
Comprehensive Musculoskeletal Care Platform Enabling At-home
Patient Care
Ghazal Ershadi
1 a
, Serena Hughes
2 b
, Raja Sundaram
3 c
and Majid Sarrafzadeh
1 d
1
Computer Science Department, University of California Los Angeles, Los Angeles, U.S.A.
2
Bioinformatics Department, University of California Los Angeles, Los Angeles, U.S.A.
3
CEO, Plethy, Inc, San Jose, U.S.A.
Keywords:
Wearable Technology, Musculoskeletal Disorders, Rehabilitation Exercises, Remote Patient Monitoring.
Abstract:
Pain and stiffness in the musculoskeletal system cause limited range of motion and loss of mobility. Reme-
diation includes home care programs, physical therapy, medication, and if necessary, surgery. Much of the
recovery occurs at home. Active engagement by patients in their care program is crucial for successful clini-
cal recovery. Recovering from a partial or total joint replacement requires active participation in an exercise
program to help minimize swelling and improve motion and strength. On the other hand, non-surgical mus-
culoskeletal indications, also require a personalized exercise plan for recovery. Patients need support with
following their care at home. Remote care programs and monitoring offer convenient, safe, and time and
cost-efficient care, including at-home physical therapy programs, and have broad clinical scope. We studied
one such program. This paper reports the results of a platform that digitizes care programs for all muscu-
loskeletal conditions, engages patients at their convenience, while providing visibility to recovery progress via
patient-reported and sensor-generated data. We introduce Plethy Recupe which is a comprehensive platform
for musculoskeletal care with a joint motion sensor, intuitive app, and intelligent clinical dashboard. Six exer-
cises were selected from this platform and 10 individuals were asked to perform the exercises to evaluate the
accuracy of the range of motion (ROM) and complete a questionnaire on the usability of the solution.
1 INTRODUCTION
The rehabilitation process is crucial for recovery af-
ter major surgical procedures and for the manage-
ment of chronic conditions. Rehabilitation exercises
may also be performed prior to surgery. This is
known as pre-habilitation and is also thought to effec-
tively improve postoperative functional performance
and strength gain (Topp et al., 2009). Typically, the
rehabilitation process involves many in-person, one-
on-one sessions with a physical therapist. In between
these regular sessions, the patient will be expected
to repeat rehabilitation exercises at home, unsuper-
vised. In order to get further feedback on their per-
formance, the patient will have to book another ap-
pointment with his/her physical therapist. This takes
up the limited time of the physical therapist, requires
means to travel to and from their office, and can be
a
https://orcid.org/0000-0003-0174-4266
b
https://orcid.org/0000-0001-9207-1452
c
https://orcid.org/0000-0001-5825-0836
d
https://orcid.org/0000-0001-8407-8689
costly. This process is thus time and labor-intensive.
It is estimated that as of 2019, there were 2.4 billion
people globally with a condition that would benefit
from rehabilitation and that the need for rehabilitation
worldwide will increase over time (Cieza et al., 2020).
Remote monitoring of physical training sessions can
improve both the efficiency and effectiveness of this
care.
Remote monitoring is convenient, safe, and time
and cost-efficient. (Tack, 2021) In addition, it offers
improvements to the quality of care that patients re-
ceive. Patients can be monitored more frequently, can
receive objective, real-time feedback on their perfor-
mance, and will have a record of consistent, thorough
data from their exercise sessions. The solution we
choose to study was Plethy Recupe, a comprehensive
system for remote care focused on all musculoskeletal
conditions. The system consists of a wearable sensor,
an intuitive phone application, and a dashboard for the
healthcare provider.
The sensor is simple, small, and versatile. While
other remote patient monitoring systems achieve finer
190
Ershadi, G., Hughes, S., Sundaram, R. and Sarrafzadeh, M.
Comprehensive Musculoskeletal Care Platform Enabling At-home Patient Care.
