
A Digital, Game-based Application to Support Treatment of
Parkinson’s Disease: A Design Thinking Approach
Anne Mainz
1a
and Sven Meister
1,2 b
1
Health Informatics, Faculty of Health, Witten/Herdecke University, Witten, Germany
2
Fraunhofer Institute for Software and Systems Engineering, Dortmund, Germany
Keywords: Design Thinking, Parkinson’s Disease, Rehabilitation, Physical Therapy, Motivation, Serious Game,
Exergame.
Abstract: One of the most common neurodegenerative disorders that affects more and more people at an advanced age
is Parkinson’s disease. Patients suffer from various symptoms and especially the motor restrictions and
psychological symptoms worsen the quality of life of the affected persons. The physical therapy for this
disease to improve motor performance and complementary exercises is characterised by repetitive training
and patients often suffer from a strong exhaustion and lack of motivation due to their disease. To address
these problems, a serious game concept for Parkinson's therapy was developed. The concept was created using
the Design Thinking methodology for a user-centred design. The final result is the concept and prototype of
a competitive multiplayer exergame that was developed to increase the motivation of the patients to participate
through social play and the idea of competition in order to support the motor therapy of Parkinson’s disease
patients.
1 INTRODUCTION
Parkinson’s disease is a neurodegenerative disorder
that affects 2-3% of the population over 65 years
(Poewe et al., 2017). The most associated symptoms
are the four cardinal signs concerning the motor
system: rest tremor, muscle rigidity, postural
instability and bradykinesia (Balestrino & Schapira,
2020). Rest tremor is manifested by alternating
involuntary movements of the hands, feet and
sometimes other body parts when the patient is at rest
(Helmich et al., 2012). Muscle rigidity refers to the
continuous and constant increase in muscle tone with
resistance to passive movements regardless of
movement speed and direction of movement
(Delwaide, 2001). Disturbed postural reflexes and
reduced control over one’s own movement often
cause balance difficulties in Parkinson’s patients,
leading to postural instability (Bloem, 1992).
Bradykinesia, the slowness of movement, often
occurs in connection with hypokinesia, the deceasing
of movement. The movements of the patients are
often under-scaled due to wrong motion perception
a
https://orcid.org/0000-0002-9790-6049
b
https://orcid.org/0000-0003-0522-986X
(Balestrino & Shapira, 2020). Through external
cueing and big flowing exercises as compensatory
movement strategies, this symptom can be alleviated
(Janssen et al., 2014).
Non-motor symptoms in Parkinson’s disease
range from autonomic dysfunctions to sensory
disorders and various psychiatric disorders. Self-
reports of patients show that especially nonmotor
symptoms like depression and fatigue affect their
perceived quality of life (Barone et al., 2009). Fatigue
is characterized by an intense feeling of tiredness,
exhaustion and listlessness and concerns more than
half of the patients with Parkinson’s (Krupp &
Pollina, 1996). Fatigue is additionally associated with
lack of motivation, pain, lower quality of life, poorer
perception of psychological well-being, more severe
depressive symptoms, and an increased prevalence of
sleep disturbances (Hagell & Brundin, 2009; Stocchi
et al., 2014). Friedman and colleagues advise physical
exercises and group motivational training to
counteract fatigue (Friedman et al., 2007).
A serious game is an interactive computer-based
game software that has been developed with the
Mainz, A. and Meister, S.
A Digital, Game-based Application to Support Treatment of Parkinson’s Disease: A Design Thinking Approach.
DOI: 10.5220/0010846100003123
In Proceedings of the 15th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2022) - Volume 5: HEALTHINF, pages 125-134
ISBN: 978-989-758-552-4; ISSN: 2184-4305
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
125

intention to be more than entertainment. It is used to
impart skills or knowledge embedded in a
motivational and entertaining context (Ritterfeld et
al., 2009). Serious games are used in various fields
from healthcare, marketing, social change, education,
military, occupation, well-being, advertising, cultural
heritage, interpersonal communication and academic
purpose (Laamarti et al., 2014; Ritterfeld et al., 2009).
A huge number of serious games in healthcare can be
classified as so-called exergames, often used for
motor rehabilitation. Exergames combine a playful
approach (game) with physical activity (exercise)
(Malaka et al., 2016). Instead of classic input devices
such as keyboard and mouse or controller,
physiological feedback from the player is used to
interact with game (Malaka et al., 2014).
Due to the repetitive nature of Parkinson's therapy
patients get physically tired and mentally bored
during classic therapy training resulting in lack of
motivation (Assad et al., 2011). Serious exergames
offer themselves as a therapy supplement for
Parkinson's therapy due to their playful motivation to
move in combination with therapeutic effects (Rego
et al., 2014). Aim of this paper is an appropriate
exergame-concept developed for Parkinson’s disease
patients with mild to moderate Parkinson’s disease to
improve hypokinesia and fatigue.
2 METHODS
To develop a suitable serious game concept for
Parkinson’s therapy the design thinking methodology
is used which was developed to systematise creative
processes and to find user-centred solutions to
problems (Brown, 2008). Depending on the selected
model, the design thinking process is divided into five
or six phases that are iterated through. Within this
work we have chosen the model presented in the work
of Wölbling and colleagues (Wölbling et al., 2012),
consisting of understand, observe, point of view,
ideate, prototype and test.
2.1 Literature Review
In the understand-phase the initial definition of the
problem and a broad outline of the subject matter are
required. The topic, main stakeholders and the
context are identified. First results can be obtained
through literature research, as in this case. Often there
are unanswered questions that can be answered in the
next step (Wölbling et al., 2012).
To gain more insight, related work was
investigated. Applications were considered that can
be classified as serious games and that define patients
with Parkinson's disease as the target group. The
applications were identified through literature
searches on the online databases ACM Digital
Library, APA PsycNet, PubMed, ScienceDirect,
IEEE Xplore Digital Library, ResearchGate,
Semantic Scholar and Springer Link. Applications
were excluded that used gamification aspects but
were not implemented as a serious game, serious
games that did not aim at motor improvement, or
applications that were not explicitly conceptualised
and implemented for Parkinson's patients. The
following keywords were used in the search:
“exergame”, “active video game”, “serious game”,
“exercise”, “exercise therapy”, “digital
rehabilitation”, “digital therapy support”,
“parkinson’s disease”, “parkinson”.
