
Artificial Intelligence Enabled Healthcare Ecosystem Model:
AIEHEM Project
Luigi Lella
1
, Ignazio Licata
1
and Christian Pristipino
2
1
ISEM, Ins. For Scientific Methodology, PA, Italy
2
Interventional and Emergency Cardiology Unit, San Filippo Neri –ASL Roma 1, Rome, Italy
Keywords: Healthcare Management Systems, Data Mining and Data Analysis, Decision Support Systems.
Abstract: The AIEHEM project aims to analyze the data made available by the regional health system, using an
unorganized Turing machine model (A-Type) trained with a swarm-evolutionary hybrid algorithm. The goal
is to identify the main factors related to certain outcomes that the healthcare organization intends to achieve
(which can be economic, organizational, social or environmental). The chosen AI model is used to enhance,
not to replace the analytical capabilities of the healthcare system management. The insights of the AI model
are in fact used not only to identify the main objects of study to be taken into consideration, but also to
define the areas of intervention and consequently also the stakeholders to be involved in the organizational
change project to be carried out through the Theory of Change methodology. AI is therefore used to identify
the most suitable ecosystem for solving the considered problem.
1 INTRODUCTION
The development of decision support systems (DSS)
is a potentially gamechanger for executives and
managers of health systems and organizations
because they offer the possibility of managing an
elevate number of variables (Longaray et al., 2016;
Khademolqorani and Hamadani, 2015). These
particular DSSs are indeed characterized by a high
level of complexity that leads to the definition of
groups or hierarchies of variables to be taken into
account to solve certain critical issues and problems.
As health is a good of a fundamental and
irreplaceable nature (Diaby et al., 2013), there is a
high level of responsibility in the decision of
adopting IT solutions to support management. This
is particularly true if one considers that wrong
management decisions can directly endanger
patients, but it can also happen that the improvement
of the medical state of some patients can negatively
affect that of other patients (Marsh et al., 2014).
Unfortunately, such DSSs are often based on
machine learning and AI algorithms working as
"black boxes", where the assumptions of their
predictions and/or choices are concealed (Academy
of Medical Royal Colleges, 2019). This increases the
difficulty in assessing the degree of reliability of
such systems, making them particularly vulnerable
to bias and deliberately malicious attacks.
Among the main machine learning and AI
models used to implement DSSs are algorithms
based on decision trees, linear and logistic
regression, Bayesian inference and classification
(Bashir et al., 2014; Zandi, 2014; Roumani et al.,
2013).
Such systems often use Multicriteria Decision
Analysis methods (MCDA) and Multicriteria
Decision Making methods (MCDM) (Aghdaiea et al.
2014).
MCDAs are algorithms that allow to simplify
complex problems by bringing them back to a series
of elementary criteria to be considered in finding the
solution (Angelis et al., 2017). In recent decades,
MCDAs have been applied in various areas
including the management of health systems
(Longaray et al., 2016). Specifically, they have been
used in the clinical (Gasol et al., 2022; Berner, 2007)
and in the health management fields (Marsh et al.,
2014; Ju et al., 2012; Wu et al., 2007; Baltussen et
al, 2006).
MCDMs are algorithms that allow to find
solutions in the presence of multiple objectives (San
Cristobal, 2013) and also have been used been used,
among others, in the clinical (Bashir et al. 2014) and
232
Lella, L., Licata, I. and Pristipino, C.
Artificial Intelligence Enabled Healthcare Ecosystem Model: AIEHEM Project.
DOI: 10.5220/0011604300003414
In Proceedings of the 16th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2023) - Volume 5: HEALTHINF, pages 232-238
ISBN: 978-989-758-631-6; ISSN: 2184-4305
Copyright
c
2023 by SCITEPRESS – Science and Technology Publications, Lda. Under CC license (CC BY-NC-ND 4.0)

in the health management fields (Narci et al., 2014;
Ishizaka and Nemery, 2013).