DOI: 10.5220/0010868300003124
In Proceedings of the 17th International Joint Conference on Computer Vision, Imaging and Computer Graphics Theory and Applications (VISIGRAPP 2022) - Volume 2: HUCAPP, pages
190-196
ISBN: 978-989-758-555-5; ISSN: 2184-4321
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

granularity through a more complex, multi-sensor
system (Lorussi et al., 2018) (Ramkumar et al., 2019),
the singular Plethy Recupe sensor prioritizes ease of
use by patients at home. This simple setup reduces
inaccuracies due to user error and is neither intimidat-
ing nor discouraging to a broad spectrum of patients.
Other work in the field of remote rehabilitation has
also used the entire phone as the sensor itself (Cho-
miak et al., 2019). The Plethy Recupe sensor is only a
little larger than a quarter, making it easy to wear and
unobstructed while exercising. Other research spe-
cializing in remote monitoring of knees has also used
sensors that are embedded in a wearable knee sleeve
(Ramkumar et al., 2019). By using a sensor that can
be attached to different locations, the Plethy Recupe
solution can be used for various joints. In addition to
the knee, the sensor can be used for the ankle, hip,
lower back, shoulder, elbow, and wrist, etc. This also
allows for future expansion of the Plethy Recupe sys-
tem to other regions, surgeries, and conditions.
The phone application is compatible with both
iOS and Android, making Plethy Recupe accessible
to nearly any patient with a smart device. The app is
designed to be straightforward and helpful for patient
motivation and recovery. It includes video demon-
strations of how to perform exercises, training videos
on sensor placement, and live visualization of the pa-
tient’s range of motion. In addition, it counts success-
ful repetitions of an exercise in real-time and gener-
ates range of motion measurements. Upon start-up, it
surveys patient symptoms, level of pain, reminds pa-
tients when to exercise, when to take medications, and
of upcoming surgery-related events. All of this data
is available to the clinician as well.
The remainder of the paper is structured as fol-
lows. Section 2 provides the requisite background
on importance of musculoskeletal conditions. Sec-
tion 3 discusses the system specification of the Plethy
Recupe, including hardware implementation, exercise
recognition algorithm, mobile application, and clin-
ical dashboard. Section 4 introduces the six exer-
cises that are evaluated in the experiments. Section 5
presents the result of the experiments and preliminary
evaluation of the Plethy Recupe. Finally, we conclude
and propose our future research direction in Section 6.
2 CLINICAL BACKGROUND
The World Health Organization names musculoskele-
tal conditions as the leading contributor to disabil-
ity worldwide. There are over 150 diagnoses which
qualify as musculoskeletal, affecting the joints, bones,
muscles, spine, and connective tissue. (World Health
Organization, 2021) These conditions are highly
prevalent and cost our society a large sum in both
treatment costs, lower quality of life, and loss of in-
come due to inability to work. In the United States
in 2018, one out of two adults were diagnosed with a
musculoskeletal condition, totaling $124 million peo-
ple (Bone and Joint Initiative, 2018). Through di-
rect and indirect costs, musculoskeletal disorders cost
the United States $150 billion and are expected to
increase by $73 between 2014 - 2024 (Optum, Inc.,
2019). As such, musculoskeletal pre-rehabilitation,
treatment, and rehabilitation are of high importance
to the well-being of society and economy.
In this study, the focus is on musculoskeletal exer-
cises intended to strengthen the knee and ankle joints,
as arthritis in the knee is the most common muscu-
loskeletal indication. Each exercise in the app in-
cludes a brief description of how to perform it along
with a video demonstration. The six exercises tested
are Long Arc Knee Extension, Heel Slides with Quad
Sets, Toe Raises, Reverse Toe Raises, Ankle Pump,
and Seated Ankle Pump. The first two exercises tar-
get muscles that support the knee and the remaining
four strengthen the ankle. For example, the Long Arc
Knee Extension exercise strengthens the quadriceps
muscles which support the range of mobility of the
knee.
It is estimated that in 2010, 1.52% of the United
States population underwent total knee replacement
surgery. This is approximately 4.7 million individ-
uals (3.0 million women and 1.7 million men) who
had this procedure done. These numbers only account
for those who had total knee replacement surgery.
In addition, there are millions of people with partial
surgeries or musculoskeletal conditions that arose for
other reasons such as overuse or traumatic impact.