2.2 Expert Interviews
The objective of the observe-phase is to understand
and empathize with the user to create a suitable
product for the target group. In most cases, qualitative
interviews or quantitative surveys are conducted. The
results are used to understand needs and obstacles and
answer open questions after the first phase (Wölbling
et al., 2012).
For the observe-phase expert interviews with
physiotherapists were hold. Expert interviews are
used to gain expert knowledge through a qualitative
survey (Meuser & Nagel, 2009). The decision was
made not to conduct the interviews with
representatives of the target group themselves, as they
might have difficulties in formulating general
requirements due to the very individual
characteristics of the disease. The expert interviews
with three physiotherapists were conducted to
identify requirements for a digital game-based
therapy support. The interviews were intended to
clarify open questions and substantiate the concept
with practical experience values. Each interview
lasted half an hour and they were held between the
23.02.32021 and the 26.02.2021 due to the pandemic
situation via the video conferencing tool Teams. For
later content analysis, the interviews were recorded
and later transcribed with consent of the participants.
Questions asked during the semi-structured interview
concerned
1. methods of motor therapy for Parkinson patients
that are suitable for a digital approach,
2. strategies for dealing with lack of motivation
during therapy,
3. requirements of the target group for game
perception and design,
HEALTHINF 2022 - 15th International Conference on Health Informatics
126

4. potentials and obstacles caused by the game
mechanics and interaction and
5. idea generation and wishes for an optimal game
design.
The analysis of the interviews follows the data
analysis of expert interviews according to Meuser and
Nagel (2009) in order to obtain interpretable results.
The data analysis according to Meuser and Nagel is
divided into transcription of the recorded interview,
paraphrasing the text according to thematic units,
ordering the paraphrased passages thematically,
category formation and comparison of the statements
and finally theoretical generalization through
arranging the categories according to their internal
relations.
2.3 Concept
During the point of view-phase the generated
information from the previous phases should be
clustered and provide answers to the questions: What
problem must be solved? For whom this problem
must be solved? In the ideate-phase ideas to solve this
problem are generated. With the help of the
knowledge base, that has been accumulated, a user-
centred solution can be found. For the prototype-
phase a concrete example implementation of the final
idea is created. The prototype gives the opportunity to
experience a tangible and assessable version of the
idea (Wölbling et al., 2012).
The result of the point of view-phase is used as a
reference point to develop a concrete concept idea.
This concept idea is implemented as a prototype using
the game engine Unity 3D in version 2020.3.1f1 in
the programming language C#.
2.4 Evaluation
The finished prototype is presented to potential users
during the test-phase to give feedback on the idea and
determine the usability of the solution. With the help
of the results, the solution approach can be iteratively
revised (Wölbling et al., 2012).
The prototype was evaluated through qualitative
interviews with experts. Six participants took part,
three of whom worked as software developers for
serious games (S1, S2, S3) and three as
physiotherapists (P1, P2, P3). Two of the
physiotherapists already had experience with serious
game applications in therapy (P1, P3). Due to the
ongoing pandemic situation, the interviews were
conducted via Teams. The subjects were not able to
use the application themselves because of the current
situation but they were shown screenshots of the
menus and interface and videos of various game
scenes (introduction, calibration, game, game end) of
the prototype with exemplary use. The participants
were then asked about the suitability of the
application for the therapy and the target group and
about the usability and development of the prototype.
The interviews were held between the 24.05.2021 and
the 30.05.2021 and each interview lasted 45 minutes.
The interviews were recorded, transcribed and
analysed according to Meuser and Nagel (2009).
3 RESULTS
The results of the different design thinking-phases are
shown below. The most important findings of the
literature review, the results of the expert interviews,
the final concept resulting from these findings and the
results of the evaluation are presented.
3.1 Literature Review
The search for related work resulted in 13 serious
games for therapy support in Parkinson's patients
(Assad et al., 2011; Dauvergne al., 2018; Dias et al.,
2017; Galna et al., 2014; Garcia-Agundez et al., 2017;
Hermann et al., 2013; Nuic et al., 2018; Pachoulakis
& Papadopoulos, 2016; Pachoulakis et al., 2018;
Palacios-Navarro et al., 2015; Paraskevopoulos et al.,
2014; Sanchez- Herrera- Baeza et al., 2020; Van der
Meulen et al., 2016).
Of the applications considered, almost all can be
classified as exergames for improvement of motor
skills. Only the game by Dauvergne et al. (2018)
trains the sense of rhythm. Evaluations of the
applications show that they are capable of improving
the skills of the patients.
Most used input device for the applications were
different kinect bodytracking solutions (Xbox 360
Kinect, Kinect for Windows, Kinect for Xbox One,
Kinect 2 for Windows, Azure Kinect). Especially due
to the use without additional input devices or optical
markers, they are well suited for the target group.
Except for the collaborative serious game
Window-Washer (Hermann et al., 2013), all games
are implemented as single-player applications. There
is potential here that has not yet been exploited by the
existing range of applications.
3.2 Expert Interviews
The most important statements on the various
subtopics of the expert interview are presented below.
A Digital, Game-based Application to Support Treatment of Parkinson’s Disease: A Design Thinking Approach
127

3.2.1 Suitable Exercises
The participants reported that the motor therapy for
Parkinson’s disease patients is very diverse, and
patients are treated differently depending on their
main symptoms (P1, P2, P3). The exercises range
from gait training, stretching exercises to muscle
building but main target for every physiotherapist is
to maintain the capability to perform everyday
movements. Gait training (P2, P3), classic exercises
like squats (P2, P3) and the LSVT BIG program (P1,
P3) named the participants as suitable for a digital
game-based application.
