
Comparison of Serum MMP-9 Value in Spondylitis Tuberculous with
Degenerative Spine Disease
Yohanes Augustinus
1*
, Otman Siregar
2
, and Benny
3*
1
Resident of Orthopaedic and Traumatology, Faculty of Medicine Universitas Sumatera Utara/ Haji Adam Malik Hospital-
Medan
2
Consultant of Orthopaedic and Traumatology, Spine Division, Faculty of Medicine Universitas Sumatera Utara/ Haji
Adam Malik Hospital-Medan
3
Staff of Orthopaedic and Traumatology, Spine Division, Faculty of Medicine Universitas Sumatera Utara/ Haji Adam
Malik Hospital-Medan
Keywords: Matrix metalloproteinase, MMP-9, Spondylitis Tuberculous, Degenerative Spine Disease
Abstract: Fourteen (14) subjects were divided into 2 groups, with seven (7) subjects of spondylitis tuberculous and 7
subjects of degenerative spine disease in the period from December 2017 to November 2018 who were
included in the inclusion criteria included in this study and blood sampling was taken for examination of
serum MMP-9 levels. There were significant differences in serum MMP-9 levels between spondylitis
tuberculous and degenerative spine diseases with a significance value of 0.002 (p<0.05) with low serum
MMP-9 levels in the spondylitis tuberculous study group 1857.14 ± 377.96 and mean in the control group
857.14 ± 243.97. There were significant differences in serum MMP-9 levels between spondylitis
tuberculous and degenerative spine diseases with a significance value of 0.002 (p<0.05) with low serum
MMP-9 levels in the spondylitis tuberculous study group 1857.14 ± 377.96 and mean in the control group
857.14 ± 243.97. Patients suffering from spondylitis tuberculous have higher serum MMP-9 levels than
patients with degenerative spine disease, although MMP-9 is not a specific marker examination for
spondylitis tuberculous, the results of this study can be suggestive into that can help to evaluate enzyme
activity in patients with spondylitis tuberculous disease.
1 INTRODUCTION
Tuberculous (TB) is one of the long-known diseases
and is still the leading cause of death in the world.
The prevalence of TB in Indonesia and other
developing countries is quite high. In 2006, new
cases in Indonesia amounted to more than 600,000
and most of them were suffered by people in
productive age (15–55 years).
About 20% of infections with pulmonary TB will
spread out of the lungs (extrapulmonary TB). Eleven
percent of extrapulmonary TB is osteoarticular TB,
and nearly half of patients suffer from spinal TB
infection. Half have lesions in the spine with
neurological deficits of 10% - 45% of sufferers.
Spondylitis tuberculous is an infection of the
spine caused by Mycobacterium tuberculous
(Lindsay et. Al., 1991; Martini and Welch, 2001;
Savant and Rajamani, 1997; Tachdjian, 1990).
Spondylitis tuberculous results in damage to the
body in the form of a defect that causes spinal
instability and disruption of surrounding structures
(Lindsay, et. Al., 1991; Tachdjian, 1990). The
occurrence of infection in spondylitis tuberculous
can originate from primary infection (Graham and
Kozak, 1993; Martini and Welch, 2001; Savant and
Rajamani, 1997), bacteria directly infect the corpus,
or secondary infections (Graham and Kozak, 1993;
Savant and Rajamani, 1997), namely bacteria spread
hematogenously or lymphogens from the location of
the primary disease to the spinal cord (Martini and
Welch, 2001). Infections that occur in spondylitis
tuberculous are generally secondary infections of the
lungs, but in some cases are primary infections. Pro-
inflammatory and anti-inflammatory cytokines play
an important role in the development and control of
Mycobacterium tuberculous infection (Patil, et. Al.,
2015). It has been demonstrated that cytokine
profiles will differ in each degree of disease
(Graham and Kozak, 1993; Lindsay, et. Al., 1991).
Augustinus, Y., Siregar, O. and Benny, .
Comparison of Serum MMP-9 Value in Spondylitis Tuberculous with Degenerative Spine Disease.
DOI: 10.5220/0009863602170220
In Proceedings of the 2nd International Conference on Tropical Medicine and Infectious Disease (ICTROMI 2019), pages 217-220
ISBN: 978-989-758-469-5
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
217

Several cytokines have been known to be
biomarkers of disease activity in tuberculous
infections. Matrix metalloproteinase (MMP) is a
zinc-dependent protease, which plays a role in the
process of degradation of the extracellular matrix
and modulates the inflammatory response by
facilitating and inhibiting different cytokines
(Salgame, 2011).
