
RoSe: Robot Sentinel as an Alternative for Medicinal or Physical
Fixation and for Human Sitting Vigils
Robert Erzgr
¨
aber, Falko Lischke, Frank Bahrmann and Hans-Joachim B
¨
ohme
University of Applied Sciences Dresden, Friedrich-List Platz 1, Dresden, Germany
Keywords:
Service Robot, Sitting Vigil, Medical Restraints, Image Classification, Human-robot Interaction.
Abstract:
An approach for a Robot Sentinel is described as an alternative to medicinal or physical fixation. The robot
offers the opportunity to give the patient some privacy while also offering protection from falling out of bed.
This approach is solely based on input data given by a Kinect One. A database with IR data with labels
according to the sleep stages of the patient was generated. With given database the presented framework is
able to detect the movement of the patient in bed from given input data and therefore warn the staff, if a
possible harmful situation occurs. In two different experimental phases the approach could be tested and was
able to successfully recognize different sleeping phases of the patient (e.g. unsettled sleep, falling asleep and
wakeup phase). An unsettling sleep serves as an indication of waking up and therefore the possible desire
of standing up. Recognizing those sleeping phases and counteracting this desire, preserves the patient from
falling out of bed and potential injury.
1 INTRODUCTION
A sitting vigil is used in hospital and nursing home
environments to observe cognitively impaired pa-
tients while sleeping or having to stay in bed, for ex-
ample after surgery or if the person is endangered by
being on their own. Preferably a medical student is
hired as sitting vigil but in most cases, an unlearned
assistant takes this position. Especially in geriatric
cases many patients can loose their sense of their cur-
rent location and are disoriented when waking up at
night. Therefore, several methods include the use
of chemicals, which keep the patient in a somno-
lent condition, or physical restraints to ensure a cer-
tain, safe position. To physically restrain a patient,
an allowance by the Court of Protection is necessary.
If waiting for the allowance would cause immediate
harm, the physical restraints can be used, but an al-
lowance has to be requested as soon as possible
1
. Sze
et al. have shown in their meta-study (Sze et al., 2012)
that the amount of falls, can not be associated with
a lesser use of physical restraints in favor for other
restriction methods. Alternative methods with their
own disadvantages would be the usage of sitting vig-
ils (shortage of staff) or chemical restraints (e.g. mis-
1
Further informations can be seen in §1906 of the
B
¨
urgerliches Gesetzbuch of the Federal Republic of Ger-
many.
use, physical and mental side effects). While (Kr
¨
uger
et al., 2013) shows that physical restraints are used in
standard care in hospitals of Germany, even though
multiple intervention programs are aimed to reduce
their usage. Either way, the privacy and the personal
freedom of the patient is restricted and it should be
one of the last methods to keep the patient in bed.
While sitting vigils potentially have a medical back-
ground of some sort, they are not allowed to interfere,
only to signal the medical staff that an emergency is
about to happen or is happening.
In Germany, night-time medical staff of a neurol-
ogy ward has, per law, at full capacity, 20 patients
per nurse (see §6 passage 1.7 in PpUGV (Leber and
Vogt, 2020)) to look after. Besides some differences
between various wards in a hospital, except for inten-
sive care units, there are more than 10 patients per
medical staff to look after. Nevertheless, neither are
all patients in one room nor is it possible to look af-
ter all of them at the same time. Therefore multiple
ward rounds, usually four hours apart, are executed at
night, where each room is visited to see whether all
patients are in good condition and/or sleeping. Be-
tween these ward rounds, the patient’s room is only
visited if an alarm is signaled by the patient. If no
alarm is signaled because, for example, the patient has
fallen out of the bed and is lying unconsciously on the
floor, the incident will only be discovered on the next
184
Erzgräber, R., Lischke, F., Bahrmann, F. and Böhme, H.
RoSe: Robot Sentinel as an Alternative for Medicinal or Physical Fixation and for Human Sitting Vigils.
DOI: 10.5220/0010827100003123
In Proceedings of the 15th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2022) - Volume 4: BIOSIGNALS, pages 184-191
ISBN: 978-989-758-552-4; ISSN: 2184-4305
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

ward round. This in combination with the rising need
for medical staff - an increase of approximately 25%
by 2035 is calculated for Germany alone (Sonnenburg
and Schr
¨
oder, 2019) - offers an opportunity to support
wards with a robot that can monitor sleeping patients
while the staff has the chance to care about the other
ones.
The proposed framework was built and tested on
the self recorded and labelled database, which was
formed in two different experimental phases.
1.1 Robot
Kinect
One
Touchscreen
Head
Body
Status LED Strip
Moveable Eyes
with Eyelids
Laser-Range-Finder
(Forwards and backwards)
Tactile collision sensor
Figure 1: The anthropomorphic robot of the type Scitos G5
features a Kinect One mounted on a pan-tilt unit, a head
with led lights and moveable eyes with eyelids, a touch-
screen and the body itself. The body contains two laser-
range-finder (forwards and backwards), a tactile sensor, and
a differential drive.