3.2.2 Strategies to Increase Motivation
Day-dependent fatigue and depression were named as
a huge hindrance of therapy. In connection with this,
a lack of motivation often occurs (P1, P2, P3).
Sometimes patients even perform aggressive
behaviour (P3). Shame for symptoms is common but
decreases with increasing trust in the therapist (P1,
P3). The interview partners described that if a patient
is disinterested, lacking motivation, or exhausted they
often use pauses or rest periods (P1, P2, P3), but the
main goal is getting the patient back to the therapy
program (P3). In difficult cases, one participant
reported implementing an alternative stretching
program with patients (P1).
3.2.3 Requirements of the Target Group
In order to support patients in the use of technology
and to avoid safety risks, the participants agreed that
a therapist as a controlling authority should support
the patients in using the application and that a home
application would not be useful (P1, P2, P3).
According to the participants, it would be
important for the target group to be able to adjust the
difficulty of the game, because the patients should
neither be over-challenged nor under-challenged (P1,
P3). In particular, since the severity of Parkinson's
disease can vary greatly, digital therapy support
should offer a certain degree of variability (P3). For
example, the possibility to interact with the game
while standing or sitting was suggested (P1, P2, P3).
Particularly with regard to hypokinesia, three-
dimensional visualisation of the patient's body
movements would be useful to provide them with
external cues to recalibrate their body sensation and
thus help them adjust their movement size (P2).
The theme of the digital game application should
be chosen with care to appeal to the target group (P1,
P2, P3). Topics such as sports, dancing, music or
outdoor activities are interesting for most
representatives of Parkinson's patients, who are
mostly of older age (P3).
The possibility to take breaks is absolutely
necessary in a digital playful therapy supplement
because the patients tire quickly (P1, P2, P3). The
breaks should be determined by the accompanying
therapist or by the patient himself and not be dictated
by the game system (P2).
Due to the advanced age of the patients,
instructions on the correct execution of the exercise
and the use of the system should not be complex and
be given several times during the game (P1, P2).
3.2.4 Obstacles
The design as a competitive game could be
problematic if there is a large difference in
performance between the players (P3), if the players
are in poor daily form (P3) or if the players have set
themselves an unrealistic objective (P1, P3) and thus
rather reduce motivation instead of promoting it.
Another danger of the competitive situation could be
that the players overreach themselves if they are too
ambitious (P1). However, the pressure to perform or
the stress can be reduced by a well thought-out game
design. Possibilities here would be to set realistic and
individual goals (P1), to offer the prospect of partial
goals (P1), to offer incentives not to overdo oneself
(P1), to create a non-judgemental and exercise-related
environment (P3) and to direct the focus of the
application on the therapy purpose and not on
competition (P2).
Due to the age of the patients, initial scepticism
and reluctance towards the new form of interaction is
likely but should reduce over time (P2, P3). The
motor control could offer the players opportunities to
not execute the movements cleanly but still achieve
high scores (P1, P3). This should be addressed
through an appropriate exercise selection and good
movement instruction (P3). Interaction movements
should be designed with the patient's motor
symptoms in mind. In particular, tremor and the
cogwheel phenomenon could hinder interaction if
they are not taken into account (P2).
3.2.5 Potentials
All participants agreed that playful therapy methods
are a high motivational incentive for the patients.
They offer additional incentives and variety to the
therapy and expand it through gamification (P1, P3).
A competitive game design offers above all a
comparison of performance (both with one's own
performance and with that of the opponent) which can
generate strong motivation in the patients (P1, P2,
HEALTHINF 2022 - 15th International Conference on Health Informatics
128

P3). The social interaction that arises from a
competitive situation is a useful and motivating
complement to individual therapy that is also used in
group therapy (P1, P2, P3), which often incorporates
social interaction with a therapeutic purpose into a
playful setting (P1).
The motor game control through optical body
tracking as a new and interesting concept is a great
motivating factor that can encourage patients to use
the application (P3). The fact that no additional aids
are required makes it very easy to start using the
system (P1). Motor control through body tracking
technology can enable the possibility of linking
different training approaches (P1). Since the patients
themselves are responsible for the control, they can
determine the pace and the extent of movement
themselves (P1), which is not always the case with
other technical therapy supports. The visualisation of
body movement made possible by optical body
tracking can sensitise the patients' body perception
and support them in recalibrating their movement size
perception (P2).
3.2.6 Idea Generation
To optimally complement conventional therapy, the
participants wanted above all varied settings as a
playful digital supplement and ideally variable offers
for different patient interests (P1, P3). Interesting
topics mentioned were realistic scenarios from
everyday life (P1), sports to create a natural
competitive situation (P2) and the use of music and
rhythm (P2, P3).
3.3 Concept
The aim of this work is to develop a serious game that
supports and complements Parkinson's therapy. The
target group of the application are people with mild
to moderate Parkinson’s disease (Hoehn and Yahr-
scale stage I to III) (Hoehn & Yahr, 1967). In these
stages of disease, motor impairments of the patients
are present but the patients are able to manage his or
her daily life independently and the ability to stand
and walk is still given. Cognitive impairments of
memory and behaviour are not yet pronounced. The
planned application is intended to improve the
hypokinesia of the patients by integrating suitable
therapy contents and visualising the body movements
of the players on the one hand, and to counteract the
fatigue symptom through a motivating and social
game design on the other hand.
3.3.1 Genre
The conceptualised game PARKinson can be
classified as a casual game. Casual games are
characterised by easy interaction, quick-to-learn
gameplay, fast achievements and the possibility of
short play sessions. They offer frequent rewards and
a benevolent play rating (Kuittinen et al., 2007). Since
casual games often have a low level of complexity,
they are particularly suitable for an older target group
in order to avoid cognitive overload (Gerling et al.,
2011). Playing casual games is additionally able to
reduce depressive symptoms of the players
(Russoniello et al., 2009).
The theme of the game is chosen according to the
preferences of the target group (McNaney et al.,
2015; Othlinghaus et al., 2011). A gardening theme
was chosen, which is also an activity associated with
relaxation and stress reduction (Scott et al., 2015).
