
Factors That Affect Coding Quality Clinical Neoplasm Case for BPJS
Claims at "Dharmais" Cancer Hospital
Siti Rohani, Witri Zuama Qomarania and Mieke Nurmalasari
Department of Health Information Management, Universitas Esa Unggul, Jl. Arjuna Utara No. 9, Jakarta, Indonesia
Keyword: Clinical Coding Quality, Clinical Coder, Knowledge, Attitude, Training.
Abstract: The diagnosis code has a very important role for health care providers as a basis for making statisticsto find
out trends in disease and is the basis for determining the cost of health services. Accurate diagnosis codes
are very important because inaccuracies in the diagnosis code can slow the process of claiming JKN or
BPJS because they have to be revised first. In 2018 at “Dharmais” Hospital the pending outpatient file is
2782 (2%), while the pending file is hospitalized as many as 58 files (1.5%). The purpose of this study was
to analyze the influence of knowledge, attitudes and clinical coder training with the quality of clinical
coding of the Neoplasm Case for BPJS claims. The study design used is cross-sectional with 14 respondents
(total population). The results with multiple linear regression analysis, there was an influence between the
knowledge and attitudes of clinical coders on the quality of clinical coding (p-value = 0.013). The
regression equation formed is Clinical Coding Quality = -94,664 + 8,360 (Knowledge) + 4,490 (Attitude).
Knowledge is the biggest influence on the quality ofclinicalcoding.
1 INTRODUCTION
The diagnosis code has a very important role for the
health service provider as a basis for making
statistics to determine disease trends. In addition, the
diagnosis code is also the basis for determining the
cost of health services. Code diagnosis that is not
quality will cause harm to the hospital both
financially and in policymaking.(WHO 2010).
Factors that can affect the quality of the
diagnosis code include doctors, other medical
personnel (nurses) and medical record personnel
(encoders). Doctors and nurses are responsible for
the quality of the patient's medical record documents
and the encoder is responsible for the quality of the
diagnosis code based on the medicaldata.(Kemenkes
RI 2008).
Good coding skills and knowledge among coders
are very important in efforts to reduce inappropriate
coding. However, the involvement of doctors in
ensuring better documentation in admission forms
and refill summaries is also needed to reduce
inappropriate coding in hospitals(Zafirah et al.
2018).
Republic of Indonesia Decree No. 377 /Menkes
/SK/III/2007 concerning the competency standards
of the medical record profession andhealth
information states that a medical recorder must be
able to determine disease codes and actions
appropriately according to the classification in force
in Indonesia (ICD-10) regarding diseases and
actions in medical services and health management.
The role of coding is used to index disease records,
input to medical diagnosis reporting systems,
facilitate the process of storing and retrieving data
related to diagnosis of patient and service provider
characteristics, basic ingredients inthegrouping of
DRG's (diagnosis-related groups) for billing systems
for payment of service fees, national and
international reporting morbidity and mortality,
tabulation of health service data for the evaluation
process of planning medical services, determining
the form of services that must be planned and
developed according to the needs of the times,
analysis of health service financing, as well as for
epidemiological and clinical research.(Hatta 2014)
Based on an interview conducted with one of the
BPJS claim coding verifiers at the "Dharmais"
Cancer Hospital, the official stated that an accurate
diagnosis code was very important, because the
inaccuracy of the diagnosis code could slow the JKN
or BPJS claim process. After all, it had to undergo a
revision first. At the "Dharmais" Cancer Hospital
210
Rohani, S., Qomarania, W. and Nurmalasari, M.
Factors That Affect Coding Quality Clinical Neoplasm Case for BPJS Claims at "Dharmais" Cancer Hospital.
DOI: 10.5220/0009589102100214
In Proceedings of the 1st International Conference on Health (ICOH 2019), pages 210-214
ISBN: 978-989-758-454-1
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
there are still medical record files that must be
revised because the code is inaccurate or inaccurate.
The number of files that must be revised due to
inaccuracies in "Dharmais" Cancer Hospital. In 2018
the outpatient file is 2782 or around 2%, while the
inpatient file is 58 files or about 1.5%.
2 RESEARCH METHODS
This study is a quantitative study with a cross-
sectional design where exposure variable
knowledge, attitude and training and outcome
variables (clinical coding quality) are examined
simultaneously. Tools used by using questionnaires
given to Clinical Coder and observation sheets to
determine factors that influence the clinical coding
quality of neoplasm cases for BPJS claims at the
"Dharmais" Cancer Hospital. The population of this
study is outpatient Clinical Coder and inpatient
Clinical Coder who is active at the "Dharmais"
Cancer Hospital with BPJS claim file of 10% of the
performance targets per day of each Clinical Coder
Data collection using questionnaires, methods or
statistical techniques used in this study is multiple
linear regression analysis with the dependent variable
is the quality of clinical coding and the independent
variables are knowledge, attitudes and training. with
the help of an application on a computer.
