
Long-term Cholesterol Risk Prediction using Machine Learning
Techniques in ELSA Database
Nikos Fazakis
a
, Elias Dritsas
b
, Otilia Kocsis
c
, Nikos Fakotakis and Konstantinos Moustakas
d
Department of Electrical and Computer Engineering, University of Patras, 26504 Rion, Greece
{fazakis, okocsis, moustakas}@ece.upatras.gr, dritsase@ceid.upatras.gr, fakotakis@upatras.gr
Keywords:
Cholesterol, Long-term Prediction, Machine Learning.
Abstract:
Cholesterol is a crucial risk factor for cardiovascular diseases (CVDs) which in their turn are among the main
causes of death worldwide and public health concern, with heart diseases being the most prevalent ones. For
cholesterol control, the early prediction is considered one of the most effective ways. Utilizing the English
Longitudinal Study of Ageing (ELSA), a large-scale database of ageing participants, a dataset is derived to
evaluate the long-term cholesterol risk of elderly men and women using Machine Learning (ML) techniques.
Several ML prediction models were assessed concerning Accuracy and Recall where the Logistic model tree
was the best performer. The ultimate goal of this study is to identify individuals at risk and facilitate earlier
intervention to prevent the future development of cholesterol.
1 INTRODUCTION
Cholesterol is a waxy substance found in many of
the consumed foods and also in the body cells.
There are three main types of cholesterol in the body
cells. High-density lipoprotein (HDL), also called the
”good” cholesterol, it helps removing excess choles-
terol from the body. In contrast, Low-density lipopro-
tein (LDL), the bad or “lousy” cholesterol, it can lead
to a buildup of plaque in the arteries. In addition,
Very low-density lipoprotein (VLDL) exists, which
also tends to promote plaque buildup.
Quantifying an individual’s risk for develop-
ing non-contiguous chronic conditions such as high
cholesterol, which are linked to controllable lifestyle
behaviours and attitudes, is an important goal of pre-
diction analysis in healthcare, as it is linked on one
side with the long-term well-being on the individual
and active and independent ageing, and on the other
side with important potential savings for the social
care systems. Recent research has demonstrated that
it is possible to use ML tools to predict individual risk
of hospitalization by only using data related to socioe-
conomic features (age group, gender and race) and be-
havioural data, without requiring clinical risk factors
a
https://orcid.org/0000-0001-7687-2380
b
https://orcid.org/0000-0001-5647-2929
c
https://orcid.org/0000-0001-6937-6442
d
https://orcid.org/0000-0001-7617-227X
(Chen et al., 2020). In this context, the SmartWork
(Kocsis et al., 2019) system has been developed with
the aim to provide the ageing sedentary population
with the right tools in order to promote healthy and
active ageing and improve their workability. During
this process the monitoring of the individual’s health
and the prognosis of several chronic diseases, i.e. high
cholesterol, is considered as a vital step.
Cholesterol levels are tested through blood choles-
terol or lipid tests, and although high levels are
asymptomatic, the relation between the different
forms of cholesterol provides an indication of risks of
developing heart diseases (Group et al., 2000). Thus,
preventing or lowering high cholesterol levels is di-
rectly linked to lowering risks of cardiovascular dis-
eases. The main risk factors (Anagnostis et al., 2015),
(Crouse et al., 1995), (Wakabayashi and Groschner,
2009) potentially impacting on the high cholesterol
levels include:
• Gender: after menopause, a woman’s LDL
cholesterol level usually goes up.
• Age: men aged 45 years or older and women aged
55 years or older are at increased risk of high
cholesterol and heart disease.
• Family history of heart diseases: the risk of
high cholesterol may increase if a father/ brother
was affected by heart disease before age 55 or a
mother/ sister was affected by heart disease before
age 65.
Fazakis, N., Dritsas, E., Kocsis, O., Fakotakis, N. and Moustakas, K.
Long-term Cholesterol Risk Prediction using Machine Learning Techniques in ELSA Database.
DOI: 10.5220/0010727200003063
In Proceedings of the 13th International Joint Conference on Computational Intelligence (IJCCI 2021), pages 445-450
ISBN: 978-989-758-534-0; ISSN: 2184-3236
Copyright © 2023 by SCITEPRESS – Science and Technology Publications, Lda. Under CC license (CC BY-NC-ND 4.0)
445
• Diet: high fat, high sodium, or frequent consump-
tion of food from animal sources (red meat, eggs,
cheese, etc.) increases total and LDL cholesterol
levels.