3.3.2 Game Idea
The interaction movements are based on the basic
idea of the LSVT BIG training to improve the
hypokinesia of the patients with extensive and
flowing movements. The LSVT (Lee Silverman Voice
Treatment) Program is a therapy concept that targets
on increasing the amplitude of the speech motor
system (LSVT LOUD) or the limb motor system
(LSVT BIG). LSVT BIG aims to enlarge motions by
recalibrating the patient’s perception of his own
movement and thus improve the hypokinesia of the
patients. The program contains different exercises,
which encourages the patient to make great
movements (Fox et al., 2012). LSVT BIG was also
considered suitable by the interview partners to be
transferred into a digital therapy application. In the
game the players have to move within their entire
kinesphere (the space around the body that can be
reached by stretching and extending limbs) (Laban &
Ullmann, 1971) in order to interact with the game.
The players select objects scattered across the game
screen with their hand. Players' body movements are
captured using the Azure Kinect. The Azure Kinect is
a camera system consisting of a depth camera and an
RGB camera. The body tracking-feature of the Azure
Kinect is able to detect human bodies and connects
them with a skeletal representation containing 32
joints. This technology allows tracking the patients’
movements and embedding them into a playful
context.
Unlike most commercial exergames, the
movements in the game only serve as a means of
interaction and not as a basis for evaluation of the
game success. Because the assessment of movement
A Digital, Game-based Application to Support Treatment of Parkinson’s Disease: A Design Thinking Approach
129
in exergames was reported as not suitable for
Parkinson's patients (McNaney et al., 2015). The
success of the game is therefore not dependent on
motor performance, which is influenced by the
disease, but on abilities that are not influenced by the
disease in mild to moderate Parkinson's disease
(Poewe et al., 2017). For a successful game, players
need to use their visual-spatial working memory
(Schumann-Hengsteler, 1996).
The game principle is derived from the classic
Matching Pairs-game (also known as Concentration
or Pairs) In Matching Pairs, the players’ task is to
find matching pairs of cards from a series of cards that
lie face down in front of the players. Players take
turns turning over two cards and the game ends when
all cards have been successfully turned over. The
player who has matched the most pairs wins (Zwick
& Paterson, 1993). The well-known game concept of
Matching Pairs facilitates the target group’s entry
into the unfamiliar field of digital therapy support
(McNaney et al., 2015; Nap et al., 2009).
Matching Pairs is a competitive multiplayer
game. Both in the interviews and in the literature, the
motivational potential of social play is emphasised
(Ryan et al., 2006). Competitive play in particular has
positive effects in terms of motivation and fun (Peng
& Crouse, 2013; Göbel et al., 2010). In this game the
players are highly interdependent because they have
access to the same resources or cards and the actions
of the opponent influence their own actions. During
the game there is negative and positive
interdependence between the players: players take
resources from each other, but the actions of the
opponent can also give players important clues about
card positions for their own actions. High
interdependence forms and strengthens social ties
(regardless of whether it is positive or negative)
(Depping et al., 2018). Social connection is in turn
associated with motivation according to the self-
determination theory (Ryan & Deci, 2000). In
addition, in Matching Pairs it is not possible to make
mistakes: either you reveal a pair of cards, or you
expand your knowledge of the card positions during
a move.
The rules of the traditional Matching Pairs game
are slightly modified in the conceptualized digital
application. Unlike Matching Pairs, there is no
provision for a player to have another turn at a found
pair to avoid long periods of inactivity and not to
further emphasis a possible cognitive imbalance of
the players.
Players interact with the game through the
position of their selected hand. They move a hand
icon across the screen and can use it to select the cards
distributed on the screen. To select, they let their hand
remain on the respective card for five seconds (which
is visually supported by a loading bar around the
icon). The motif of the selected card is then revealed.
Following the same principle, the player then selects
a second card, and its motif is also revealed. If the
card motifs are identical, the player receives a point
and, for further visual support, the captured cards are
marked with flowers in the player's colour. The
players take turns to select two cards. The game ends
automatically when all pairs of cards have been found
but can also be ended manually at any time. In both
cases, a closing screen is displayed with the players'
scores.
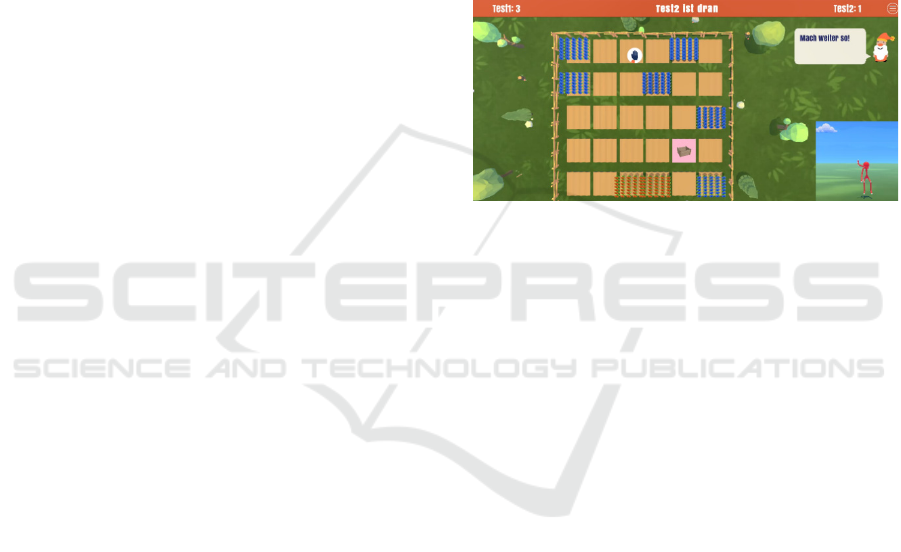
Figure 1: Exemplary play scene of PARKinson.
