
Study of the User Behaviour Caused by Automatic Recommendation
Systems Call to Action
Georgy Kopanitsa
1a
and Sergey Kovalchuk
2,1 b
1
ITMO University, Birzhevaya 4, Saint-Petersburg, Russia
2
Almazov National Medical Research Centre, Akkuratova Street, Saint-Petersburg, Russia
Keywords: Symptom Checker, User Acceptance, Follow-up Rates.
Abstract: Diagnostics accuracy and usability of symptom checkers have been researched in several studies. Their ability
to set a correct diagnosis especially in the urgent cases is questionable. There is one aspect of symptom
checkers that has not been deeply studied yet. It is their ability to motivate patients to follow up after receiving
a direct recommendation and to decrease a load on the health care professionals. The goal of this research is
to study how patients behave after receiving a recommendation from a symptom checker and motivation of
this behaviour. We studied how patients react on the symptom checker recommendations and the motivation
behind this behaviour. In total we invited 3615 patients to have a symptom checker screening; 2374 of them
agreed to run a symptom checker screening; 867 of them agreed to participate in the study. The proportion of
the patients who agreed to have a symptom checker screening. So, we can clearly see that symptom checker
screening doesn’t result in a significant decrease of the load on healthcare professionals. This is supported by
the quantitative study results. The patients emphasized the ease of use of the tool and clearness of the
recommendations it gives. However, they perceived it as rather a second opinion tool or a tool that helps to
prepare to the doctor’s visit.
1 INTRODUCTION
The World Health Organisation (WHO) stated in
2013 that the world was short of 7.2 million
healthcare professionals of all disciplines. This
number will likely increase to 12.9 million by 2035
(Aluttis, Bishaw, & Frank, 2014). Primary care is
particularly (Karimi‐Shahanjarini et al., 2019)
affected, with severe lack of health care professionals
in most of the countries (Poppe et al., 2014; Wu,
Zhao, & Ye, 2016; Zihindula, John, Gumede, &
Gavin, 2019).
In large countries with remote area there is
another problem to transport patients to the points of
care.
This has several consequences for the healthcare
systems. One of the main and most problematic
issues are a reduced access to health care, growing
inequity, long waiting times (Griffith, Evans, & Bor,
2017), increased load on the emergency services
(Djahel, Smith, Wang, & Murphy, 2015; Stewart,
a
https://orcid.org/0000-0002-6231-8036
b
https://orcid.org/0000-0001-8828-4615
Lang, Wang, & Innes, 2019). This all lead to the late
diagnostics and not optimal treatment. Traditional
doctors oriented clinical decision support systems
could reduce a workload on the doctors. This was
not enough to solve all the listed problems. Machine
learning (ML) and Artificial Intelligence (AI)
methods in data-driven decision support systems
helped to reduce healthcare professionals workload,
allowed more efficient management of clinical
resources and help patients access medical services
(Battineni, Sagaro, Chinatalapudi, & Amenta, 2020;
Fraser, Coiera, & Wong, 2018).
Online and point of care symptom checkers are
becoming a tool that is supposed to be patient
oriented and solve the problem of initial screening
and help people in remote areas to have a first
medical contact (Baker et al., 2020).
Diagnostics accuracy and usability of symptom
checkers have been researched in several studies.
Their ability to set a correct diagnosis especially in
the urgent cases is questionable (Ceney et al., 2021).
Kopanitsa, G. and Kovalchuk, S.
Study of the User Behaviour Caused by Automatic Recommendation Systems Call to Action.
DOI: 10.5220/0010840000003123
In Proceedings of the 15th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2022) - Volume 5: HEALTHINF, pages 499-503
ISBN: 978-989-758-552-4; ISSN: 2184-4305
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
499
There is one aspect of symptom checkers that has
not been deeply studied yet. It is their ability to
motivate patients to follow up after receiving a
direct recommendation and to decrease a load on the
health care professionals.
The goal of this research is to study how
patients behave after receiving a recommendation
from a symptom checker and motivation of this
behavior.