• Obesity/ High BMI: a BMI higher than 25 is
a high-risk factor for increased LDL cholesterol
levels.
• Physical activity: increased physical activity and
regular exercising helps to lower LDL and raise
HDL cholesterol levels.
• Alcohol: although moderate alcohol intake is
linked to increasing HDL-cholesterol, excessive
alcohol intake may increase LDL-cholesterol and
triglyceride levels.
• Smoking: past or present smoking, or exposure
to tobacco smoke (passive smoking) increases
cholesterol levels.
• Diabetes: persons suffering of diabetes have in-
creased cholesterol levels.
The contribution of this paper is twofold: i) the
engineering of a meaningful dataset that can facilitate
the prognosis of high cholesterol regarding the elder
workers, ii) a comparative assessment of different ML
models families in order to spot the most efficient for
the long-term cholesterol risk prediction of older peo-
ple aged at least 50 years. At this point, it should be
noted that these models will be integrated into the pre-
dictive AI tools of the SmartWork system, which aims
to sustain workability of older office workers (Kocsis
et al., 2019) based on personalized models acquired
from the integration of the health condition of specific
patient models. Cholesterol is one of the chronic con-
ditions that will be considered in SmartWork (Fazakis
et al., 2021).
The rest of this paper is organized as follows. Re-
lated work regarding the prediction of high choles-
terol as chronic disease is discussed in Section 2. In
Section 3 the main parts of the methods for the long-
term risk prediction of cholesterol are displayed. In
particular, the design of a training and testing dataset,
feature selection and the experiments setup are pre-
sented. Section 4 concludes the paper.
2 RELATED WORKS
Many studies have been conducted, in relation to high
cholesterol risk assessment, but in most of the cases
these are directly linked to risk of cardiovascular dis-
eases.
The Framingham Heart Study (Mahmood et al.,
2014) led to the development of LDL Cholesterol
Goal Level Calculator
1
, which is mainly based on de-
mographic and lifestyle variables.
Jian Liu et al (Liu et al., 2005), assess coronary
heart disease (CHD) risk within levels of the joint
distribution of non-HDL and LDL cholesterol among
individuals with and without diabetes. The results
of their study indicated that diabetes condition is a
strong risk factor for coronary heart disease (CHD)
death. Cengiz Colak et al, (Colak et al., 2016) study
was carried out to predict the cholesterol level in pa-
tients with Myocardial Infarction (MI) using Artifi-
cial Neural Networks (ANN) and Support Vector Ma-
chines (SVM) models. The results pointed out that
ANN has higher predictive performance in compari-
son with SVM in predicting cholesterol level. More-
over, the prediction of blood cholesterol levels from
genotype data was studied by Francesco Reggiani et.
al, (Reggiani et al., 2020). In addition, Jin Sol Lee
et al, (Lee et al., 2018) considered the prediction of
cholesterol ratios within a Korean population.
Finally, the most significant risk factors contribut-
ing to the development of high cholesterol, as sug-
gested by the different research works, are summa-
rized in Table 2.
3 LONG-TERM CHOLESTEROL
RISK ASSESSMENT
Although high cholesterol levels are usually asymp-
tomatic, their assessment is important as a risk screen-
ing tool for cardiovascular diseases. In particular, the
ratios
totalcholesterol
HDL
and
LDL
HDL
provide a good indication
of risk of cardiovascular diseases, as shown in Table
1.
Table 1: Cholesterol Levels and Risk of Cardiovascular Dis-
eases.
