
Contribution of Social Support to Health Belief
in Patients with Chronic Renal Failure
Sulis Mariyanti, Safira Tias Rangganis and Aziz Luthfi
Department of Psychology, Faculty of Psychology, Universitas Esa Unggul, Jakarta, Indonesia
Keywords: Social Support, Health Belief, Patients, Chronic Renal Failure, Adulthood.
Abstract: The number of patients with chronic renal failure is increasing every year. Various therapeutic treatments that
must be undertaken and the risk if not doing treatment can cause stress for patients. Patients with chronic renal
failure are required to comply with doctor's advice and can develop confidence that they will be healthy or in
other words have health beliefs. One factor that contributes to one's health beliefs is social support. The
purpose of this research was to determine the contribution of social support to health belief in patients with
chronic renal failure. The design of this research is quantitative correlational, with a purposive sampling
technique. The sample of this research were 100 patients with chronic renal failure. Social support was
measured with 36 valid items and the reliability coefficient (α) = 0.920 and the health belief were measured
with 25 items and the reliability coefficient (α) = 0.848. The results showed that social support had a positive
significant influence on health belief with a sig (p) = 0,000 (p <0.05). Social support contributed 16.4% to
health belief. Patients with chronic renal failure had more negative health beliefs (51%). Male patients have
higher health beliefs than females.
1 INTRODUCTION
Currently, health issues are a concern in Indonesia.
Based on the 2018 Rikesdas data, Indonesia has
experienced an increase in the development of non-
communicable diseases caused by the lifestyle
adopted by the community (Rossa, 2018). According
to AIA Healthy Living Index research in 2018,
healthy living activities undertaken by the Indonesian
people in 2016 were 4.0% and decreased in 2018 by
3.6%. In his research explained that the most
influential lifestyle is the lack of a person doing
physical movements such as sports and also consume
healthy food because it is considered complicated,
expensive and also a waste of time ("Research:
Indonesia's Lowest Healthy Life Index in the Asia
Pacific, "2018). This causes an increase in the
development of non-communicable diseases one of
which decreases kidney function. According to data
from the Ministry of Health 2018, chronic renal
failure ranks second as a disease that incurs a lot of
costs and life-threatening in Indonesia with growth of
almost 100% within a year, this development is
greater than other non-communicable diseases
("Potret Sehat Indonesia dari Riskesdas 2018”, 2018).
In 2018 there were 43,000,000 patients with chronic
renal failure ("Potret Sehat Indonesia dari Riskesdas
2018", 2018).
The chronic renal failure for the body, among
others, as a regulator of blood volume and
composition, formation of red blood cells, helps
maintain acid-base balance, regulates blood pressure,
expulsion of foreign components and regulates the
number of electrolyte concentrations in extracellular
fluid (Zurmeli, Bayhakki and Utami, 2006).
Meanwhile, along with increasing age and doing
unhealthy lifestyles, such as having a diet that is high
in fat and carbohydrates, lack of drinking and not
doing exercise can cause decreased organ function in
the body including kidney function (Alam, S., &
Hadibroto, I., 2007).
The chronic renal failure is a condition where the
body fails to maintain metabolism and fluid and
electrolyte balance, causing uremia (Zurmeli,
Bayhakki, & Utami, 2006). chronic renal failure is
usually caused by several diseases both from kidney
disease itself and other diseases such as diabetes and
hypertension (Tandra, 2018). In Tandra (2018),
chronic renal failure can occur gradually and also
occur suddenly. chronic renal failure that occurs
gradually usually has unclear initial symptoms so that
patients feel it when it is said to be the final stage
Mariyanti, S., Rangganis, S. and Luthfi, A.
Contribution of Social Support to Health Belief in Patients with Chronic Renal Failure.