Both MCDAs and MCDMs work by grouping or
ranking possible alternative solutions to
administrative problems. For this reason they also
behave like decision-making black boxes that hide
the criteria that guided the choice of the suggested
solution, as well as the biases and all the other
factors that influenced the selection. Therefore, it is
crucial instead to develop algorithms that may help
in explaining the causal links between the variables
considered in the identification of the solution. This
will allow a posteriori to verify whether the
automated decision-making process has been based
on a sufficient number of data, whether these are
characterized by a sufficient level of quality and
consistency, whether or not their selection has been
influenced by cognitive biases. Indeed, a simplified
logical representation of the causal links between the
key variables selected by the DSSs, can help human
decision-makers in assessing the reliability of the
system and in making the most appropriate
decisions.
All these considerations led to the definition of
the project called "Artificial Intelligence Enabled
Healthcare Ecosystem Model" (AIEHEM), a DSS
based on an innovative AI model capable of
providing not only accurate predictions on the
outcome of certain operational or management
activities, but also to identify the main critical
factors correlated with the achievement of certain
organizational objectives.
The example shown in this article is related to
the optimization of the management of patients at
high risk of death. In this preliminary phase of
analysis we decided to use the exceeding the
regional expenditure threshold linked to patient
treatment as a proxy variable correlated with this
organizational outcome.
The used AI model is able not only to
autonomously identify the independent variables
most closely related to the chosen dependent
variable, but it is also able to tie them together
within a single logical formula. This knowledge
representation can be considered as a kind of
guideline used to evaluate the possibility of
incurring an overrun of care costs.
The advantage of defining a rule expressed
through a logical formalism is that it allows a group
of human experts to evaluate subsequently the
appropriateness of the reasoning followed by the AI
model. Just examining the set of independent
variables taken into consideration by the system in
making its predictions, it is possible to understand if
it has left out important factors of analysis and if its
reasoning was influenced by the cognitive biases of
the human experts who selected the data to be
analyzed. Furthermore, once the appropriateness of
the logical formula proposed by the AI model is
verified, it is possible to identify the stakeholders of
the healthcare ecosystem to be involved in order to
find a solution to the analysed organizational
problem. The next processing of the AI model on the
updated database can allow to understand whether or
not the healthcare ecosystem has managed to
intervene effectively on the critical factors identified
by the system and if other critical factors to be taken
into consideration have emerged over time. In this
way it is possible to establish a Deming cycle (plan-
do-check-act) to progressively improve the results
achieved by the healthcare ecosystem (Taylor et al.,
2014).
The AIEHEM project aims to assess the
multidimensional key factors which are related to
the strategic goals of a regional health system, by
using a specific artificial intelligence model.
Strategic goals can be: economic (e.g.: optimize the
consumption of system resources in chronicity, etc.),
organizational (e.g.: reduce waiting lists, increase
the quality of services provided, etc.), social (e.g.:
highlight the risk conditions for a pro-active risk
management, etc.) and environmental (e.g.: reduce
the environmental impact of health facilities, etc.).
The innovation of this project is based on the
specific methods, as well as on its global, systemic
approach. For the first time, in fact, an AI model will
support the identification of the actors, the facilities,
the activities, the knowledge, the opportunities, and
the most suitable ecosystem to achieve the the
regional health system goals, involving the relevant
end users.
The AIEHEM project is in line with the "One
Health" approach described by the 6
th
Mission of the
National Recovery and Resilience Italian Plan, as it
aims to promote interdisciplinarity and inter-
professionalism through the enhancement of
available health system data and information. The
purpose is to enhance the efficacy of planning and
decision-making of social and health services
through the use of an AI model built to simplify the
volume and complexity of social-health interactions.
The collection, refinement and processing of the
available data will be in compliance with the code
for the protection of personal data (GDPR) and with
the ethical values and fundamental principles of
health promotion and public health, through the
involvement of the data protection officer and the
regional ethics committee.
Artificial Intelligence Enabled Healthcare Ecosystem Model: AIEHEM Project
233

2 DSS DESCRIPTION
The recent pandemic crisis has highlighted the
problems that can arise from poor healthcare
management or unoptimized health system
resources. All these problems derive essentially from
the lack of effective cooperation strategies between
the various regional stakeholders resulting in an
insufficient integration of territory services,
hospitals and social services in facing health
challenges.