Musculoskeletal problems in the foot and ankle are
experienced by approximately 1 out of every 5 peo-
ple. Further, it has been found that the number of total
ankle replacement surgeries performed in the United
States increased by 261% from 2005 to 2014. In this
same time period, ankle fracture surgeries increased
by 82% (Burton et al., 2020). As such, the develop-
ment of a rehabilitation program with exercises for
knee and ankle recovery like the ones tested here is
crucial and increasingly critical.
3 MATERIAL AND METHODS
The Plethy Recupe Solution is composed of three
main components: a wearable sensor, a smartphone
application, and a clinical dashboard as in figure 1.
The sensor unit is designed to measure the range of
Comprehensive Musculoskeletal Care Platform Enabling At-home Patient Care
191

Figure 1: Components of the platform: a sensor unit, linked
smartphone application, and clinic dashboard.
joint angle movement using an IMU. It is mounted on
a casing that’s easy to wear and attached to any part
of the body using a reusable adhesive. The sensor unit
is programmed with different algorithms to count the
number of successful repetitions along with the range
of movement angle for each exercise. The readings
of the sensor unit are transmitted to an application
via Bluetooth. The application stores the recordings
in the cloud-based database along with the number
of successful repetitions. It also displays the num-
ber of care sessions including the home exercise pro-
gram. The dashboard enables the healthcare provider
to monitor the patient’s functionality and progress
throughout the entire care journey ( pre-surgery to
post-surgery) or the non-surgical treatment process.
3.1 Hardware
An Inertial Measurement Unit (IMU) has been uti-
lized to measure the joint angle and count the num-
ber of repetitions per exercise. It is a 9-axis motion
tracking device that incorporates a triple-axis gyro-
scope, a triple-axis accelerometer, and a triple-axis
magnetometer all integrated into a Quad Flat No-
leads (QFN) package. The IMU precisely offers full
9-axis Motion Fusion performance with its dedicated
I
2
C sensor bus. It involves a total of nine 16-bit
analog-to-digital converters (ADCs) for 3-axis gyro-
scope, 3-axis accelerometer, and 3-axis magnetome-
ter output digitization. In this work, three vibratory
MEMS rate gyroscopes are used, which detect rota-
tion around the 3-axis, and acceleration around a par-
ticular axis that causes displacement on the associ-
ated proof mass with a measurement range of up to ±
16g. The Coriolis effect (McDonald, 1952) induces
a vibration detected by a capacitive pickoff while the
gyroscope is rotated along either of the axes. Then,
a voltage that is proportional to the angular velocity
is generated. This voltage is digitized using 16-bit
ADCs with a range of up to ± 2000 degrees per sec-
ond (dps).(Invensense TDK, 2021)
The IMU data is transmitted to the phone applica-
tion via Bluetooth 5 connection. The Bluetooth mod-
ule communicates with the IMU via I
2
C bus at 400
kHz frequency. Low energy consumption, small area
requirements (a 6.5mm × 6.5mm package), and sim-
plified development costs of this module make it per-
fectly fitted for wearable devices.(Silicon Labs, 2017)
The system chip is equipped with a square TACT
switch with no stem on it (ALPS, 2021) and a
through-hole mount battery holder that provides solid
electrical contact for a lithium coin battery. They are
all housed in an 18mmDia × 9mmH Recupe package.
The housing consists of a bottom and a cap which are
detachable in case the battery has to be replaced and
they can be coupled afterward. With a little press on
the housing, the sensor starts connecting to the paired
smartphone with a blinking blue light. The sensor is
automatically turned off after 15 seconds if it cannot
find the paired phone and have a successful connec-
tion via Bluetooth. This can occur if the Recupe ap-
plication is closed on the smartphone, or if the smart-
phone is out of the sensor range. The sensor blinking
green light confirms that it is successfully connected
to the smartphone.
3.2 Algorithm
In order to count the repetitions per exercise, the al-
gorithm properly fuses Gyroscope and Accelerometer
inputs. The confidence on each sensor can be con-
figured independently. With the help of sensor fu-
sion, the strengths of the gyroscope and accelerome-
ter are obtained and the effects of weaknesses in each
are mitigated. The algorithm accounts for calibra-
tion of gyroscope signal and accelerometer, and post-
processing of algorithm output. In this algorithm, an-
gular velocity is also considered as a metric.
