
Peculiarities of Health Care System in the Union State Countries and
Priority Directions of Their Marketing Development and Interaction
Tatiana S. Malakhova
1a
, Natalia N. Zubareva
2b
and Marina E. Botalova
2c
1
kuban State University, Krasnodar, Russia
2
belgorod State National Research University, Belgorod, Russia
Keywords: Union State, Foreign Economic Relations, Health System, Morbidity, Outpatient Facilities, Sanctions
Regime, Risks and Threats.
Abstract: The modern health care system is transforming, not only in the Union State countries but also worldwide. The
introduction of new technologies, digitalization, and the transition to a new technological way of life are
giving states a different perspective on the healthcare system, its key gaps, and problems of development. The
presented article is aimed at the research of the key indices in the health care system of the Union State
countries, construction of the econometric model of the correlation between the indices of physical volume
of paid medical services to the population and the volume of paid services to the population of Russia as well
as calculation of forecasts of some economic indices in the mentioned sphere. In addition, the relations of the
Union State countries in the field of health care are investigated, and, on this basis, the directions of their
cooperation are improved. As a theoretical and methodological basis, the article uses historical, logical,
dialectical principles and contradictions, the scientific abstraction method. The process-system approach,
which was used in an in-depth analysis of key indicators in the given area, has become essential in the
argument about the need to strengthen the relations between the countries of the integration group in the socio-
economic sphere. Based on in-depth economic analysis and econometric model formation, the priority
directions of healthcare development in the Union State countries are outlined. The emphasis is shifted to the
development of large-scale projects between the countries of the Union State in the field of healthcare, with
the attraction of public and private investments, development of new technologies for the dynamic
development of this sphere and reduction of import dependence. The study of the health care system of the
Union State countries, identification of problems and contradictions in this field open up opportunities for
further elaboration of the priority directions of development of the mentioned field.
1 INTRODUCTION
In the current context, a new world economic order is
taking shape globally (Malakhova and Kolesnikov,
2019). Russian-Belarusian relations in the format of
the Union State have always implied a balance of
interests of the two countries, which were formed
taking into account political and economic
transformations and upheavals at the end of the XX
century. Today the Union State is more than 20 years
old. The partner countries strive not only to maintain
the mentioned format but also to strengthen mutual
a
https://orcid.org/0000-0002-5971-8178
b
https://orcid.org/0000-0002-4872-3377
c
https://orcid.org/0000-0003-0265-2750
relations in various spheres, including the healthcare
system.
2 RESEARCH METHODOLOGY
In modern conditions, the research in health care is
carried out by the famous Russian scientists A.A.
Redko, V.N. Anisimov, A.V. Finagentov, V.H.
Khavinson, A.V. Shabrov (Redko, Anisimov,
Finagentov, Khavinson & Shabrov, 2020),
considering the problems of creating a system of
integrated medical and social care in Russia, T.V.
Malakhova, T., Zubareva, N. and Botalova, M.
Peculiarities of Health Care System in the Union State Countries and Priority Directions of Their Marketing Development and Interaction.
DOI: 10.5220/0010666800003223
In Proceedings of the 1st International Scientific Forum on Sustainable Development of Socio-economic Systems (WFSDS 2021), pages 247-253
ISBN: 978-989-758-597-5
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
247

Chubarova, E.E. Shestakova (Chubarova and
Shestakova, 2019), denoting that the state remains the
key regulator of social relations and social support for
citizens, G.E. Ulumbekova, A.V. Moklyachenko
(Ulumbekova and Moklyachenko, 2017), exploring
the current state of the Russian healthcare system and
analyzing indicators to assess the performance of
medical organizations, etc. Also, special attention to
this topic is paid by B. Rozenfeld (Rozenfeld, 2021),
who notes that the uneven development of the health
care system has become increasingly evident, the
dissatisfaction of the population with medical
personnel, and the quality of services provided has
increased, P.L. Ferreira, A.I. Tavares, C. Quintal, P.
Santana (Ferreira, Tavares, Quintal and Santana,
2018), highlighting that to date, a significant number
of tools and analytical tools have been developed and
used to classify health systems, but most proposed
typologies include a small number or incomplete set
of countries, etc. On this basis, it can be noted that the
mentioned topic is researched and considered by
scientists from different positions, which makes it
possible to analyze the healthcare system using both
Russian and foreign experience.