In determining the form of treatment for
spondylitis tuberculous, it is generally divided into
two groups of patients, namely groups of patients
accompanied by complications in the way of
neurological disorders and groups that are not
accompanied by neurological disorders. In patients
without neurological complications, medical
treatment is the primary choice in treatment, and
surgical treatment is only needed in some special
cases. But in patients who are accompanied by
neurological complications, the combination of
medical treatment and surgical management is the
most appropriate treatment.
Matrix Metalloproteinase is a zinc-dependent
proteinase that has an important role in the
degradation and rotation of the extracellular matrix.
[4] Since it was first reported, 24 members of MMP
have been identified with specificity and function of
overlapping substrates.4 Following each substrate
and function specification, MMP is divided into six
classes: stromelysins, collagenases, matrilysins,
gelatinases, membrane-type MMPs, and others.
Two gelatinases, MMP-2, and MMP-9 can reduce
original type IV collagen and denaturation of type I
collagen (gelatin). Both circulation and resident
inflammatory cells can synthesize MMP-9.
Experimental studies have provided evidence that
MMP-9 levels were significantly higher in
bronchoalveolar fluid patients with cavitary active
tuberculous, and lung extracts of mice infected with
M. tuberculous, compared to the control group. An
increased significance of MMP-9 was also observed
in tuberculous cerebrospinal fluid (CSF) meningitis
patients and also compared with people suffering
from viral meningitis, where usually these enzymes
are generally not found in cerebrospinal fluid.
Many previous studies have shown that M.
tuberculous can stimulate MMP-9 expression in the
lungs of infected organisms, but no studies have
examined how the expression of MMP-9 in
tuberculous spondylitis when compared to the control
group. Therefore, researchers are interested in trying
to evaluate and compare the expression of MMP-9 in
tuberculous spondylitis using serum levels in the
blood of patients suffering from tuberculous
spondylitis and compared to the control group, in this
case, the control group in this study were patients
with degenerative diseases of the spine.
2 METHODS
This cross-sectional study was conducted at the
Faculty of Medicine, Universitas of North Sumatra /
Haji Adam Malik Hospital, North Sumatra,
Indonesia for 11 months from December 2017 to
November 2018 by taking patient data and
examining serum values of MMP-9, 14 subjects met
the inclusion criteria.
Patients who met the inclusion criteria recorded
age, sex and blood tests to determine serum MMP-9
levels.
The study sample was divided consecutively
with equal numbers into two groups, namely:
spondylitis tuberculous, degenerative spine disease.
Patients were obtained from outpatient or inpatient
care diagnosed with spondylitis tuberculous and
degenerative spine disease. Patients who were
included in the inclusion criteria were taken for
blood sampling to examine levels of MMP-9.
The MMP-9 examination in this study used
MMP-9 (Matrix Metallo Proteinase 9) ELISA Kit
from Fine Test with the catalog number ERB0080,
size 48T / 96T and reactivity to humans. The scale
value used is 3.125-200ng / ml with sensitivity:
<1.875ng / ml. The application of this dosage
application is a quantitative detection of MMP-9 in
serum, plasma, tissue homogenates, and other
biological fluids. Differences in serum MMP-9
values in spondylitis tuberculous with the
degenerative disease in the spine were analyzed
using the Mann-Whitney test because the data
obtained were abnormally distributed. All statistical
calculations are carried out using a computer-based
statistical program. The study was approved by the
Health Research Ethics Committee of the Medical
Faculty of the University of North Sumatra / Haji
Adam Malik Hospital, and informed consent was
obtained from all subjects.
3 RESULTS
Before discussing the results of the study, because
this study had no references, it was conducted with a
small-scale preliminary study using 10 balanced
numbers of research subjects (5 subjects with
spondylitis tuberculous, 5 subjects with degenerative
spine disease) with women as many as 6 people
ICTROMI 2019 - The 2nd International Conference on Tropical Medicine and Infectious Disease
218
(60%) and men as many as 4 people (40%). With a
mean and standard deviation of 41.6 ± 18.8 years.
While the mean of subjects with spondylitis
tuberculous (ST) 1800 ± 447.2 and mean
degenerative spine disease (DSD) 800 ± 273.8.