totalcholesterol
HDL
LDL
HDL
Risk
Male Female Male Female
< 3.4 < 3.3 1 1.5 Low
5.0 4.5 3.6 3.2 Average
9.5 7.0 6.3 5.0 Moderate
> 23 > 11 8 6.1 High
3.1 Training
The training and test dataset for the high cholesterol
risk prediction is based on the ELSA (Marmot et al.,
1
https://www.mcw.edu/calculators/
ldl-cholesterol-goal-level
SmartWork 2021 - 2nd International Workshop on Smart, Personalized and Age-Friendly Working Environments
446
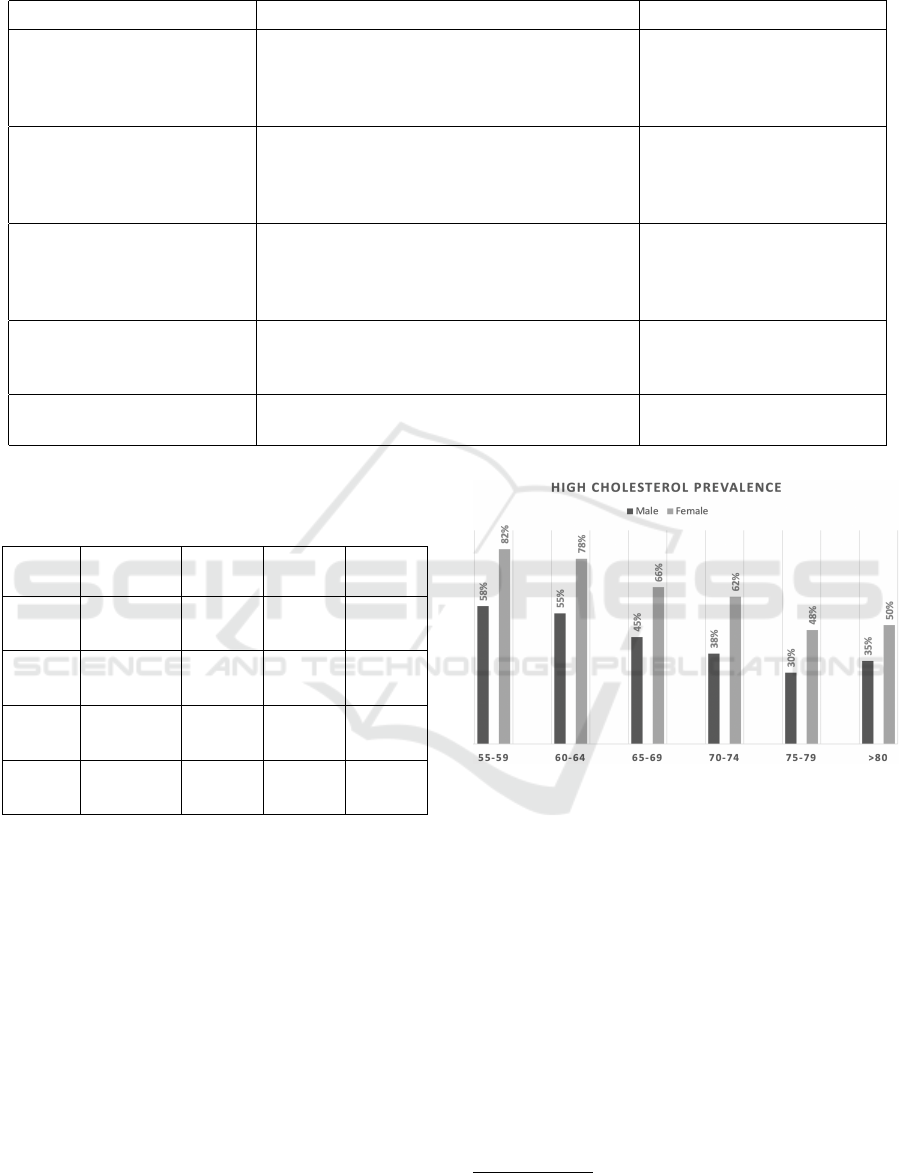
Table 2: Cholesterol risk scoring systems.
Author Model Tool Risk factors included
Framingham Heart 10-year
risk LDL cholesterol Level
LDL cholesterol Level calculator Gender, Age, Smoke status,
High Blood Pressure, Medi-
cation for High Blood Pres-
sure
Jian Liu et al (Liu et al.,
2005)
Joint Distribution of Non-HDL and LDL
Cholesterol and Coronary Heart Disease
Risk Prediction Among Individuals with and
Without Diabetes
Ethnicity, Gender, Age,
Smoke status, Drinking
Alcohol, High Blood
Pressure
Cengiz Colak et al (Colak
et al., 2016)
Prediction of Cholesterol Level in Patient
with Myocardial Infarction Based on Data
Mining Methods
Age, Gender, Smoke sta-
tus, High Blood Pressure,
Physical Activity, Sedentary
lifestyle
Francesco Reggiani et al
(Reggiani et al., 2020)
Prediction of blood cholesterol levels from
genotype data
BMI, Age, Ethnicity, Gen-
der, High Blood Pressure,
Physical Activity
Jin Sol Lee et al (Lee et al.,
2018)
Prediction of cholesterol ratios within a Ko-
rean population
Triglyceride, Age, Gender,
BMI, High Blood Pressure
Table 3: Distribution per gender of newly diagnosed
with High Cholesterol at 2-years follow-up in the original
dataset.
