
Forecasting Thresholds Alarms in Medical Patient Monitors using Time
Series Models
Jonas Chromik
1 a
, Bjarne Pfitzner
1 b
, Nina Ihde
1 c
, Marius Michaelis
1 d
, Denise Schmidt
1 e
,
Sophie Anne Ines Klopfenstein
2 f
, Akira-Sebastian Poncette
2 g
, Felix Balzer
2 h
and Bert Arnrich
1 i
1
Hasso Plattner Institute, University of Potsdam, Germany
2
Charité – Universitätsmedizin Berlin, Berlin, Germany
Keywords:
Patient Monitor Alarm, Medical Alarm, Intensive Care Unit, Vital Parameter, Time Series Forecasting, Alarm
Forecasting, Alarm Fatigue.
Abstract:
Too many alarms are a persistent problem in today’s intensive care medicine leading to alarm desensitisation
and alarm fatigue. This puts patients and staff at risk. We propose a forecasting strategy for threshold alarms
in patient monitors in order to replace alarms that are actionable right now with scheduled tasks in an attempt
to remove the urgency from the situation. Therefore, we employ both statistical and machine learning mod-
els for time series forecasting and apply these models to vital parameter data such as blood pressure, heart
rate, and oxygen saturation. The results are promising, although impaired by low and non-constant sampling
frequencies of the time series data in use. The combination of a GRU model with medium-resampled data
shows the best performance for most types of alarms. However, higher time resolution and constant sampling
frequencies are needed in order to meaningfully evaluate our approach.
1 INTRODUCTION
Alarm fatigue is a persisting problem in today’s in-
tensive care medicine with negative outcomes for pa-
tients and staff (Cvach, 2012). Although the problem
is well understood from a medical point of view, there
is no sufficient technical solution to the alarm fatigue
yet. Among the alarms produced by medical patient
monitors, threshold alarms are of particular interest.
Alarms, in general, are supposed to express acute crit-
ical events that need immediate attention. This is, for
example, the case with arrhythmia alarms. Thresh-
old alarms, however, do not necessarily result from
a
https://orcid.org/0000-0002-5709-4381
b
https://orcid.org/0000-0001-7824-8872
c
https://orcid.org/0000-0001-5776-3322
d
https://orcid.org/0000-0002-6437-7152
e
https://orcid.org/0000-0002-6299-0738
f
https://orcid.org/0000-0002-8470-2258
g
https://orcid.org/0000-0003-4627-7016
h
https://orcid.org/0000-0003-1575-2056
i
https://orcid.org/0000-0001-8380-7667
an acute event but can be the result of a continued
trend as we learned from a contextual inquiry at an
intensive care unit (ICU).
In this paper, we want to forecast the foreseeable
share of threshold alarms in order to transform these
alarms into scheduled tasks, thus removing the ur-
gency of the situation. Rather than having an alarm
that has to be taken care of immediately, we want to
present scheduled tasks to the medical staff. For ex-
ample: "In approximately one hour the blood pressure
of the patient will rise above the high threshold. Dur-
ing the next hour, some member of staff should take
care of this issue." This is especially relevant since the
majority of audible and actionable alarms are thresh-
old alarms (Drew et al., 2014).
Forecasting threshold alarms is done in this work
by means of time series models, such as autoregres-
sive integrated moving average (ARIMA) models and
recurrent neural networks (RNNs). As data source we
chose the MIMIC-III database (Johnson et al., 2016)
since this is – to the best of our knowledge – the only
clinical database containing data on patient monitor
alarms. Our approach is optimised for high speci-
26
Chromik, J., Pfitzner, B., Ihde, N., Michaelis, M., Schmidt, D., Klopfenstein, S., Poncette, A., Balzer, F. and Arnrich, B.
Forecasting Thresholds Alarms in Medical Patient Monitors using Time Series Models.
DOI: 10.5220/0010767300003123
In Proceedings of the 15th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2022) - Volume 5: HEALTHINF, pages 26-34
ISBN: 978-989-758-552-4; ISSN: 2184-4305
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

ficity rather than high sensitivity since we acknowl-
edge that not all threshold alarms are the continuation
of a prolonged trend and hence foreseeable. We want
to avoid exacerbating the problem of alarm fatigue by
false positives of our approach.
The rest of this work is structured as follows: In
section 2 we describe the data and models we use
in this work. In section 3 we present the results we
achieve with our approach. In section 4 we discuss
these results. Finally, in section 5 we conclude our
work.
2 MATERIALS & METHODS
In order to forecast threshold alarms in medical pa-
tient monitors, we need both data on said threshold
alarms and means to forecast the corresponding vi-
tal parameter. As data source, we use the MIMIC-III
clinical database as we describe in section 2.1. As
forecasting methods, we compare a variety of time se-
ries models as we describe in section 2.2.