The robot has a pin-shape design with multiple
sensors and features built in (see Figure 1). It is
based on the Scitos G5 platform from MetraLabs
2
but
has several additions, like the Kinect One on top of
the head and two additional speakers which are po-
sitioned nearby the head. The camera can be moved
and tilted to some degree, which enables the patient to
see what direction the robot currently observes. The
head features no sensors built into it, but has two eyes
which serves directly as interaction point for the pa-
tient and are able to keep eye contact while speaking
to her or him. Furthermore the robot has a touch-
screen monitor built in. During the Robot Sentinel
functionality the monitor is usually powered off, but
can also be used to display medical data for staff or
2
For further information about the platform please refer
to https://www.metralabs.com/mobiler-roboter-scitos-g5/
patient alike. The body has a protective chassis to
hide the computing system and sensors. In the lower
body of the robot is one front and one back-facing
laser-range-finder, and a tactile sensor, which stops
the robot instantly as an emergency system in case
an unforeseeable collision occurs. The entirety of the
robot is 1.8m tall, with the head being at comfortably
1.6m and weighs 80kg. This results in a trustable plat-
form with a human-like appearance.
1.2 State of the Art
Two different approaches to the presented framework
that work in a similar way could be found. One is
a market-ready product and a camera-based approach
with edge-computing.
The camera-based system Ocuvera was created
for patient monitoring with the same goal of alarming
the hospital staff in advance, if the patient would leave
the bed (Bauer et al., 2017). This system is mounted
in a docking station at the wall and has therefore a
fixed field of view where the patients bed has to be,
but can be moved easily between different docking
stations. The system has a display and a speaker at-
tached to it, so that music and/or images or videos
can be displayed. The difference to our proposed ap-
proach is that the robot itself has a human-like ap-
pearance with an head, so that the patient has a fixed
position to speak to. Moreover, the robot itself is not
immobile. The mobility of the robot can react to dif-
ferent positions of the bed in the room without dis-
mounting and mounting the docking station. Even if
the bed has to be moved at night the robot can posi-
tion itself to have an unobstructed view of the patients
bed.
Another camera-based fall protection system that
uses deep learning methods is described in (Chang
et al., 2021). In this case, only a camera, mounted
on the wall behind the bed, and a wifi-router with
edge-computing is needed. This allows the camera
to directly include the birds-eye-view of the patients
bed and therefore saves computing time. The router
will send an alarm to a mobile device if the patient is
sitting up or is in immediate danger of falling out of
bed. The advantage of this system over the proposed
approach is that the birds-eye-view of the camera does
not have to be calculated and therefore offers a better
point of view (see Section 2.5). But, like the Ocu-
vera system, the mobility of the proposed system is a
disadvantage while a hidden camera is monitoring the
patient.
RoSe: Robot Sentinel as an Alternative for Medicinal or Physical Fixation and for Human Sitting Vigils
185
2 APPROACH
IR datadepth data
DetectedBed
Image Separator
Processor
People
Divider
Processor
Float Image
To 3D Data
Converter
Movement
Detection
Processor
Alarm
face data
BedFrameCha
nged
Body Part
Clustering
Processor
Bed Detection Processor
Fast
Detection
Processor
Update
Detection
Processor
Neural
Network
Yolov5
Camera
Information gatheringBed detectionImage separation
Movement
detection
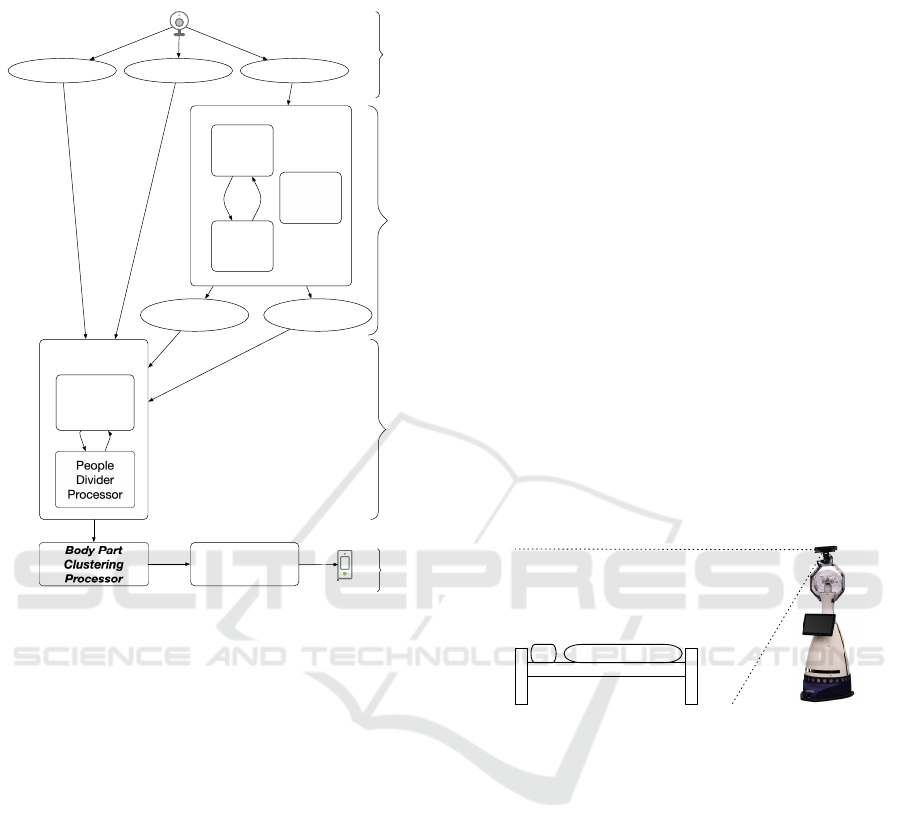
Figure 2: The data flow of the proposed approach from the
camera to the warning system, which is enabled if a move-
ment was detected. It is separated into four parts - gathering
information, bed detection, image separation and movement
detection.
