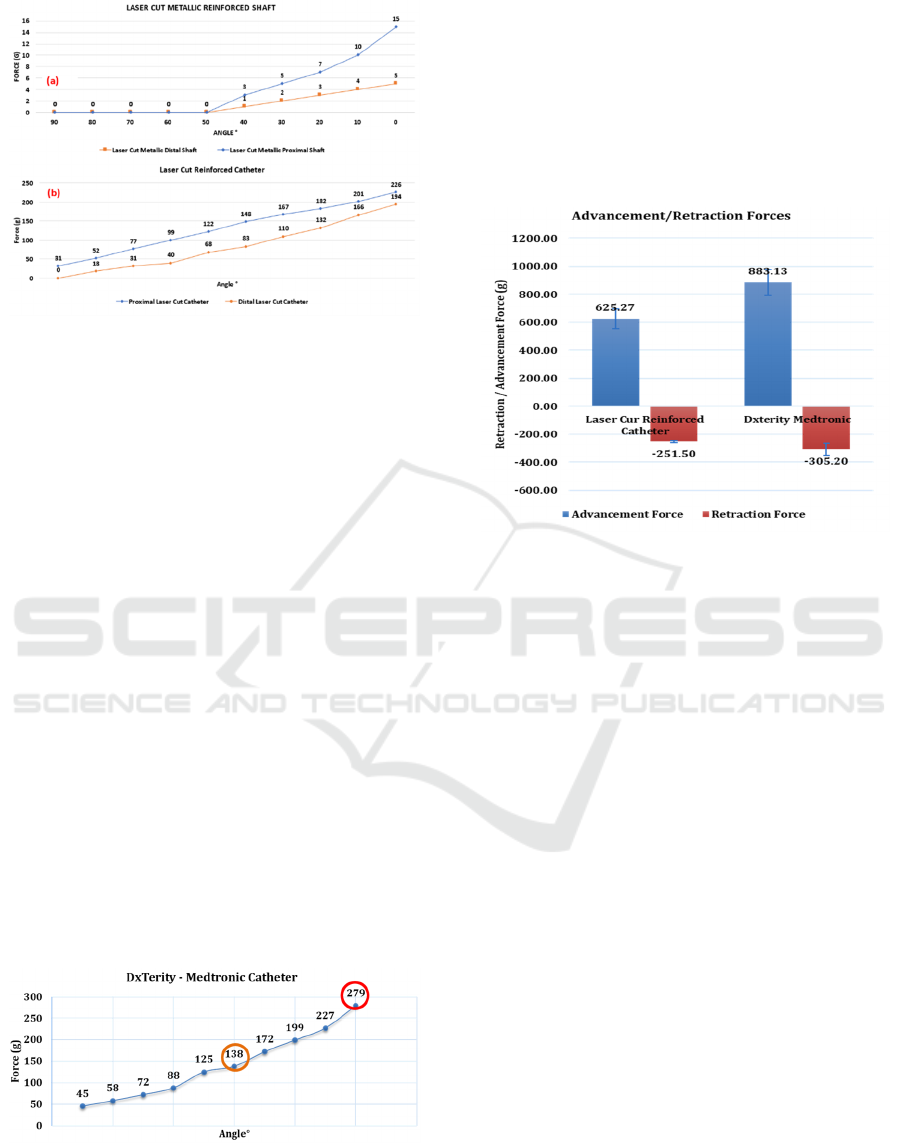
Figure 10: (a) Flexural Rigidity of Proximal and Distal end
of Laser-Cut Metallic Shaft, The proximal end of the laser-
cut reinforced catheter experienced a maximum force of
15.0g when moved from 90-0°, whereas the distal end of
the laser-cut reinforced catheter experienced a maximum
force of 5.0 g (b) Flexural Rigidity of Proximal and Distal
end of Laser-Cut Reinforced Catheter, The proximal end of
the laser-cut reinforced catheter experienced a maximum
force of 226.0g when moved from 90-0° whereas the distal
end of the laser-cut reinforced catheter experienced a
maximum force of 194.0g.
Figure 10(b) illustrates the flexural rigidity of the
distal and proximal end of the laser-cut reinforced
catheter. The proximal end of the laser-cut reinforced
catheter experienced a maximum force of 226.0g
when moved from 90-0°. In contrast, the distal end of
the laser-cut reinforced catheter experienced a
maximum force of 194.0g, which is less than the
proximal shaft. These results depict the distal end as
more responsive to external forces than the proximal
end of the catheter, whose characteristic is to maintain
its patency when subjected to external stresses.
Kinks usually occur with counterclockwise
rotation when trying to engage the left coronary artery
and with clockwise rotation when engaging the right
coronary artery. The best prevention is to refrain from
rotating the catheter more than 180° to prevent the
Figure 11: Dxterity™ Medtronic double braid (2x1, 32
wire) began to kink, and loss of ovality initiated at 40°
(shown in green circle), and kinking, loss of braid ovality
and integrity were noted at 0° (shown in red circle).
build-up of torque proximally that is not transmitted
to the catheter tip (Itsik Ben-Dor, 2018).