Wave High
Cholest.
Male Female Total
Ref 2 No 2,339 2,829 5,168
F-up 3 Yes 400 552 952
Ref 4 No 2,531 3,161 5,692
F-up 5 Yes 292 293 585
Ref 6 No 2,196 2,797 4,993
F-up 7 Yes 167 173 340
All No 7,066 8,787 15,853
Yes 859 1,018 1,877
2018) database, which consists of reference waves 2,
4 and 6 as baseline and the respective waves 3, 5,
and 7 for the 2-years follow-up assessment. Although
the number of participants in ELSA waves selected
as reference one (namely waves 2, 4, and 6) is very
large, initially we drop out participants that already
have high cholesterol levels at reference waves and
participants that did not take the interview at both, the
reference and the corresponding follow-up wave. In
Tables 3 and 5, the distributions of selected partici-
pants that satisfied the above criteria, per age group
and per gender are presented.
These distributions however correspond to a
dataset that is not representative for the population,
as they do not relate well to the prevalence of high
cholesterol for these age groups as they have been re-
Figure 1: Age Group and Gender distributions in England.
ported at country level
2
. The reported distributions
per age group and per gender in England are shown in
Figure 1.
Similarly, the prevalence of high cholesterol
among people of older age at European level has been
reported as being at over 80% for people aged 55-
64, and at 79% for people aged 65-74 years old. It is
worth noticing, that in Portugal (one of the pilot sites
of SmartWork system), the prevalence of high choles-
terol among adult population (25-74 years old) is at
63.3% (Rodrigues et al., 2016).
Taking into account these findings, we balanced
the dataset using random undersampling, in order to
reach distributions similar to those reported for the
reference population. The distributions of the partici-
2
https://www.statista.com/statistics/983478/
england-high-cholesterol-among-older-people/
Long-term Cholesterol Risk Prediction using Machine Learning Techniques in ELSA Database
447

Table 4: Distribution per gender of newly diagnosed with
High Cholesterol at 2-years follow-up in balanced dataset.
Wave High
Cholest.
Male Female Total
Ref 2 No 756 978 1,734
F-up 3 Yes 400 552 952
Ref 4 No 509 541 1,050
F-up 5 Yes 292 293 585
Ref 6 No 287 320 607
F-up 7 Yes 167 173 340
All No 1552 1839 3,391
Yes 859 1,018 1,877
pants per age group and gender in the balanced dataset
are shown in Tables 4 and 6.
3.2 Features Selection
The initial features set considered for the training of
the ML-based models included 106 variables, with 61
being categorical and 45 numeric attributes, among
those collected at the reference waves of ELSA
dataset. However, their importance was established
using utilizing a feature selection method based on
a variation of Random Forests (Genuer et al., 2010).
According to this method, the attributes are ranked
using the Gini importance score of the model’s trees.
The Gini index (Sundhari, 2011) is calculated as fol-
lows
Gini = 1 −
c
∑
i=1
p
2
i
, (1)
where c is the number of classes and p
i
the relative
frequency of class i in the dataset.
To further reduce the selected number of attributes
without harming the information content of the con-
structed dataset a stepwise backward elimination pro-
cess was also employed using the Logistic model.
The final list of features was reduced to 22 attributes,
among which the most important are: total, HDL
and LDL cholesterol levels at the reference wave, age
group, gender, weight and BMI, drinking and smok-
ing habits, physical activity, education level, diagno-
sis of other chronic conditions (e.g. diabetes, stroke,
high blood pressure), and self-assessed health status.
3.3 Performance Evaluation
In order to assess the overall performance of the en-
gineered dataset, several ML algorithms were em-
ployed, covering a wide range of classifier fami-
lies. The models Na
¨
ıve Bayes (NB) (Quinlan, 2014),
Support Vector Machines (SVM) (Cortes and Vap-
nik, 1995) , Artificial Neural Network (ANN) using
2 hidden layers, 5 Nearest Neighbors (5-NN) (Aha
et al., 1991), Rotation Forest (RotF) (Rodr
´
ıguez et al.,
2006), Decision Trees (DT) (Quinlan, 1986), Logistic
Model Trees (LM Trees) (Landwehr et al., 2005) and
Random Forest (RF) (Breiman, 2001) were applied
on the constructed dataset using a 10-cross validation
(Stone, 1978) experimentation setup.