2.1 Information Gathering
In Figure 2 the data flow from the camera to the warn-
ing signal is depicted. It starts with the information
gathering by the Kinect One. The gathered informa-
tion is a 640x480px infrared(IR)/depth image and, if
spotted, face detections as a rectangle with hypoth-
esis. The RGB image is not usable in this context
because the setting will most likely be used at night
without any light-sources, so the RGB image will stay
at most times black. These information are stored sep-
arately into different containers to reduce the amount
of information spread throughout the code.
2.2 Bed Detection
As input for the Bed Detection Processor the infrared
image is used. At the beginning of the program a
Fast Detection Processor is started, which uses ev-
ery given image. The information will be sent to
a trained YOLOv5S (Jocher et al., 2020) network
which therefore returns a rectangle and a hypothe-
sis. The YOLOv5S is the smallest network within
the YOLO architecture and consists of 7.3m param-
eters with a speed of 2ms per image on a V100 GPU.
The smallest network was chosen because of hard-
ware restrictions by the robot and the fastest speed
for any picture to be calculated by the neural net-
work. An additional training with each possible ar-
chitecture was implemented but showed that no sig-
nificant improvement could be achieved by using any
bigger YOLO network. The network was trained on
a custom dataset composed of infrared data acquired
within the experimentation environment and consists
of 420 images of beds with different obstructions and
from different angles. This dataset includes patients
lying in a bed in different positions. Due to these im-
ages and their privacy protection the dataset unfortu-
nately cannot be released to the public (see Figure 5
for an impression of the dataset). The neural network
pretrained on the COCO data set was used for fur-
ther training, and within 300 episodes a mean average
precision of 95% was reached. For the further train-
ing the above mentioned dataset was used, with the
included mnemonic data set.
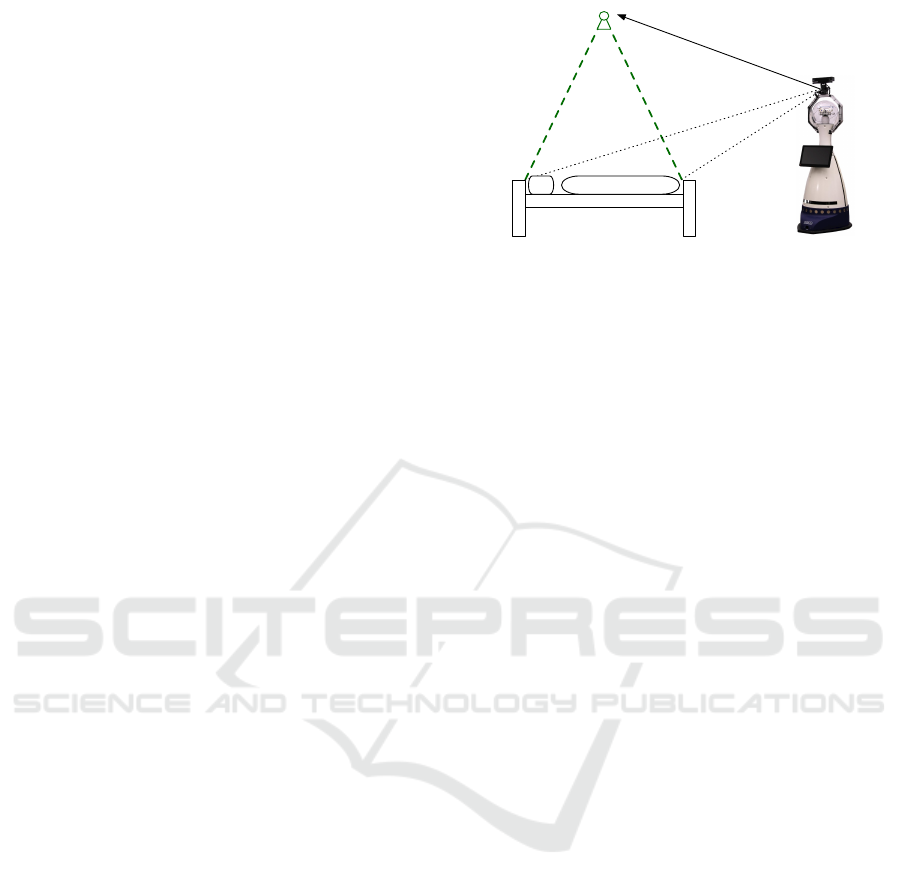
Figure 3: The robot is placed at the bottom of the patient’s
feet, so that it has a full view of the bed and the patient itself.