2.1 Materials
The MIMIC-III database contains 26 tables provid-
ing a wide range of information on the events at the
ICUs of Beth Israel Deaconess Medical Center. For
our use case, however, only the CHARTEVENTS ta-
ble is of interest. This table contains, among others,
measured values and alarm thresholds of a variety of
vital parameters such as heart rate (HR), respiratory
minute volume (MV), non-invasively measured sys-
tolic blood pressure (NBP
s
), respiratory rate (RR),
and peripheral blood oxygen saturation (SpO
2
). For
forecasting, we require time series with sufficiently
high and relatively stable sampling frequencies over
an extended period of time. This is not the case for
all vital parameters. Thus, we chose to use only HR,
NBP
s
, and SpO
2
as these vital parameters satisfy the
aforementioned requirements. Specifically, we are in-
terested in the data items listed in table 1.
2.2 Methods
We want to apply time series forecasting on the vi-
tal parameter data described in section 2.1 in order
to achieve our ultimate goal of forecasting threshold
alarm events. To do this, we require methods for fore-
casting time series. For this work, we decided to em-
ploy two fundamental approaches: statistical models
and machine learning models.
Statistical models aim at forecasting the future of
a time series with only the time series itself as prior
Table 1: Complete list of ITEMIDs in the CHARTEVENTS
table that are relevant for this work.
ITEMID Label
220045 HR
220046 HR Alarm - High
220047 HR Alarm - Low
220179 NBP
s
223751 NBP
s
Alarm - High
223752 NBP
s
Alarm - Low
220277 SpO
2
223769 SpO
2
Alarm - High
223770 SpO
2
Alarm - Low
knowledge. Specifically, we are using the ARIMA
model and its variation additionally featuring exoge-
nous variables (ARIMAX).
Machine learning (ML) models learn from train-
ing data and can then be applied to previously unseen
test data. In our case, we employ RNNs trained with
80% of the available vital parameter time series to
forecast on the remaining 20% of vital parameter time
series. Specifically, we are using vanilla RNNs, gated
recurrent units (GRUs), and long short-term memory
neural networks (LSTMs) because variations of recur-
rent neural networks is what is usually used on time-
series data, e.g. in (Mussumeci and Coelho, 2020),
(Pathan et al., 2020), and (Dai et al., 2021).
We frame the problem as a regression problem,
i.e. forecasting the vital parameter, instead of a clas-
sification problem, i.e. predicting whether an alarm
will occur or not, because we want to keep the ML
approach as close to the ARIMA approach as possi-
ble to ensure comparability. For the same reason, we
also do not provide additional information such as age
or sex to the ML models.
Resampling and Chunking. Both statistical and
machine learning models have in common that they
require constant sampling frequencies which are not
always given in medical databases. We address this
issue by resampling the vital parameter measurement
from the MIMIC-III database to one sample per hour
( f
s
= 1 h
−1
) which is close to the database’s original
sampling frequency present in most cases.
For resampling, we employ three different strate-
gies in order to fuse samples together: Minimum re-
sampling, maximum resampling, and median resam-
pling. Thus, we create three distinct but related time
series which can be used for forecasting.
Furthermore, we use a chunking strategy. We no-
ticed that there are gaps in the time series, i.e. ex-
tended periods of time where there are no data points.
We assume, that this is due to the patient being in
a different ward, surgery, or some other procedure.
Forecasting Thresholds Alarms in Medical Patient Monitors using Time Series Models
27

These missing data pose a difficulty for resampling.
Hence, we subdivide the data of a patient’s ICU stay
along the data gaps into multiple chunks and operate
only on these chunks throughout the rest of our work.
By subdividing the patients’ data into chunks and
treating these chunks as distinct time series, we cir-
cumvent a missing data issue. In practice, this im-
plies that whenever a period of missing data arises, the
model has to re-learn and cannot build upon the data
from the prior chunk. Nevertheless, we reason that
this approach makes sense because we cannot know
what happened in the period of missing data. For ex-
ample, when the period of missing data was caused by
a surgical procedure, the patient might be in a com-
pletely different condition after the surgery than be-
fore. Consequently having a completely different vi-
tal parameter distribution that can not be associated
with the period before the surgery.
Experiment Setup. Regardless of whether the
model in use is a statistical model or a ML model,
we always employ the same experiment setup: We
use 12 or 30 timesteps (lags) equivalent to 12 or 30
hours of vital parameter data as input for the model.
We chose these specific periods because we wanted to
compare performances for a rather short and a rather
long observation. The 12 hours period primarily aims
at providing clinicians with alarm forecasts in a timely
manner. With this approach, forecasts are provided
after the patient spent half a day at the ICU. In con-
trast, the 30 hours time frame aims at sufficiently
spanning a complete cycle of the circadian rhythm
hence giving a more holistic picture of the patient’s
vital parameter distribution.
The model produces a forecasted value for the
hour following the input lags. We compare the fore-
casted value to the currently active high or low alarm
threshold. If the value is above the high threshold or
below the low threshold, a respective threshold alarm
is forecasted. Otherwise, no alarm is forecasted. Sub-
sequently, we compare the forecast with the actual
situation, i.e. whether there was actually a threshold
alarm triggered by the actual vital parameter measure-
ment.
This common approach is used for all models
we evaluated. However, details differ since there
are conceptual differences between the models. The
most striking one is that ML models require dedicated
training data while statistical models learn only on the
given input sequence. Hence, we describe the con-
crete experiment setups for specific models in the fol-
lowing.