The gyroscope model is as in equation 1, where ω
is the true angular velocity, b is bias, and σ is addi-
tive zero-mean Gaussian noise. The static bias can be
calibrated out. The white noise is mainly due to the
nature of the sensor.
˜
ω = ω + b + η, η ∼ N(0,σ
2
gyro
)) (1)
The equation 2 is used to calculate the orienta-
tion resulting from the gyroscope measurements. This
equation is the result of applying Taylor expansion to
gyroscope measurements.
θ(t + ∆t) ≈ θ(t) +
∂
∂t
θ(t)∆t + ε, ε ∼ O(∆t
2
) (2)
Given θ(t) which is the angle at last time step,
∂
∂t
θ(t) = ω which is the gyro measurement(angular
HUCAPP 2022 - 6th International Conference on Human Computer Interaction Theory and Applications
192

velocity), ∆t which is time step, and ε which is ap-
proximation error, we seek θ(t + ∆t) which is the an-
gle at current time step. When the sensor is used for
long periods, the approximation error leads to drift.
Since the duration it takes to do an exercise is short, it
can be neglected.
Linear acceleration is measured by equation 3.
With the accelerometer in a stationary position, the
linear acceleration results in the noisy gravity vector,
a
(g)
+ η. The direction of this vector is pointing up
with magnitude 9.81 m/s
2
= 1g. However, any accel-
eration yields the linear acceleration to a combined
vector of external forces,a
(l)
, and noisy gravity.
˜a = a
(g)
+ a
(l)
+ η, η ∼ N(0,σ
2
acc
)) (3)
Equation 4 relates the roll and pitch angles to the
normalized accelerometer readings. Depending on
the rotation sequences this matrix might hold differ-
ent row ordering.
ˆa =
˜a
k
a
k
=
−cos(−θ
x
)sin(−θ
z
)
cos(−θ
x
)cos(−θ
z
)
sin(−θ
x
)
(4)
By solving equation 4, the roll and pitch angles are
computed. A challenge to be addressed is that at mul-
tiples of 2π, the equations for the roll and pitch angles
have an infinite number of solutions. It is somewhat
beneficial to limit the range of the roll and pitch an-
gles to fall in the range of −π to π, but it still leads to
two distinct roll and pitch angle solutions. The solu-
tion is to limit either the angle of the roll or the angle
of the pitch to lie in between −
π
2
to
π
2
. In this work,
the role angle is restricted to −π to π, and the pitch
angle is ranged between −
π
2
to
π
2
.
The aim of this work is to be able to accurately
estimate 3D orientation using accelerometer and gy-
roscope data. To better estimate orientation, roll and
pitch angles that are estimated from accelerometer
data are fused with the gyroscope angle.
After calibrating gyroscope data by removing the
static bias from it, incorporating the output of the gy-
roscope to turn the angular velocity into an angular lo-
cation, applying a low pass filter to the accelerometer
data to eliminate the noise in the output, and finding
the accelerometer roll and pitch angles; the sensors’
data can be fused by equation 5. Alpha is a constant
weight that needs to be adjusted and Theta is a single
state orientation.
θ
(t)
= α(θ
(t−1)
+
˜
ω∆t) + (1 − α) − ( ˆa
z
,
q
a
2
x
+ a
2
y
)
(5)
Velocity information is taken into consideration as
well. Velocity is calculated as the integration of ac-
celerometer results fused with the raw gyroscope data.
Calculating the angular velocity gives us additional
metrics to characterize exercises.
Once the algorithm generates the orientation sig-
nal, a moving average filter is implemented to smooth
the output. The moving average filters the output de-
pending on the frequency of the data stream. Among
the Theta and velocity signals, we choose the one
that is appropriate depending on the exercise. Then
the chosen signal might need to be shrunk or ex-
panded to output the correct angle reading which can
be achieved by multiplying to a constant parameter,
Gamma. Finally, after selecting the proper filtered
signal and scaling it, the number of peaks in the signal
are counted by setting correspondent threshold angles
per exercise.