DOI: 10.5220/0009567100970102
In Proceedings of the 1st International Conference on Health (ICOH 2019), pages 97-102
ISBN: 978-989-758-454-1
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
97

(Alam, S., & Hadibroto, I., 2007). In Tandra (2018),
when it is in its final stages that the kidneys have a
GFR below 15ml / min of normal function, actions
such as hemodialysis or kidney transplantation will be
performed. But if kidney function is still in stages 1
to 4, the condition of the kidney can be prevented by
severing lifestyle changes such as electrical
imbalance control, control of hypertension and on a
high-calorie, low-protein diet that is scheduled by the
doctor and also sports (Tandra, 2018).
According to Tandra (2018) said that there are still
patients with chronic renal failure who do not follow
the doctor's recommendations, especially in
undergoing diet and exercise. This was also stated by
a specialist consultant kidney, Aida Lydia who said
that many patients also do not take medication and
control to the doctor routinely so that it can trigger
complications and dialysis (Purba, 2019). Whether or
not the patient follows the doctor's recommendations
such as a control to the doctor routinely, does not
undergo diet and exercise and does not take
medication regularly is thought to be caused because
the patient has a negative health belief.
According to Rosenstock (Janz & Becker, 1984)
said that health belief is a belief or assessment of
behavior related to health. Assessments are obtained
through a cognitive process from information
obtained through the environment or through an
assessment process through individual experiences.
In the results of Nugraha & Nurhayati's research
(2011), stated that patients with chronic renal failure
in Al Ihsan Regional Hospital have negative health
beliefs that are characterized by irregularity in taking
medication and inconsistent dieting. The results of
interviews with patients who are suspected of having
positive health beliefs are subject M, a 60-year-old
female patient who has chronic renal failure and has
a history of diabetes. The subject said that following
the doctor's advice was not easy especially for dieting
but the subject continued to follow the doctor's advice
because he was sure his condition would improve
besides the subject was also afraid if not following the
doctor's advice his condition worsened because the
subject knew his illness was quite severe. Unlike the
56-year-old subject L, a patient who experienced
chronic renal failure and had a history of diabetes. He
does not have confidence that the existing treatment
can make it better. In addition, children from the
subject also do not support to follow the advice of
doctors. The subject did not get support so that made
the subject less motivated to carry out the treatment.
According to Rosenstock (Janz & Becker, 1984) and
based on interviews above one of the factors that
influence health beliefs are supported.
Sarafino (2002), states that social support refers to
providing comfort to others, caring for them or
appreciating them. Sarafino (2002), also said that
social support can make a patient not stressed in
dealing with his illness, makes someone able to
overcome the problem and can see the good side of
the problem he is facing. In addition, social support
makes a person stronger, more able to live a healthy
lifestyle and make others feel cared for and needed so
that someone will be encouraged to exercise, eat
healthy, not smoke and not drink alcohol. In Smet
(1994), when someone is supported by the
environment, everything will feel easier. If someone
gets social support from the environment it will make
the individual feel calm, cared for, loved, self-
confidence and competence arise (Smet, 1994). Thus
high social support is characterized by getting
attention and care coming from people around, there
are other people who support in any condition, there
is help in the form of material, physical or
psychological coming from people around, directed
about treatment, advised to follow doctor's advice,
have a place to tell stories, accompanied when going
to the hospital, have someone who can be trusted to
give advice or advice, and have a group of friends
who can provide a sense of togetherness among group
members. With the high social support from the
surrounding environment can make patients chronic
renal failure feel stronger, more excited, more
motivated to carry out treatment, patients feel cared
for, given affection from the surrounding environment,
facilitated to follow treatment because it is facilitated,
patients get the right information both from medical
personnel or the surrounding environment, there are
always other people who always provide assistance
and this is thought to make patients feel happy, happy
because someone who supports it encourages patients
to believe whatever is said by others including doctors
and families if patients follow the advice given will be
healthier and ready to follow the recommended
treatment such as taking medication regularly,
consistent in diet, doing exercise and control to the
doctor regularly. Meanwhile, low social support will
make patients chronic renal failure feel uninspired, not
motivated to carry out treatment, feel less cared for and
given affection from the surrounding environment, it is
difficult to follow a healthy lifestyle because there are
no supporting facilities, also feel alone This is thought
to cause the patient to be unsure of the advice given by
the doctor and not follow it because he feels it will not
make him healthier.