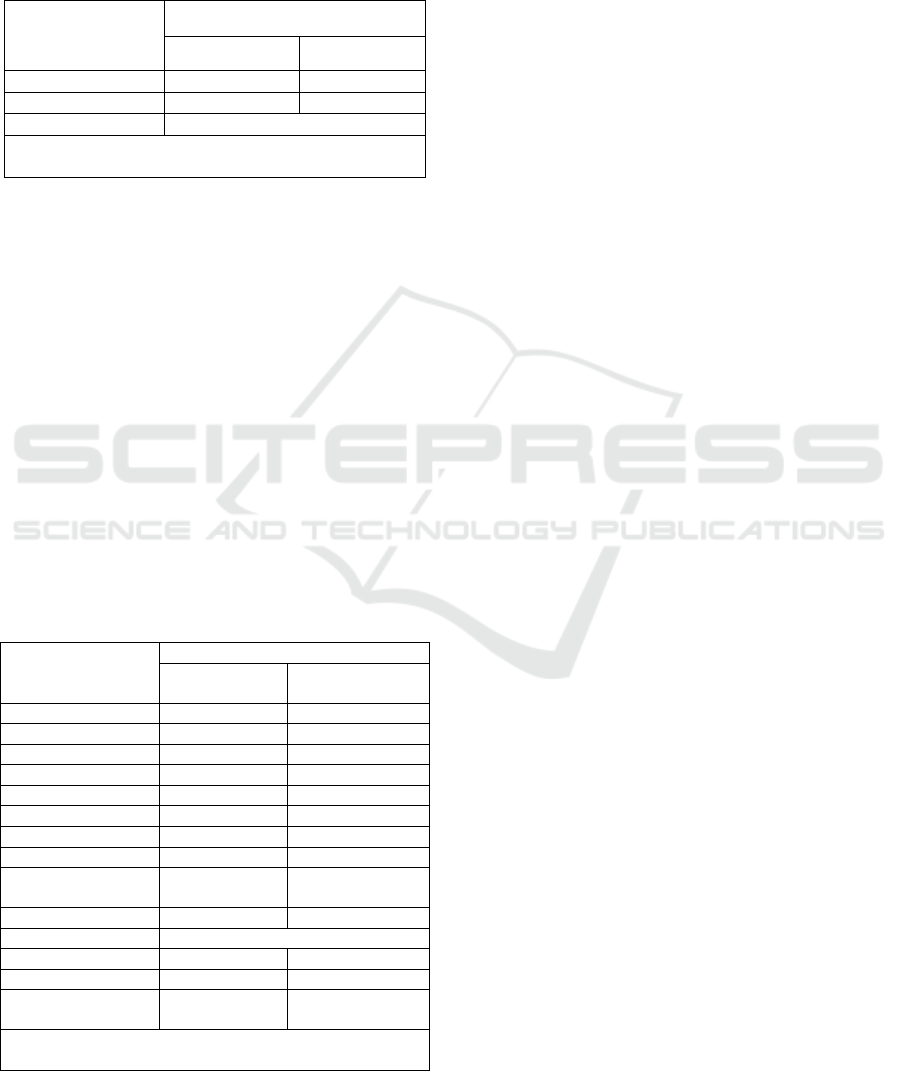
Table 1. Preliminary Study Distribution
Variable
Disease
ST DSD
Gender M/F 1/4 3/2
MMP-9 (nm/ml) 1800 ± 447.2 800 ± 273.8
Mean age 41.6 ± 18.8
ST, Spondylitis Tuberculous; DSD, Degenerative
Spine Disease; n, Subject
A total of 14 subjects were studied until the final
analysis. Data retrieval and examination of serum
MMP-9 values in spondylitis tuberculous (ST) and
degenerative spine disease (DSD) were carried out
in stages with the initial phase of selecting samples
of subjects included in the inclusion criteria. 7
subjects with diagnosed spondylitis tuberculous
(ST), 7 subjects with diagnoses of degenerative
spine disease (DSD), 8 women (57.1%) and 6 men
(42.9%), 13 years youngest research subjects and 73
years old oldest subjects with mean and standard
deviations amounting to 44.79 ± 16.98 years. From
the results of the analysis, it was found that the mean
and standard deviation of serum ST MMP-9 values
were 1857.14 ± 377.96 while the mean and standard
deviation of serum DSD levels of MMP-9 were
857.14 ± 243.97.