The angle of aperture of the Kinect One has a wider view
so that more than just the bed can be seen.
If in two succeeding frames a bed was found and
the differences between the outliers of them are within
a certain margin, the Fast Detection Processor (de-
picted in Figure 2) is switched to the Update Detec-
tion Processor. The Update Detection Processor will
not be toggled by every image of the Kinect One but
uses one image every 5 minutes to update the detected
bed if needed. If the newly detected bed is outside
the margin surrounding the original bed detection, the
frame will be updated and then a switch to the Fast
Detection Processor will be executed. The output of
the Bed Detection Processor consists of two objects,
one being the found quadrangle for the bed with the
highest certainty and one being a value if the quadran-
gle was changed in this time-step. This dual proces-
sor design is due to the limited capacities of the CPU
of the robot itself as it does not have any GPU. The
BIOSIGNALS 2022 - 15th International Conference on Bio-inspired Systems and Signal Processing
186
load on the CPU should be kept low, as it produces
less heat and therefore fan noise and could disturb the
patients sleep. The face hypothesis is used to decide
where the patient is lying. In the current experimental
design the robot was placed at the feet of the patient
- see Figure 3 - and therefore the face hypothesis was
not needed to decide how the patient is lying in bed.
In any other context, the robot can move by itself to
achieve a good position for the observation and there-
fore has to decide where the patient is lying.
2.3 Image Separation
The inputs for the Image Separation Processor are the
outputs of the previous Bed Detection Processor:
• Quadrangle of the bed
• Whether or not the quadrangle has changed
• Depth data as a matrix of distance values (float
image)
• Face detection hypothesis from the Kinect One
At first the bed detection will be updated if needed
and the quadrangle of the bed detection, depth data,
and face detection hypothesis are sent to the FloatIm-
ageTo3DDataConverter. The data converter uses the
given depth data image, filters the image according to
the detected quadrangle and transforms it to a birds-
eye-view. The position for the virtual birds-eye-view
camera is in the middle of the detected quadrangle.
The equations for the birds-eye-view transformation
are:
ˆn = (n
1
,n
2
,n
3
)
T
(1)
~x =
depth
−depth ∗ azimuthTangent
depth ∗ elevationTangent
(2)
M~x = M ·~x
= ˆn( ˆn ·~x) + cos(α)( ˆx × ˆn + sin(α)( ˆn ×~x)
(3)
For each point of the point cloud, ˆn is the vector to the
point in the current basis, α is the rotation, M is the
rotation matrix and depth is the length of the vector
of the current point. The values for the azimuth and
elevation tangents are derived from the Kinect One
itself. As result a point cloud is generated with a view
from above the bed and enables the robot to determine
the possible elevation and movement of the patient.
The birds-eye-view of the detected quadrangle
will be sent to the People Divider Processor. The pur-
pose of this processor is to divide the bed into several
parts matching the limbs of the patient lying in it. For
this, two different ways are included. The movement
of the head has little to no effect on the movement if
the patient wants to stand up or slide out of bed. So,
Figure 4: A virtual birds-eye-view camera will be calcu-
lated, which enables a better overview and easier gathering
of information for the movement detection.
if a face detection hypothesis from the Kinect One
is provided within the quadrangle containing the bed,
then the image is cut to the lowest point of the de-
tected face as upper line for the detected bed. The
resulting image is then split into half, resulting in an
upper and a lower body image of the patient. Both im-
ages are set as output for the Image Separation Pro-
cessor. Using both the upper and the lower body as
separate images results in the opportunity to calcu-
late clusters in each of the images clusters at the same
time, thus reducing the calculation time and resulting
in multiple clusters in both of them.
2.4 Movement Detection
The Body Part Clustering Processor uses both images
and a k-nearest-neighbor algorithm (KNN) to cluster
the given information in each image. For this part,
two lists of images will be stored, one for the upper
body and one for the lower body. Both lists will con-
tain a history of 100 images. At every time-step an
image (either the upper or the lower body image) is
added to their list, so that the list contains 100 consec-
utive images. These lists have their own KNN worker
that tries to find three clusters within this timeframe.
The clusters are specified by µ and Σ, where µ rep-
resents the mean of the cluster and Σ the covariance
matrix. To find a moving cluster between the different
timeframes, the Mahalanobis distance is used. Both
timeframes of images are now represented in their list
of clusters.
The lists of clusters will be used in the Movement
Detection Processor, which analyzes the given move-
ments and decides whether a warning should be sent.