Twenty individuals were asked to do 2 sets of 10
repetitions for each exercise and a brute force search
was run to find the best Alpha (fusion weight param-
eter), Gamma (scaling signal parameter), and best-
fitted threshold angles for the counter.
3.3 Application
The application is both Android and IOS compatible.
The Bluetooth connection status can be checked at the
bottom of the Application screen. Before turning the
sensor on, it shows ”Searching for Sensor”. By click-
ing the sensor on, the connection status updates to
”Sensor Connecting”. As soon as the sensor connects
to the app via Bluetooth, the care sessions associated
with the patient are displayed on the screen. The ap-
pearance of a blinking green light on the sensor, sig-
Figure 2: Application screen for a sample home screen.
Comprehensive Musculoskeletal Care Platform Enabling At-home Patient Care
193

nals that the connection is established, the connection
status at the bottom of the screen changes from ”Sen-
sor Connecting” to ”Sensor Ready” as well. Rele-
vant pre-surgery and post-surgery exercise program
is selected by the patient’s orthopedic surgeon and is
included in the care session of the patient. Before
starting the program exercises, the patients are asked
about their pain level. The care sessions are easy to
follow and each of the home exercises that appears
on the care session screen includes text and video in-
struction on how to correctly do the exercise. Fig-
ure 2 shows the screen of the application including
a sample exercise, Long Arc Knee Exercise. When
the sensor is stable, the start button in the bottom left
corner activates. By selecting the start button, it turns
into a pause option to allow patients to pause the ex-
ercise if they need to. The number of sets and repeti-
tions per set is determined by the patient’s doctor. In
Figure 2, there are 2 sets of 10 repetitions for Long
Arc Knee Exercise. The gauge at the right bottom
of the exercise screen tracks the angle measurements
in real-time. Whenever a repetition is successfully
completed, the table at the left bottom of the exercise
screen updates the repetitions.
The application records the medications that the
patients take and once the patients complete their ex-
ercise program, the application reminds them to take
their medications.
Moreover, patients’ symptoms are checked daily
through a survey by asking them about how they feel
compared to the last care session, how their exercises
go through the session, what their current pain level
is, and what they feel about their Recupe program.
The application assesses patients to follow their icing
and elevation instructions throughout the day and to
track their icing time by an ice countdown.
3.4 Dashboard
Plethy Recupe enables the patients’ care team to track
their progress and contact them as needed. Clinicians
can track patients’ progress while they manage their
care plan at home. The Plethy Recupe clinical dash-
board gives clinician and Recupe team authorized ac-
cess to the library of exercises and patients’ accounts.
They can monitor patient’s pain level, medication,
symptoms, physical therapy adherence, range of mo-
tion percentage, pre-operation checklist, and their el-
evation and icing. Figure 3 illustrates the look of
a patient’s account. Access authorizers may modify
the pre-operation and post-operation exercises per pa-
tient and the number of daily repetitions for each ex-
ercise. Moreover, they can write notes and activity
reports to their patients, set an appointment for them,
Figure 3: Sample screen from a patient account in dash-
board.
check the surveys that patients have filled out, sched-
ule their daily medications, and manage the instruc-
tions and checklists of pre-operation, post-operation,
and non-surgical programs. The Plethy Recupe care
team monitors the battery level of devices and no-
tify patients to exchange the battery of their device if
they need to. Registering the demographic character-
istics of a new patient, an account will be added to the
patients’ list. Then, clinicians can create a template
from the existing exercises in the library and assign
it to the account. There exist hundreds of exercises
in the library and it’s possible to add a new exercise
to the library along with the exercise description and
instruction video. The parameters and threshold an-
gles associated with the algorithm for the exercise are
set in the exercise dashboard profile. Furthermore, in
the exercise dashboard profile, its number of repeti-
tions, the duration, and hold time per repetition are all
defined.
4 CLINICAL APPLICATION
The system has been tested on 10 healthy subjects, 1
female and 9 males with an average age of 53. They
were asked to do 6 exercises and fill out the user sat-
isfaction survey that has been approved by our expert
clinicians. The participants are expected to complete
2 sets of 10 successful repetitions for each exercise.