Laser-cut reinforced catheter exhibited an average
advancement force of 624.97g. Dxterity exhibited an
average advancement force of 882.9g. 29.2% lesser
advancement force was used to push the catheter to
the required point. 17.6% reduced retraction force
was recorded during retraction.
Figure 12: Laser-cut reinforced catheter exhibited an
average advancement force of 624.97g. Dxterity exhibited
an average advancement force of 882.9g. 29.2% lesser
advancement force was used to push the catheter to the
required point. 17.6% reduced retraction.
Along with a laser-cut reinforced catheter, Dxterity
Medtronic was also evaluated; the distal shaft is
hydrophilic coated to evaluate a fully braided catheter
performance where it experienced a maximum
resistive force of 922.1g and a retractive force of -
402.3g. However, laser-cut reinforced catheters and
Dxterity catheters lost their distal shapes after
continuous usage.
4
DISCUSSION
The objective of this study was twofold: (I) designing
and manufacturing a laser-cut metallic reinforced
shaft in a novel way and (II) configuring this laser-cut
metallic shaft as a laser-cut reinforced catheter for
radiopaque media delivery.
The stiffness and flexural rigidity of various shafts
may be assessed using two and three-point bend tests
or other deflection-based techniques. With this
knowledge, the stiffness of the adjacent shafts may be
adjusted to provide a virtually perfect transition. The
laser-cut metallic catheter shaft and laser-cut
reinforced catheter, as shown in Figure 10, exhibit the
flexural rigidity of the proximal and distal end of a
BIODEVICES 2023 - 16th International Conference on Biomedical Electronics and Devices
34

laser-cut metallic shaft, where the distal end
experienced the maximum force of 5.0g when moved
to 90-0°, whereas proximal end experienced a
maximum force of 15.0g. Figure 10 illustrates that the
proximal end of the laser-cut reinforced catheter
experienced a maximum force of 226.0g when moved
from 90-0°, whereas the distal end of the laser-cut
reinforced catheter experienced a maximum force of
194.0g, which is less than the proximal shaft. To
deliver radiopaque media to coronary arteries, high
pressures are required. The laser-cut reinforced
catheter must maintain lumen patency and endure
high pressure to avoid any vessel injuries. Laser-cut
reinforced catheter can endure 1000psi static burst
pressure and power injection pressure of 1200psi
when evaluated on a liquid pressure tester; however,
the simulation study of the design exhibited
endurance till 700psi (Inam, 2022). Injecting
radiopaque media multiple times during an
angiographic intervention might become necessary.
Therefore, not only flexible behaviours but also
pressure endurance is important.
In this study, due to the limited availability of
medical extruders, the direct extrusion method can be
adopted to develop angiographic catheters so that cost
and time can be saved.
5
CONCLUSIONS
As the medical device industry is evolving at a higher
pace, there is a great need to improve the
angiographic treatment of coronary heart disease
patients suffering from narrowed coronary arteries.
All available angiographic catheters are braided in
nature; the flat and round wire braids are used as a
sandwich layer between two polymeric layers. There
are mainly three costs involved in the placement of an
angiographic catheter to the targeted site (i)
fluoroscopic guidance, (ii) angiographic catheter, and
(iii) patient-specific radiopaque dye. Furthermore,
due to the compromised radial strength and
flexibility/ pushability tradeoff within a low-profile
angiographic catheter, catheters may require a few
episodes of retraction to reach the targeted site. This
research was conducted with the aim of using the
unique hollow ‘I’ pattern geometry for the
development of a novel laser-cut metallic reinforced
shaft and laser-cut reinforced angiographic catheter,
which demonstrates to provide better pushability of
625 0g, keeping catheter profile to lower end. One of
the critical questions addressed in this research is the
deployment of the significantly lower profile,
2.00mm outer diameter of the catheter without
compromising pushability and flexibility. The
fabrication route also determines the enhancement of
hydrophilicity.
The outcome of the comparative analysis, which
was conducted based on the results obtained from the
manufacturing and surface characterization study,
clearly showed that the laser cutting method is an
effective and rapid way of producing flexible, lower-
profile reinforced shaft. It was also established that
laser cutting of stainless-steel tubes to produce
flexible lower profile reinforced shaft would avoid
the problem of continuous ovality throughout. The
distal tube shaping of the laser-cut angiographic
catheter by complete thermal exposure was found to
be more efficient and enhanced the hydrophilic
properties of the catheter (71.3° angle depicts
hydrophilicity of the catheter). It is envisaged that the
laser-cut reinforced angiographic catheter comprising
of variable geometry patterns from proximal to the
distal end provides betters flexibility and flexural
rigidity of an average of 210g without compromising
on the advancement force; this feature of the laser-cut
reinforced catheter has an advantage over the
commercially available braided catheter. Building on
the current findings, clinical studies on the robust use
of this catheter as part of a radiopaque media delivery
functionality in medical devices may be conducted.