Statistical Models. We use both ARIMA and ARI-
MAX models as can be seen in Table 2. The ARIMA
models are used with the median and minimum or
maximum resampled time series. For ARIMAX we
use the maximum resampled time series for fore-
casting high threshold alarms and the minimum re-
sampled time series for forecasting the low threshold
alarms. For both ARIMAX cases, the median resam-
pled time series is used as exogenous series. All three
described model setups are processed with a train size
of 12 lags or 30 lags, respectively, which determines
the minimum length of chunks required.
Table 2: Complete list of IDs for ARIMA and ARIMAX
models.
Model ID Train Size Model Type Endog.
A_01_12 12 ARIMA Median
A_02_12 12 ARIMA Min/Max
A_03_12 12 ARIMAX Min/Max
A_01_30 30 ARIMA Median
A_02_30 30 ARIMA Min/Max
A_03_30 30 ARIMAX Min/Max
Machine Learning Models. Here, we also com-
bine different models with different resampling strate-
gies. As model types we chose vanilla RNNs, GRUs,
and LSTMs. As with statistical models, we have one
setup that is equivalent to the ARIMA setup where
we train and forecast only with the median resampled
time series. In another setup which is equivalent to
the ARIMAX approach, we use the maximum resam-
pled time series for forecasting high threshold alarms
and the minimum resampled time series for forecast-
ing the low threshold alarms and in both cases the me-
dian resampled time series as exogenous series.
To make a prediction for each chunk, we introduce
a windowing technique that uses 80% of the data of
the respective vital parameter for training and 20%
for predicting per window. Thus, a total of five differ-
ent windows are considered, each predicting different
20% of the chunks ensuring that no previously seen
data is used. The entire chunk length is employed
for training. The prediction on the pre-trained model
starts after 12 timesteps, as already described above.
We have chosen this "waiting period" in order to bet-
ter compare the results with those of the ARIMA(X)
approach and because a prediction after 12 data points
is in practice more crucial than after 30 data points.
As shown in Table 3, each model type is run not
only with and without exogenous input, but also with
non-scaled (suffix "n"), standard scaled (suffix "s1")
and min-max scaled (suffix "s2") time series.
Equation 1 shows how standard scaling is applied
on a series value x. It removes the mean and scales
HEALTHINF 2022 - 15th International Conference on Health Informatics
28

Table 3: Complete list of IDs for ML models. Standard
scaling is indicated by suffix "s1" and min-max scaling by
suffix "s2". If no scaling is performed, suffix is "n" for "non-
scaled".
Model ID Scaling Model Type Endog.
LS_01_s1 Standard LSTM Median
LS_02_s1 Standard LSTM Min/Max
GR_01_s1 Standard GRU Median
GR_02_s1 Standard GRU Min/Max
RN_01_s1 Standard RNN Median
RN_02_s1 Standard RNN Min/Max
LS_01_s2 Min-Max LSTM Median
LS_02_s2 Min-Max LSTM Min/Max
GR_01_s2 Min-Max GRU Median
GR_02_s2 Min-Max GRU Min/Max
RN_01_s2 Min-Max RNN Median
RN_02_s2 Min-Max RNN Min/Max
LS_01_n None LSTM Median
LS_02_n None LSTM Min/Max
GR_01_n None GRU Median
GR_02_n None GRU Min/Max
RN_01_n None RNN Median
RN_02_n None RNN Min/Max
x
scaled
=
x − µ
σ
(1)
1: Transformation of series value x to scaled series value
x
scaled
using standard scaling (referred to as s1). The
same mean µ and standard deviation σ is used for all train
series and all prediction series.
the values to unit variance. We performed this scaling
method globally, meaning all train and all prediction
time series are transformed with the same mean µ and
same standard deviation σ. This ensures that equal x
values are transformed to equal x
scaled
values across
all available time series.
x
scaled
=
x − min
max − min
(2)
2: Transformation of series value x to scaled series value
x
scaled
using min-max scaling (referred to as s2). min and
max are the minimum and maximum of the available data
values. This transformation is performed individually for
each series resulting in a 0-1 value range.
In contrast to the first scaling method, min-max
scaling transforms each value to a given min-max
range. In addition, we performed this transformation
with each time series individually and not globally.
Equation 2 shows how we applied it to our data re-
sulting in a 0-1 value range.
Evaluation. To evaluate the performance of the dif-
ferent models, we employ an adapted version of the
evaluation formula used in (Clifford et al., 2015).
There, the goal was to evaluate models for identify-
ing false cardiac arrhythmia alarms. We adapted the
formula to ignore true negatives and flipped the roles
of false positives and false negatives to account for
the inverse scenario we are facing in this paper. The
evaluation formula is shown in eq. (3).
Evaluation Score =
T P
T P + FN + 5 · FP
(3)
3: Evaluation score formula, adapted from (Clifford et al.,
2015).
True positives, present in the numerator and the
denominator, represent alarms that are correctly fore-
cast, i.e. the forecasting model predicts an alarm and
the alarm is in fact present.