If one or more clusters in either list exceeds a thresh-
old, a warning signal is emitted. If a warning is sig-
naled to the backend, the current infrared stream is
displayed at the device for the medical staff and they
have the opportunity to either dismiss the current sit-
uation as a false positive or react accordingly to save
RoSe: Robot Sentinel as an Alternative for Medicinal or Physical Fixation and for Human Sitting Vigils
187
the patient from harm. As devices for the medical
staff a tablet, which will be positioned in the nurses
room and can therefore only be used by them, and a
smartphone is supplied, which can be carried on ward
rounds. If a false positive is signaled, the information
will be send back to the backend and the Movement
Detection Processor will get the notice to change the
threshold to a higher amount. The threshold for move-
ment detection is lowered over time if no movement is
detected. This option is needed as not every patients
movements are the same and some patients tend to
sleep still while others have a more active sleep.
2.5 Constraints
Figure 5: Example for a situation that could not be reli-
ably analyzed because most of the body is hidden behind
the legs. In this situation the patient was not able to move
the legs and slept with them standing up. Therefore neither
a possible moving upper body could be seen nor would the
lower body move.
The constraints of the proposed approach are for a
typical set of movements and are not sensitive enough
for a more diverse set of movements for either dis-
abled patients or patients with a neurological pain
treatment. The movement set for a patient with neu-
rological treatment can be flatten out by medicine
and would undergo the threshold that is currently set.
A possibility would be that with the decline of the
threshold over time a recognition is possible, but fur-
ther research in such direction is needed to verify this
proposition. Also a change of bed linen to a thicker
one could introduce some errors as the movement
seen through the linen can be obstructed and flatten
out.
An unobstructed view of the bed is needed for the
proposed approach to work (see Figure 5) and the bed
should stand in front of the robot.
3 EXPERIMENTS
3.1 Setup
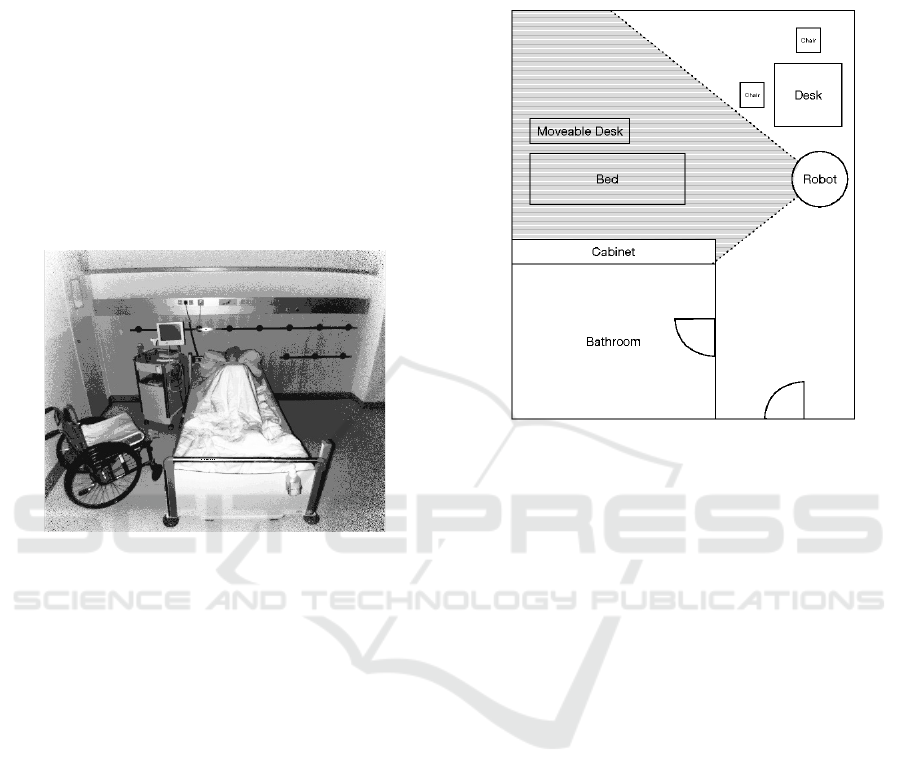
Figure 6: The patients room with the field of vision (striped
gray area) of the robot. The robot is positioned to see the
bed with some margin around it, but leave several blind
spots in the room for the patient. While the robot is visible
from every angle of the room the patient is not monitored in
every angle.
The patients are lying alone in the room, where the
sessions are recorded. At each session the robot will
be placed at the bottom of the patient’s feet facing him
- depicted in Figure 3. To ensure the goal of monitor-
ing the patient and keep her or him within the field of
view, the camera setting is facing the bed so that the
angle of aperture of the Kinect One aligns with a mar-
gin to it (Figure 6). There is also a gap between the
bed and the robot so that the medical staff or the pa-
tient itself can go safely in front of the robot without
the risk of tripping or falling over any cable. To en-
sure operation over a period of eight to twelve hours,
the robot is attached to a power outlet, and to not fur-
ther disturb the patient the cable will be attached at the
start of the session. The robot is placed in the room
at dinner so that the patient has the opportunity to ask
questions about the robot or the recording session and
to familiarize her/himself with the robot. The record-
ing session will start at the signal of the patient when
nighttime arrives. Therefore the amount of video data
is reduced to the needed timespan and the privacy of
the patient can be extended as long as she or he needs.