3 RESULTS
3.1 Clinical Coder Knowledge
Knowledge is the result of knowing a clinical coder
on clinical coding, clinical coding implementation
and BPJS system. The following is the frequency
distribution of answers to knowledge variables
(Table 1).
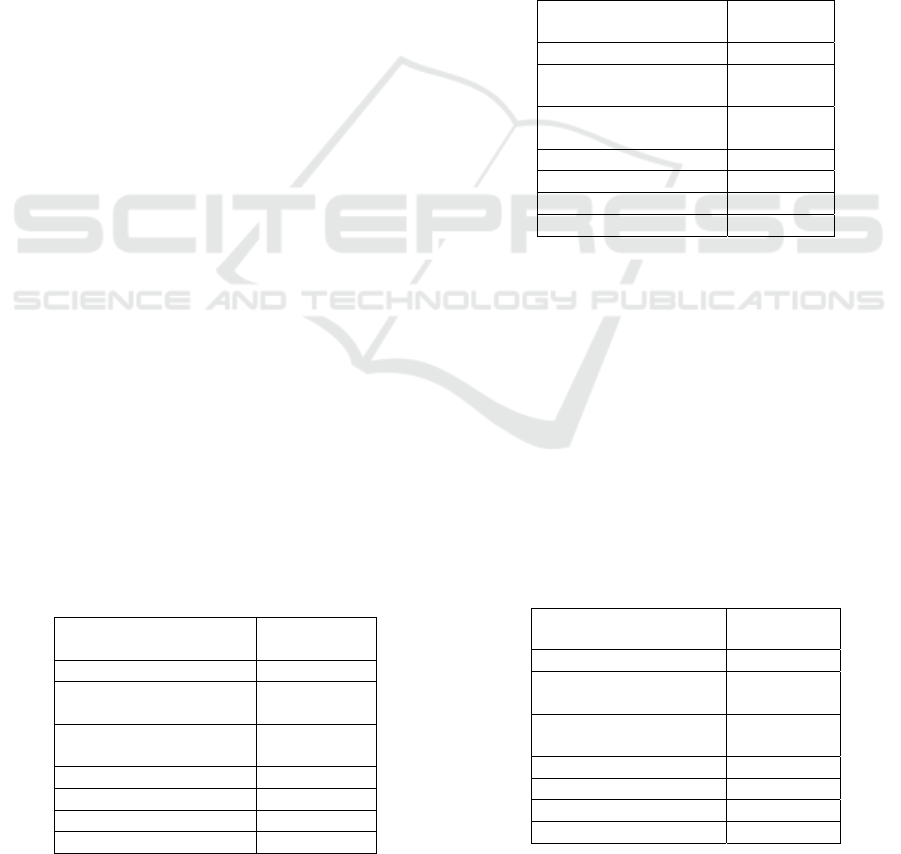
Table 1: Calculation of Total Respondents Answer Scores
Regarding Clinical Coder Knowledge in 2019.
Clinical Coder
Knowledge
Scores
Mean 8.21
95% Confidence
Interval Lower Bound
7.12
95% Confidence
Interval Upper Bound
9.30
Std. Deviation 1.888
Median 9.00
Minimum 4
Maximum 11
From the results of data processing in table 1, an
average score of data obtained is 8.21 with an
estimated interval at a 95% confidence level ranging
from 7.12 to 9.30 with a standard deviation of 1.888.
The median value is 9 and the minimum value is 4
and the maximum value is 11.
3.2 Clinical Coder Attitude
Attitude is the response of a clinical coder in
responding to an object that is organized through
experience in carrying out clinical coding of
neoplasm cases. Here is the frequency of answers
about attitude variables (Table 2).