The AIEHEM project is aimed at supporting the
regional health management with an AI-based DSS
to identify the relevant areas of intervention,
stakeholders, and resources associated to an
effective achievement of their strategic objectives.
As an example, we present here the use of the
AIEHEM methodology to optimize the management
of system resources for patients at high risk of death
in Marche region (Italy). Particularly, we focus on
the need of enhancing sustainability by reducing the
costs of inappropriate use of resources in the last
quarter of life of the patients, which also lead to an
unjustified and dangerous delay of the diagnostic
services for patients with the right indications.
The strategic aim was to encourage palliative
care by avoiding clinical investigations that do not
help in improving the prognosis of patients. In order
to identify the factors related to an above-average in-
hospital consumption of resources in patients in the
last trimester of life, the AI model analysed the
2019 hospital discharge records (12344 records).
Data relating to the pandemic period were excluded
as the allocation of resources for the management of
the pandemic could influence the outcome of the
analysis.
The variables taken into account by the AI
model are the following: gender, age class, type of
hospitalization, method of discharge from the
previous structure, main diagnosis category,
residency, the exceeding the regional threshold for
assistance expenditure. The sex variable assumed
two values (male or female), the age was divided
into 5 strata (0-60, 61-70, 71-80, 81-90, 90+), the
type of hospitalization (reqType) was cathegorised
in 4 values (scheduled not urgent, urgent,
compulsory treatment, scheduled with
prehospitalization), the method of discharge
(disMode) encompassed 8 values (without the
proposal of the family doctor, with sending of the
family doctor, scheduled discharge, discharge from
public hospital, discharge from accredited private
structure, discharge from non-accredited private
structure, discharge from other hospitalization
regime, discharge from emergency urgency
department). In addition, 25 major diagnostic
cathegories (MDC) values were taken into account
and the regional threshold for assistance expenditure
was set by calculating the average diagnosis related
group (DRG) value, equal to 4579.71 euros
(Mistichelli, 1984).
To identify the analysis variables most correlated
with the problem that we intend to investigate, we
have chosen to use a single-state type A model of
Unorganized Turing Machine (UTM) (Turing,
1948), consisting of a combinatorial network of
NAND gates whose optimal configuration is
selected by the evolution of a population of
individuals each of which represents the encoding of
a UTM configuration. In this way the UTM is
generated "in an unsystematic and random way"
from a set of two-input NAND gates. Turing chose a
NAND gate because any other logical operation can
be performed by a set of NAND gates. An
Unorganized Turing Type A Machine can be
considered "a kind of Boolean neural network
without a layered structure, since recurrent
connections are allowed without constraints"
(Teuscher and Sanchez, 2000).
Every possible configuration of the NAND gates
that make up the UTM was coded with a binary
vector and to identify the optimal configuration, that
is the vector that would allow to maximize the
predictive accuracy of the model, a swarm-
evolutionary hybrid algorithm was used, which we
have called the Evolutionary Bait Balls Model
(EBBM), in which NAND gate configuration
vectors are considered as individual members of a
swarm. Each of them is able to perform only three
elementary operations (repulsion from others,
attraction to another particularly performing
individual, orientation towards others). The
evolution of this population leads to the appearance
of emerging behaviors (the state in which a sort of
bubble is formed in which most individuals tend to
orient themselves with respect to others),
manifesting a kind of collective intelligence (Lella et
al., 2022).
The original evolutionary model of the bait ball,
which inspired our EBBM, was developed by
researchers who found that within the group of fish
trying to escape predators a spontaneously generated
core constitutes what they called "selfish herd"
(Roberts, 2021; Yang, 2018). This denomination
comes from the selfish theory of the pack according
to which individuals within the population attempt to
reduce the risk of predation by placing other
conspecifics between them and predators. Returning
HEALTHINF 2023 - 16th International Conference on Health Informatics
234

to the bait ball model, it is precisely this "selfish"
behavior adopted by individuals that leads to the
formation of the optimal collective configuration.