2 METHODS
2.1 Symptom Checker
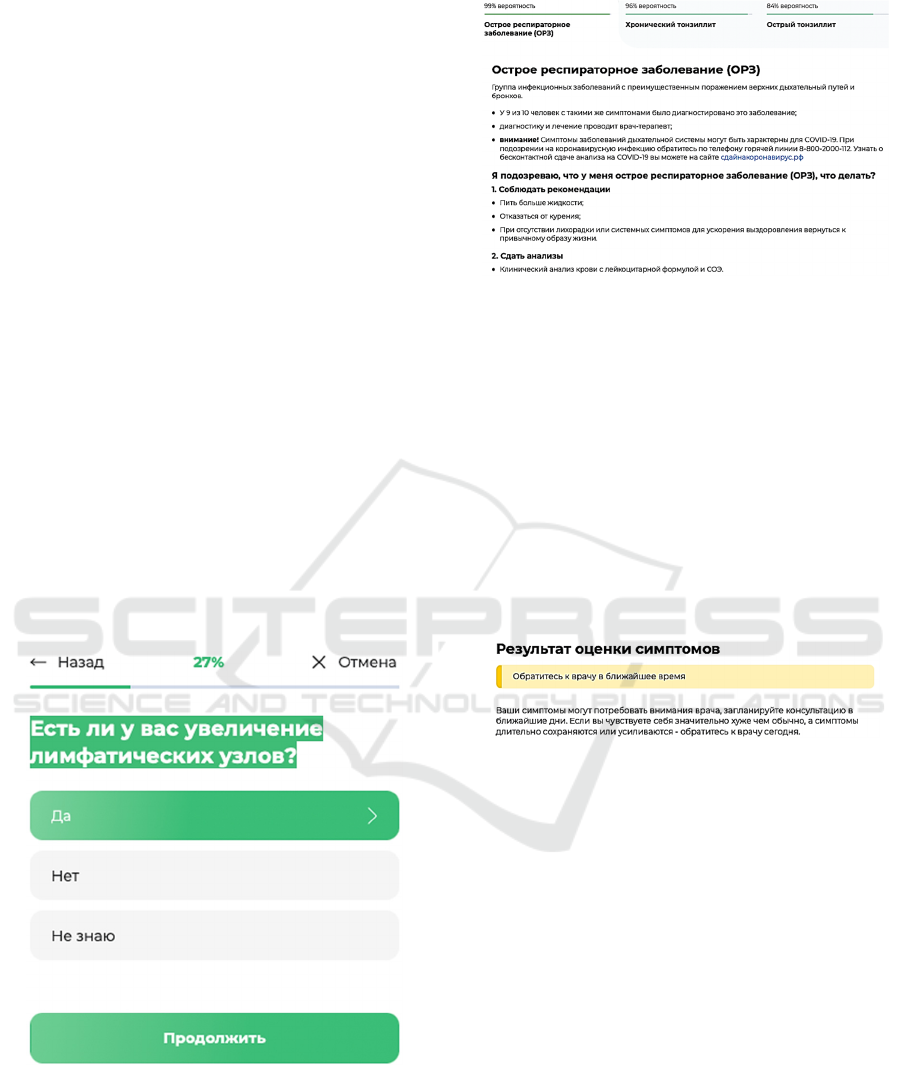
A symptom checker that is being studied is a general-
purpose diagnostic symptom checker that is based on
the Bayesian classifier. It askes multiple choice
questions (figure 1), suggests 3 most probable
diagnosis after a conversation (figure 2), and offers a
call to action (figure 3) to follow up with a doctor or
not. The average number of questions in one patient
interaction was 11. There were 3 types of call for
action messages: You need to see a doctor urgently
(red), it would be good to see a doctor soon if you feel
worse (yellow), there is no need to see a doctor now
(green).
Figure 1: Question example. Translation from Russian: Do
you have enlarged lymph nodes? Yes, No, Not Sure;
Continue.
Figure 2: Diagnosis suggestions.
Translation from Russian:
Acute respiratory disease
A group of infectious diseases that mainly affects the
upper respiratory tract and bronchi.