3 RESEARCH RESULTS
In modern conditions, the health care system in
Russia and Belarus is undergoing a significant
transformation. On this basis, let us analyze some
indicators characterizing the current state of
healthcare in the Union State countries. It should be
noted that the number of hospital facilities in Russia
and Belarus is decreasing every year. For example, in
Russia, the number of hospital facilities in 2000 was
10,704, 6,308 in 2010, 5,433 in 2015, 5,293 in 2017
and 5,257 in 2018. In 2018, compared to 2000, the
number of hospital facilities decreased by 5,447 units.
A similar trend was observed in the Republic of
Belarus. In 2000, the number of hospital facilities was
830, in 2015 - 640, in 2016. - 636, in 2017. - 622, in
2018. - 612 units. In 2018, compared to 2000, the
number of hospital facilities decreased by 218 units.
If we examine the CIS countries by this indicator,
only Tajikistan and Uzbekistan showed a positive
trend in this indicator for the specified period of time.
For example, in Tajikistan, the number of hospitals in
2000 was 441, in 2010 - 444, in 2015 - 474, in 2017 -
484, in 2018 - 490. In Uzbekistan, this indicator is
unstable, but no significant reductions in the number
of hospitals have been observed. In 2000 there were
1,162 units, in 2010 - 1,158, in 2015 - 1,071, in 2017
- 1,135, in 2018 - 1,165 units. In 2018, compared to
2000, the number of hospitals increased by 3 units. In
the rest of the CIS countries, a decrease in hospital
facilities was observed over the specified period.
Based on this trend, the number of hospital beds in
Russia and Belarus is also decreasing. There were
126,000 hospital beds in Belarus in 2000. A sharp
decline occurred in 2015. So, in 2015 the number of
hospital beds was 82 thousand, in 2016 - 80, in 2017
- 80, in 2018 - 80 thousand. In 2018, the number of
hospital beds decreased by 46,000 compared to 2000.
A similar trend was observed in Russia. In 2000, the
number of hospital beds was 1,672 thousand, in 2010
- 1,339, in 2015 - 1,222, in 2017 - 1,183, in 2018 -
1,173 thousand. Compared to 2000, in 2018 the
number of hospital beds in Russia decreased by 499
thousand. The number of hospital beds, including for
children, in the Union State countries was also
decreasing. In Russia in 2000 there were 229
thousand of them, in 2010 - 179, in 2015 - 163, in
2017 - 158, in 2018 - 157 thousand. The number of
hospital beds for children decreased by 72,000 in
2018 compared to 2000. In the Republic of Belarus,
there were no significant reductions in this indicator.
In 2000, their number was 15 thousand, in 2015 - 11,
in 2016 - 11, in 2017 - 11, in 2018 - 11 thousand. In
2018, the number of hospital beds for children
decreased by 4,000 compared to 2000. Among the
CIS countries, Kazakhstan, Tajikistan and
Uzbekistan had the most stable indicators. In
Kazakhstan, the number of hospital beds for children
in 2000 was 19 thousand, in 2010 - 19, in 2015 - 18,
in 2017 - 18, in 2018 - 19 thousand. In Tajikistan, in
2010, the number of hospital beds for children was 9
thousand, in 2015 - 9, in 2017 - 11, in 2018 - 10
thousand. In Uzbekistan in 2000 there were 29
thousand hospital beds for children, in 2010 - 29, in
2015 - 27, in 2017 - 27 thousand. It is also important
to analyze the number of outpatient facilities in the
Union State countries. In the Republic of Belarus,
their number has increased over the period under
analysis. In 2000, the number of outpatient clinics
was 1.8 thousand, in 2015 - 2.3, in 2016 - 2.3, in 2017
- 2.2, in 2018 - 2, 2 thous. In 2018, the number of
outpatient facilities in the Republic of Belarus
increased by 0.4 thousand compared to 2000. In
Russia, the number of outpatient clinics in 2000 was
21 thousand, in 2010 - 16, in 2015 - 19, in 2017 - 20,
in 2018 - 20 thousand. Compared to 2010, the number
of outpatient clinics increased by 4,000 in 2018. The
capacity of outpatient clinics (number of visits per
shift) in Russia is increasing every year. In 2000, this
indicator was 3,534 thousand, in 2010 - 3,696, in
2015 - 3,861, in 2017 - 3,967, in 2018 - 3,998
thousand. The number of visits per shift increased by
WFSDS 2021 - INTERNATIONAL SCIENTIFIC FORUM ON SUSTAINABLE DEVELOPMENT OF SOCIO-ECONOMIC SYSTEMS
248
464,000 in 2018 compared to 2000. As statistics and
calculations show, this indicator has been increasing
over the years in many CIS countries. For example,
in Uzbekistan, the capacity of outpatient clinics
(number of visits per shift) in 2000 was 415 thousand,
in 2010 - 423, in 2015 - 407, in 2017 - 405, in 2018 .