Table 2. Study Subject Distribution
Variable
Disease
ST MMP-9
(nm/ml)
DSD MMP-9
(nm/ml)
Patient
1 2000 1000
2 1000 1000
3 2000 500
4 2000 500
5 2000 1000
6 2000 1000
7 2000 1000
Mean MMP-9
(nm/ml)
1857.14 857.14
SD ± 377.96 ± 243.97
p-Value 0.002
Youngest age 13 year old 43 year old
Oldest age 62 year old 73 year old
Tuberculous drug
consumption
9.14 ± 5.29
weeks
0
ST, Spondylitis Tuberculous; DSD, Degenerative Spine
Disease; n, Subject
From the results of the statistical analysis of the
comparison of serum MMP-9 values in tuberculous
spondylitis (ST) with degenerative spine disease
(DSD), the results were significant that the serum
MMP-9 values were higher and this was indicated
by a p-value of 0.002 (p <0.05).
4 DISCUSSION
Pott's disease is the most common spinal
granulomatous bacterial infection and is the most
frequent bone TB. [6] The occurrence of infection in
spondylitis tuberculous can originate from primary
infection (Graham and Kozak, 1993; Martini and
Welch, 2001; Savant and Rajamani, 1997), i.e.
bacteria directly infect the corpus, or secondary
infections (Graham and Kozak, 1993; Savant and
Rajamani, 1997), namely bacteria spread
hematogenously or lymphogens from the location of
the primary infection to the spinal cord (Martini and
Welch, 2001). Infections that occur in spondylitis
tuberculous are generally secondary infections of the
lungs, but in some cases are primary infections. Pro-
inflammatory and anti-inflammatory cytokines play
an important role in the development and control of
Mycobacterium tuberculous infection (Patil, et. Al.,
2015). It has been demonstrated that cytokine
profiles will differ in each degree of disease
(Graham and Kozak, 1993; Lindsay, et. Al., 1991).
Several cytokines have been known to be
biomarkers of disease activity in tuberculous
infections. Matrix metalloproteinase (MMP) is a
zinc-dependent protease, which plays a role in the
process
of degradation of the extracellular matrix and
modulates the inflammatory response by facilitating
and inhibiting different cytokines (Salgame, 2011).
Two gelatinases, MMP-2, and MMP-9 have the
ability to reduce original type IV collagen and
denaturation of type I collagen (gelatin). Both
circulation and resident inflammatory cells have the
capacity to synthesize MMP-9. Experimental studies
have provided evidence that MMP-9 levels were
significantly higher in bronchoalveolar fluid patients
with cavitary active tuberculous, and lung extracts of
mice infected with M. tuberculous, compared to the
control group.
In a study conducted by Hrabec et al., 2002 it
was found that serum MMP-9 levels in patients with
active pulmonary tuberculous had significantly
higher levels of the control group with mean MMP-9
levels in the group with pulmonary tuberculous 1.23
± 0.43 µU / µL, while the mean MMP-9 level in the
Comparison of Serum MMP-9 Value in Spondylitis Tuberculous with Degenerative Spine Disease
219

control group was 0.37 ± 0.10 µU / µL and this
result was in accordance with the function of MMP-
9 which could induce enzymes produced by
mononuclear phagocytes and stimulated neutrophils.
This finding is in accordance with the study
conducted that there was a significant difference in
MMP-9 levels in patients with spondylitis
tuberculous with a control group used in this group
with subjects with degenerative spine disease with
mean spondylitis tuberculous patients 1857.14 ±
377.96 while the mean in patients with degenerative
spine disease 857.14 ± 243.97 with p-value 0.002 (p
<0.05), but in this study there was no comparison of
the ratio of white blood cell levels in the two study
groups as did the research conducted by Hrabec et al
2002 with this study obtained MMP-9 rate with an
increase in white blood cells was significantly higher
in the study group with pulmonary tuberculous
0.150 ± 0.054 mU/ml/L while in the control group
0.059 ± 0.023 mU/ml/L. In this study no correlation
was found between the duration of consumption of
anti-tuberculous drug and an increase in serum
MMP-9 levels (p> 0.05) with an average use for
tuberculous medicines 9.14 ± 5.29 weeks, although
this was not a primary goal in this study, but need to
be reviewed, because this assessment only uses 7
research subjects.