Nine out of 10 people with the same symptoms have
been diagnosed with this disease.
Diagnosis and treatment are carried out by a general
practitioner;
Warning! Respiratory system symptoms may be
characteristic of COVID-19. If you suspect a
coronavirus infection, call the hotline at 8-800-2000-
112. To learn about noncontact testing for COVID-
19, visit сдайнакоронавирус.рф
Figure 3: Call to action. Translation from Russian: Result
of symptom screening.
It would be good to see your doctor soon.
Your symptoms may need your doctor's attention,
schedule a consultation in the next few days. If you
feel significantly worse than usual and your
symptoms persist or get worse, see your doctor today.
2.2 Recommendations Follow Up
The first part of the study was dedicated to calculation
of a follow-up rate.
The patients were offered to work with a symptom
checker before a doctor’s visit. Facilitators, who were
not healthcare professionals supported patients with
the symptom checker operation. The patients were
motivated by a gift voucher that they could use for the
medical services in the clinic.
A proportion of patients who accepted the offer
was calculated by the research team.
HEALTHINF 2022 - 15th International Conference on Health Informatics
500

After the patients have completed a symptom checker
session, we invited them to participate in the study.
Inclusion criteria were:
Age > 18
Purpose of visit: primary visit
Completed a symptom checker session
Exclusion criteria were:
Age < 18
Secondary visit scheduled by a doctor
Those who had agreed were offered to sign a consent
for that contained the purpose and the details of the
study. They were also asked to fill in a short
questionnaire that contained basic demographic
information: age, gender, education and contact
details.
After the consent form and a questionnaire were
submitted to the research team, the patients were
asked to provide the results of the symptom checker
session.
The patients were asked if they would like to have a
follow up visit with a doctor or not.
We calculated the proportion of patients who wanted
to have a follow up and those how didn’t for the
following groups of the patients:
Green call to action (No need to see a doctor)
Yellow call to action (Self-observation and
may be see a doctor later)
Red call to action (Urgently see a doctor)
The study was performed in a private outpatient clinic
in March-April 2021.
The study got the approval by the local ethics
committee.
2.3 Motivation Study
The second part of the study was dedicated to
understanding the motivation to follow up or not on
the symptom checker recommendations. We invited
all the patients to take part in the interview. All the
patients invited to interview were notified of the
objectives of the study and of the purpose of the
interviews in written.
The study was designed as a series of semi-structured
interviews based on a topic guide, which was
developed by the study team and reviewed by the
local ethics committee.
Interviews has the following agenda:
1. Was the symptom checker user friendly and easy
to use?
1.1. Did you understand the recommendations?
1.2. Did you understand the diagnosis that the
symptom checker provided?
2. Did the symptom checker influence your decision
to follow up with a doctor?
3. Why did you decide to follow up or not after a
symptom checker session?
The guide included open questions to provide good
understandings of the patients’ opinion, without
influencing from an interviewee. We applied a
probing approach (Eeg-Olofsson, Johansson, Linder,
& Leksell, 2020) during interviews to encourage
patients to express openly.
Demographic characteristics of the study population
are presented in the table 1.
Table 1: Demographic details of the study population.
Gender Aver
age
age
Age
> 60
Education
Higher Secondary Below
secondary
346
Males
42.6 106 98 238 10
521
Females
43.1 134 125 384 12
Total
867
42.9 240 223 622 22
The interviews were performed by two members of
the research team.
Each interviewee was in written assured of anonymity
and confidentiality of the study participation. They
were informed of their right to revoke personal data
from the study at any time.
The interview duration was 10 to 20 minutes and all
of them provided sufficient information for the study.
A combination of thematic analysis and a grounded
theory approach was used to analyze the
interviewees’ responses (Marcellus, 2005; Skeat &
Perry, 2008).
3 RESULTS
3.1 Recommendations Follow Up
Results
In total we invited 3615 patients to have a symptom
checker screening; 2374 of them agreed to run a
symptom checker screening; 867 of them agreed to
participate in the study. The proportion of the patients
who agreed to have a symptom checker screening.