They have been instructed on how to use the platform
and where to place the sensor regarding each exercise.
The exercises are as follows:
• Long Arc Knee Extension, participants are asked
to sit with their back against a chair and thighs
fully supported. They are instructed to lift the op-
erated foot up, straighten the knee, and hold for a
five-second count. They must not raise thigh off
of the chair.
• Heel Slides with Quad Sets, participants are
asked to lie down on their back with their not af-
fected leg bent at the knee. They are instructed to
tighten the thigh and buttocks of the affected leg
HUCAPP 2022 - 6th International Conference on Human Computer Interaction Theory and Applications
194
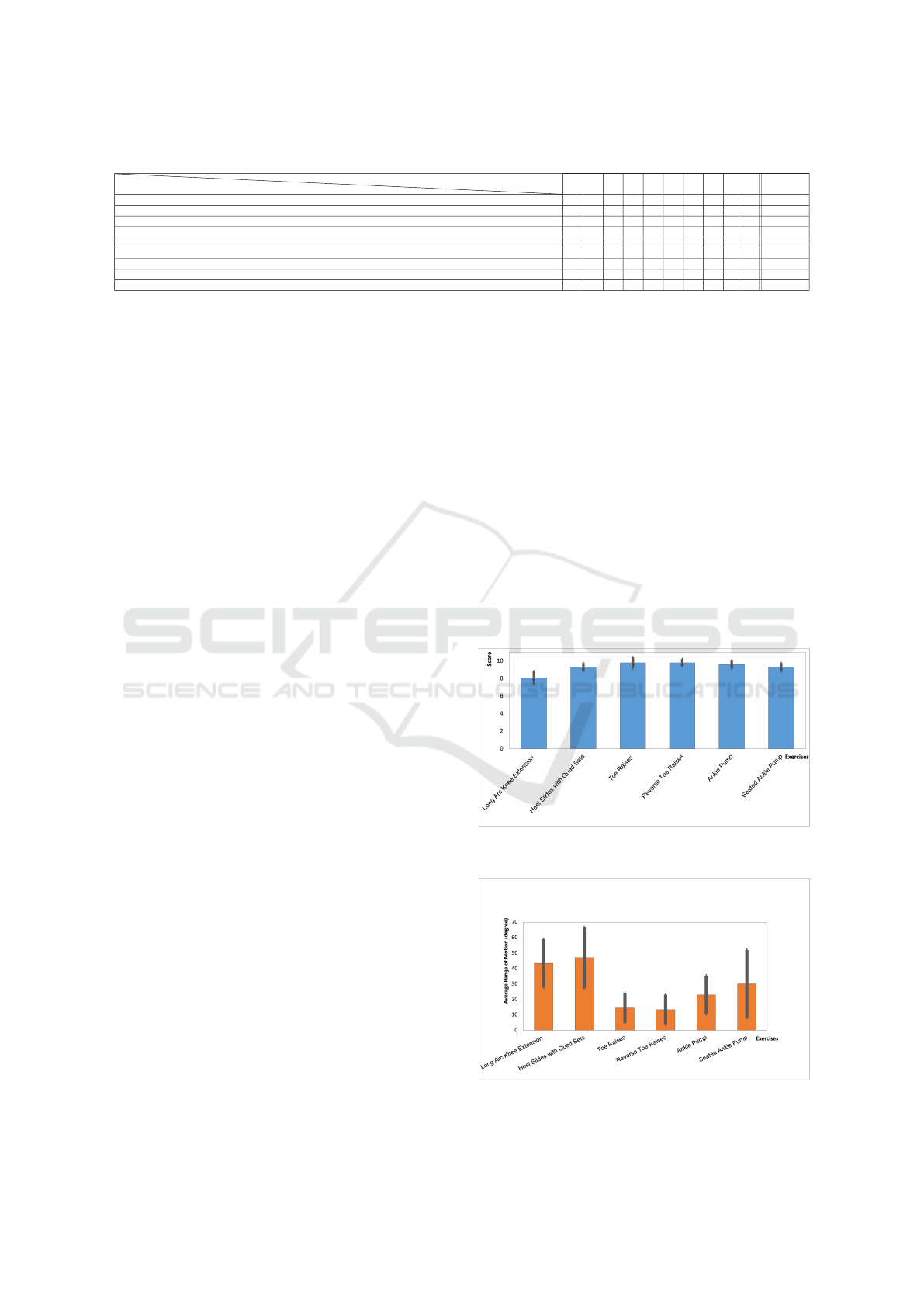
Table 1: Users’ scoring the 10-point Likert scale usability questions (strongly disagree (1) to strongly agree (10)).