- 441 thousand. The capacity of outpatient clinics in
Kazakhstan was rather unstable. In 2000, this
indicator was 252 thousand, in 2010 - 263, in 2015 -
269, in 2017 - 215, in 2018 - 268 thousand. In 2018,
compared to 2000, this indicator increased by 16
thousand. In Armenia, the capacity of outpatient
clinics in 2000 was 42 thousand, in 2015 - 39, in 2016
- 40, in 2017 - 40, in 2018 - 40 thousand. The
commissioning of health care facilities is of particular
importance in the health care system. Figure 1 shows
statistical data (in dynamics) for Russia and Belarus
on outpatient and polyclinic facilities (visits per shift)
from 2000 to 2019 and forecast calculation till 2025.
Figure 1: Commissioning of health facilities. Outpatient
facilities (visits per shift) from 2000 to 2019 and projection
to 2025. (calculated by the authors)
Calculations showed that outpatient clinics (visits
per shift) in the Republic of Belarus in 2021 will be
824.4, in 2022 - 747.9, in 2023 - 762.7, in 2024 - 499,
0, in 2025 - 651.2. Compared to 2015, this indicator
may increase by 195.2 in 2025. In Russia, based on
the calculations carried out, in 2021 this indicator will
be 24,013.2, in 2022 - 23,525.3, 2023 - 24,577.1, in
2024 - 25,064.7, in 2025 - 24,301.5. Compared to
2015, it could increase by 592.5 in 2025.
The number of medical personnel is an important
indicator when assessing the health care system in the
Union State countries. Let us analyze this indicator in
more detail in the dynamics from 2000 to 2018. The
number of medical personnel will be represented per
10,000 people in Russia and Belarus. Overall, Russia
and Belarus did not experience a significant reduction
in this indicator. In the Republic of Belarus in 2000
this indicator was 46 people, in 2010 - 54, in 2015 -
43, in 2017 - 44, in 2018 - 45 people. There were 12
general practitioners in 2000, 14 in 2010, 18 in 2015,
19 in 2017 and 20 in 2018. There were also more
surgeons during the analyzed period of time. In 2000
there were 6 of them, in 2010 - 7, in 2015 - 13, in 2017
- 13, in 2018 - 14 people. A similar trend was evident
with pediatricians. In 2000, there were 18 of them in
Belarus, in 2010 - 21, in 2015 - 22, in 2017 - 22, in
2018 - 22 people. The number of pediatricians
increased by 4 per 10,000 population in 2018
compared to 2000. The number of nursing staff is
gradually increasing. In general, the total number of
nursing staff includes all persons with a secondary
medical education. In addition, they are employed in
medical and sanitary organizations, social welfare
institutions, preschools, schools, orphanages, etc. In
2000, the number of nursing staff was 123 people, in
2010 - 129, in 2015 - 133, in 2017 - 133, in 2018 -
134 people. In 2018, the number of nursing staff
increased by 11 compared to 2000. Of these, the
number of nurses was also increasing. In 2000, this
indicator was 77 people, in 2010 - 90, in 2015 - 93, in
2017 - 93, in 2018 - 93 people. Compared to 2000, the
number of nurses increased by 16 in 2018. In Russia,
the situation is less stable and positive according to
the indicators presented above. In 2000, the number
of doctors of all specialties per 10,000 thousand
people of the population was 47 people, in 2010 - 50,
in 2015 - 46, in 2017 - 48, in 2018 - 48 people.