The EBBM algorithm used as an optimization
algorithm can be described as follows:
Input: Array of individuals I to be
updated
Output: The position vectors (binary
vectors) of each individual in I will be
changed.
1: call function to alter the positions
of each individual
2: for all i ϵ I do
3: perform ZOR, ZOA, ZOO sets
calculations
4: if individual detected in ZOR then
5: perform repulsion (R)
6: else if individual detected in ZOO
then
7: perform orientation (O)
8: else if individual detected in ZOA
then
9: perform attraction (A)
10: end if
11: end for
Where ZOR is the Repulsion Zone: one
individual cannot occupy the position of another,
that is, it cannot be represented by the same binary
vector. In this case it assumes another random
position (every single bit of the individual is
modified with probability RepulsionRate). ZOA is
the Zone of Attraction: an individual tends to
approach individuals characterized by a greater
fitness (with a probability equals to the attraction
rate, every single bit of the individual can assume
the same value of the bit in the same position of the
best performing individual in the ZOA set). ZOO is
the Orientation Zone: an individual tends to orient
itself, among the individuals close to it, towards the
most performing one (with a probability equals to
the orientation rate, every single bit of the individual
can assume the same value of the bit in the same
position of the best performing individual in the
ZOO set). To define the sets ZOR, ZOA, ZOO, the
parameters ZORrange, ZOArange and ZOOrange
were introduced, representing the maximum number
of different bits between the vector of the individual
considered and that of the individual belonging
respectively to the ZOR, ZOA and ZOO zone
(attraction rate=0.05, orientation rate=0.3, repulsion
rate=0.5, ZOA range=70, ZOO range= 5, ZOR range
= 0). The fitness function of the individual is set as
the prediction accuracy of the corresponding UTM.
With this swarm-evolutionary hybrid algorithm,
better results are obtained in terms of predictive
accuracy than other classical evolutionary models
such as the genetic algorithm, as demonstrated in
(Lella et al., 2022) where the EBBM model was
used to implement an expert system capable of
diagnosing with a fair level of accuracy the risk of
incurring type II diabetes mellitus.
Every possible UTM configuration, which
corresponds to a given binary vector, has been coded
as follows. The first 59 bits represent the values that
can take all the classes of variables that can be
selected for the first input of the NAND gates of the
UTM model. The following 59 bits represent the
values that can take all selectable variable classes for
the second input of the NAND gates of the UTM
model. The remaining 54 bits were used to encode
the architecture of the 18 available NAND gates.
The values of these variables were encoded in binary
format using a single bit for the sex variables and the
exceeding of the regional spending threshold and a
"one-hot" encoding for all the others, that is, using n
bits for all the n possible values of the variable and
valuing to 1 only the bit whose position is associated
with the corresponding category. The variable of the
exceeding of the regional expenditure threshold is
considered as class variable, all the other ones are
considered non-class variables.
Each NAND gate has been encoded with three
bits. If the value of the first bit is 1 the first input of
the NAND gate considered is a first class of input
variable, otherwise the first input is connected to the
output of the next NAND gate. If the value of the
second bit is 1 the second input of the considered
NAND gate is a second class of input variable,
otherwise the first input is connected with the output
of another NAND gate. If the value of the third bit is
1 it means that the inputs of the NAND gates
considered are short-circuited and only the first input
should be considered. In this way each individual,
which represents a possible NAND network
configuration, is represented by 59+59+54=172 bits.
To represent a combinatorial NAND, when a
individual is tested for suitability, all the first classes
of input variables, all the second classes of input
variables, and all 18 available NAND gates are
selected sequentially once. The first NAND gate
(NAND#1) of the 54-bit sequence is the network
output gate. If the first bit of its code is 1, NAND#1
input 1 is the first input class variable that can be
selected. If the first bit of its code is 0, input 1 of
NAND#1 is the output of NAND#2, the code of
which is represented by the following three bits of
the 54-bit sequence. If the second bit of NAND#1 is
1, NAND#1 input 2 is the first input class variable
that can be selected. If the second bit of NAND#1 is
0, input 2 of NAND#1 is the output of NAND#3, the
Artificial Intelligence Enabled Healthcare Ecosystem Model: AIEHEM Project
235
code of which is represented by the third bit triplet
within the 54-bit sequence.