REFERENCES
ASTM F756. (2017, april 19). Standard Practice for
Assessment of Hemolytic Properties of Materials.
ASTM F756-17. ASTM.
Baim, D. &. (1986). Coronary angiography. In M. Mauro
Moscucci MD, Cardiac Catheterization, Angiography,
and Intervention. Philadelphia, USA.
Ghelfi, J., Bacle, M., Stephanov, O., de Forges, H.,
Soulairol, I., Roger, P., Frandon, J. (2022).
Collagenase-Induced Patellar Tendinopathy with
Neovascularization: First Results towards a Piglet
Model of Musculoskeletal Embolization. Biomedicines.
Hafsa Inam, M. N. (2022). Design Development and
Modeling of the Laser-Cut Reinforced Shaft for
Radiopaque Media Delivery to Coronary Artery Using
Finite Element Method: Laser cut catheter reinforced
shaft." . 12th International Conference on Bioscience,
Biochemistry and Bioinformatics (pp. 101-107). Tokyo
Japan: ACM.
Heart, A. (2022, 13 02). American Heart Association
Coronary Artery Disease – Coronary Heart Disease.
Retrieved from heart.org: https://www.heart.org/en/
health-topics/consumer-healthcare/what-is-
cardiovascular-disease/coronary-artery-disease
Low Profiled Angiographic Catheter with Enhanced Pushability and Flexibility: A Novel Design, Fabrication, and in-Vitro Analysis
35

Inam, H. N. (2022). Design Development and Modeling of
the Laser-Cut Reinforced Shaft for Radiopaque Media
Delivery to Coronary Artery Using Finite Element
Method: Laser cut catheter reinforced shaft. . 12th
International Conference on Bioscience, Biochemistry
and Bioinformatics. Tokyo, Japan: ACM.
Itsik Ben-Dor, T. R. (2018). Reduction of catheter kinks
and knots via radial approach. Catheter
CardiovascInterv., 1141–1146.
Kevin Hartke. (2020, January). Enhanced catheter
performance made possible with laser cut tubing.
Retrieved from https://resonetics.com/wp-content/
uploads/2020/03/Laser-Cut-Tubing-White-Paper-.pdf
Kostromina, M., Tukhovskaya, E., Shaykhutdinova, E.,
Slashcheva, G., Ismailova, A., Palikov, V., . . .
Lykoshin. (2022). Screening of the Promising Direct
Thrombin Inhibitors from Haematophagous
Organisms. Part I: Recombinant Analogues and Their
Antithrombotic Activity In Vitro. . Biomedicines .
Lappegård, K., Kjellmo, C., & Hovland, A. (2021). High-
Density Lipoprotein Subfractions: Much Ado about
Nothing or Clinically Important? . Biomedicines.
Liam Farrissey. (2004, December). Metal Shafts: Designs
To Meet The Required Performance. Retrieved from
Creganna: https://www.creganna.com/wp-content/up
loads/metalshaft.pdf
Liao, M.-T., Lai, C.-L., Wang, T.-C., Lin, J.-W., Ho, Y.-L.,
& Chan, K. (2022). Red Cell Distribution Width and
Mortality in Patients Undergoing Percutaneous
Coronary Intervention. . Biomedicines .
Lorkowski, S., & Smith, J. (2022). HDL Is Not Dead Yet. .
Biomedicines .
Medical Grade & Surgical Stainless Steel. (2022).
Retrieved from Bergsen Medical: https://berg
sen.com/medical-surgical-stainless-steel
Medtronic. (2016). DxTerity™ diagnostic catheters.
Retrieved from https://www.medtronic.com/us-en/
healthcare-professionals/products/cardiovascular/cathe
ters/dxterity.html
Moran AE, F. M. (2014). Temporal trends in ischemic heart
disease mortality in 21 world regions, 1980 to 2010: the
Global Burden of Disease 2010 study. . Circulation.,
1483–1492.
Mozaffarian D, B. E. (2016). Heart disease and stroke
statistics-2016 update. A report from the American
Heart Association. Circulation. .
NHS. (2021, 12 03). Risks, Cardiac catheterisation and
coronary angiography. Retrieved from NHS: https://
www.nhs.uk/conditions/coronary-angiography/risks/
Prabhakaran D, J. P. (2018). The changing patterns of
cardiovascular diseases and their risk factors in the
states of India: the Global Burden of Disease Study
1990-2016. Lancet Glob Health., 1339–1351.
Roth, G. A.-A. (2017). Global, regional, and national
burden of cardiovascular diseases for 10 causes, 1990
to 2015. Journal of the American college of cardiology.
Sampasa-Kanyinga H, L. R. (2015). Frequent use of social
networking sites is associated with poor psychological
functioning among children and adolescents. .
Cyberpsychology Behav Soc Netw. , 380–385.
Silvio Genna, E. M. (2020). Experimental Investigation of
Industrial Laser Cutting: The Effect of the Material
Selection and the Process Parameters on the Kerf
Quality. Applied Sciences , MPDI.
BIODEVICES 2023 - 16th International Conference on Biomedical Electronics and Devices
36
