
The Correlation between Apolipoprotein B Levels and
Inflammatory Markers in Obese Individuals
Dian Anindita Lubis
1
, Dharma Lindarto
1*
1
Department of Internal Medicine, Faculty of Medicine, Universitas Sumatera Utara,
H. Adam Malik Hospital, Jalan Bunga Lau No 17, Medan 20136, Indonesia
Keywords: Apolipoprotein B, obesity, cardiovascular disease, atherosclerosis.
Abstract: Apolipoprotein B (ApoB) levels reflect the total number of potentially atherogenic particles that can
predict cardiovascular risk. The purpose of this study was to assess if the ApoB in obese subjects is
associated with inflammatory markers. This cross-sectional study was conducted in 80 obese patients at
Haji Adam Malik Hospital, Medan, Indonesia. Of the 80 patients studied, the average age was 38.95 +
8.13 years old. There was a strong positive correlation between ApoB and triglycerides (r=0.44,
P<0.001), low-density lipoprotein cholesterol (r=0.74, P<0.001), and HOMA-IR (r=0.31, P=0.005).
However, no strong correlation with the inflammatory markers were seen; adiponectin (r=-0.23,
P=0.41) and Chemerin (r=0.021, P=0.851). In obesity, ApoB is significantly associated with lipid and
insulin resistance, as a risk factor for cardiovascular disease.
1 INTRODUCTION
Obesity, characterized by the excess amount of
abnormal fat, may interfere in an optimal state of
health. It may increase the mortality risk through
chronic diseases, such as cardiovascular disease,
type 2 diabetes, and cancer (Tobias and Hu, 2018).
The increment of cardiovascular disease risk is due
to inflammation, hyperlipidemia, high blood
glucose, elevated insulin levels and high blood
pressure (Adams et al., 2006; Klop et al., 2013).
In obese individuals, the risk for atherosclerotic
disease is still high even after adjustment for
established risk factors. It is thought that there are
abnormalities in lipoprotein metabolism that do not
cause hyperlipidemia and yet accelerate
atherosclerosis (Egusa et al., 1985). Low-density
lipoprotein (LDL) are atherogenic; however, when
triglyceride concentration is high, LDL values are
often not available. Therefore, other markers of
lipoprotein-related to cardiovascular disease are
needed. The measurement of lipoprotein particle
such as apolipoprotein B (ApoB) may enhance the
prediction of the risk of cardiovascular disease
(Holme et al., 2007; Khadem-Ansari et al., 2009).
As part of metabolic syndrome, chronic
inflammation has also been associated with obesity.
Larger adipocytes in abdominal obesity alter the
ability to suppress lipolysis. Fat tissue releases
adipocytokines that may cause insulin resistance and
increased risk of cardiovascular disease. There are
two types of adipocytokines; classical
adipocytokines (adiponectin, resistin, and leptin) and
new adipocytokines (chemerin, omentin, and
omentin) (Ellulu et al., 2015; Gateva et al., 2018).
Several studies have examined the association
between plasma lipid and inflammatory markers.
However, the evaluation of ApoB is rarely included.
Therefore, we aim to examine the association
between ApoB and inflammatory markers such as
adiponectin and chemerin in obesity.
2 MATERIALS AND METHODS
This cross-sectional study was conducted in Haji
Adam Malik Hospital, Medan, Indonesia. Obese
nurses (BMI > 25 kg/m2) aged 30-55 were recruited.
Eighty subjects agreed to participate. Informed
consent was obtained from each subject, following
ethical approval from the Health Research Ethical
Committee of Universitas Sumatera Utara,
Indonesia. Subjects with a secondary illness such as
acute inflammation, anemia, menopause, diabetes,
cardiovascular disease, chronic kidney disease, liver
64
Lubis, D. and Lindarto, D.
The Correlation between Apolipoprotein B Levels and Inflammatory Markers in Obese Individuals.
DOI: 10.5220/0009858900640067
In Proceedings of the 2nd International Conference on Tropical Medicine and Infectious Disease (ICTROMI 2019), pages 64-67
ISBN: 978-989-758-469-5
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
dysfunction and subjects with secondary obesity
such as pregnancy, smoking cessation, patients
treated with corticosteroid, estrogen, beta-adrenergic
receptor agonists, nitrates, or other vasodilator
agents were excluded.
Blood samples were collected from the subjects
in the morning after 10-12 hours of fasting
combined with ethylenediaminetetraacetate (EDTA)
containing heparin, and then centrifuged.
2.1 Biochemical Analysis
Serum HDL cholesterol (HDL-C) and triglycerides
(TG) were analyzed by the enzymatic colorimetric
method, while Apo-B levels were assessed by the
immunoassay method with Hitachi Modular
analyzer using the Roche Diagnostic kit. Insulin
levels were determined by the chemiluminescence
immunoassay method using the DPC Immulite-I
analyzer (Diagnostic Products Corp, Los Angeles,
CA, USA) kit.