Compared to 2010, in 2018 the number of specialty
doctors decreased by 2 persons. Let us analyze this
indicator in more detail with a breakdown by
specialty. In general, the number of general
practitioners has not changed significantly. In 2000,
this indicator was 11 people, in 2010 - 12, in 2015 -
11, in 2017 - 12, in 2018 - 12 people. Compared to
2000, the number of general practitioners in 2018
increased by 1 person. The number of surgeons in
Russia also did not increase significantly (in 2000 - 4
people, in 2010 - 5, in 2015 - 5, in 2017 - 5, in 2018 -
5 people). There has been a fairly significant
reduction in the number of pediatricians over the
period under analysis. In 2000, there were 28 of them
per 10,000 people of the population of Russia, in 2010
- 32, in 2015 - 23, in 2017 - 23, in 2018 - 20 people.
In 2018, the number of pediatricians decreased by 8
compared to 2000. The number of dentists during the
analyzed period has not changed. In both 2000 and
2018, there were 4 per 10,000 people in Russia. There
were 2 psychiatrists and narcologists in 2000, 2 in
2010, 1 in 2015, 2 in 2017, and 2 in 2018. It is
important to analyze the number of nursing staff. As
in the Republic of Belarus, Russia saw a decrease in
this indicator. In 2000, the number of paramedical
personnel was 108 people, in 2010 - 106, in 2015 -
400
900
1400
1900
0
10000
20000
30000
1996 2006 2016 2026
Russia Belarus
Peculiarities of Health Care System in the Union State Countries and Priority Directions of Their Marketing Development and Interaction
249
106, in 2017 - 104, in 2018 - 102 people. Compared
to 2000, the number of nursing staff decreased by 6
persons in 2018. Of these, there were 70 nurses in
2000, 73 in 2010, 73 in 2015, 73 in 2017, and 73 in
2018. If we analyze individual CIS countries by these
indicators, a negative trend was observed in many
countries. For example, the number of pediatricians
in Kazakhstan in 2000 was 14 people, in 2010 - 16, in
2015 - 12, in 2017 - 1, in 2018 - 3. On this basis, the
number of pediatricians in Kazakhstan in 2018
compared to 2000 decreased by 11 people. A similar
situation took place in Kyrgyzstan. In 2000, the
number of pediatricians was 10 people, in 2010 - 4, in
2015 - 4, in 2017 - 4, in 2018 - 4 people. In 2018,
compared to 2000, the indicator decreased by 6
persons. The number of ambulance stations
(departments) in Belarus in 2018 was 147 units, and
in Russia - 2,276 units.
Particular attention should be paid to final
consumption expenditures of public administration
by function (Table 1). Let us compare the health care
system with other socio-economic and political
spheres. Based on the data presented in Table 1, it
should be noted that every year there has been an
increase in public administration final consumption
expenditures. This trend was also observed in defense
(in 2015 - 1,345.6 billion rubles, in 2016 - 1,832.3, in
2017 - 1,892.8, in 2018 - 1,900.4, in 2019 - 2174.0
billion rubles), and on economic issues (in 2015 -
1,381.2 billion rubles, in 2016 - 1,574.3, in 2017 -
1,676.7, in 2018 - 1,881.2, in 2019 - 2,028.9 billion
rubles), etc. The increase was particularly significant
in health care. In 2015, this indicator was 1,987.2
billion rubles, in 2016 - 1,994.1, in 2017 - 2,130.2, in
2018 - 2,487.7, in 2019 - 2,559.2 RUB bln On this
basis, it is important to forecast the future state of the
analyzed indicator (Population, Employment and
Living Conditions in the Countries of the
Commonwealth of Independent States, 2019).