In addition to the free hand selection, it is possible
to play the game both sitting and standing. The
individualization of the game that was suggested in
the interviews is complemented by the fact that the
arm span of both players is recorded in a calibration
phase and the outermost cards are placed in the
individual maximum range of the players in order to
create a higher equality of opportunity with different
sizes or degrees of mobility. Pauses, that are
considered absolutely necessary by the interview
partners, are possible at any time during the game
because the players themselves take the initiative for
actions and do not have to react to actions in the game.
If the exhaustion is too great that not all pairs of cards
can be found, it is possible to end the game manually
at any time and be forwarded to the final scene. The
body movements of the players are visualised during
the game by using the skeletal representation of the
Kinect body tracking. This visualisation was
considered useful by the interviewees and in the
literature external cues about the magnitude of one's
own body movement are advised (e.g. through verbal
cues or videos) in order to adjust the patient's body
awareness and improve hypokinesia (Berardelli,
2001).
The game should be used as a supplement in the
therapy setting and supervised by a therapist (e.g. in
group therapy).
HEALTHINF 2022 - 15th International Conference on Health Informatics
130

3.4 Evaluation
The introduction of the game was considered useful
by the interview participants in order to convey the
first basic information (goals, rules, characters) (P1,
P2, P3, S2). Especially the embedding in a story or in
a dialogue with one of the characters was rated
positively as this can create an interactive feeling and
more engagement (S2).
The playful and narrative embedded testing of the
interaction including the calibration of the arm span
was rated as entertaining for the patients and good
access to the game (P1). The possibility to adapt the
game individually to the players through the
calibration and the possibility to play both sitting and
standing increases the accessibility and makes the
game therapeutically useful (P1, P2). It was suggested
that the prototype should be supplemented with the
ability to recalibrate during the play session (P3). One
respondent suggested that it would be useful to
explicitly inform the supervising therapist about the
possibility of playing while standing or sitting. At the
same time, it would be important to make sure that
the players are not demotivated when the therapist
decides that they are "only" able to play sitting down
(P1). Free hand selection is considered very useful as
it gives the supervising therapist the freedom to
choose which hand to train: The strong or the weak
side, both of which can have positive effects: either
regarding the training effect or the motivation (P1).
For the main game, the participants suggested
even stronger visual and auditory highlighting of
game-relevant events and actions for better attention
control but also motivating effects (P1, S1, S3).
Likewise, they considered different levels for
different difficulty degrees and game lengths to be
useful. Different items and functions that are
unlocked over time would increase the long-term
motivation even more (P1, P2, P3, S1, S2, S3).
The gardening theme was rated as appealing to
the target group (P1, P2, S1) but one of the
participants noted that the subject is probably more
attractive for women than for men (P2). The game
concept was rated as simple and understandable, but
nevertheless creative and appealing (P1). The familiar
game concept offered an easy entry for the target
group (P1, S1, S2). The controller-less interaction
would be intuitive and particularly well suited to the
target group (P1). The card positioning and thus the
required movements are a good adaptation of the
basic idea of LSVT BIG (S2) and would motivate the
patients to make therapeutic movements without
them happening consciously, as in the case of
working through the exercises (P1). Large and
targeted movements are trained in this way (P1, S1).
The holding times would increase the therapeutic
effectiveness (P1). It was also positively emphasised
that there is no temporal component that could create
stress among the players (P2, P3, S2). The linking of
the movements with cognitive training is useful for
the target group (P1, S2).
The ending of the game even if it is ended
prematurely was emphasised positively, because this
would not create the feeling among the players that
they would abandon the game (S1).
The participants are of the opinion that the game
would be a suitable therapy support. The patients are
challenged to use their entire range of motion (P2).
The game offers a suitable and meaningful movement
interaction for the target group to reach their
movement amplitude and can increase motivation and
thus achieve the required number of repetitions (P3).
The interaction would have effects on mobility
because the concrete targets, i.e. the cards to be
reached, would prevent powerless and listless
movements (P1). The stretching would train the
flexibility of the chest and spine, which in turn would
support breathing (P1). At the same time, balance and
coordination are trained (P1). The design as a
competition could additionally increase motivation
and the new and interactive approach could create
more interest in using it (S2). One respondent noted
that the application was not only suitable for
Parkinson's patients but could also be used for
patients with hemiparesis or for neurological patients
(P2).
In addition, the interviewees mentioned several
tangible suggestions for improvement of the interface
and the game mechanics during the evaluation, which
would go beyond the scope of this paper to mention
them all, but which were implemented additionally
after the interviews.
4 DISCUSSION
The aim of the work was to develop a concept for an
exergame for Parkinson’s disease patients with mild
to moderate Parkinson’s disease to improve
hypokinesia and fatigue. The interaction with this
exergame is made via optical body tracking through
the Azure Kinect without additional devices like
controller or physical marker.
The interview results show that the lack of
motivation, which is often caused by the disease
(Hagell & Brundin) but also by the repetitive nature
of the therapy (Fox et al., 2012), is a common
problem in Parkinson's therapy. Due to their
A Digital, Game-based Application to Support Treatment of Parkinson’s Disease: A Design Thinking Approach
131

motivating nature, serious games are suitable to be
used as a therapy addition (Rego et al., 2014). Serious
games offer a very high potential, but some
requirements and challenges have been identified for
their use as a therapy supplement for Parkinson's
patients.
This includes choosing an appropriate theme for
the target group, therefore a gardening theme was
chosen that appeals to the target group (McNaney et
al., 2015; Othlinghaus et al., 2011) and is associated
with relaxation (Scott et al., 2015). The adaptability
to the abilities of the respective players is realized
through different play modes (sitting/standing), hand
selection and calibration through arm span of the
players. In order to visualise the body movements to
recalibrate body awareness (Berardelli, 2001) the
three-dimensional skeletal representation detected by
the Kinect body tracking is displayed parallel to the
game. The last requirement mentioned in the
interviews was the possibility for players to take a
break at any time. In the concept developed, this is
made possible by the fact that the players themselves
interact proactively with the game and do not have to
react to the game. The game can be paused and, in the
event of severe exhaustion, also be stopped at any
time.