The model performance results can be seen in
Table 7, with metrics of accuracy and recall being
recorded for each prediction model. As can be ob-
served, although all trained models present similar
moderate accuracies, with the highest being 62.99%
for the LM Trees classifier, the recall demonstrated by
the models is relatively high, meaning that the preva-
lence of high cholesterol can be indicated with a satis-
fying probability in populations similar with the engi-
neered dataset, and thus this fact is considered advan-
tageous for the prognosis of the disease in the context
of the SmartWork system. Finally, the best overall
performance was obtained with the LM Trees model,
which performed best both with respect to accuracy
and recall metrics.
4 CONCLUSIONS
In this research work, a dataset was constructed based
on the ELSA database, aiming at the prognosis of
high cholesterol, targeting the elder office workers.
Several ML methods were examined and the LM
Trees classifier was found to wield the best prediction
performance against the different families of classi-
fiers. Although, the recorded accuracies were moder-
ate, the results presented consistently high recalls, a
fact that seems promising for the discrimination abil-
ity of the models regarding possible positive subjects.
Moreover, a possible path for increasing the
achieved accuracy is the employment of deep learning
(Liu et al., 2017) models and techniques, as they can
provide complex decision boundaries and thus better
fit the training data.
A limitation of the current study is that the engi-
neered dataset does not consider in the features set the
family history in relation to high cholesterol levels as
such information was not available in ELSA.
Future directions of this research work could in-
clude, the further research on feature ranking and
selection techniques such as Least Absolute Shrink-
age and Selection Operator (LASSO) (Muthukrishnan
and Rohini, 2016), and the imputation of the miss-
ing values of the dataset in order to improve the con-
tained information of the dataset. Moreover, learn-
ing paradigms such as self-labeling (Triguero et al.,
2015) can be proved very useful in exploiting the
SmartWork 2021 - 2nd International Workshop on Smart, Personalized and Age-Friendly Working Environments
448
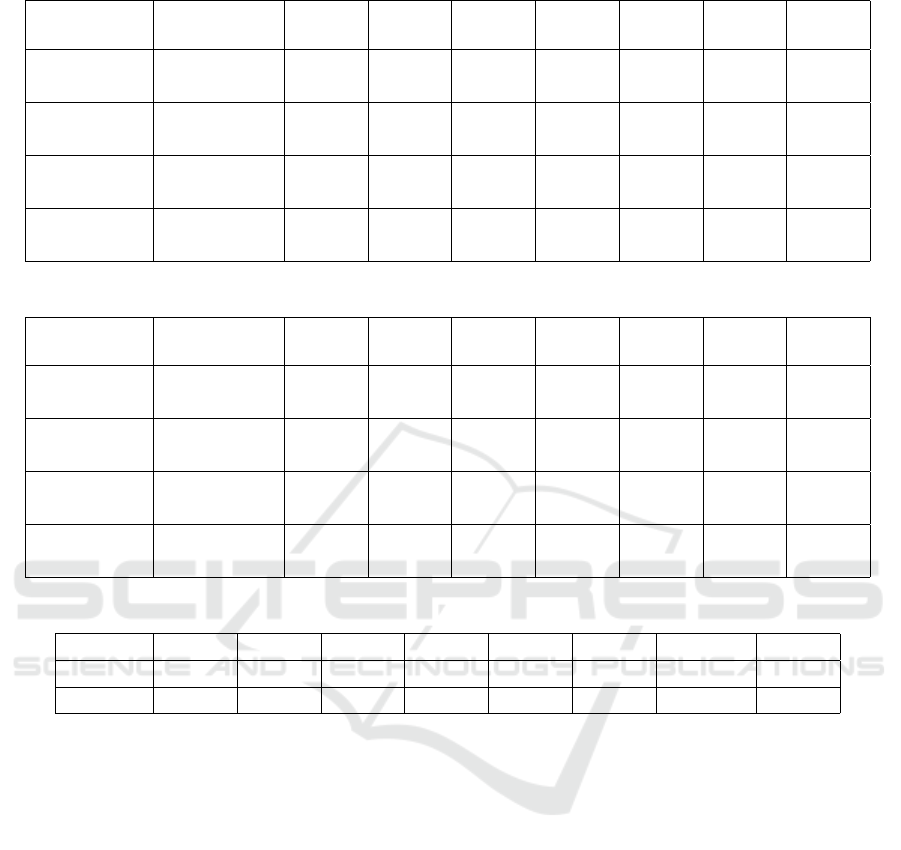
Table 5: Distribution per age group of newly diagnosed with High Cholesterol at 2-years follow-up in the original dataset.