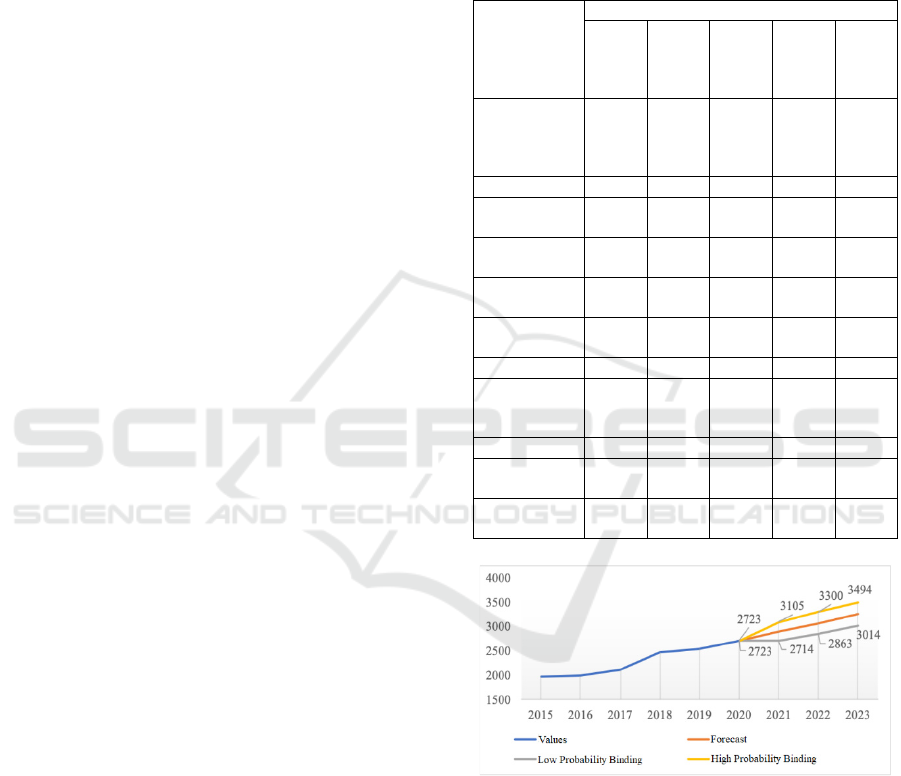
Table 1. As can be seen, the forecast of this
indicator increases under either option. If we consider
the forecast with a low probability, then expenditures
on final consumption of public administration in the
health care sector in 2021 will amount to 2,723 billion
rubles, in 2022 - 2,863, in 2023 - 3,014 billion rubles.
As for the forecast with a high probability, the
expenditures on final consumption of public
administration in the health care sector in 2021 will
be 3,105 billion rubles, in 2022 - 3,300, in 2023 -
3,494 billion rubles. In the first and in the second
case, costs are projected to increase.
Figure 2 shows the calculation of the forecast
(high and low probability) of public administration
final consumption expenditure in health care. Note
that the calculations were made based on the
dynamics of public administration final consumption
expenditure in health care for 2015-2019 presented in
Table 1: Public administration final consumption
expenditure by function for 2015-2019, bln. rub. (National
Accounts of the Commonwealth of Independent States,
2020).
Public
administration
final
consumption
expenditure
Years
2015 2016 2017 2018 2019
General
government
services
1766.6 1801.0 1978.3 2141.5 2247.4
Defense 1345.6 1832.3 1892.8 1900.4 2174.0
Public order
and safet
y
2120.7 2148.9 2200.4 2384.2 2424.0
Economic
issues
1381.2 1574.3 1676.7 1881.2 2028.9
Environmental
p
rotection
22.9 20.9 27.6 29.7 32.0
Housing and
utilities
360.4 365.1 416.8 406.5 434.7
Health 1987.2 1994.1 2130.2 2487.7 2559.2
Recreation,
culture and
religion
147.7 149.4 160.2 172.0 178.3
Educatio
n
638.0 599.8 620.5 666.4 657.6
Social
p
rotection
1409.7 1506.8 1569.6 1615.7 1695.6
Other
functions
3580.7 3817.1 4057.8 4708.8 4947.3
Figure 2: Calculation of projected (high and low
probability) public administration final consumption
expenditure on health (calculated by the authors)
On this basis, let us build an econometric model,
which includes the ratio of indices of physical volume
of paid medical services to the population and the
volume of paid services to the population of Russia
(Figure 3).
WFSDS 2021 - INTERNATIONAL SCIENTIFIC FORUM ON SUSTAINABLE DEVELOPMENT OF SOCIO-ECONOMIC SYSTEMS
250

Figure 3: Econometric model of the ratio of indices of the
physical volume of paid medical services to the volume of
paid services to the population of Russia (calculated by the
authors).
In general, Figure 3 shows the observations'
uniformity presence, also there is the regression
equation and the determination coefficient (R2). The
minimum requirement for model building is for the
coefficient of determination to be greater than 0.5%.
Based on the data provided, this requirement is
complied with.