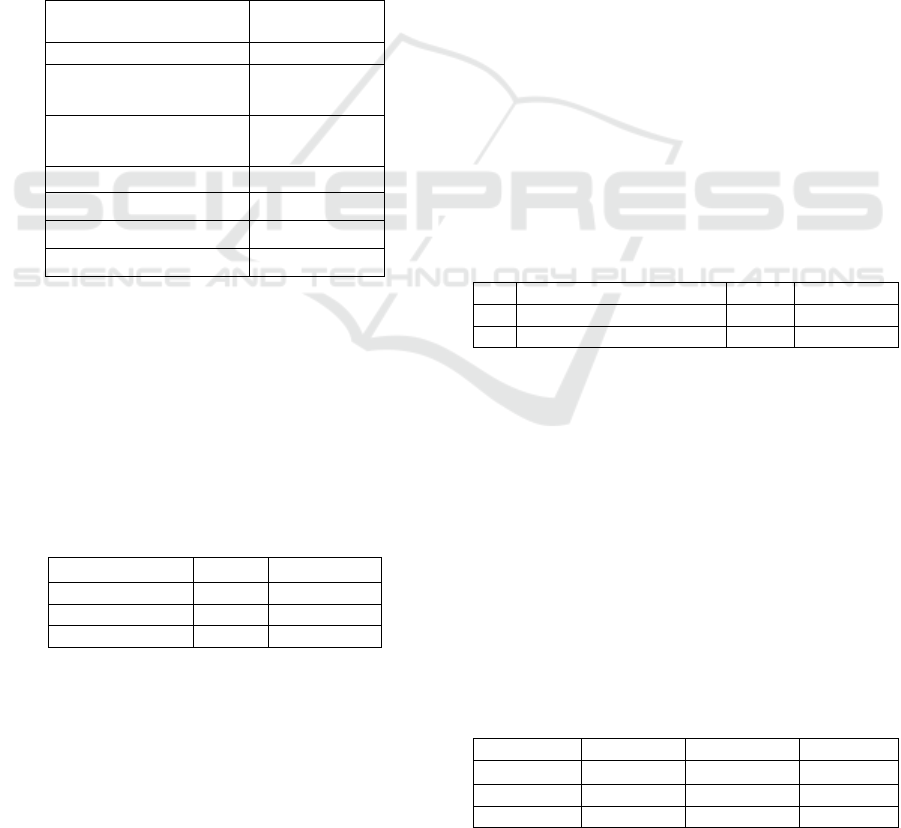
Table 2: Scores Regarding Clinical Coder Attitudes in
2019.
Clinical Coder
Attitude
Scores
Mean 21.86
95% Confidence
Interval Lower Bound
20.18
95% Confidence
Interval Upper Bound
23.53
Std. Deviation 2.905
Median 22.50
Minimum 16
Maximum 25
From the results of data processing in table 2, an
average score of 21.86 was obtained with an
estimated interval at a 95% confidence level ranging
from 20.18 to 23.53 with a standard deviation of
2.905. The median value is 22.50 and the minimum
value is 16 and the maximum value is 25.
3.3 Clinical Coder Training
Training deals with the skills and abilities needed for
the work done. The following is the frequency
distribution of training variables (Table 3):
Table 3: Calculation of Total Respondents' Answer Scores
Regarding 2019 Clinical Coder Training.
Clinical Coder Training Scores
Mean 4.07
95% Confidence
Interval Lower Bound
2.78
95% Confidence
Interval Upper Bound
5.36
Std. Deviation 2.235
Median 3.00
Minimum 0
Maximum 9
Factors That Affect Coding Quality Clinical Neoplasm Case for BPJS Claims at "Dharmais" Cancer Hospital
211
From the results of data processing in table 3, an
average score of data is obtained at 4.07 with an
estimated interval at a 95% confidence level ranging
from 2.78 to 5.36 with a standard deviationof 2.235.
The median value is 3.00 and the minimum value is
0 and the maximum value is 9.
3.4 Quality of ClinicalCoding
Clinical coding data is used for various purposes.
Among them are benchmarking, financing, clinical
and financial decision making, public health
tracking, health policy, research. The following is
the frequency distribution of clinical coding
qualityvariables (Table4).
Table 4: Calculation of Total Scores Regarding Quality of
Clinical Coding in 2019.
Quality of Clinical
Coding
Scores
Mean 72,14
95% Confidence Interval
Lower Bound
56,96
95% Confidence Interval
Upper Bound
87,32
Std. Deviation 26,291
Median 75.00
Minimum 0
Maximum 100
From the results of data processing in table 4, an
average score of 72.14 was obtained with an
estimated interval at a 95% confidence level ranging
from 56.96 to 87.32 with a standard deviation of
26.291. The median value is 75.00 and the minimum
value is 0 and the maximum value is 100.
3.5 Bivariate Analysis
Table 5: Relationship between Knowledge, Attitudes and
Clinical Coder Training with Quality of Clinical Coding.
Variable R P-Value
Knowledge 0,548 0,043
Attitude 0,432 0,123
Training 0,121 0,681
Based on table 5 it is known that:
a.