Wave High
Cholesterol
50-54 55-59 60-64 65-69 70-74 75+ Total
Ref wave 2 No 652 1,142 827 754 629 1,164 5,168
F-up wave 3 Yes 92 221 183 158 129 169 952
Ref wave 4 No 852 1,245 1,165 759 711 960 5,692
F-up wave 5 Yes 65 119 122 113 89 77 585
Ref wave 6 No 561 994 1,027 857 566 988 4,993
F-up wave 7 Yes 46 74 74 54 47 45 340
All waves No 2,065 3,381 3,019 2,370 1,906 3,112 15,853
Yes 203 414 379 325 265 291 1,877
Table 6: Distribution per age group of newly diagnosed with High Cholesterol at 2-years follow-up in the balanced dataset.
Wave High
Cholesterol
50-54 55-59 60-64 65-69 70-74 75+ Total
Ref wave 2 No 167 316 275 285 258 433 1,734
F-up wave 3 Yes 92 221 183 158 129 169 952
Ref wave 4 No 118 170 183 204 178 197 1,050
F-up wave 5 Yes 65 119 122 113 89 77 585
Ref wave 6 No 84 106 111 97 94 115 607
F-up wave 7 Yes 46 74 74 54 47 45 340
All waves No 369 592 569 586 530 745 3,391
Yes 203 414 379 325 265 291 1,877
Table 7: Performance Evaluation of ML models.
NB SVM ANN 5-NN RotF DT LM Trees RF
Accuracy 62.69% 59.51% 61.42% 56.56% 61.86% 61.39% 62.99% 61.36%
Recall 68.90% 72.70% 66.70% 67.70% 69.60% 72.20% 73.50% 68.80%
vast amounts of unlabeled data presented in ELSA
database, thus significantly increasing the constructed
dataset size. Finally, the planned future updates on
the ELSA database waves can be utilized to extend
the engineered dataset, providing better modeling ca-
pabilities.
ACKNOWLEDGEMENTS
This work has been partially supported by the Smart-
Work project (GA826343), EU H2020 and SC1-
DTH-03-2018 - Adaptive smart working and living
environments supporting active and healthy ageing.
REFERENCES
Aha, D. W., Kibler, D., and Albert, M. K. (1991).
Instance-based learning algorithms. Machine learn-
ing, 6(1):37–66.
Anagnostis, P., Stevenson, J. C., Crook, D., Johnston, D. G.,
and Godsland, I. F. (2015). Effects of menopause,
gender and age on lipids and high-density lipoprotein
cholesterol subfractions. Maturitas, 81(1):62–68.
Breiman, L. (2001). Random forests. Machine learning,
45(1):5–32.
Chen, S., Bergman, D., Miller, K., Kavanagh, A., Frown-
felter, J., and Showalter, J. (2020). Using applied ma-
chine learning to predict healthcare utilization based
on socioeconomic determinants of care. Am J Manag
Care, 26(01):26–31.
Colak, C., C¸ olak, M. C., Ermis¸, N., Erdil, N., and
¨
Ozdemir,
R. (2016). Prediction of cholesterol level in patients
with myocardial infarction based on medical data min-
ing methods.
Cortes, C. and Vapnik, V. (1995). Support-vector networks.
Machine learning, 20(3):273–297.
Crouse, S. F., O’Brien, B. C., Rohack, J. J., Lowe, R. C.,
Green, J. S., Tolson, H., and Reed, J. L. (1995).
Changes in serum lipids and apolipoproteins after ex-
ercise in men with high cholesterol: influence of in-
tensity. Journal of Applied Physiology, 79(1):279–
286.
Long-term Cholesterol Risk Prediction using Machine Learning Techniques in ELSA Database
449

Fazakis, N., Kocsis, O., Dritsas, E., Alexiou, S., Fakotakis,
N., and Moustakas, K. (2021). Machine learning tools
for long-term type 2 diabetes risk prediction. IEEE
Access, 9:103737–103757.