The equation of the linear pairwise regression
model describing the relationship between the index
of physical volume of paid medical services to the
population and the volume of paid services to the
population is as follows:
y=38.947+0.606*x (1)
It is important to analyze the quality of the
presented model. To do this, we will estimate the
regression coefficients significance using the
Student's t-criteria. Then we will evaluate the model
using variance and correlation analysis.
The Student's test value is 2.262. It is important to
establish the significance of the coefficients a and b,
so we assume that:
No_a: a = 0 - not
statistically
significant
N1_a: a = 0 - not
statistically
si
g
nifican
t
No_b: b = 0 - not
statistically
significant
N1_b: b = 0 - not
statistically
si
g
nifican
t
2.937 > 2.306
Ho_a is rejected with
a probability of 95%
18.462 > 2.306
Ho_b is rejected with
a probability of 95%
Coefficient a is
statistically
si
g
nifican
t
Coefficient b is
statistically
si
g
nifican
t
The next way to analyze the quality of the model
is the Fisher F-criteria or regression dispersive
analysis. The hypothesis is as follows:
Ho: b=0 (there is no linear relationship between
x and
y
)
F critical
–
5.318
F observed 22.114 > F critical 5.318, hence,
the Ho: b=0 hypothesis is deviated, i.e. there is a
linear relationship between the x and
y
variables.
The multiple R is the correlation coefficient value
(the linear relationship tightness measure between the
x and y variables). The multiple R was 0.857, i.e., the
relationship between x and y is strong and direct as
the index ranges from 0.7 to 0.9. Next, we transfer the
correlation coefficient into a percentage and it is
73.43%. Variation of the variable y (volume of paid
services to population) by 73.43% is explained by
variability of the variable x (index of physical volume
of paid medical services to population). The effect of
x on y is 73.43%. Consequently, 26.57% is accounted
for by other factors not taken into account in the
model. The average approximation error is 0.625%,
which indicates the quality of the presented model.
The approximation coefficient should be lower than
7%. It is important to calculate the forecast of the
analyzed data. Thus, x was 104.876% and y was
102.547%. Thus, if x increases by 2% of the average
value, then y will be 102.547%. The intervals of the
predicted value y: min - 100.49%, max - 104.61%.
With a 95% chance of increasing x by 2%, y will be
in the range of 100.49% to 104.61%. The analysis
showed that based on the current situation in the
healthcare system in Russia, the maximum increase
in y is most likely in the future.
The Union State is actively implementing the
priority areas and priorities of its further development
for 2018-2022. Particular attention is paid to
improving the mechanism of health care provision to
Russian citizens in the Republic of Belarus and
citizens of Belarus in the Russian Federation, as well
as health insurance for Russian and Belarusian
citizens temporarily staying in the territory of the
Union State (Figure 4).
Until 2022, the priority task is to ensure sanitary
and epidemiological well-being in the territory of the
Union State. This situation is about cooperation in
sanitary and epidemiological well-being and jointly
overcoming emerging risks and threats. Also, the
development of information technologies and
telemedicine; provision of accessibility and quality of
specialized, including high-tech medical care;
provision of continuous medical and pharmaceutical
education using modern technologies, etc., are of
particular importance in the priority areas of
cooperation in healthcare.
Peculiarities of Health Care System in the Union State Countries and Priority Directions of Their Marketing Development and Interaction
251

Figure 4: Interaction of the Union State countries in
healthcare and improvement of its regulatory framework
(compiled by the authors)
(Priority areas and priorities for further
development of the Union State for 2018-2022,
2018). On this basis, it is important to improve further
the mechanisms of relations between the Union State
countries in health care development, active
involvement of research centers for joint work in this
area (Figure 4).
4 DISCUSSION OF RESULTS
Today it is possible to further form joint
developments and programs in healthcare within the
framework of the Union State. This is a strategically
important area because countries need to move away
from imported technology and medicines. This
problem is especially relevant in the context of the
prolongation of the sanctions regime by the countries
of the European Union and the United States
(Malakhova, 2019). Health care development in both
the Union State and the EAEU countries is a priority
area ensuring their national security. In addition, it
should be noted that further development of the
Eurasian Economic Union involves strengthening
cooperation ties, including in healthcare. Some
private projects directly related to healthcare (e.g.,
Teledoctor, Oriense, Button of Life, Medesc, 3D
Bioprinting Solutions) are developing in Russia
today. In addition to private projects, there are federal
projects for which the Russian government is
responsible (e.g., Demography, Health, etc.)