From Nugraha and Nurhayati's (2011) research on
the correlations between health belief and compliance
behavior in patients with chronic renal failure in Al
ICOH 2019 - 1st International Conference on Health
98
Ihsan Regional Hospital, which says that there is a
low relationship between health belief and
compliance behavior, which means that the more the
patient is convinced of his illness, the more the
patient's adherence to the doctor's recommendations
was also high. In addition, Khotimah Research (2014)
states that there is a correlation between family
support and health care provider support for
adherence to ARV therapy. Patients who get low
family support are proven to have a 6 times greater
risk for undisciplined taking medication than those
who get high family support. Based on the description
above, is there any influence of social support on the
health beliefs of patients with chronic renal failure
2 METHODS
This study uses quantitative research methods that are
non-experimental. This study is included in a causal-
comparative study with simple linear regression with
the aim of the study to determine the effect of social
support on health beliefs. The sample in this study
amounted to 100 patients with chronic renal failure in
Jakarta with the characteristics of a sample having a
partner, living with family and not having dialysis.
Retrieval of data in this study using a questionnaire
using a Likert scale.
Social support measurement tools are adapted
based on measuring tools made by Gidion (2010)
based on Sarafino (2002) theory. Researchers made
modifications by adding 10 items so that the initial
number of items was 60 items. After the validity test,
26 items have been dropped so that they have a total of
34 items. The reliability in this item amounted to 0.920.
While the measure of health belief is adapted from
Widyaningsih (2018) based on Rosentrock's theory (in
Janz & Becker, 1984). Researchers made
modifications by adding 12 items so that the initial
number of items was 40 items. After the validity test,
15 items have been dropped so that they have a total of
25 items. The reliability in this item amounted to 0.848.
3 RESULT
Table 1: Description of gender.
Age Frequency Precentage (%)
Early Adulthood 24 24%
Middle Adulthood 40 40%
Late Adulthood 36 36%
Total 100 100%
Most of the respondents were male, 53% and female
were 47%.
Table 2: Description of age’s respondents.
Gender Frequency Percentage(%)
Male 53 53%
Female 47 47%
Total 100 100%
Most of the respondents were middle adulthood
40%, early adulthood 24% and late adulthood 36%.
Table 3: Normality Test Result.
Variable Kolmogorof-Smirnov
Social Support 0,103
Health Belief 0,127
Kolmogorov-Smirnov One-Sample normality test
results obtained the probability of social support
0.103 and health belief 0.127.
Table 4: Simple Linear Regression.
Score Social Support and Health Belief
Konstanta B +0,308
Sig. (2-tailed)
0,000
N
100
The results of simple linear regression tests that
have been carried out in table 4 of the ANOVA results
can be seen that the value of sig. (p) 0,000 (p <0.05),
which means that there is an influence of social
support for health belief in patients with chronic renal
failure. Besides that, the constant value of B is
+0.308, which means that social support has a
positive influence on health belief, so the hypothesis
in this study is accepted. If social support is high, it
will be followed by high health beliefs.
Table 5: Categorization of Social Support.
Score Category Frequency Percentage
X ≥ 105,02 High 51 51%
X ˂ 105,02 Low 49 49%
Total 100 100%
Most respondents who have high social support as
much as 51% and low social support are 49%.