5 CONCLUSION
From the results of the comparison of serum
MMP-9 values in spondylitis tuberculous with
degenerative spine diseases, it was found that the
serum MMP-9 values in spondylitis tuberculous
gave higher results so that MMP-9 examination
could be used as a barometer for the diagnosis of
spondylitis tuberculous.
Further studies are needed to find out whether the
increase in serum MMP-9 levels in tuberculous
spondylitis is also accompanied by an increase in the
ratio of white blood cells and further studies are
needed to determine whether an increase in serum
MMP-9 levels can also be influenced by the duration
of use of anti-tuberculous drugs.
REFERENCES
Agarwal P, Rathi P, Verma R, Pradhan CG. (199)
Tuberculous spondylitis: “Global lesion”. Special
issues on Tuberkulosa. Bombay Hospital Journal.
Hrabec E, Strek M, Zieba M, Kwiatkowska S, Hrabec Z.
(2002) Circulation level of matrix metalloproteinase-9
is correlated with disease severity in tuberculosis
patients. INT J TUBERC LUNG DIS 6(8):713–719.
Graham JM, Kozak J. Spinal Tuberculosis. In: Hochschule
SH, Cotler HB, Guyer RD., editor. Rehabilitation of
The Spine: Science dan Practice. St. Louis: Mosby-
Year Book, Inc., 1993: 387-90.
Leibert E, Haralambou G. Tuberkulosa. (2004). In: Rom
WN and Garay S, eds. Spinal tuberculosis. Lippincott,
Williams, and Wilkins.
Lindsay, KW, Bone I, dan Calldaner R. Spinal Cord dan
Root Compression. In: Neurology dan Neurosurgery
Illustrated. 2
nd
ed. Edinburgh: Churchill Livingstone,
1991: 388
López-Otín C, Palavalli LH, Samuels Y. (2009) Protective
roles of matrix metalloproteinases: from mouse
models to human cancer. Cell Cycle.
Martini F.H, Welch K. The Lymphatic System dan
Immunity. In: Fundamentals of Anatomy dan
Physiology. 5th ed. New Jersey: Upper Saddle River,
2001: 132,151.
Patil T, Garg RK, Jain A, Goel MM, Malhotra HS, Verma
R, Singh GP, dan Sharma PK. Serum dan CSF
Cytokines dan matrix metalloproteinases in spinal
tuberculosis. Inflamm. Res. (2015) 64:97-106.
Salgame P. MMPs in tuberculosis: granuloma creators
dan tumor destroyers. J Clin Invest. 2011;121:1686-8.
Singh S, Dawar H, Das K, Mohapatra B, Prasad S. (2017)
Functional and radiological outcomes of anterior
decompression and posterior stabilization via
posterior transpedicular approach in thoracic and
thoracolumbar Pott's disease: A Retrospective Study.
Asian Spine J 11(4):618-626.
Tachdjian, M.O. Tuberculosis of the spine. In: Pediatric
Orthopedics.2nd ed. Philadelphia: W.B. Saunders,
1990: 1449-54.
Venkateshwari A, Sri Manjari K, Krishnaveni D, Nallari
P, Vidyasagar A, Jyothy A. (2011). Role of plasma
MMP 9 levels in the pathogenesis of chronic
pancreatitis. Indian J Clin Biochem.
Velazquez V, Barrera D, Arenas G, Rosales C, Heiva A.
Macrophage Mycobacterium Tuberculosis
Interactions: Role of Complement Receptor 3.
Microbiology Pathology. 2003;35(3):125-31.
Walker NF, Clark SO, Oni T, Danreu N, Tezera L, Singh
S, Saraiva L, Pedersen B, Kelly DL, Tree JA,
D’Armiento JM, Friedldan JS, dan Elkington PT.
Doksisiklin dan HIV Infection Suppress Tuberculosis-
induced Matrix Metalloproteinases. 2012. Am J
Respir Crit Care Med Vol. 185, Iss.9, pp989-997.
Zhang M, Lin Y, Iyer DV, Gong J, Abrams JS, dan
Barnesi PF. T-Cell Cytokine Responses in Human
Infection with Mycobacterium tuberculosis. Infect
Immun. 1995;63(8):3231-4.
ICTROMI 2019 - The 2nd International Conference on Tropical Medicine and Infectious Disease
220