False positives denote situations where the model
predicts an alarm but there is in fact none. False
positives are penalised with a factor of five because
we want to avoid increasing the alarm load since this
would be opposed to our goal of alleviating alarm fa-
tigue.
False negatives, on the other hand, are situations
where the model predicts no alarm to occur but there
is in fact an alarm in the respective period of time.
False negatives are less problematic since we ac-
knowledge that changes in vital parameter measure-
ments can happen abruptly and unforeseeably due to
external factors that are not recorded in the data set.
False negative, in this case, does not mean that the
alarm itself is suppressed but rather that the model
did not forecast the alarm. Consequently, the alarm
stays an indicator for an acute event that needs urgent
action rather than being transformed to a scheduled
task.
3 RESULTS
In this section, we show and compare the perfor-
mances of the employed models in terms of our eval-
uation metric. We first show the performances of the
statistical models. Then, we show the performances
of the ML models. Finally, we compare the best per-
forming models from both categories amongst each
other.
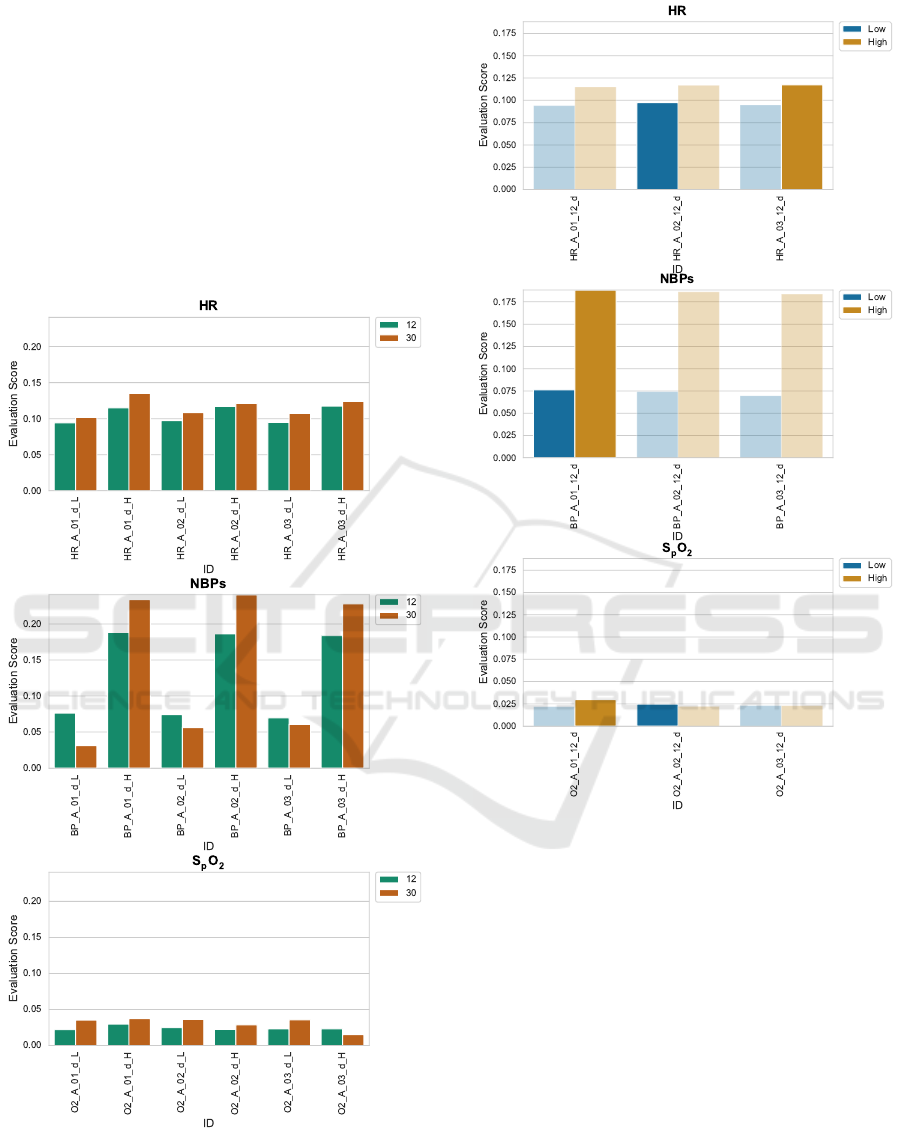
Statistical Models. Figure 1 shows a performance
comparison for all statistical models and all parame-
ters with respect to the train size. We compare train-
ing with 12 lags against training with 30 lags. We em-
ploy a constant sampling frequency of f
s
= 1 h
−1
be-
cause MIMIC-III does not allow for higher f
s
. Hence,
Forecasting Thresholds Alarms in Medical Patient Monitors using Time Series Models
29
12 lags are equivalent to 12 hours of ICU stay and 30
lags are equivalent to 30 hours of ICU stay, respec-
tively. Since there are fewer ICU stays lasting up to
30 hours than ICU stays lasting up to 12 hours, there
are consequently fewer ICU stays to be considered for
the 30 lags train size approach.
Figure 2 compares the statistical models’ perfor-
mance for high alarms against the performance for
low alarms and across the different vital parameters.
There are striking performance differences amongst
parameters and alarm types which will be further dis-
cussed in section 4.