3 EBBM UTM PERFORMANCE
The performance of the UTM model trained by
EBBM (EBBM UTM) was compared with other AI
and machine learning models that allow to model an
explicit representation of the causal links identified
between the study variables considered. All the
models were trained using 60% of the available data
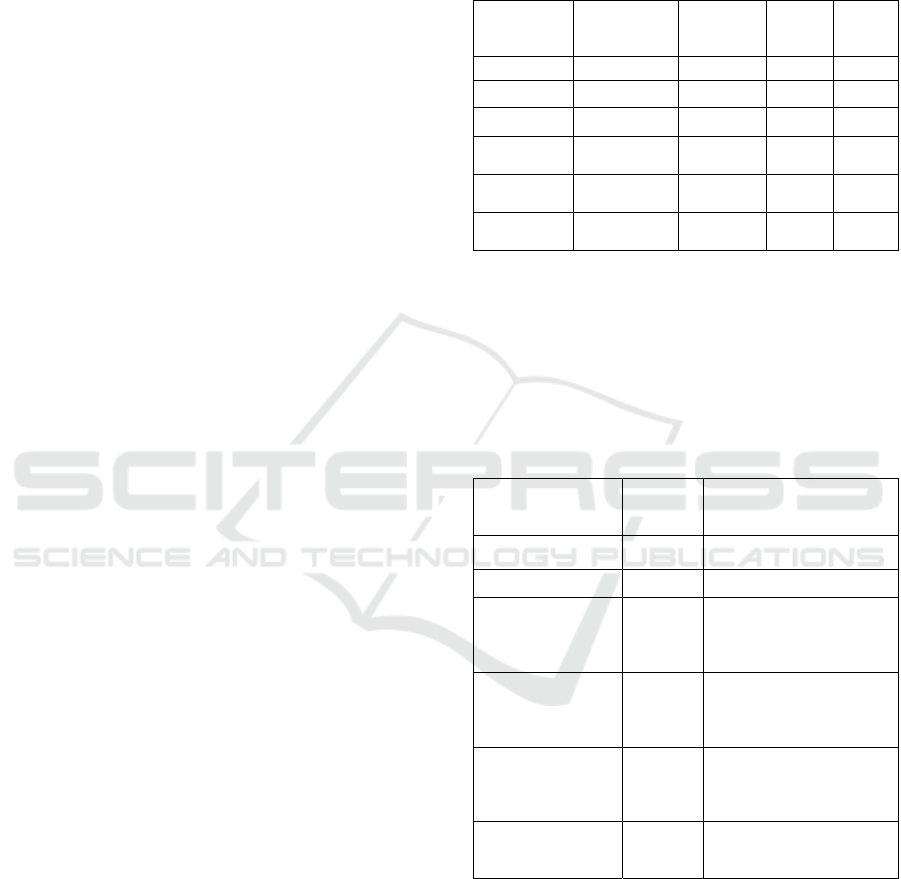
and tested with the remaining 40% of the data. Table
1 shows the predictive accuracies of the tested
models together with precision, recall and F1-score
measures. Table 2 reports the number of decision
nodes that make up the model and the number of
non-class variables taken into account by the models
to make their predictions.
The ZeroR model (Witten et al., 2011) was used
as a benchmark to verify that all other algorithms
used have been configured and used correctly.
ZeroR always predicted the most frequent class
variable in the presence of any combination of input
variables. Given its simplicity it typically had a
much lower level of predictive accuracy than the
other algorithms that have been tested. Alternatively,
the result found may be due to a bad selection and
encoding of the input data with which the models
were trained and tested or to a bad configuration of
the models used.
The OneR, which stands for "one Rule" (Holte,
1993), is nothing more than a one-level decision
tree. In various areas and predictive tasks this model
has proved to be much more performing than other
more complex models, and it is always appropriate
to verify whether the problem under consideration
can be effectively treated using this model that uses
a reduced amount of resources.