HOMA-IR formula (Matthews et al., 1985) was
used to determine the index of insulin resistance
using the following formula:
HOMA-IR = [(fasting glucose serum (mmol / l)
x fasting insulin (μU / ml) / 22,5]
2.2 Statistical Analysis
Data are presented as mean + standard deviation.
All data were summarized as descriptive statistics.
To determine whether a variable was normally
distributed, we used the Shapiro-Wilk test. The
parametric analysis was performed on variables with
normal distribution, whereas the nonparametric test
was performed on variables with the abnormal
distribution. Furthermore, the Pearson and Spearman
test were used to evaluate the correlation between
variables according to the variable distribution. A
value of P < 0.05 was accepted as an indication of
statistical significance. SPSS for Windows 22.0 was
used for the statistical analysis.
3 RESULTS
This analysis included 80 obese individuals with no
previous history of cardiovascular disease. The mean
age was 38.95 + 8.13 years. The risk factors for
cardiovascular disease and inflammatory markers
(adiponectin and chemerin) measured in this study
are presented in Table 1.
Pearson correlation of Apo-B with all
traditional risk factors is presented in Table 2. In
general, apoB correlated positively with LDL-C,
TG, HOMA-IR and negatively with HDL-C. Apo-B
also has a strong correlation with HOMA-IR.
However, there is no correlation between Apo-B and
inflammatory markers.
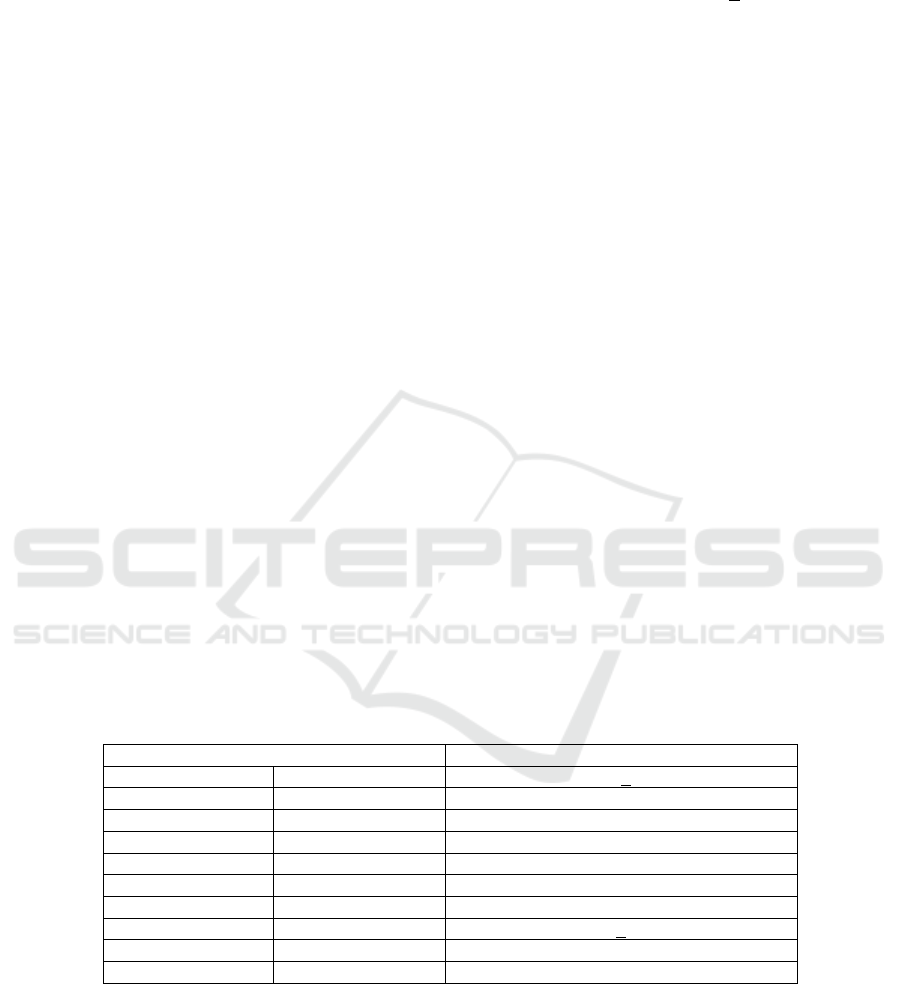
Table 1: Baseline Characteristic of Obese Individuals.