Figure 1: Comparison of train sizes for statistical models
(ARIMA and ARIMAX). For all parameters and model we
compare a train size of 12 lags with a train size of 30 lags
both for high alarms (suffix _H) and low alarms (suffix _L).
Figure 2: Comparison of alarm types (high alarm and low
alarm) for statistical models across all vital parameters.
ML Models. Figure 3 shows a comparison of the
different ML model types, i.e. vanilla RNN, LSTM,
and GRU. The plots show no clear superiority of
one model type. However, the plots suggest that in-
put variables, alarm type, and especially the scal-
ing methods distinctly influence the models’ perfor-
mance. Hence, we further explore the influence of the
scaling method in fig. 4. In this figure, two facts are
to be seen. Firstly, scaling seems to have a distinctly
negative influence on the model’s performance. This
is most obvious for the SpO
2
vital parameter but the
effect is also present for HR and NBP
s
. Secondly,
the type of alarm (high alarm or low alarm) appears
to also have an influence on the ML models’ perfor-
mances but differently than in the statistical models’
HEALTHINF 2022 - 15th International Conference on Health Informatics
30
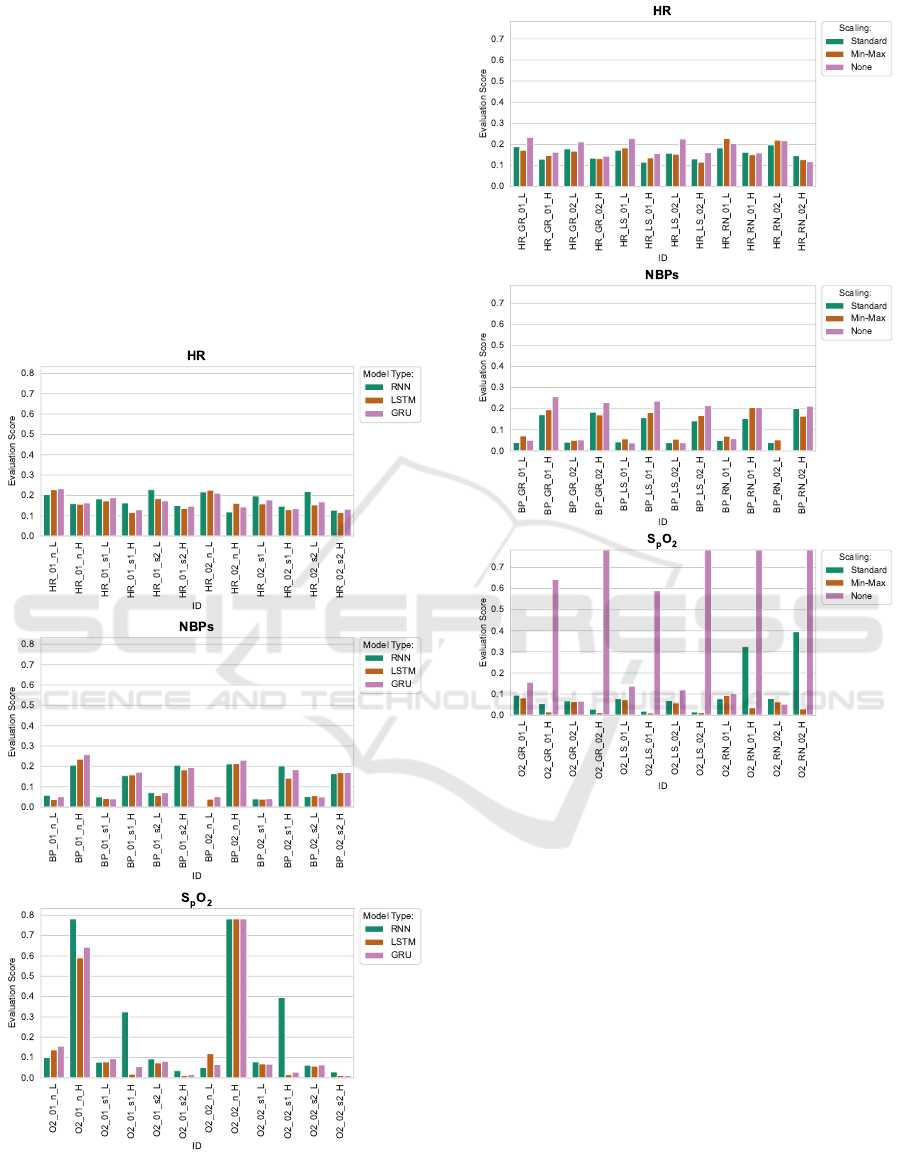
case. For HR, low alarms seem to be forecast slightly
more successfully. For NBP
s
, high alarms seem to be
forecast distinctly more successfully. For SpO
2
the
influence of the scaling method is too high to clearly
see an effect here.
Figure 5 shows an overall comparison of all ML
models and highlights the best performing model for
each combination of vital parameter and alarm type.
For HR and NBP
s
there is one clear best model con-
figuration for each alarm type. For SpO
2
, however,
there are multiple best models for the high alarm type.