Questions
Subject ID
1 2 3 4 5 6 7 8 9 10 Average
Did you enjoy your experience with the system? 9 9 9 8 9 9 9 8 7 9 8.6 ± 0.7
Were you successful using the system? 10 9 9 9 10 10 9 9 7 9 9.1 ± 0.88
Is the information provided by the system clear? 9 9 8 9 9 9 9 8 8 10 8.8 ± 0.63
Do you find the system easy to use? 9 8 9 8 9 9 8 9 7 9 8.5 ± 0.71
How easily did you learn to use the system? 9 9 8 8 10 9 8 8 8 9 8.6 ± 0.7
How accurate did you find the angle measurement? 9 8 8 9 10 9 9 9 8 8 8.7 ± 0.67
How accurate did you find the rep counts? 10 9 9 9 10 10 9 9 8 10 9.3 ± 0.67
Do you think that this system will be helpful for your rehabilitation? 10 9 9 9 10 10 9 9 9 9 9.3 ± 0.48
If prescribed by a healthcare practitioner, would you use the Recupe and perform the exercise program daily? 10 10 10 10 10 10 10 10 9 10 9.9 ± 0.32
and hold it for 5 seconds, then, bend their knee
and pull the heel towards the buttocks for 3 sec-
onds.
• Toe Raises , participants are asked to stand facing
the kitchen sink with a firm hold on the kitchen
sink. They are instructed to rise up on toes then
back on heels and stand as straight as possible.
• Reverse Toe Raises, participants are asked to
stand holding onto a chair or supportive object.
They are instructed to raise their toes and feet off
the floor, then, slowly lower toes back to the floor.
• Ankle Pump, participants are asked to place a pil-
low under the ankle, and lie flat on the floor. They
are instructed to bend ankles to move feet up and
down. They must not make use of a chair to do
this exercise.
• Seated Ankle Pump, participants are asked to be-
gin sitting upright with one leg straight forward.
They are instructed to slowly pump their ankle
by bending their foot up toward their body, then
pointing their toes away from their body. They
must make sure to move their foot in a straight
line and try to keep the rest of their leg relaxed.
5 RESULTS AND DISCUSSION
The questionnaire that the subjects were asked to fill
out after their experiment, is designed by our expert
clinicians and engineers to evaluate the system usabil-
ity and accuracy of exercises. The system usability
questions along with the participants’ 10-point Lik-
ert scale scores, where 1 strongly disagrees and 10
strongly agrees, are included in the Table 1. The aver-
age 10-point score given to each usability question is
determined in the last column of this table. Each par-
ticipant rated the exercises based on their experience,
the average scores given by the participants to each
of the exercises are visualized in Figure 4. The grey
error bar located in the center of the exercise bar rep-
resents the standard deviation of exercise scores. The
Users’ average range of motion for each exercise that
has been measured by the algorithm, is extracted from
the database, and Figure 5 indicates the participants’
average range of motion measured for each exercise.
The grey error bar in the middle of each exercise bar
identifies the standard deviation of participants’ range
of motion. Based on the records, the average user sat-
isfaction of the platform is 93%±6.4, and the average
participants’ score to the accuracy of the 6 exercises
is 90% ± 4.6.
6 CONCLUSION AND FUTURE
WORK
In this paper, Plethy Recupe has been introduced to
assist the patients through their musculoskeletal reha-
bilitation beyond the clinical environment. The sys-
tem consists of a wearable sensor, a smartphone appli-
cation, and a clinical dashboard that enables therapists
to remotely set up specific rehabilitation programs de-
Figure 4: Average 10-point score given by participants to
each of the 6 exercises.