The J48 (Witten et al., 2011) is a decision tree
based on the "divide and conquer" strategy used
recursively. At each training step the node
characterized by the highest amount of information
is selected and split into a series of nodes
corresponding to some possible values that the
original node can assume. The process ends when all
instances considered reference the same value as the
class attribute.
The Bayesian network (Ben-Gal, 2007) is a
probabilistic graphic model that represents a set of
stochastic variables with their conditional
dependencies through the use of a direct acyclic
graph.
A random forest is an aggregate classifier
obtained by bagging aggregation of decision trees.
The name comes from the random decision forests
that were first proposed by Kam Ho (1995).
Table 1: Prediction accuracy of the AI tested models.
Model
Prediction
Accuracy
(%)
Precision Recall
F1-
Score
Zero R 72.11 0 0 0
One R 80.57 0.731 0.48 0.58
J 48 81.29 0.792 0.446 0.571
Bayes
Network
80.70 0.745 0.469 0.575
Random
Fores
t
75.92 0.578 0.508 0.541
EBBM
UTM
81.14 0.796 0.435 0.563
Compared to the other considered machine
learning and AI models, the UTM EBBM allowed to
create a predictive model characterized by a limited
number of nodes and which also takes into account
only a subset of the non-class variables presented in
making its predictions.
Table 2: Complexity level of the final knowledge
representations.
Model
Number
of nodes
Considered variables
Zero R 0 -
One R 1 MDC
J 48 31
MDC, type of
hospitalization, residency,
mode of discharge, age,
gende
r
Bayes Network 26
MDC, type of
hospitalization, residency,
mode of discharge, age,
gende
r
Random Forest 30
MDC, type of
hospitalization, residency,
mode of discharge, age,
gende
r
EBBM UTM 17
MDC, type of
hospitalization, mode of
discharge
This model allows human experts to evaluate the
criteria used by the model, explaining possible biases
in the selection of the data used for its training.
Because of its simplicity, the model obtained through
the UTM EBBM, could also be used, after a proper
validation by a team of human experts, to write
decision-making guidelines to be adopted by
managers or clinicians (figure 1).
HEALTHINF 2023 - 16th International Conference on Health Informatics
236

Figure 1: UTM forecast model selected through EBBM.
Only the UTM EBBM model was able to
establish that sex, age and residency were negligible
variables. Consequently, this finding allows to
exclude the referents of the territorial districts as
stakeholders to be involved. Also no sex-based or
age-based inequalities were observed, therefore the
involvement of associations of patients who deal
with them may not be necessary. The same AI
model built in this first analysis suggested to involve
psychiatric and hospital services in the management
of certain types of scheduled hospitalizations.
However, to be noted that the choice to use the
exceeding of the regional spending threshold as a
class variable may have introduced cognitive bias.
We will repeat the analysis of the UTM EBBM
model using different proxies to assess the
appropriateness of the assistance that has been
provided to patients close to death. Alternative
proxies could be given by the number of accesses to
the emergency room or the cost of drug therapies
that have been administered to patients close to
death. These new simulations will allow to validate
or not the predictive model that has been defined.
ACKNOWLEDGEMENTS
Special thanks to Dr. Remo Appignanesi, Dr. Maria
Rita Mazzoccanti, Dr. Antea Maria Pia Mangano,
Dr. Elena Di Tondo, Dr. Marco Morbidoni, Dr.
Pietro Serafini, Dr. Mariaflavia Spagna, Dr. Cristina
Omenetti and Dr. Cristiana Sisti for their kind and
valuable support.
4 CONCLUSIONS
The AIEHEM project has the ambitious goal of
suggesting to the organizational management the
most suitable strategy to undertake in achieving a
certain long-term outcome, using the support of an
AI model.
The chosen model (EBBM-based UTM) is able
not only to identify the critical factors related to the
achievement of a certain strategic objective, but through
the extrapolation of a rule that binds them it can help to
better understand the phenomenon that underlies the
achievement of the objective, suggesting which
stakeholders to involve in defining an adequate
intervention strategy.