Genuer, R., Poggi, J.-M., and Tuleau-Malot, C. (2010).
Variable selection using random forests. Pattern
recognition letters, 31(14):2225–2236.
Group, B. S. et al. (2000). Secondary prevention by raising
hdl cholesterol and reducing triglycerides in patients
with coronary artery disease. the bezafibrate infarction
prevention (bip) study. Circulation, 102:21–27.
Kocsis, O., Moustakas, K., Fakotakis, N., Vassiliou, C.,
Toska, A., Vanderheiden, G. C., Stergiou, A., Amaxi-
latis, D., Pardal, A., Quintas, J., et al. (2019). Smart-
work: designing a smart age-friendly living and work-
ing environment for office workers. In Proceedings
of the 12th ACM International Conference on PErva-
sive Technologies Related to Assistive Environments,
pages 435–441.
Landwehr, N., Hall, M., and Frank, E. (2005). Logistic
model trees. Machine learning, 59(1-2):161–205.
Lee, J. S., Cheong, H. S., and Shin, H. D. (2018). Prediction
of cholesterol ratios within a korean population. Royal
Society open science, 5(1):171204.
Liu, J., Sempos, C., Donahue, R. P., Dorn, J., Trevisan,
M., and Grundy, S. M. (2005). Joint distribution of
non-hdl and ldl cholesterol and coronary heart disease
risk prediction among individuals with and without di-
abetes. Diabetes care, 28(8):1916–1921.
Liu, W., Wang, Z., Liu, X., Zeng, N., Liu, Y., and Alsaadi,
F. E. (2017). A survey of deep neural network ar-
chitectures and their applications. Neurocomputing,
234:11–26.
Mahmood, S. S., Levy, D., Vasan, R. S., and Wang, T. J.
(2014). The framingham heart study and the epidemi-
ology of cardiovascular disease: a historical perspec-
tive. The lancet, 383(9921):999–1008.
Marmot, M., Oldfield, Z., Clemens, S., Blake, M., Phelps,
A., Nazroo, J., et al. (2018). English longitudinal
study of ageing: Waves 0–8, 1998–2017.
Muthukrishnan, R. and Rohini, R. (2016). Lasso: A fea-
ture selection technique in predictive modeling for
machine learning. In 2016 IEEE international confer-
ence on advances in computer applications (ICACA),
pages 18–20. IEEE.
Quinlan, J. R. (1986). Induction of decision trees. Machine
learning, 1(1):81–106.
Quinlan, J. R. (2014). C4. 5: programs for machine learn-
ing. Elsevier.
Reggiani, F., Carraro, M., Belligoli, A., Sanna, M., Dal Pr
`
a,
C., Favaretto, F., Ferrari, C., Vettor, R., and Tosatto,
S. C. (2020). In silico prediction of blood cholesterol
levels from genotype data. PloS one, 15(2):e0227191.
Rodr
´
ıguez, J., Kuncheva, L., and Alonso, C. (2006). Rota-
tion forest: A new classifier ensemble method. IEEE
transactions on pattern analysis and machine intelli-
gence, 28:1619–30.
Rodrigues, A. P., Kislaya, I., Antunes, L., Gaio, V., Bar-
reto, M., Santos, A., Gil, A., Namorado, S., Lyshol,
H., Nunes, B., et al. (2016). Prevalence of elevated
cholesterol in portugal: National health examination
survey results (2015) ana paula rodrigues. The Euro-
pean Journal of Public Health, 26(suppl 1):ckw174–
112.
Stone, M. (1978). Cross-validation: A review. Statis-
tics: A Journal of Theoretical and Applied Statistics,
9(1):127–139.
Sundhari, S. S. (2011). A knowledge discovery using de-
cision tree by gini coefficient. In 2011 International
Conference on Business, Engineering and Industrial
Applications, pages 232–235. IEEE.
Triguero, I., Garc
´
ıa, S., and Herrera, F. (2015). Self-labeled
techniques for semi-supervised learning: taxonomy,
software and empirical study. Knowledge and Infor-
mation systems, 42(2):245–284.
Wakabayashi, I. and Groschner, K. (2009). Modification
of the association between alcohol drinking and non-
hdl cholesterol by gender. Clinica Chimica Acta,
404(2):154–159.
SmartWork 2021 - 2nd International Workshop on Smart, Personalized and Age-Friendly Working Environments
450