For the recording only the Kinect One is active and
the robot will not move at all. That ensures an undis-
turbed sleep and minimizes the noise that is emitted
BIOSIGNALS 2022 - 15th International Conference on Bio-inspired Systems and Signal Processing
188

by the robot. The proposed approach can also be used
as an all-day monitoring system if needed, but was
currently only tested at night.
3.2 Execution
The chosen hyperparameter configuration for the
YOLOv5S network utilized for the bed detection in
the infrared image is listed in Table 1. This set of hy-
perparameters was automatically determined and op-
timized by utilizing the evolutionary algorithm pro-
vided by the YOLOv5 framework.
All executions of the experiments were done in
two separate instances with the resulting of five nights
being recorded. Each recorded session is in median
eight hours and eleven minutes long, with the mini-
mum value of six hours and forty minutes and max-
imum value of nine hours and fifteen minutes. Each
of the recordings were seen by the authors and each
movement was labeled. The possible labels were:
• sleeping still
• fall asleep phase
• unsettled sleep
• bathroom visit
• wakeup phase
These phases were chosen according to the different
characteristics the robot has to chose from. The stan-
dard case would be sleeping still, where no movement
could be seen and the patient is sleeping. While the
patient is either falling asleep or is in a wakeup phase,
the robot has to be at the utmost surveillance mode as
in these phases the patient tends to move the most and
has as such the highest possibility to fall out of bed. If
the patient is in an unsettled sleep she or he can move
but most likely will not fall out of bed, because the
movements tend to switch the sleeping position. As
for the last possible phase, the patient would be out
of bed and the robot has a phase where it does not al-
ter the threshold at all. In this phase the robot should
only emit an emergency signal if the patient is lying
on the floor, but this case was not observed in both
experimental phases.
Each possible phase had a margin of maximum of
five minutes to include possible not detected move-
ments. For the training the first label - sleeping still -
was removed, as it does not contain any information
for the robot to learn and for the other labels a mar-
gin was included, so that a no movement phase is in
them also included. This resulted in training data of
sixteen hours and fifteen minutes with a typical length
of about twenty to thirty minutes for each patient (de-
picted in Table 2). In this dataset several bathroom
visits could be recorded but luckily no falling inci-
dents were recorded.
In the first experimental phase, three patients (1-3)
could be recorded with a moderate set of movements,
which resulted in a basic set of information. The
second phase had two patients (4 & 5) with a more
unique set of movements including disability in the
lower limbs and a neurological pain treatment. Both
of these patients resulted in constraints for the algo-
rithm which are described in Section 2.5.
4 EVALUATION
The recorded data are analyzed in Table 2 and are
showing that a significant amount of data could be
logged. The experimental phases showed that the
amount of bathroom visits increased with the age of
the patients and that the patient with the neurologi-
cal treatment had the most unsettled sleep. It also
shows that the patients tend to sleep about 8 hours
and were up before breakfast was served. Both visits
at night resulted in unsettling sleeps for the patients,
with number 1 and 2 not being asleep when the first
visit had come. In most cases just a quick checkup on
the patient had been done, but in some cases a medical
treatment had to be given, which resulted in a longer
phase in which the patient was awake and tried to get
to sleep again. The mean time per scene tended to be
around 30 to 35 minutes, which included about 20 to
25 minutes off the to be recorded movements due to
keep the uprising and the laying down phase within
the record. This shows that in most cases the pa-
tients will have some troubled sleep before rising up
and/or a bathroom visit. Therefore, for the standard
visits without the need of the patient waking up, a vir-
tual visit by the robot would significantly increase the
sleep quality overall.