Figure 5: Average range of motion performed by partici-
pants for each of the 6 exercises.
Comprehensive Musculoskeletal Care Platform Enabling At-home Patient Care
195

pending on patient disorder and characteristics and to
monitor patient progress over time. With the aid of ac-
celerometer and gyroscope signals read by the single
IMU in the sensor unit, we count the successful ex-
ercise repetitions and guide the user to correctly per-
form the exercises. We picked 6 pre-tested exercises
from the library. These six exercises are under pilot
study in the hospitals we collaborate with as well. The
result of the study on 10 healthy subjects with the su-
pervision of a team of expert clinicians proves 90%
of the user satisfaction score for the exercises. The
major limitation of this study is that the system eval-
uation and the evaluation results are conducted only
on healthy subjects, however, our future prospective
is to extensively evaluate the Plethy platform by mus-
culoskeletal disorders patients.
REFERENCES
ALPS (Accessed 2021). Tact switch 5.2mm square low-
profile (surface mount type). https://www.mouser.
com/datasheet/2/15/SKQG-1155865.pdf.
Burton, A., Aynardi, M. C., and Aydogan, U. (2020). De-
mographic Distribution of Foot and Ankle Surgeries
Among Orthopaedic Surgeons and Podiatrists: A 10-
Year Database Retrospective Study. Foot and Ankle
Specialist.
Chomiak, T., Sidhu, A. S., Watts, A., Su, L., Graham, B.,
Wu, J., Classen, S., Falter, B., and Hu, B. (2019). De-
velopment and validation of ambulosono: Awearable
sensor for bio-feedback rehabilitation training. Sen-
sors (Switzerland), 19(3):6–13.
Cieza, A., Causey, K., Kamenov, K., Hanson, S. W., Chat-
terji, S., and Vos, T. (2020). Global estimates of the
need for rehabilitation based on the Global Burden
of Disease study 2019: a systematic analysis for the
Global Burden of Disease Study 2019. The Lancet,
396(10267):2006–2017.
Invensense TDK (Accessed 2021). Mpu-9250: Tdk.
https://invensense.tdk.com/products/motion-
tracking/9-axis/mpu-9250. (Accessed on
01/02/2021).
Lorussi, F., Lucchese, I., Tognetti, A., and Carbonaro, N.
(2018). A wearable system for remote monitoring of
the treatments of musculoskeletal disorder. Proceed-
ings - 2018 IEEE International Conference on Smart
Computing, SMARTCOMP 2018, pages 362–367.
McDonald, J. E. (1952). The coriolis effect. Scientific
American, 186(5):72–79.
Ramkumar, P. N., Haeberle, H. S., Ramanathan, D.,
Cantrell, W. A., Navarro, S. M., Mont, M. A., Bloom-
field, M., and Patterson, B. M. (2019). Remote Pa-
tient Monitoring Using Mobile Health for Total Knee
Arthroplasty: Validation of a Wearable and Machine
Learning–Based Surveillance Platform. Journal of
Arthroplasty, 34(10):2253–2259.
Bone and Joint Initiative (2018). The Hidden Impact of
Musculoskeletal Disorders on Americans. 4th edition.
Optum, Inc. (2019). Complex, costly conditions: A strate-
gic imperative for payers and employers. White Paper.
Silicon Labs (2017). BGM121/BGM123 Blue
Gecko Bluetooth SiP Module Data Sheet.
https://www.silabs.com/documents/login/data-
sheets/bgm12x-datasheet.pdf.
Tack, C. (2021). A model of integrated remote monitoring
and behaviour change for osteoarthritis. BMC Muscu-
loskeletal Disorders, 22(669).
Topp, R., Swank, A. M., Quesada, P. M., Nyland, J., and
Malkani, A. (2009). The Effect of Prehabilitation Ex-
ercise on Strength and Functioning After Total Knee
Arthroplasty. PM and R, 1(8):729–735.
World Health Organization (2021). Musculoskeletal con-
ditions. https://www.who.int/news-room/fact-sheets/
detail/musculoskeletal-conditions. (Accessed on
03/02/2021).
HUCAPP 2022 - 6th International Conference on Human Computer Interaction Theory and Applications
196