Parameters Total (mean±SD); n=80
Age (years) 38.95 + 8.13
Body weight (Kg) 75.35 ±13.49
WC (cm) 91.95 ± 9.59
LDL-C (mg/dL) 138.12 ± 32,40
HDL-C (mg/dL) 53.72 ± 16.73
TG (mg/dL) 131.30 ± 75.92
Adiponectin 4.42 ± 2.40
Chemerin (ng/mL) 408.64 + 118.41
ApoB (g/L) 98..43 ± 20.27
HOMA-IR 2.36 ± 3.02
Abbreviations: WC, waist circumference; HOMA-IR: homeostasis model assessment of insulin
resistance; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein
cholesterol; TG, triglycerides; ApoB: apolipoprotein B.
The Correlation between Apolipoprotein B Levels and Inflammatory Markers in Obese Individuals
65
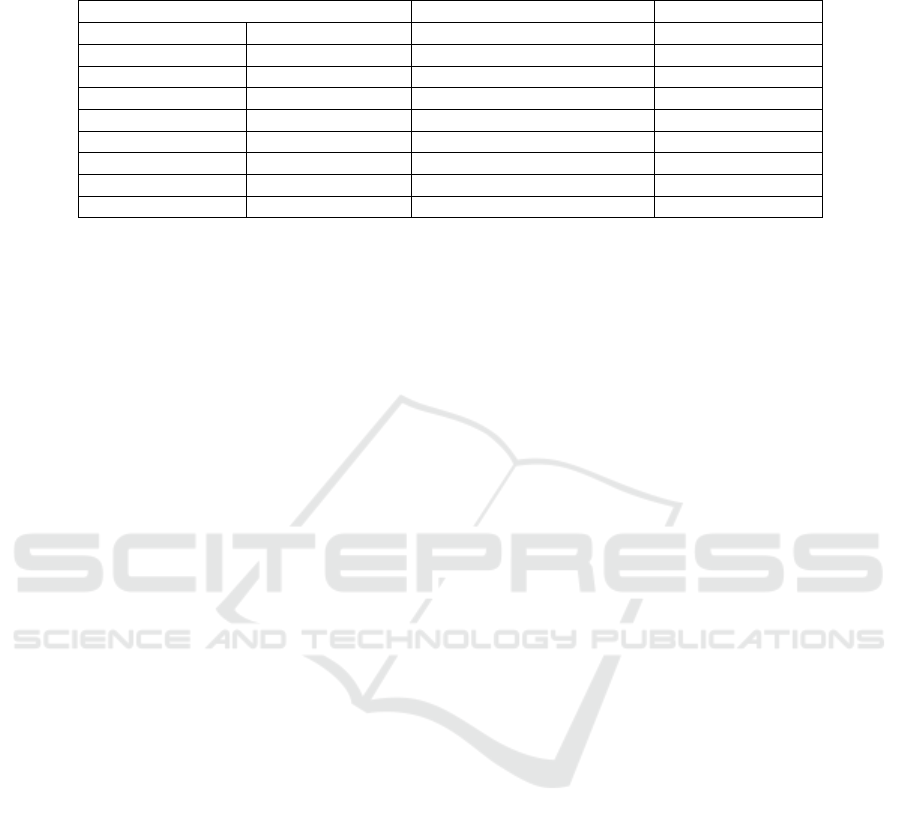
Table 2: Association between ApoB, Traditional Risk Factors of Cardiovascular Disease and Inflammatory Markers in
Obese Individuals.
Abbreviations: BMI, body mass index; WC, waist circumference; HOMA-IR: homeostasis model
assessment of insulin resistance; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density
lipoprotein cholesterol; TG, triglycerides; ApoB: apolipoprotein B.
*P<0.05, ** P <0.01
4 DISCUSSION
This study demonstrated that in obese individuals,
plasma ApoB is positively correlated with several
traditional risk factors for cardiovascular disease and
type 2 diabetes (insulin resistance, LDL-C, and TG).
ApoB is a better atherogenic parameter
compared to the traditional lipid parameters (LDL-C
and TG) because ApoB levels indicate the number
of atherogenic lipoprotein particles, such as LDL,
VLDL, and intermediate-density lipoprotein. One
cross-sectional study examined the correlation of
ApoB and the risk of coronary heart disease
(n=13,523), ApoB was found to be independently
related to the risk of CHD using Framingham risk
score (FRS) (Ryoo et al., 2011). Moreover, the
elevation of ApoB levels is also found in
normolipidemic patients with the early coronary
arterial disease even when the total and LDL-C
levels are normal (Dati and Tate, 2001).
Insulin resistance, measured with the
homeostasis index (HOMA-IR), is correlated with
ApoB as shown in this study supports the
association of insulin resistance with lipoprotein
transport. The results of the present study are in
agreement with the previous study on 476 subjects
demonstrating that ApoB was correlated with insulin
resistance (HOMA-IR) (Wang et al., 2017)
Earlier studies have shown that the
increment of plasma ApoB was associated with
inflammatory markers (hsTNF-α, IL-6, hsCRP, and
orosomucoid) (Faraj et al., 2006). Lipoprotein
thought to have triggered inflammation in humans.