In general, the GRU model with median resampling
shows the overall best performance according to this
figure.
Figure 3: Comparison of ML model types vanilla RNN,
LSTM and GRU with different configurations across vital
parameters and alarm types (suffix _H for high alarms and
suffix _L for low alarms).
Figure 4: Comparison of ML models executed with differ-
ent scaling methods applied (Standard, Min-Max) or with-
out scaling (None) across vital parameters and alarm types
(suffix _H for high alarms and suffix _L for low alarms).
Comparison. Figure 6 compares the best perform-
ing statistical and ML models with each other hav-
ing vital parameter and alarm type as independent
variable. Except for low blood pressure alarms, the
ML models always outperform the statistical models,
most strikingly in the SpO
2
case.
To give a more in-depth view into the model per-
formances, fig. 7 visualises the confusion matrix for
the best performing models. There, we can see that
the statistical models most prominently produce more
false positives than the ML models. Since our evalua-
tion metric penalises false positives more heavily than
false negatives, this explains the considerably lower
performance of the statistical models in fig. 6.
Forecasting Thresholds Alarms in Medical Patient Monitors using Time Series Models
31
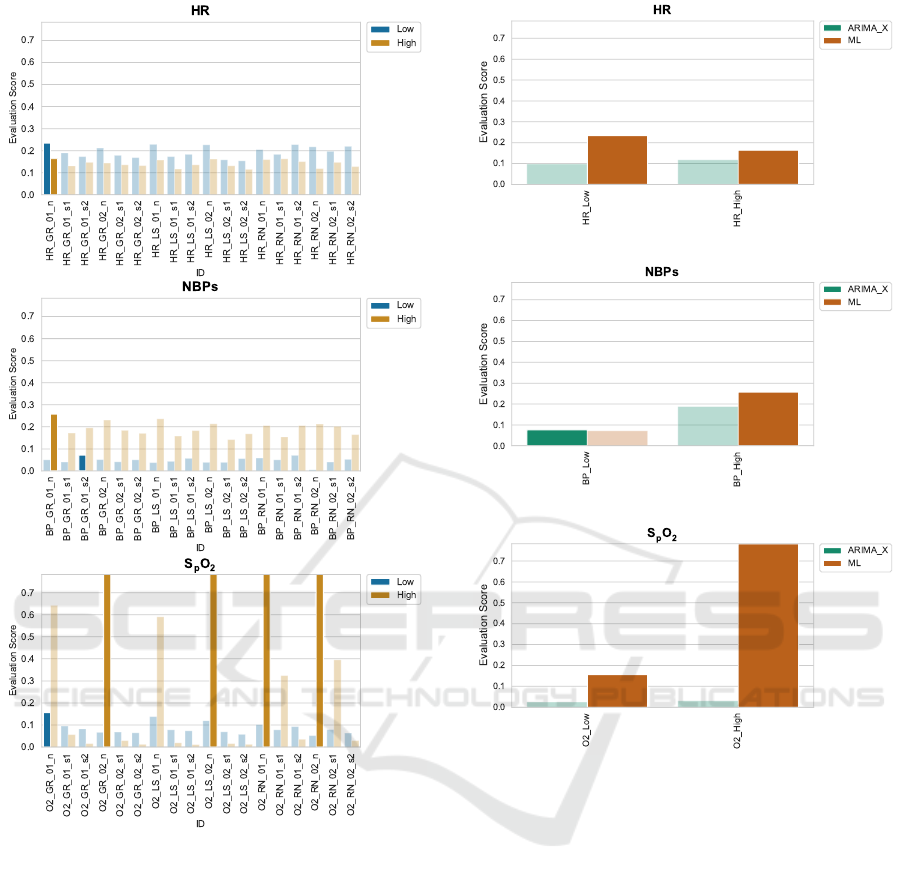
Figure 5: Selection of best ML models. Models with model
type GRU and median resampled chunks as endogenous
input variable always perform best (except for high alarm
forecasting of SpO
2
).
4 DISCUSSION
In this paper, we aimed at forecasting threshold
alarms in patient monitors. Therefore, we used the
vital parameter and alarm data as provided by the
MIMIC-III database and employed a wide variety of
forecasting models ranging from statistical models to
machine learning methods. In general, the overall
forecasting performance is not fully satisfactory re-
gardless of the model in use. However, the results
give important insights that can guide further research
into this area which we discuss in the following.
Figure 6: Comparison of best performing statistical models
to best performing ML models.
Train Sizes. In fig. 1 we compare different ARIMA
and ARIMAX models each of which being evaluated
with a train of 12 lags and with a train size of 30 lags
respectively. As a general finding, longer train sizes
tend to yield better forecasting performance. How-
ever, a longer train size also entails that the patient
needs to stay in the ICU for a longer period of time
before the alarm forecasting model can be used, in
our case 12 hours vs. 30 hours. Another approach
is to raise the time-resolution of the vital parameter
data. With more data points per period of time a larger
train size can be achieved in less time. This mani-
fests future research work and investigations into ICU
databases featuring a higher time resolution, see sec-
tion 4.2.