Obstacles identified in the interviews of the
requirements analysis were a possible scepticism of
the patients towards the new technical application,
which should be overcome by using a familiar casual
game concept (Nap et al., 2009) and an appealing
theme (Othlinghaus et al., 2011). As requested in the
interview, the focus is diverted from the (motor)
competition in order to avoid demotivation and
overexertion. For this reason, the Matching Pairs
concept, which challenges the visual-spatial working
memory, was chosen. The high interdependence of
the players in this concept ensures social connections
(Depping et al., 2018) and thus higher motivation
(Ryan & Deci, 2000).
The LSVT BIG training was named as a therapy
concept suitable for transfer to a digital therapy
support, which is used to improve hypokinesia (Fox
et al., 2012), which is also the aim of the application.
The basic idea of this training concept of wide and
flowing movements was adopted and combined with
a competitive game design of Matching Pairs.
In the expert interviews evaluating the concept
and the prototype, the application was rated very
positively and as suitable for supporting the therapy
of Parkinson's patients. The expert interviews were
conducted as a formative evaluation and were well
suited to identify areas for improvement and further
research potential. Unfortunately, it is not possible to
make any substantiated statements about the player's
experience, as the test persons were only able to view
screenshots and videos of the application. In order to
finally evaluate the usability and effectiveness of the
application, the comparison of objective health
variables by means of standardised measuring
instruments of a user group with a suitable control
group is necessary. In addition, individual experience
reports of the test persons should be collected (Kato,
2012). Unfortunately, this kind of testing was not
possible due to the current pandemic situation, but it
will be carried out as soon as possible. However, the
interviews revealed some potential for improvement
of the current prototype in the sense of a formative
evaluation, which can be implemented or further
investigated in the future.
Limitations for the results of both qualitative
studies are the small sample sizes. Unfortunately, the
corona pandemic has made a laboratory study for
evaluation impossible, which makes the significance
for interaction assessment very weak. A patient
perspective on the prototype would have further
enriched the evaluation, which will be included in
further studies.
Overall, the results support the assumption that a
serious exergame can be a suitable therapy
supplement for Parkinson's patients and some
characteristics for a suitable application could be
identified. In any case, further studies are needed to
evaluate training effects and to obtain assessments of
the prototype by patients and potential users. These
are planned for the near future.
REFERENCES
Assad, O., Hermann, R., Lilla, D., Mellies, B., Meyer, R.,
Shevach, L., Siegel, S., Springer, M., Tiemkeo, S.,
Voges, J., Wieferich, J., Herrlich, M., Krause, M., &
Malaka, R. (2011). Motion-based games for Parkinson’s
disease patients. Lecture Notes in Computer Science
(Including Subseries Lecture Notes in Artificial
Intelligence and Lecture Notes in Bioinformatics), 6972
LNCS, 47–58. https://doi.org/10.1007/978-3-642-
24500-8_6
Balestrino, R., & Schapira, A. H. V. (2020). Parkinson
disease. European journal of neurology, 27(1), 27-42.
https://doi.org/10.1111/ene.14108
Barone, P., Antonini, A., Colosimo, C., Marconi, R.,
Morgante, L., Avarello, T. P., Bottacchi, E., Cannas, A.,
Ceravolo, G., Ceravolo, R., Cicarelli, G., Gaglio, R., M.,
Giglia, R. M., Iemolo, F., Manfredi, M., Meco, G.,
Nicoletti, A., Pederzoli, M., Petrone, A., … Del Dotto, P.
(2009). The PRIAMO study: a multicenter assessment of
nonmotor symptoms and their impact on quality of life in
Parkinson's disease. Movement disorders: official
HEALTHINF 2022 - 15th International Conference on Health Informatics
132

journal of the Movement Disorder Society, 24(11), 1641-
1649. https://doi.org/10.1002/mds.22643
Berardelli, A. (2001). Pathophysiology of bradykinesia in
Parkinson’s disease. Brain, 124(11), 2131–2146.
https://doi.org/10.1093/brain/124.11.2131
Bloem, B. R. (1992). Postural instability in Parkinson’s
disease. Clinical Neurology and Neurosurgery,
94(SUPPL.), 41–45. https://doi.org/10.1016/0303-
8467(92)90018-X
Brown, T. (2008). Design thinking. Harvard business review,
86(6), 84.
Dauvergne, C., Bégel, V., Gény, C., Puyjarinet, F., Laffont,
I., & Dalla Bella, S. (2018). Home-based training of
rhythmic skills with a serious game in Parkinson’s
disease: Usability and acceptability. Annals of Physical
and Rehabilitation Medicine, 61(6), 380– 385.
https://doi.org/10.1016/j.rehab.2018.08.002
Delwaide, P. J. (2001). Parkinsonian rigidity. Functional
Neurology, 16(2), 147–156.
Depping, A. E., Johanson, C., & Mandryk, R. L. (2018).
Designing for friendship: Modeling properties of play,
in-game social capital, and psychological well-being.
CHI PLAY 2018 - Proceedings of the 2018 Annual
Symposium on Computer-Human Interaction in Play, 5–
17. https://doi.org/10.1145/3242671.3242702
Dias, S. B., Konstantinidis, E., Diniz, J. A., Bamidis, P.,
Charisis, V., Hadjidimitriou, S., Stadtschnitzer, M.,
Fagerberg, P., Ioakeimidis, I., Dimitropoulos, K.,
Grammalidis, N., & Hadjileontiadis, L. J. (2017). On
Supporting Parkinson’s Disease Patients: The i-
Prognosis Personalized Game Suite Design Approach.
Proceedings - IEEE Symposium on Computer-Based
Medical Systems, 2017-June, 521–526. https://doi.org/
10.1109/CBMS.2017.144
Fox, C., Ebersbach, G., Ramig, L., & Sapir, S. (2012). LSVT
LOUD and LSVT BIG: Behavioral treatment programs
for speech and body movement in Parkinson disease.