Contribution of Social Support to Health Belief in Patients with Chronic Renal Failure
99
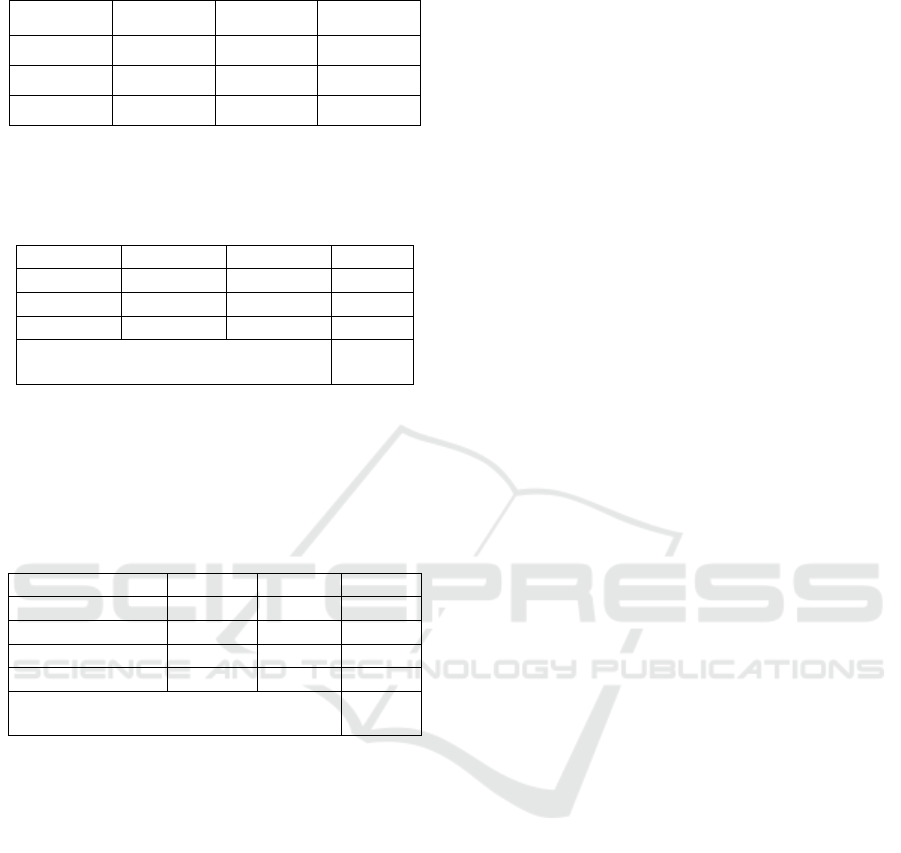
Table 6: Categorization of Health Belief.
Score Category Frequency Percentage
X ≥ 77,59 Positif 49 49%
X ˂ 77,59 Negatif 51 51%
Total 100 100%
Most respondents who have negative health
beliefs of 51% and positive health beliefs are 49%.
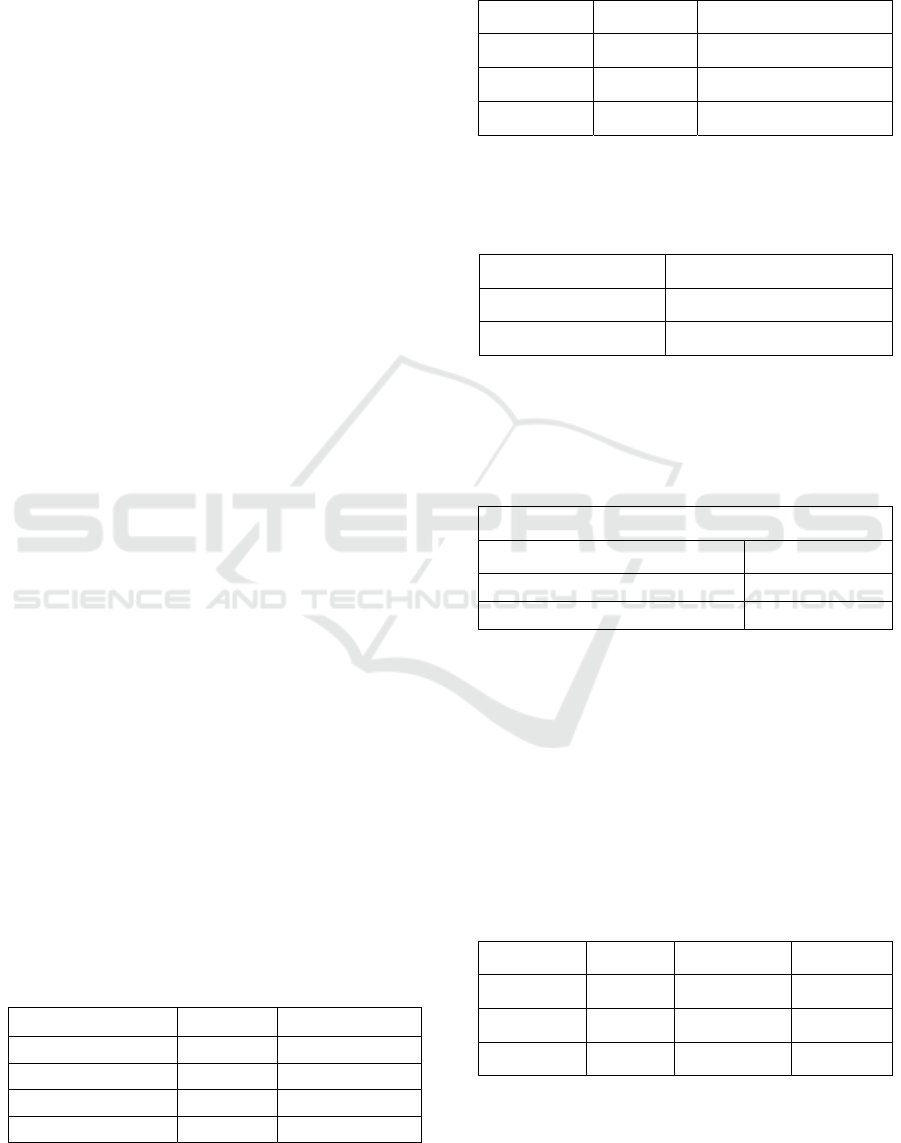
Table 7: Description of Health Belief base on Gender.
Gender
Negative Positive Total
Male
26 27 53
Female
25 22 47
Total
51 49 100
Asymp. Sig. (2-tailed)
Pearson Chi-Square
0,680
Male respondents more have positive health
beliefs and female have negative health beliefs. But
Chi-Square results obtained sig = 0.680 (p> 0.05)
which means there are no correlations between health
beliefs with the sex of the respondent.
Table 8: Description of Health Belief Base on Age.
Age
Negative Positive Total
Early Adulthood
13 11 24
Middle Adulthood
21 19 40
Late Adulthood
17 19 36
Total
51 49 100
Asymp. Sig. (2-tailed)
Pearson Chi-Square
0,573
Respondents of late adulthood more have positive
health and early adulthood and middle adulthood
more have low health beliefs. Chi-Square results
obtained sig = 0.573 (p> 0.05) which means there are
no correlations between health beliefs with the age of
the respondent.
4 DISCUSSION
In this study statistical tests with simple linear
regression obtained sig values. (p) 0,000 (p <0.05)
and the regression coefficient is +0.308 which means
the hypothesis is accepted. These results indicate that
there is a positive influence of social support on
health belief in patients with chronic renal failure.
Based on the value (R2) shows a result of 0.164 which
means that social support has a significant influence
that is 16.4%, while the rest is influenced by other
factors. The results of the linear regression equation
show the value of Y = 45.195 + 0.308x, meaning that
when social support increases by 1 then health belief
will also increase by 0.308, and vice versa if social
support decreases then health belief also decreases by
the same amount.
The results of this research are in line with
research previously conducted by Maulana (2015),
whose research results say that there is a positive and
significant influence of social support with healthy
dietary behavior in early adult women, which means
that the higher the social support, the higher the score
for healthy diet behavior. Other research was also
carried out by Irnawati, Siagian, & Ottay (2016), the
results of his study showed that social support had a
positive influence on medication adherence for
tuberculosis patients. The results of the study show
that social support influences healthy dietary
behavior and medication adherence including health
belief behavior.