High and Low Alarms. Figure 2 and fig. 5 show
that model performance vastly differs between high
HEALTHINF 2022 - 15th International Conference on Health Informatics
32
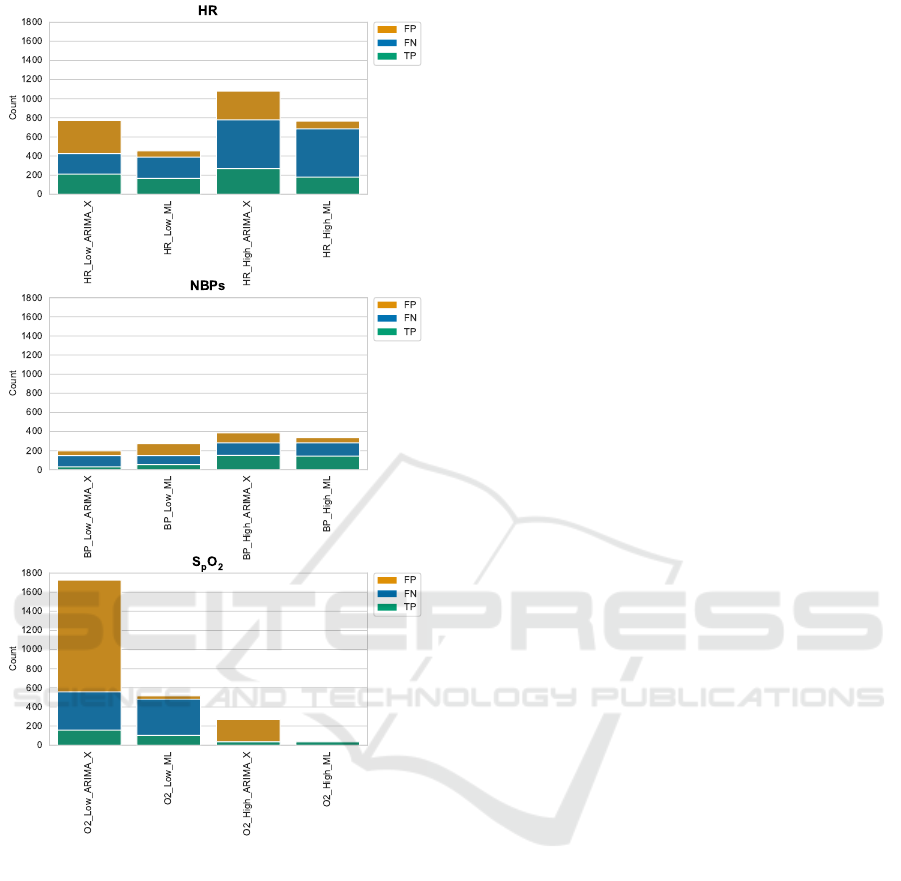
Figure 7: Comparison of confusion matrix values (false
positives, false negatives, and true positives; not showing
true negatives) of best performing statistical models to best
performing ML models.
and low alarms even concerning the same vital pa-
rameter. Especially for HR and NBP
s
, high alarms are
generally forecast with higher performance regarding
the evaluation score we utilise. Furthermore, peak
forecasting performance for high and low threshold
alarms is not necessarily achieved by the same model.
In the cases of HR and SpO
2
forecasting, the peak
evaluation score for high alarms is achieved by a dif-
ferent model than the one achieving peak evaluation
performance for the low alarm. Consequently, high
and low alarms of the same vital parameter have to be
considered nonetheless as distinct forecasting tasks.
There is no universal one-fits-all model for threshold
alarm forecasting.
Effects of Scaling. Scaling does not seem to have
a positive effect on the models’ forecasting perfor-
mance, as is to be seen in fig. 4 and fig. 5. In fact,
models using unscaled data consistently exhibit su-
perior or hardly worse performance than their coun-
terparts that do apply scaling methods. An example
where min-max scaling works better than no scaling is
the prediction of alarms of type low in SpO
2
. We have
no theory on why this is the case. Hence, this man-
ifests a need for further research, ideally in a simpli-
fied forecasting setting (e.g. only forecasting the vital
parameter measurement and no alarms yet) and time
series having a higher and more consistent time reso-
lution, as provided by HiRID and eICU CRD. This is
also described as future work in section 4.2.
Best Performing Models. Figure 6 and fig. 7 show
that amongst the best performing models (both sta-
tistical and ML), the ML models exhibit a superior
performance. This is rooted in the evaluation metric
we utilise that penalises false positives heavier than
false negatives. In fig. 7 it is to be seen that the statis-
tical models tend to produce a higher quantity of false
positives which negatively influences their scoring in
fig. 6, especially for HR and SpO
2
.
4.1 Limitations
In our efforts to forecast threshold alarms in patient
monitors we faced a couple of limitations which we
already mentioned previously and which we want to
summarise here.
Firstly, the relatively low and partially unstable
sampling frequency of the vital parameter measure-
ments poses a problem to our approach. This is two-
fold: On the one hand, the low amount of samples
per period of time forces us to use smaller train sizes
since larger train sizes would correspond to ridicu-
lously long ICU stays. Hence, we have only 12 to
30 lags of training for the statistical models. We as-
sume that this reduces the forecasting performance of
the models since we were able to show that larger
train sizes correspond to better model performance.