(Borkova, Napolova, and Orlov, 2019). Undoubtedly,
it is important to develop this key social sphere with
the EAEU partner countries.
5 CONCLUSION
In modern conditions in the Union State countries, it
is important to increase real incomes of the
population, develop a socially-oriented model of
economy, increase financing and efficiency of
healthcare. These areas can lead to an improvement
in the quality of life and, in the long term, allow for
an increase in life expectancy. The statistical data
analysis and construction of the econometric model
showed that in the Union State countries, the number
of hospital facilities, the number of hospital beds,
including those for children, decreases every year.
The capacity of outpatient clinics (number of visits
per shift) in Russia was 3,534 thousand in 2000, and
3,998 thousand in 2018, i.e., the increase was by 464
thous.
Thus, firstly, the number of hospital facilities, the
number of hospital beds, including those for children,
the number of medical personnel, etc., were analyzed
in detail. The problems and contradictions in the
development of health care systems in Russia and
Belarus associated with the reduction of the number
of doctors for certain specialties and a parallel
increase in the morbidity of the population on the
main classes of diseases, including malignant tumors,
respiratory diseases, diseases of the circulatory
system, digestive diseases, etc. have been revealed.
Secondly, the priority areas and priorities of
further development of the Union State for 2018-2022
have been investigated. Particular attention is paid to
the development of cooperation in healthcare, as well
as the improvement of the regulatory framework. On
this basis, the priorities of the priority areas and
options for their solutions are explored. It is proposed
to pay special attention to the development of large-
scale projects between the countries of the Union
State in the field of healthcare with the attraction of
public and private investments, development of new
technologies, etc.
REFERENCES
Anisimov, V.N., Redko, A.A., Finagentov, A.V.,
Khavinson, V.Kh., Shabrov, A.V. (2020). Creation of a
regional system for providing comprehensive medical
and social assistance to citizens of the older generation:
the experience of St. Petersburg. Advances in
gerontology, 5: 809-824.
WFSDS 2021 - INTERNATIONAL SCIENTIFIC FORUM ON SUSTAINABLE DEVELOPMENT OF SOCIO-ECONOMIC SYSTEMS
252

Borkova, E.A., Napolova, E.A., Orlov, E.R. (2019).
Problems of development and implementation of
innovations in healthcare in Russia. Creative economy,
13(7): 1495-1502.
Population, employment and living conditions in the
countries of the Commonwealth of Independent States,
2018: stat. Sat. Interstate Statistical Committee of the
CIS. - M. (2019), pages 73–85.
National accounts of the countries of the Commonwealth of
Independent States 2015-2019: Stat. Sat. Interstate
Statistical Committee of the CIS. - M. (2020) . p. 306.
Priority areas and priorities for the further development of
the Union State for 2018-2022. http:
https://www.postkomsg.com/documentation/
Ulumbekova, G.E., Moklyachenko, A.V. (2017). Indicators
for assessing the performance of medical organizations:
international experience. Bulletin of the Higher School
of Economics, 3.
Chubarova T.V., Shestakova E.E. (2019). State in the social
sphere: vectors of change. World of change, 3: 126-142.
Ferreira, P.L., Tavares, A.I., Quintal, C., Santana, P. (2018).
EU health systems classification: a new proposal from
EURO-HEALTHY. BMC Health Services Research.
http:
https://bmchealthservres.biomedcentral.com/articles/1
0.1186/s12913-018-3323-3
Malakhova, T.S., Dubinina, M.A., Maksaev, A.A., Fomin
R.V. (2019). Foreign Trade and Marketing Processes in
the Context of Sustainable Development. International
Journal of Economics and Business Administration,
Greece. Special Issue 2: 195202.
Malakhova, T.S., Kolesnikov, N.P. (2019). Trends and
contradictions of the global economy crisis and
transformation of the world financial institutions.
European. Journal of Economics and Management
Sciences, Scientific journal, Vienna, 1: 38-41.
Rozenfeld, B. The Crisis of Russian Health Care and
Attempts at Reform. Objective Analysis. Effective
Solutions. http:
https://www.rand.org/pubs/conf_proceedings/CF124/
CF124.chap5.html
Peculiarities of Health Care System in the Union State Countries and Priority Directions of Their Marketing Development and Interaction
253