Parkinson’s Disease, 2012, 391946. https://doi.org/
10.1155/2012/391946
Friedman, J. H., Brown, R. G., Comella, C., Garber, C. E.,
Krupp, L. B., Lou, J. S., Marsh, L., Nail, L., Shulman, L.,
& Taylor, C. B. (2007). Fatigue in Parkinson’s disease:
A review. In Movement Disorders (Vol. 22, Issue 3, pp.
297–308). John Wiley & Sons, Ltd. https://doi.org/
10.1002/mds.21240
Galna, B., Jackson, D., Schofield, G., McNaney, R., Webster,
M., Barry, G., Mhiripiri, D., Balaam, M., Olivier, P., &
Rochester, L. (2014). Retraining function in people with
Parkinson’s disease using the Microsoft kinect: Game
design and pilot testing. Journal of NeuroEngineering
and Rehabilitation, 11(1), 1–12. https://doi.org/
10.1186/1743-0003- 11-60
Garcia-Agundez, A., Folkerts, A.-K., Konrad, R., Caseman,
P., Göbel, S., & Klabe, E. (2017). PDDanceCity: An
Exergame for Patients with Idiopathic Parkinson’s
Disease and Cognitive Impairment. In M. Burghardt, R.
Wimmer, C. Wolff, & C. Womser-Hacker (Eds.),
Mensch und Computer 2017 - Tagungsband (pp. 381–
386). Gesellschaft für Informatik e.V. https://doi.org/
10.18420/muc2017-mci-0334
Gerling, K. M., Schulte, F. P., & Masuch, M. (2011).
Designing and evaluating digital games for frail elderly
persons. ACM International Conference Proceeding
Series, 1–8. https://doi.org/10.1145/2071423.2071501
Göbel, S., Hardy, S., Wendel, V., Mehm, F., & Steinmetz, R.
(2010). Serious games for health - Personalized
exergames. MM’10 - Proceedings of the ACM
Multimedia 2010 International Conference, 1663–1666.
https://doi.org/10.1145/1873951.1874316
Hagell, P., & Brundin, L. (2009). Towards an understanding
of fatigue in Parkinson disease. Journal of Neurology,
Neurosurgery and Psychiatry, 80(5), 489–492.
https://doi.org/10.1136/jnnp.2008.159772
Helmich, R. C., Hallett, M., Deuschl, G., Toni, I., & Bloem,
B. R. (2012). Cerebral causes and consequences of
parkinsonian resting tremor: A tale of two circuits?
Brain, 135(11), 3206–3226. https://doi.org/10.1093/
brain/aws023
Hermann, R., Herrlich, M., Wenig, D., Smeddinck, J., &
Malaka, R. (2013). Strong and Loose Cooperation in
Exergames for Older Adults with Parkinson’s Disease. In
S. Boll, S. Maaß, & R. Malaka (Eds.), Workshopband
Mensch & Computer 2013 (pp. 249–254). Oldenbourg
Verlag.
Hoehn, M. M., & Yahr, M. D. (1967). Parkinsonism: onset,
progression, and mortality. Neurology, 17(5), 427–442.
https://doi.org/10.1212/WNL.17.5.427
Janssens, J., Malfroid, K., Nyffeler, T., Bohlhalter, S., &
Vanbellingen, T. (2014). Application of LSVT BIG
Intervention to Address Gait, Balance, Bed Mobility, and
Dexterity in 102 People With Parkinson Disease: A Case
Series. Physical Therapy, 94(7), 1014–1023.
https://doi.org/10.2522/ptj.20130232
Kato, P. M. (2012). Evaluating Efficacy and Validating
Games for Health. Games for Health Journal, 1(1), 74–
76. https://doi.org/10.1089/g4h.2012.1017
Kuittinen, J., Kultima, A., Niemelä, J., & Paavilainen, J.
(2007). Casual games discussion. Proceedings of the
2007 Conference on Future Play, Future Play ’07, 105–
112. https://doi.org/10.1145/1328202.1328221
Krupp, L. B., & Pollina, D. A. (1996). Mechanisms and
management of fatigue in progressive neurological
disorders. Current Opinion in Neurology, 9(6), 456–460.
103 https://doi.org/10.1097/00019052-199612000-
00011
Laamarti, F., Eid, M., & El Saddik, A. (2014). An overview
of serious games. International Journal of Computer
Games Technology, 2014, 54–68. https://doi.org/
10.1155/2014/358152
Laban, R., & Ullmann, L. (1971). The Mastery of Movement.
Macdonald & Evans.
Malaka, R., Herrlich, M., & Smeddinck, J. (2016).
Anticipation in motion-based games for health. In
Anticipation and Medicine (pp. 351–363). Springer
International Publishing. https://doi.org/10.1007/978-3-
319-45142-8_22
Meuser, M., & Nagel, U. (2009). The expert interview and
changes in knowledge production. In Interviewing
experts (pp. 17-42). Palgrave Macmillan, London.
https://doi.org/10.1057/9780230244276_2
A Digital, Game-based Application to Support Treatment of Parkinson’s Disease: A Design Thinking Approach
133

McNaney, R., Balaam, M., Holden, A., Schofield, G.,
Jackson, D., Webster, M., Galna, B., Barry, G.,
Rochester, L., & Olivier, P. (2015). Designing for and
with people with Parkinson’s: A focus on exergaming.
Conference on Human Factors in Computing Systems -
Proceedings, 2015-April, 501–510.
https://doi.org/10.1145/2702123.270231
Nap, H. H., Kort, Y. A. W. De, & Ijsselsteijn, W. A. (2009).
Senior gamers: Preferences, motivations and needs.
Gerontechnology, 8(4).
https://doi.org/10.4017/gt.2009.08.04.003.00
Nuic, D., Vinti, M., Karachi, C., Foulon, P., Hamme, A. Van,
& Welter, M.-L. (2018). The feasibility and positive
effects of a customised videogame rehabilitation
programme for freezing of gait and falls in Parkinson’s
disease patients: a pilot study. Journal of
NeuroEngineering and Rehabilitation, 15(1), 31–42.
https://doi.org/https://doi.org/10.1186/s12984-018-
0375-x
Othlinghaus, J., Gerling, K. M., & Masuch, M. (2011).