However, contradicting to our findings, we did not
find the correlation between ApoB and
inflammatory markers (adiponectin and chemerin).
Schlitt et al. also found that there is no correlation
between ApoB and C-Reactive Protein (Schlitt et al.,
2005).
Our study has some limitations. Since this study
used a cross-sectional method, we could not reflect
causality. This study also did not exclude patients
who used lipid-lowering medication that could affect
the results.
5 CONCLUSION
The association between ApoB and increased
cardiovascular disease risks were related to lipid,
and insulin resistance. Thus, further prospective
studies should be used to investigate the causality
between ApoB and inflammatory markers.
REFERENCES
Adams KF, Schatzkin A, Harris TB, Kipnis V, Wouw T,
Ballard-Barbash R, et al. 2006. Overweight, obesity,
and mortality in a large prospective cohort of persons
50-71 years old. N Engl J Med, 355, pp. 763-78.
Dati F, Tate J. 2001. Reference materials for the
standardization of the Apolipoproteins A-I and B, and
lipoprotein(a). The Journal of the International
Federation of Clinical Chemistry and Laboratory
Medicine, 13, pp. 073-9.
Egusa G, Beltz WF, Grundy SM, Howard BV. 1985.
Influence of obesity on the metabolism of
apolipoprotein B in humans. J Clin Invest, 76, pp. 596-
603.
Parameter r P
Age (year) 0.209 0.063
Body weight (Kg) 0.90 0.420
WC (cm) 0.173 0.124
LDL-C (mg/dl) 0.74 0.000**
HDL-C (mg/dl) -0.33 0.001**
TG (mg/dl) 0.44 0.000**
HOMA-IR 0.31 0.005**
Adiponectin -0.23 0.410
Chemerin (ng/dl) 0.021 0.851
ICTROMI 2019 - The 2nd International Conference on Tropical Medicine and Infectious Disease
66

Ellulu MS, Patimah I, Khaza’ai H, Rahmat A, Abed Y.
2015. Obesity and inflammation: the linking
mechanism and the complications. Arch Med Sci, 13,
pp. 851-63.
Faraj M, Messier L, Bastard JP, Tardif A, Godbout A,
Prud’homme D, et al. 2006. Apolipoprotein B: a
predictor of inflammatory status in postmenopausal
overweight and obese women. Diabetologia, 49, pp
1637-46.
Gateva A, Assyov Y, Tsakova A, Kamenov Z. 2018.
Classical (adiponectin, leptin, resistin) and new
(chemerin, vaspin, omentin) adipocytokines in patients
with prediabetes. Horm Mol Biol Clin Investig, pp. 1-
9.
Holme I, Hostmark AT, Anderssen SA. 2007. ApoB but
not LDL-cholesterol is reduced by exercise training in
overweight healthy men.results from the 1-year
randomized Oslo diet and exercise study. J Intern
Med, 262, pp. 235-43.
Khadem-Ansari MH, Rasmi Y, Rahimi-Pour A,
Jafarzadeh M. 2009. The association between serum
apolipoprotein A-I and apolipoprotein B and the
severity of angiographical coronary artery disease.
Singapore Med J, 50(6), pp. 610-3.
Klop B, Elte JW, Cabezas MC. 2013. Dyslipidemia in
obesity: Mechanisms and potential targets. Nutrients,
5, pp. 1218-40.
Matthews DR, Hosker JP, Rudenski AS, Naylor BA,
Treacher DF, et al. 1985. Homeostasis model
assessment: insulin resistance and β-cell function from
fasting plasma glucose and insulin concentrations in
man. Diabetologia, 28, pp. 412–9.
Ryoo JH, Ha EH, Kim SG, Ryu S, Lee DW. 2011.
Apolipoprotein B is highly associated with the risk of
coronary heart disease as estimated by the
Framingham risk score in healthy Korean men. J
Korean Med Sci, 26, pp. 631-6.
Schlitt A, Blankenberg S, Bickel C, et al. 2005. Prognostic
value of lipoproteins and their relation to
inflammatory markers among patients with coronary
artery disease. Int J Cardiol, 102, pp. 477-85.
Tobias DK, Hu FB. 2018. The association between BMI
and mortality: implications for obesity prevention.
Lancet Diabetes Endocrinol, 6, pp. 916-7.
Wang W, Blackett P, Khan S, Lee E. 2017.
Apolipoprotein A-I, B, and C-III and obesity in young
adult Cherokee. Journal of Lipids, 2017, pp. 1-7.
The Correlation between Apolipoprotein B Levels and Inflammatory Markers in Obese Individuals
67