A patient with chronic renal failure who gets high
social support will feel cared for, get affection, get the
right information about his illness so that makes the
patient feel happy and happy because he is taken care
of so that he is more motivated and enthusiastic in
undergoing his treatment, the patient also does not
feel alone and is stronger in fighting the disease. So
that patients have confidence that the benefits
obtained when doing treatment, believe the risks if
not doing treatment, know that the disease will be
more severe, believe the treatment can make health
conditions improve, adhere to treatment such as
regularly taking medication and a healthy diet, and
seeking information regarding his illness.
Conversely, if a patient with chronic renal failure gets
low social support, he will feel alone in dealing with
his illness, feel alienated from his environment, feel
sad so that he is not motivated and enthusiastic about
taking medication because there is no support from
his environment, and makes patients less confident
about their healthy development, they are not sure
that they will be healthier if they take medication,
they are not sure of the risks that will occur if they do
not take medication, and they are not ready to take
advice from their doctor, do not regularly take
medication and do not comply with the doctor's
recommended diet.
Sarafino (2011), said that social support can make
patients not stressed in dealing with their illnesses,
make someone able to overcome their problems,
make someone see the good side of the problem he is
facing, besides social support, makes a person
stronger, more lead a lifestyle healthy and make
others feel cared for and needed so that someone will
be encouraged to exercise, eat healthy, no smoke and
ICOH 2019 - 1st International Conference on Health
100

no drink alcohol or in other words believe in a healthy
lifestyle.
Based on the results of health belief categoriza-
tion, there are 51 people in the negative category.
Patients who have negative health beliefs will be less
sure of the risk of the disease, not ready to face
treatment and do not believe in the benefits of
treatment. In Nugraha & Nurhayati's (2011) research
results, it was stated that kidney failure patients in Al
Ihsan Regional Hospital had negative health beliefs
marked by not believing that kidney failure was a
dangerous disease, lacking confidence that patients
were able to follow the doctor's recommendations,
and lacking confidence that the disease can pose
medical risks. Health belief in Rosenstock (1974),
makes patients think that they have a serious illness
and must be cured, makes a person motivated that he
can live healthily, make someone try to avoid the
disease. Other than that. In addition, Sarafino (2011)
also said that individuals who were convinced of the
consequences of their illness, both medically,
psychologically and socially, the greater the belief
that the threat of these consequences would approach
them. This belief makes individuals encouraged to
make health recommendations such as a healthy diet
because of the many benefits gained.
One that affects one's health belief according to
Rosentrock is gender. The results of cross-tabulation
between sex and health beliefs showed a sig of 0.680
which means that there was no influence of health
beliefs with the gender of the patient chronic renal
failure. This is in line with research Hayati (2011),
which says that sex does not indicate compliance with
taking medication in pulmonary tuberculosis patients.
From cross-tabulation data with health beliefs, it is
stated that more women have negative health beliefs
than men. According to Korin, et al (2017), women
pay more attention to their health before being
exposed to the disease, while men pay more attention
to their health after being exposed to the disease. This
is because women's mindsets that change after living
a healthy lifestyle remain affected by the disease. The
results of Ulum, Widyawati, & Kusnanto (2014)
stated that men were more obedient to undergo
diabetes treatment of diabetes 2 because the number
of respondents in the study was more dominant.
Besides gender, according to Rosenstock (1974),
another demographic factor that affects health beliefs
is age. The cross-tabulation between age and health
belief shows sig. (p) as much as 0.573 (p> 0.05)
which means that there is no relationship between age
and health beliefs of patients with chronic renal
failure. According to WHO (2003), said that age and
sex have no relationship with patient compliance
following the doctor's advice in several places. In
addition, Hayati (2011) also said that there was no
relationship between age and adherence to the taking
of tuberculosis patients in pulmonary tuberculosis
patients. From cross-tabulation data between age and
health belief shows that in the early adult and middle
age groups more negative health beliefs and in the late
adult group more patients who have positive health
beliefs. This is in line with the statements of
Budiman, Khambri & Bachtiar (2013), who said that
age can affect one's motivation to adopt a healthy
lifestyle, the more age the higher the level of one's
compliance with medication or therapy.