Study of the User Behaviour Caused by Automatic Recommendation Systems Call to Action
501
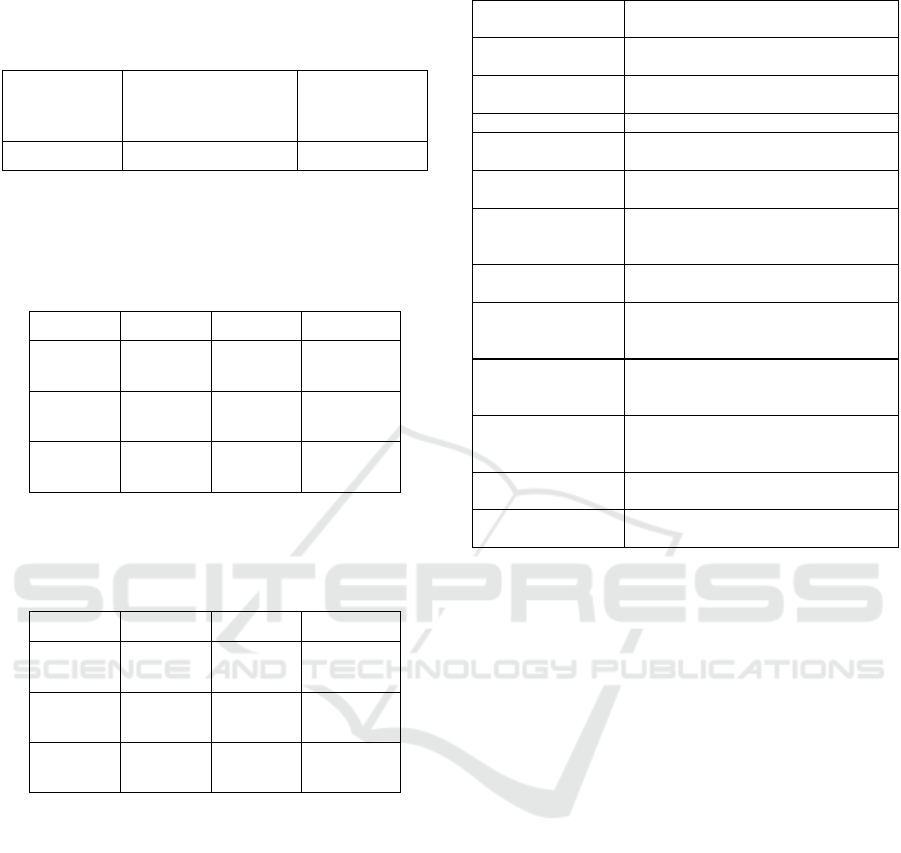
Table 2 contains the details of the patients’
acceptance rates.
Table 2: Study population.
Patients
approached
Agreed to the
symptom checker
screening
Agreed to
participate in
the study
3615 2374 (65,67%) 867 (23,98%)
Table 3 provides a classification of the study
participants into groups.
Table 3: Distribution of the patients according to the call to
action.
Gender Green Yellow Red
Male
(346)
65
(18,79%)
213
(61,6 %)
68
(19,65%)
Female
(521)
101
(19,38%)
341
(65,45%)
79
(15,16%)
Total
(867)
166
(19,15%)
554
(63,9%)
147
(16,96%)
Table 4 presents follow up rates for each group of
patients.
Table 4: Follow-up rates.
Gender Green Yellow Red
Male
46
(70,8%)
204
(95,8 %)
68 (100%)
Female 74
(73,3%)
329
(96,5%)
79 (100%)
Total 120
(72,3%)
545
(96,2%)
147
(100%)
3.2 Behaviour Motivation
We have interviewed 48 patients, who agreed on this
part of the study and signed a consent form.
The thematic analysis identified 4 core topics
related to the patients’ responses, namely: (1)
usability, (2) intention to use, (3) trust, and (4) data
protection.
The first core topic highlighted the usability and
clearness of the questions and recommendations. The
second core topic demonstrated that the patients have
strong wish to use the symptom-checker for
screening. The core topic number 3 identified the
issue of trust. The topic 4 identified personal data
security and protection awareness. Table 5 present
selected responses to support the obtained results.