As no falling incident should happen under the
supervision of the robot, we concentrated on recog-
nizing the uprising movements. In most cases, if the
patient wants to stand up the movement of the lower
body part indicates a sliding process towards either
side of the bed. It is then followed by the upper body
sitting up and therefore creating a movement cluster,
or in one case by tuck up one’s leg. If the patient
has an unsettled sleep the movement of the lower and
upper body part could indicate a change of sleeping
position. In these cases, the upper body will not move
upward but a shoulder is raised if a sidewise sleeping
position is reached. In either case the movement pro-
cess is smaller and happens over a longer period of
time, which results in a smaller covariance matrix Σ
in the clusters. Both movement possibilities are rec-
RoSe: Robot Sentinel as an Alternative for Medicinal or Physical Fixation and for Human Sitting Vigils
189
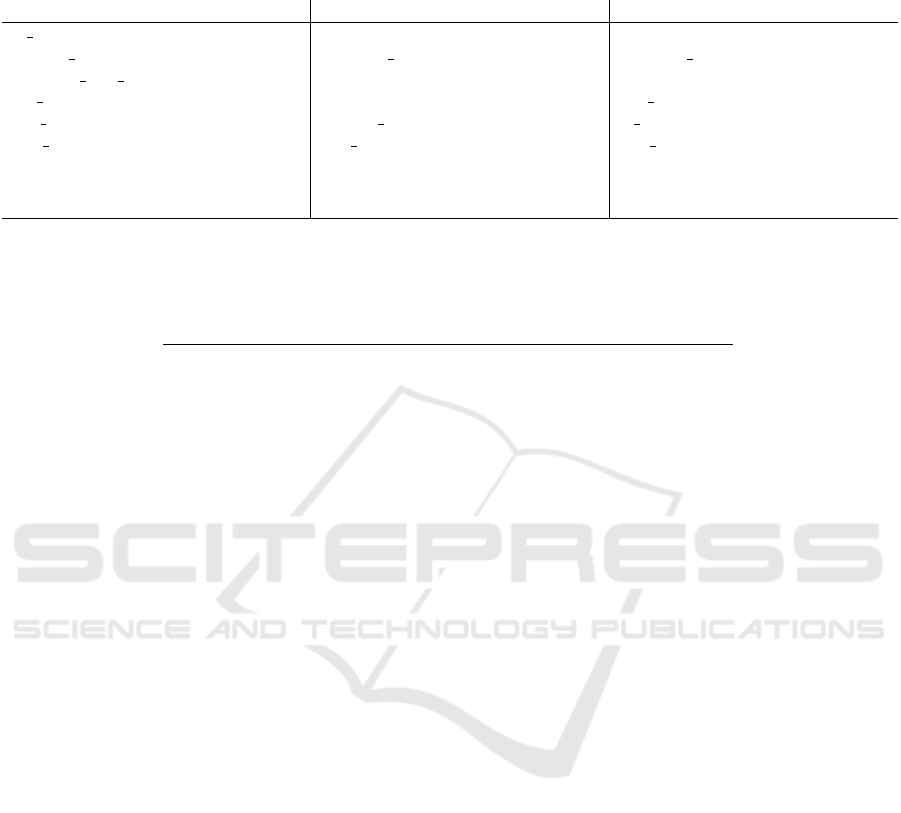
Table 1: Hyperparameter configuration for the bed detection. The listed parameters were automatically optimized by utilizing
the evolutionary algorithm provided by the YOLOv5 framework. A default YOLOv5S network was configured with these
values.
param value param value param value
lr 0 0.00855 lrf 0.193 momentum 0.88
weight decay 0.00049 warmup epochs 4.51 warmup momentum 0.95
warmup bias lr 0.193 box 0.0541 cls 0.386
cls pw 0.974 obj 2.23 obj pw 1.42
iou t 0.2 anchor t 5.1 fl gamma 0.0
hsv h 0.00888 hsv s 0.727 hsv v 0.454
degrees 0.0 translate 0.056 scale 0.604
shear 0.0 perspective 0.0 flipud 0.0
fliplr 0.5 mosaic 0.919 mixup 0.0
Table 2: All scenes that were labeled with the exception of fall asleep and wakeup, because there were for each patient just
one scene. For mean time per scene the data given are in minutes and total time asleep are given in hours.
patient # scenes # unsettled # bathroom mean time total
total sleep visit per scene time
asleep
1 4 1 1 35 6:40
2 4 1 1 40 9:15
3 6 3 1 32,5 8:00
4 9 4 3 24 8:40
5 9 5 2 27 8:20
ognized by the Movement Detection Processor using
the amount of found clusters and their mean µ and
covariance matrix Σ. If either part reaches a certain
threshold a warning is indicated. The threshold can
be adjusted if a warning was called and dismissed by
the medical staff. In this case, the threshold would be
moderately increased.
With the proposed approach we were able to rec-
ognize the anticipated greater movements prior to
the uprising of the patient for their bathroom visit
and smaller movements which indicated an unsettled
sleep. Due to finetuning, which had to be done for
each patient, a threshold between both of these states
could be established. On the second experiment one
edge case was introduced that could not yet be reli-
ably detected. The edge case consists of a patient who
is paralyzed downwards from the hip (see Figure 5).
Furthermore, we gathered data on unsettled sleep in-
duced by neurological pain.
Additionally, differences in the amount of time
taken for a patient to sit up or slide to the side of the
bed could be observed. Despite those differences, in
every case, at least as the patient rises, an unsettled
sleep was detected. According to the proposed ap-
proach the video-stream would have been established
while the patient rises. In this time the medical staff
can intervene through the robot by either speaking
with the patient or playing soothing music and prob-
ably slowing down the process of standing up. This
would give the medical staff some time to intervene
personally if needed.
After each experimental phase information from
each site were gathered. This included the medical
staff - in this case, nurses and doctors - and the pa-
tients. As mentioned in Figure 1, the robot has a
LED strip at its head, which was only dimmable to
low emission mode but could not be turned off, and in
some cases, the fans of the robot could be heard. This
was not a point to end the recording - which was at
every point of the night possible - but was only men-
tioned in the talk at the morning. Each patient that
mentioned either point of the above, identified it as a
minor nuisance. To further reduce the fan speed of
the computer, the amount of the clusters to be found
by the KNN was reduced to three. It was empiri-
cally identified to be the sweet spot between noise and
recognition.
The amount of images saved in the list for the
Body Part Clustering Processor was also empirically
identified to be 100, as to be in the middle of time
taken to calculate the KNN and emitted noise by the
fans.