The main beneficiary of the outcomes deriving from
the adoption of the AIEHEM methodology is the patient.
In the given example aimed at optimizing the system
resources in the care of patients at risk of death, the
medium-long term advantages are mainly the
improvement in the quality of palliative care and the
reduction of the waiting lists for specialty visits and
instrumental examinations. As a matter of fact, our
analysis revealed the use of unnecessary investigations,
perhaps deriving from defensive medicine practices.
Therefore, the insights obtained with the AIEHEM
methodology may support the staff operating in the
territorial and hospital structures to better coordinate their
activities and optimize the use of their resources. The
enhanced quality of services will therefore affect not only
the patients, but also their family members and caregivers
who would be given more precise instructions on how to
manage these patients.
It should be underlined that the AI model taken into
consideration, however, must serve to extend, complement
and support, not to replace, the analytical skills of human
experts who must in any case prepare the best lines of
intervention to achieve the specific management goals. In
a wide perspective, the EBBM UTM model may give its
best as a support tool in structured strategies of
management of change. The "Theory of Change", as used
by UNICEF and other UN organizations, has proved
particularly effective in finding solutions to contingent
problems that require political, administrative and
organizational interventions (ToC Center, 2021) and may
be an ideal framework to enhance AI-driven decision
support tools.
An estimate of the potential savings by optimizing the
system resources for patients in their fourth quarter of life
with the AIEHEM methodology is 16 million euros per
year.
REFERENCES
Academy of Medical Royal Colleges (2019), Artificial
Intelligence in Healthcare, retrieved on June 29th,
2022 from https://www.aomrc.org.uk/reports-
guidance/artificial-intelligence-in-healthcare/ .
Aghdaiea, M.H., Zolfanic, S.H., Zavadskas, E.K.,
Synergies of Data Mining and Multiple Attribute
Decision Making, Procedia – Social and Behavioral
Sciences, vol.73, pp. 388-395.
Angelis, A., Kanavos, P. (2017), Multiple Criteria
Decision Analysis (MCDA) for evaluating new
medicines in health technology assessment and
Artificial Intelligence Enabled Healthcare Ecosystem Model: AIEHEM Project
237

beyond: The advance value framework. Soc. Sci.
Med., vol. 188, pp. 137-156.
Baltussen, R., Stolk, E., Chisholm, D., Aikins, M. (2006),
Towards a multi-criteria apporach for priority setting: an
application to Ghana. Health Econ, vol 15, pp. 689-696.
Bashir, S., Qamar, U., Khan, F.H. (2014), Heterogeneous
classifiers fusion for dynamic breast cancer diagnosis
using weighted vote based ensemble. Quality &
Quantity, DOI: 10.1007/s11135-014-0090-z.
Ben-Gal, I. (2007). Bayesian Networks. In Ruggeri F,
Kennett RS, Faltin FW (eds.). Support-
Page. Encyclopedia of Statistics in Quality and
Reliability. John Wiley & Sons.
Berner, E.S. (2007), Clinical Decision Support Systems,
Theory and Practice. Second Edition Springer, 2007.
Diaby, V., Campbell, K., Goeree, R. (2013), Multi-criteria
decision analysis (MCDA) in health care. A
bibliometric analysis. Oper Res Health Care, vol.2,
PP.20-24.
Gasol, M., Bosch, J.A.; Pontes, C., Obach, N. (2022),
Early Access to Medicines: Use of Multicriteria
Decision Analysis (MCDA) as a Decision Tool in
Catalonia (Spain). J. Clin. Med., vol.11, p.1353.
Holte, R.C. (1993). Very simple classification rules
perform well on most commonly used datasets.
Machine Learning.
Ishizaka, P., Nemery, P. (2013), Multi-Criteria Decision
Analysis: Methods and Software. Wiley, 2013
Ju, Y., Wang, A., Liu, X. (2012). Evaluating emergency
response capacity by fuzzy AHP and 2-tuple fuzzy
linguistic approach. Expert. Syst. Appl., vol 39,
pp.6972-6981.