Table 5: Selected answers.
Core topic and
Code
Selected responses
Usability Time It doesn’t take much time to do a
screening [A1]
Usability clearness The questions were clear to me, I could
answe
r
them easily [A2]
Usability Time This tool can save my time [A3]
Intention to use
Second opinion
I think this tool can be best used as a
second opinion [A4]
Intention to use
Second opinion
I can use it to better prepare to the
doctor’s questions [A5]
Intention to Use
Second opinion
The portal allows to quickly update It
can help me to be better informed on
my health conditions [A6]
Intention to Use
Second opinion
I still want to talk to a real doctor [A7]
Trust Explanation The system explains the results clearly,
so I can make an informed decision
[A8]
Trust Explanation I can see the logic behind the decision,
so I can base my decision on what the
system recommends [A9]
Trust User
enthusiasm
The recommendations are clear, so I
can rely on them when deciding to
follow up [A10]
Data protection
Privacy
It’s good that no personal data is
collected [A11]
Data protection
Privacy
The session is anonymous, so I can trust
the system [A12]
4 DISCUSSION
As we can see from the follow up rate results, the
urgent recommendations cause a 100% follow up
rate. A red message always resulted in the doctor’s
visit. Yellow messages with a recommendation to
visit a doctor soon if the health conditions do not
improve also resulted in almost a 100% follow up rate
with actual number of 96,2%. The only
recommendation that filtered some of the patients and
prevented some of the not required visits was a green
message with 72,3% follow up rate. So, we can
clearly see that symptom checker screening doesn’t
result in a significant decrease of the load on
healthcare professionals. This is supported by the
quantitative study results. The patients emphasized
the ease of use of the tool and clearness of the
recommendations it gives. However, they perceived
it as rather a second opinion tool or a tool that helps
to prepare to the doctor’s visit.
Our results add a discussion point to the
efficiency of the symptom checker in terms of being
able to decrease a load on the healthcare professionals
or even replace them in some situations.
We didn’t observe any behavioral difference
between males and females.
HEALTHINF 2022 - 15th International Conference on Health Informatics
502

4.1 Limitations of the Study
In this study we did not assess the accuracy and other
efficiency characteristics of the symptom checker.
This will become a subject of the further study. The
second limitation of the study is that we didn’t
research how the screenings affected the length of the
actual doctor’s visit, which will also become an
objective of the further studies.
5 CONCLUSIONS
Our findings suggest that automatic symptom
checkers don’t significantly decrease a load on
healthcare professionals as they are mostly perceived
as a second opinion tool.
ACKNOWLEDGEMENTS
This work was supported financially by the Ministry
of Science and Higher Education of the Russian
Federation, Agreement No. 075-15-2021-1013
(08.10.2021) (Internal project number
13.2251.21.0067).
REFERENCES
Aluttis, C., Bishaw, T., & Frank, M. W. (2014). The
workforce for health in a globalized context – global
shortages and international migration. Global Health
Action, 7(SUPP.1). Retrieved October 6, 2021 from
https://doi.org/10.3402/GHA.V7.23611
Baker, A., Perov, Y., Middleton, K., Baxter, J., Mullarkey,
D., Sangar, D., Johri, S. (2020). A Comparison of
Artificial Intelligence and Human Doctors for the
Purpose of Triage and Diagnosis. Frontiers in Artificial
Intelligence, 3. Retrieved October 6, 2021 from
https://doi.org/10.3389/FRAI.2020.543405
Battineni, G., Sagaro, G. G., Chinatalapudi, N., & Amenta,
F. (2020). Applications of Machine Learning Predictive
Models in the Chronic Disease Diagnosis. Journal of
Personalized Medicine 2020, Vol. 10, Page 21, 10(2),
21. Retrieved October 6, 2021 from https://doi.org/
10.3390/JPM10020021
Ceney, A., Tolond, S., Glowinski, A., Marks, B., Swift, S.,
& Palser, T. (2021). Accuracy of online symptom
checkers and the potential impact on service utilisation.