Intergenerational Play: Exploring the Needs of Children
and Elderly. In M. Eibl & M. Ritter (Eds.), Workshop-
Proceedings der Tagung Mensch & Computer 2011 (pp.
317–322). Universitätsverlag Chemnitz.
Pachoulakis, I., & Papadopoulos, N. (2016). Exergames for
Parkinson’s Disease patients: The balloon goon game.
2016 International Conference on Telecommunications
and Multimedia, TEMU 2016, 12–17.
https://doi.org/10.1109/TEMU.2016.7551908
Pachoulakis, I., Papadopoulos, N., & Analyti, A. (2018).
Kinect-based exergames tailored to Parkinson patients.
International Journal of Computer Games Technology,
2018. https://doi.org/10.1155/2018/2618271
Palacios-Navarro, G., García-Magariño, I., & Ramos-
Lorente, P. (2015). A Kinect-Based System for Lower
Limb Rehabilitation in Parkinson’s Disease Patients: A
Pilot Study. Journal of Medical Systems, 39(9), 1–10.
https://doi.org/10.1007/s10916-015-0289-0
Paraskevopoulos, I. T., Tsekleves, E., Craig, C., Whyatt, C.,
& Cosmas, J. (2014). Design guidelines for developing
customised serious games for parkinson’s disease
rehabilitation using bespoke game sensors.
Entertainment Computing, 5(4), 413–424.
https://doi.org/10.1016/j.entcom.2014.10.006
Peng, W., & Crouse, J. (2013). Playing in parallel: The
effects of multiplayer modes in active video game on
motivation and physical exertion. Cyberpsychology,
behavior, and social networking, 16(6), 423-427.
https://doi.org/10.1089/cyber.2012.0384
Poewe, W., Seppi, K., Tanner, C. M., Halliday, G. M.,
Brundin, P., Volkmann, J., Schrag, A. E., & Lang, A. E.
(2017). Parkinson disease. Nature reviews Disease
primers, 3(1), 1-21. https://doi.org/10.1038/nrdp.20
17.13
Rego, P. A., Moreira, P. M., & Reis, L. P. (2014).
Architecture for serious games in health rehabilitation.
Advances in Intelligent Systems and Computing, 276(2),
307–317. https://doi.org/10.1007/978-3-319-05948-
8_30
Ritterfeld, U., Cody, M., & Vorderer, P. (Eds.). (2009).
Serious games: Mechanisms and effects. Routledge.
Russoniello, C. V., O’Brien, K., & Parks, J. M. (2009). The
effectiveness of casual video games in improving mood
and decreasing stress. Journal of CyberTherapy and
Rehabilitation, 2(1), 53–67.
Ryan, R. M., & Deci, E. L. (2000). Self-determination theory
and the facilitation of intrinsic motivation, social
development, and well-being. American Psychologist,
55(1), 68–78. https://doi.org/10.1037//0003-066x.5
5.1.68
Ryan, R. M., Rigby, C. S., & Przybylski, A. (2006). The
motivational pull of video games: A self-determination
theory approach. Motivation and Emotion, 30(4), 347–
363. https://doi.org/10.1007/s11031-006-9051-8
Sánchez-Herrera-Baeza, P., Cano-de-la-Cuerda, R., Oña-
Simbaña, E. D., Palacios-Ceña, D., Pérez-Corrales, J.,
Cuenca-Zaldivar, J. N., Gueita-Rodriguez, J., Balaguer-
Bernaldo de Quirós, C., Jardón-Huete, A., & Cuesta-
Gomez, A. (2020). The Impact of a Novel Immersive
Virtual Reality Technology Associated with Serious
Games in Parkinson’s Disease Patients on Upper Limb
Rehabilitation: A Mixed Methods Intervention Study.
Sensors, 20(8), 2168. https://doi.org/10.3390/s20082168
Schumann-Hengsteler, R. (1996). Children’s and adults’
visuospatial memory: The game concentration. Journal
of Genetic Psychology, 157(1), 77–92. https://doi.org/
10.1080/00221325.1996.9914847
Scott, T. L., Masser, B. M., & Pachana, N. A. (2015).
Exploring the health and wellbeing benefits of gardening
for older adults. Ageing and Society, 35(10), 2176–2200.
https://doi.org/10.1017/S0144686X14000865
Stocchi, F., Abbruzzese, G., Ceravolo, R., Cortelli, P.,
D’Amelio, M., De Pandis, M. F., Fabbrini, G., Pacchetti,
C., Pezzoli, G., Tessitore, A., Canesi, M., Iannacone, C.,
& Zappia, M. (2014). Prevalence of fatigue in Parkinson
disease and its clinical correlates. Neurology, 83(3), 215–
220. https://doi.org/10.1212/WNL.0000000000000587
Van Der Meulen, E., Cidota, M. A., Lukosch, S. G., Bank, P.
J. M., Van Der Helm, A. J. C., & Visch, V. T. (2017). A
Haptic Serious Augmented Reality Game for Motor
Assessment of Parkinson’s Disease Patients. Adjunct
Proceedings of the 2016 IEEE International Symposium
on Mixed and Augmented Reality, ISMAR-Adjunct 2016,
102–104. https://doi.org/10.1109/ISMAR-Adjunct.20
16.0050
Wölbling, A., Krämer, K., Buss, C. N., Dribbisch, K., LoBue,
P., & Taherivand, A. (2012). Design thinking: An
innovative concept for developing user-centered
software. In Software for people (pp. 121-136). Springer,
Berlin, Heidelberg.
Zwick, U., & Paterson, M. S. (1993). The memory game.
Theoretical Computer Science, 110(1), 169–196.
https://doi.org/10.1016/0304-3975(93)90355-W
HEALTHINF 2022 - 15th International Conference on Health Informatics
134