The findings in this study are social support in this
study is high but patients have low health beliefs, it is
allegedly because it is influenced by the age factor of
the respondents. Where respondents in this study
more middle adulthood, which in theory (Hurlock,
2003), said that in middle adulthood both men and
women are having an increasingly warm relationship
with their environment but this period is also a
transition period from middle adulthood to old age
and at that time physical health began to decline but
someone has not been able to accept it.
5 CONCLUSION
Based on research that has been done, it can be
concluded that there is an influence of social support
on health belief in patients with chronic renal failure
with sig (p). 0,000 (p <0.05). With the results of the
linear regression equation, Y = 45.195 + 0.308x
shows the coefficient of variable (x) of +0.308 which
means that social support has a positive effect on
health belief which means the hypothesis is accepted.
It states that the higher the social support the more
positive the patient's health beliefs chronic renal
failure, and vice versa the lower the social support,
the lower the health beliefs owned by the patient's
chronic renal failure. Based on the R2 value shows a
result of 0.164 or 16.4%, which means social support
has an influence of 16.4% on the patient's health
belief in chronic renal failure.
From the results of this study more patients
chronic renal failure who had negative health beliefs
by 51% compared to positive. From the results of the
cross-tabulation shows that there is no relationship
between sex on one's health belief, but the data shows
that men have more positive health beliefs because
the number of respondents in this study is dominated
by men. This research also shows that age has no
correlations with the health beliefs of patients with
chronic renal failure
Contribution of Social Support to Health Belief in Patients with Chronic Renal Failure
101

REFERENCES
Alam, S., & Hadibroto, I. (2007). Gagal Ginjal. Jakarta: PT
Gramedia Pustaka Utama.
Budiman, A., Khambri, D., & Bachtiar, H. (2013).
Affecting’s factor to medication adherence of patients
with Tamoxifen after surgery. Jurnal FK Universitas
Andalas, 2(1), 20–24.
Gidion, H. (2010). Dukungan Sosial dengan Resiliensi
Pada Subyek yang Menderita Stroke (skirpsi tidak
diterbitkan) Fakultas Psikologi Universitas Indonesia,
Depok.
Hayati, A. (2011). Evaluasi Kepatuhan Berobat Penderita
Tuberkolosis Paru Tahun 2010-2011 di Puskesmas
Kecamatan Pancoran Mas Depok. (Skirpsi Fakultas
Matematika dan Ilmu Pengetahuan Alam Universitas
Indonesia). Diambil dari http://lib.ui.ac.id-20205393-
S121-Evaluasi-Kepatuhan/
Hurlock, E. B. (2003). Psikologi Perkembangan: Suatu
Pendekatan Sepanjang Rentang Kehidupan (Edisi 5).
Jakarta: Erlangga.
Irnawati, N. M., Siagian, I. E. T., & Ottay, R. I. (2016).
Pengaruh Dukungan Keluarga Terhadap Kepatuhan
Minum Obat pada Penderita Tuberkulosis di
Puskesmas Motoboi Kecil Kota Kotamobagu. Jurnal
Kedokteran Komunitas Dan Tropik, IV, 59–64.