PLOS ONE, 16(7), e0254088. Retrieved October 6,
2021 from https://doi.org/10.1371/JOURNAL.PONE.0
254088
Djahel, S., Smith, N., Wang, S., & Murphy, J. (2015).
Reducing emergency services response time in smart
cities: An advanced adaptive and fuzzy approach. 2015
IEEE 1st International Smart Cities Conference, ISC2
2015. Retrieved October 6, 2021 from https://doi.org/
10.1109/ISC2.2015.7366151
Eeg-Olofsson, K., Johansson, U.-B., Linder, E., & Leksell,
J. (2020). Patients’ and Health Care Professionals’
Perceptions of the Potential of Using the Digital
Diabetes Questionnaire to Prepare for Diabetes Care
Meetings: Qualitative Focus Group Interview Study.
Journal of Medical Internet Research, 22(8). Retrieved
October 6, 2021 from https://doi.org/10.2196/17504
Fraser, H., Coiera, E., & Wong, D. (2018). Safety of
patient-facing digital symptom checkers. The Lancet,
392(10161), 2263–2264. Retrieved October 6, 2021
from https://doi.org/10.1016/S0140-6736(18)32819-8
Griffith, K., Evans, L., & Bor, J. (2017). The affordable care
act reduced socioeconomic disparities in health care
access. Health Affairs, 36(8), 1503–1510. Retrieved
October 6, 2021 from https://doi.org/10.1377/
HLTHAFF.2017.0083/ASSET/IMAGES/MEDIUM/2
017.0083FIGEX1.EPS.GZ.GIF
Karimi-Shahanjarini, A., Shakibazadeh, E., Rashidian, A.,
Hajimiri, K., Glenton, C., Noyes, J., Colvin, C. J.
(2019). Barriers and facilitators to the implementation
of doctor-nurse substitution strategies in primary care:
a qualitative evidence synthesis. The Cochrane
Database of Systematic Reviews, 2019(4). Retrieved
October 6, 2021 from https://doi.org/10.1002/
14651858.CD010412.PUB2
Marcellus, L. (2005). The Grounded Theory Method and
Maternal-Infant Research and Practice. Journal of
Obstetric, Gynecologic & Neonatal Nursing, 34(3),
349–357. Retrieved October 6, 2021 from
https://doi.org/10.1177/0884217505276053
Poppe, A., Jirovsky, E., Blacklock, C., Laxmikanth, P.,
Moosa, S., Maeseneer, J. de, Peersman, W. (2014).
Why sub-Saharan African health workers migrate to
European countries that do not actively recruit: a
qualitative study post-migration. Global Health Action,
7(1), 24071. Retrieved October 6, 2021 from
https://doi.org/10.3402/GHA.V7.24071.
Skeat, J., & Perry, A. (2008). Grounded theory as a method
for research in speech and language therapy.
International Journal of Language and Communication
Disorders, 43(2), 95–109. Retrieved October 6, 2021
from https://doi.org/10.1080/13682820701437245
Stewart, D., Lang, E., Wang, D., & Innes, G. (2019). Are
emergency medical services offload delay patients at
increased risk of adverse outcomes? Canadian Journal
of Emergency Medicine, 21(4), 505–512. Retrieved
October 6, 2021 from https://doi.org/10.1017/
CEM.2018.478
Wu, Q., Zhao, L., & Ye, X.-C. (2016). Shortage of
healthcare professionals in China. BMJ, 354, i4860.
Retrieved October 6, 2021 from https://doi.org/
10.1136/BMJ.I4860
Zihindula, G., John, R. A., Gumede, D. M., & Gavin, M. R.
(2019). A review on the contributions of NGOs in
addressing the shortage of healthcare professionals in
rural South Africa. http://www.editorialmanager.com/
cogentsocsci, 5(1). Retrieved October 6, 2021 from
https://doi.org/10.1080/23311886.2019.1674100
Study of the User Behaviour Caused by Automatic Recommendation Systems Call to Action
503