5 CONCLUSION AND OUTLOOK
We have generated a database, which could not
be found prior, containing different sleeping data,
recorded in IR images and labelled different sleeping
phases of several patients. In return the robot was able
to successfully detect different sleeping phases and
could monitor the patient, if she or he has an unsettled
BIOSIGNALS 2022 - 15th International Conference on Bio-inspired Systems and Signal Processing
190

sleep or a wakeup phase was reached. With these cal-
culated information the robot is able to warn the med-
ical staff prior or while the intention of standing up
arises and can intervene in a situation that can be pos-
sibly harmful for the patient. The robot is especially
useful as it is an embodied interaction partner and can
therefore be easily recognized as the one currently
speaking to the patient, opposing a solely camera-
based approach with attached speakers. The mobility
of the robot will come in handy, as to broaden the ser-
vice in observing multiple patients at once in a multi-
bed room with a single device. Additionally, the robot
can also be used at daytime as enhancement and as-
sistance in the context of MAKS therapy in hospital
wards, proposed in (Bahrmann et al., 2020).
A succeeding study will research on how the
Robot Sentinel performs and how the patients react
when the robot directly intervenes, if a possibly harm-
ful situation is discovered. This includes a direct
intervention triggered by the medical staff or auto-
matically playing music to soothe the patient back
to sleep. For this situation, the medical staff will be
handed a tablet or smartphone with an application that
displays the current situation and emits an alarm. The
staff will have the possibility to dismiss the current
situation, which will be recorded for further adjust-
ment of the algorithm, monitoring the current situa-
tion.
As it could be seen in the second experimental
phase, a possible detection of pain even while sleep-
ing, is a possibility for the proposed approach and
could serve as an early-warning system for the medi-
cal staff to intervene prior to the occurrence of an in-
cident. Also the monitoring and recording of atypical
sleeping behaviors can be useful for further diagnos-
tics.
It was seen that the typical sleep circle of about 1.5
hours is an indicator for movements in between each
cycle and was mostly used for a bathroom break. It
could be possible to determine a wider range of vital
signs from the patient to describe the sleep stage that
she or he is currently in. This would also improve the
warning process in a way to differentiate between a
sleeping or an awake person.
ETHICAL STATEMENT
All human studies described have been conducted
with the approval of the responsible Ethics Com-
mittee, in accordance with national law and in ac-
cordance with the Helsinki Declaration of 1975 (as
amended). A declaration of consent has been obtained
from all persons involved.
ACKNOWLEDGEMENT
The presented work was funded by the ’Euro-
pean Regional Development Funds (ERDF)’ (ERDF-
100293747 & ERDF-100346119). The support is
gratefully acknowledged. We also want to thank all
participants of this project that let us monitor them
throughout their nights at the hospital and the med-
ical staff that provided many informations to further
improve the approach for the hospital use.
REFERENCES
Bahrmann, F., Vogt, S., Wasic, C., Graessel, E., and
Boehme, H.-J. (2020). Towards an all-day assign-
ment of a mobile service robot for elderly care homes.
American Journal of Nursing, 9(5):324–332.
Bauer, P., Kramer, J. B., Rush, B., and Sabalka, L. (2017).
Modeling bed exit likelihood in a camera-based auto-
mated video monitoring application. In 2017 IEEE In-
ternational Conference on Electro Information Tech-
nology (EIT), pages 056–061.
Chang, W.-J., Chen, L.-B., Ou, Y.-K., See, A. R., and Yang,
T.-C. (2021). A bed-exit and bedside fall warning
system based on deep learning edge computing tech-
niques. In 2021 IEEE 3rd Global Conference on Life
Sciences and Technologies (LifeTech), pages 142–143.
Jocher, G., Stoken, A., Borovec, J., NanoCode012, Christo-
pherSTAN, Changyu, L., and et. al. (2020). ultralyt-
ics/yolov5: v3.0.
Kr
¨
uger, C., Mayer, H., Haastert, B., and Meyer, G. (2013).
Use of physical restraints in acute hospitals in ger-
many: a multi-centre cross-sectional study. Interna-
tional Journal of Nursing Studies, 50(12):1599–1606.
Leber, W.-D. and Vogt, C. (2020). Reformschwerpunkt
pflege: Pflegepersonaluntergrenzen und drg-pflege-
split. In Krankenhaus-Report 2020, pages 111–144.
Springer.
Sonnenburg, A. and Schr
¨
oder, A. (2019). Pflegewirtschaft
in Deutschland: Entwicklung der Pflegebed
¨
urftigkeit
und des Bedarfs an Pflegepersonal bis 2035.
Gesellschaft f
¨
ur Wirtschaftliche Strukturforschung
(GWS) mbH.
Sze, T. W., Leng, C. Y., and Lin, S. K. S. (2012). The
effectiveness of physical restraints in reducing falls
among adults in acute care hospitals and nursing
homes: a systematic review. JBI Evidence Synthesis,
10(5):307–351.
RoSe: Robot Sentinel as an Alternative for Medicinal or Physical Fixation and for Human Sitting Vigils
191