Janz, N. K., & Becker. (1984). The Health Belief Model: A
Decade Later reprint requests to. Health Education
Quarterly, 11(1), 1–47. Retrieved from https://journals.
sagepub.com/doi/pdf/10.1177/109019818401100101
Khotimah, M. (2014). Hubungan Antara Dukungan
Keluarga dan Peran Petugas Kesehatan dengan
Kepatuhan Minum Obat Kusta di Kabupaten Blora
Tahun 2011. Unnes Journal of Public Health, 3(2), 1–
5. Retrieved from http://journal.unnes.ac.id/sju/
index.php/ujph
Korin, M. R., Chaplin, W. F., Shaffer, J. A., Butler, M. J.,
Ojie, M. J., & Davidson, K. W. (2017). Public Access
NIH Public Access. Health Educ Behav, 32(7), 736–
740. https://doi.org/10.1371/journal.pone.0178059
Maulana, D. H. (2015). Pengaruh dukungan sosial dan
health belief model terhadap perilaku diet sehat pada
wanita dewasa awal. (Skripsi Fakultas Psikologi
Universitas Negeri Syarif Hidayatullah). Diambil dari
http://repository.uinjkt.ac.id/
Nugraha, S., & Nurhayati, R. (2011). Hubungan Health
Belief dengan Perilaku Compliance pada Pasien Gagal
Ginjal Kronis di RSUD Al Ihsan. Prosiding Penellitian
Civitas Akademika Unisba (Sosial Dan Humaniora),
2, 30–39. https://doi.org/10.1017/CBO9781107415
324.004
Potret Sehat Indonesia dari Riskesdas 2018. (2018,
November). Depkes.Go.Id. Retrieved from
http://www.depkes.go.id/
Purba, T. A. (2019, March). Hari Ginjal Sedunia, Ayo
Cegah Penyakit Ginjal Sejak Dini.
Bisnis.Com.
Retrieved from https://lifestyle.bisnis.com/
Riset: Indeks Hidup Sehat Penduduk Indonesia Terendah di
Asia Pasifik. (2018, December). Kumparan.Com.
Retrieved from https://kumparan.com/
Rosenstock, I. M. (1974). The Health Belief Model and
Personal Health Behavior. Health Education
Monographs, 2(4), 354–386. https://doi.org/10.1177/
014572178501100108
Rossa, V. (2018, November). Hasil Riskesdas 2018,
Penyakit tidak menular semakin meningkat.
Suara.Com. Retrieved from https://www.suara.com/
health/2018/11/02/101437/hasil-riskesdas-2018-penya
kit-tidak-menular-semakin-meningkat
Sarafino, E. P. (2002). Health Psychology: Biopsychosocial
Interactions. New York: John Wiley & Sons Inc.
Sarafino, E. P. (2011). Health Psychology: Biopsychosocial
Interactions (7th ed.). United States of America: John
Wiley & Sons Inc.
Smet, B. (1994). Psikologi Kesehatan. Jakarta: Grasindo.
Tandra, H. (2018). Dari Diabetes Menuju Ginjal. Jakarta:
Gramedia Pustaka Utama.
Ulum, Z., Widyawati, I. Y., & Kusnanto. (2014).
Kepatuhan Medikasi Penderita Diabetes Mellitus Tipe
2 Berdasarkan Teori Health Belief (HBM) Di Wilayah
Kerja Puskesmas Mulyorejo Surabaya. Jurnal
Keperawatan, 3(1), 64–74.
WHO. (2003). Adherence to long-term therapies: Evidence
for action (Vol. 2). https://doi.org/10.1016/S1474-
5151(03)00091-4
Widyaningsih, T. H. (2018). Gambaran Health Belief
Pengkonsumsi Mie Insan Pada Mahasiswa (skripsi
tidak diterbitkan) Fakultas Psikologi Universitas Esa
Unggul, Jakarta
Zurmeli., Bayhakki., & Utami, G. T. (2006). Hubungan
Dukungan Keluarga Dengan Kualitas Hidup Pasien
Gagal Ginjal Kronik Yang Menjalani Terapi
Hemodialisis Di Rsud Arifin Achmad Pekanbaru.
Jurnal Keperawatan. 670-681. diambil dari
http://jom.unri.ac.id
ICOH 2019 - 1st International Conference on Health
102