There is a significant relationship between
clinical coder knowledge with clinical coding
quality with p-value = 0.043 <0.05. The
relationship of knowledge with clinical coding
quality shows a strong relationship (r = 0.548)
and is positively patterned meaning that the
more the level of clinical coder knowledge the
greater the value of clinicalcoding
quality.(Ifalahma 2013).
b.
There is no significant relationship between
clinical coder attitude with the quality of
clinical coding with p-value =0.123>0.05.The
results of this study are in line with research by
Zubaedah (2007)which states that there is no
relationship between attitude and performance
of DBD Working Group officials with a value
of p = 0.279 (Zubaedah 2007).
c.
There was no significant relationship between
clinical coder training and clinical coding
quality with p-value =0.681>0.05.(Ali 2019)
3.6 Multivariate Analysis
3.6.1 Multivariate Modeling
Multivariate analysis was performed for the
selection if variables included in the model. When it
is included in the multivariate model, then the
variables included in the multivariate model are
variables that have a p-value <0.05. If the variable p-
value> 0.05 means it does not enter the multivariate
model. The method used is the backward method
which means looking at the value of adjusted R
square.
Table 6: Model Multivariate MethodeBackward.
No
Model
R
2
Ad
j
usted
r
2
1 Knowledge, Attitude, 0,550 0,415
2 Knowledge and Attitude 0,543 0,460
Based on the results of the table 6, it is known
that the adjusted value of r2 model 1 <model 2
(0.415 <0.460) therefore the researcher chooses the
best model used ismodel2.
3.6.2 Assumption Test
After knowing the variables included in the
multivariate model, the next step is the assumption
test. The assumptions made are, Normality Test,
Heteroscedasticity Test, Multicollinearity Test and
Autocorrelation Test.
3.6.3 Regression Equation
Table 7: Linear Regression Equations.
Variable B t P-Value
Constant -94,664 -1,924
Knowledge 8,360 2,931 0,014
Attitude 4,490 2,421 0,034
ICOH 2019 - 1st International Conference on Health
212

Based on table 7 t test results (partial), it can be
explained as follows:
1)
KnowledgeVariable
The results of the statistical test analysis revealed the
significance value (P-Value) of the knowledge
variable amounted to = 0.014. Because the P-value
=0.014 <0.05, it can be concluded that there is a
significant influence between clinical coder
knowledge and clinical coding quality.The results of
this study support previous research conducted by
Alias (2018) that knowledge has a positive and
significant effect (p-value = 0.039) on the
performance of employees at the Makassar Branch
BPJS Employment Office(Alias and Serang 2018).
2)
AttitudeVariable
The results of the statistical test analysis revealed the
significance value (P-value) of the attitude variable
amounted to = 0.034. Because the P-value = 0.034
<0.05, it can be concluded that there is a significant
influence between the clinical coder attitude and the
quality of clinical coding.This is in line with
research conducted by Wahyudi (2011) showing that
attitude significantly influences the quality of
medical records with a significant value of
0.001(Wahyudi 2011).
Based on the results of the F test
(simultaneously) it can be seen that the value of F =
6.547 and the significance value (P-value) is equal to
0.013. Because the P-value of 0.013 <0.05, it can be
concluded that there is a significant influence
between knowledge and attitudes simultaneously on
the quality ofclinicalcoding.Based on research by
Tamara (2019)also states that there is a significant
influence between knowledge, attitudes and work
experience of employees simultaneously on the
performance of employees of Islamic microfinance
institutions in Tulungagung with a significance
value = 0,000(Tamara 2019).This is in line with
research conducted by Suprapti (2004)showing that
of the three variables tested namely knowledge,
skills and attitude variables jointly influence (p-
value = 0,000) on performance variables with
indicators of quality, quantity, ability , initiative and
collaboration(Suprapti 2004).
It is found in Table 7 Value (a) = -94,664 and the
value of the regression coefficient (b1) = 8.360 and
the regression coefficient (b2) = 4.490 to obtain the
regression equation, namely:
Y = a + b1.X1 + b2.X2
Quality of Clinical Coding =
-94,664+ 8,360(Knowledge) + 4,490 (Attitude)
Based on the results of the above equation can
predict the quality of clinical coding using clinical
coder knowledge and attitudes. The meaning of the
coefficient, namely:
1)
Every knowledge of a clinical coder increases
by 1 point on condition that the value of a
constant attitude, then the quality of clinical
coding will increaseby8.360.
2)
Every attitude of a clinical coder increases by
1 point on condition that the value of
knowledge remains constant, then the quality
of clinical coding will increaseby4,490.
In the above results it can be concluded that the
variable with the greatest effect on the quality of
clinical coding is the knowledge variable.
4 CONCLUSION
a.