Kam Ho, T. (1995). Random Decision Forests, Proceedings
of the 3rd International Conference on Document
Analysis and Recognition, Montreal, QC, pp. 278–282
Khademolqorani, S., Hamadani, A.Z. (2015).
Development of a Decision Support System for
Handling Health Insurance Deduction. Int. J. of Adv.
Comp. Sci. And App., vol 6, no.2
Lella, L., Licata, I., Pristipino, C. (2022). Pima Indians
Diabetes Database Processing through EBBM-
Optimized UTM Model. In Nathalie Bier, Ana L. N.
Fred, Hugo Gamboa, editors, Proceedings of the 15th
International Joint Conference on Biomedical
Engineering Systems and Technologies, BIOSTEC
2022, vol 5: HEALTHINF, Online Streaming, February
9-11, 2022. pages 384-389, SCITEPRESS, 2022.
Longaray, A.A., Ensslin, L., Munhoz, P., Tondolo, V.,
Quadro, R., Dutra, A., Ensslin, S. (2016). A systematic
literature review regarding the use of multicriteria
methods towards development of decision support
systems in health management, Procedia Computer
Science, vol., 100, pp.701-710.
Marsh, K., Lanitis, T., Neasham, D., Orpanos, P., Caros, J.
(2014). Assessing the value of health care
interventions using multi-criteria decision analysis: A
review of the literature. PharmacoEconomics, vol. 32,
pp. 345-365.
Mistichelli, J.A. (1984), Diagnosis Related Groups
(DRGs) and the Prospective Payment System:
Forecasting Social Implications. Kennedy Institute of
Ethics, Center for Bioethics Library (January 1, 1984).
Narci, H.O., Ozcan, Y.A., Sahin, I. (2014), An
examination of competition and efficiency for hospital
industry in Turkey. Health Care Management Science,
DOI: 10.1007/s10729-014-9315-x.
Roberts T.J.: Dynamical and computational structures
under the sea: modelling of fish motion,
http://studentnet.cs.manchester.ac.uk/resources/library/
3rd-year-projects/2016/timothy.roberts-2.pdf , last
accessed 2021/09/30.
Roumani, Y.F., May J.H., Strum, D.P., Vargas, L.G.
(2013). Classifying higly imbalanced ICU data, Health
Care Management Science, vol.16, no.2, pp.119-128.
San Cristobal, J.R. (2013). Critical Path Definition Using
Multicriteria Decision Making: PROMETHEE
Method, J. Manag. Eng., vol 29.
Taylor, M.J., McNicholas, C., Nicolay, C. (2014).
Systematic review of the application of the plan–do–
study–act method to improve quality in healthcareBMJ
Quality & Safety 2014, vol.23, pp.290-298.
Teuscher C., Sanchez E. (2000). A Revival of Turing’s
Forgotten Connectionist Ideas: Exploring Unorganized
Machines. In Proceedings of the 6th Neural
Computation and Psychology Workshop, NCPW6,
University of Lige.
ToC Center, (2021). What is Theory of Change, retrieved
on June 29th, 2022 from https://www.theoryofchange.
org/what-is-theory-of-change/
Turing A. (1948). Intelligent Machinery. In Collected
Works of A.M. Turing: Mechanical Intelligence. Edited
by D.C. Ince. Elsevier Science Publishers, 1992.
Witten, I. H., Frank,E., Hall,M.A. (2011). Data Mining
Practical Machine Learning Tools and Techniques.
Morgan Kaufmann Publishers.
Wu, C.R., Lin, C.T., Chen, H.C. (2007). Optimal selection
of location for Taiwanese hospitals to ensure a
competitive advantage by using the analytics hierarchy
process and sensitivity analysis. Build. Environ.,
vol.42, pp.1431-1444.
Yang W. (2018). When the Selfish Herd is Unsafe in the
Middle. In: The 22nd Asia Pacific Symposium on
Intelligent and Evolutionary Systems
Zandi F. (2014). A bi-level interactive decision support
framework to identify data mining-oriented electronic
health record architectures, Applied Soft Computing,
vol.18, pp.136-145.
HEALTHINF 2023 - 16th International Conference on Health Informatics
238