On the other hand, the large temporal distance (≈ 1h)
between the samples prevents the forecasting models
from picking up on changes that happen on a more
fine-grained (higher) temporal resolution, potentially
causing false negatives. Higher temporal resolutions
in vital parameter measurements and more detailed
and accurate alarm event data are needed in order to
successfully build accurate alarm forecasting models.
Forecasting Thresholds Alarms in Medical Patient Monitors using Time Series Models
33

Secondly, our work suggests that each alarm type
requires a dedicatedly tuned model and that there is no
one-fits-all model for forecasting all types of alarms.
Hence, a narrower research focus might be required
for example limiting the forecasting task on one type
of alarms using a more detailed or even specialised
data set.
4.2 Future Work
Forecasting threshold alarms in patient monitors is
basically an extension of forecasting vital parameter
measurements by not only forecasting the value itself
but also comparing the value to the alarm thresholds.
We chose the MIMIC-III database because a unique
feature of this database is that it contains alarm thresh-
olds. However, if we accept that forecasting vital pa-
rameter measurements without accounting for alarms
is a valid preliminary goal, other clinical databases are
eligible as well. For example, HiRID (Hyland et al.,
2020) provides vital parameters measurements with a
vastly higher time resolution and eICU CRD (Pollard
et al., 2018) even provides such data with a steady
sampling frequency of f
s
=
1
5 min
(one value every
five minutes). This is in sharp contrast to MIMIC-
III which has varying sampling frequencies leaning
towards one value per hour. Using HiRID and eICU
CRD might improve the forecasting accuracy for vi-
tal parameters and also spare us the resampling step
which introduces an additional source of inaccuracies
and errors. Such a simplified forecasting setting can
then also be used to further investigate the effects of
scaling on the forecasting performance.
5 CONCLUSIONS
The contribution of this paper is a first attempt to
forecasting threshold alarms in ICU patient monitors.
Due to the lack of alarm data having a sufficiently
high and consistent sampling frequency, the resulting
models are still worthy of improvement and are not
yet ready to be applied in clinical practice. However,
our results show that the general approach of forecast-
ing threshold alarms through vital parameters princi-
pally works and that the model setup used in this work
is promising.
ACKNOWLEDGEMENTS
This work was partially carried out within the
INALO project. INALO is a cooperation project be-
tween AICURA medical GmbH, Charité – Univer-
sitätsmedizin Berlin, idalab GmbH, and Hasso Plat-
tner Institute. INALO is funded by the German Fed-
eral Ministry of Education and Research under grant
16SV8559.
REFERENCES
Clifford, G. D., Silva, I., Moody, B., Li, Q., Kella, D.,
Shahin, A., Kooistra, T., Perry, D., and Mark, R. G.
(2015). The physionet/computing in cardiology chal-
lenge 2015: reducing false arrhythmia alarms in the
ICU. In 2015 Computing in Cardiology Conference
(CinC), pages 273–276. IEEE.
Cvach, M. (2012). Monitor alarm fatigue: an integrative
review. Biomedical instrumentation & technology,
46(4):268–277.
Dai, X., Liu, J., and Li, Y. (2021). A recurrent neural net-
work using historical data to predict time series in-
door PM2.5 concentrations for residential buildings.
Indoor Air.
Drew, B. J., Harris, P., Zègre-Hemsey, J. K., Mammone,
T., Schindler, D., Salas-Boni, R., Bai, Y., Tinoco, A.,
Ding, Q., and Hu, X. (2014). Insights into the problem
of alarm fatigue with physiologic monitor devices: a
comprehensive observational study of consecutive in-
tensive care unit patients. PloS one, 9(10):e110274.
Hyland, S. L., Faltys, M., Hüser, M., Lyu, X., Gumbsch, T.,
Esteban, C., Bock, C., Horn, M., Moor, M., Rieck, B.,
et al. (2020). Early prediction of circulatory failure in
the intensive care unit using machine learning. Nature
medicine, 26(3):364–373.
Johnson, A. E. W., Pollard, T. J., Shen, L., Lehman, L.-
W. H., Feng, M., Ghassemi, M., Moody, B., Szolovits,
P., Celi, L. A., and Mark, R. G. (2016). MIMIC-III, a
freely accessible critical care database. Scientific data,
3(1):1–9.
Mussumeci, E. and Coelho, F. C. (2020). Large-scale mul-
tivariate forecasting models for dengue-LSTM versus
random forest regression. Spatial and Spatio-temporal
Epidemiology, 35:100372.
Pathan, R. K., Biswas, M., and Khandaker, M. U. (2020).
Time series prediction of COVID-19 by mutation rate
analysis using recurrent neural network-based LSTM
model. Chaos, Solitons & Fractals, 138:110018.
Pollard, T. J., Johnson, A. E., Raffa, J. D., Celi, L. A.,
Mark, R. G., and Badawi, O. (2018). The eICU col-
laborative research database, a freely available multi-
center database for critical care research. Scientific
data, 5(1):1–13.
HEALTHINF 2022 - 15th International Conference on Health Informatics
34