The results of the scores of 14 respondents who
filled out the questionnaire regarding knowledge
obtained an average score of dataof8.21 with an
estimated interval at a 95% confidence level
ranging from 7.12 to 9.30 with a standard
deviation of 1.888. The median value is 9 and the
minimum value is 4 and the maximum valueis11.
b.
The results of the score of 14 respondents who
filled out questionnaires about attitudes obtained
an average score of 21.86 data with an estimated
interval at a 95% confidence level ranging from
20.18 to 23.53 with astandard deviation of 2.905.
The median value is 22.50 and the minimum
value is 16 and the maximum value is 25.
c.
The results of the scores of 14 respondents who
filled out the questionnaire regarding training
obtained an average score of dataof4.07 with an
estimated interval at a 95% confidence level
ranging from 2.78 to 5.36 with a standard
deviation of 2.235. The median value is 3.00 and
the minimum value is 0 and the maximum value
is9.
d.
The results of the BPJS claim file assessment of
the quality of clinical coding from 14
respondents obtained an average data
scoreof72.14 with an estimated interval at a 95%
confidence level ranging from 56.96 to 87.32
with a standard deviation of 26.291. The median
value is 75.00 and the minimum value is 0 and
the maximum value is100.
e.
The influence of variable knowledge and clinical
coder attitude partially on the quality of clinical
coding for BPJS claims at the "Dharmais"
Cancer Hospital, with a significance value of
lessthan0.05.
Factors That Affect Coding Quality Clinical Neoplasm Case for BPJS Claims at "Dharmais" Cancer Hospital
213

f.
The influence of knowledge variables and
clinical coder attitude simultaneously on the
quality of clinical coding for BPJS claims at the
"Dharmais" Cancer Hospital, with a significance
valueof0.013.
REFERENCES
Ali, Mulyohadi. 2019. “Faktor-Faktor Yang Berpengaruh
Pada Akurasi Kode Diagnosis Di Puskesmas Rawat
Jalan Kota Malang.” 30(3): 228–34.
Alias, and Serlin Serang. 2018. “Pengaruh Pengetahuan,
Sikap Kerja Dan Pengalaman Kerja Terhadap Kinerja
Karyawan.” 1.
Hatta, Gemala. 2014. Pedoman Manajemen Informasi
Kesehatan Di Sarana Pelayanan Kesehatan. 3rd ed.
ed. Gemala R Hatta. Jakarta: Universitas Indonesia.
Ifalahma, Darah. 2013. “Hubungan Pengetahuan Coder
Dengan Keakuratan Kode Diagnosis Pasien Rawat
Inap Jaminan Kesehatan Masyarakat Berdasarkan
ICD-10 Di RSUD Simo Boyolali.” Jurnal Ilmiah
Rekam Medis dan Informatika Kesehatan 3(2): 14–26.
Kemenkes RI. 2008. “Peraturan Menteri Kesehatan
Republik Indonesia Nomor 269/Menkes/Per/III/2008.”
Suprapti, Wulan Martini. 2004. “Pengaruh Pengetahuan,
Ketrampilan Dan Sikap Terhadap Kinerja Pegawai
Pada Dinas Pengelolaan Sumber Daya Air Propinsi
Jawa Tengah.”
Tamara, Pingky Dwi Annisa. 2019. “Analisis Pengaruh
Pengetahuan, Sikap Dan Pengalaman Kerja Karyawan
Terhadap Kinerja Karyawan Lembaga Keuangan
Mikro Syariah Di Tulungagung.”
Wahyudi, Guridno Sri. 2011. “Pengaruh Pengetahuan,
Keterampilan Dan Sikap Pengisi Rekam Medis
Terhadap Kualitas Rekam Medis Rawat Inap Di
Rumah Sakit Daerah Kalisat Jember Tahun 2011.”
WHO. 2010. International Satistical Classification of
Diseases and Related Health Problems Tenth Revision
Volume 1,2,3. Geneva.
Zafirah, S. A., Amrizal Muhammad Nur, Sharifa Ezat
Wan Puteh, and Syed Mohamed Aljunid. 2018.
“Potential Loss of Revenue Due to Errors in Clinical
Coding during the Implementation of the Malaysia
Diagnosis Related Group (MY-DRG) Casemix System
in a Teaching Hospital in Malaysia.” BMC Health
Services Research 18(1): 1–11.
Zubaedah, Ida Siti. 2007. “Hubungan Faktor-Faktor
Sumber Daya Manusia Terhadap Kinerja Petugas
Pokja DBD Tingkat Kelurahan Di Kota Tasikmalaya.”
ICOH 2019 - 1st International Conference on Health
214
