
Detection of Factors That Influence Preeclampsia in Pregnant
Women
Erlina Hayati
1
, Husna Sari
1
, G. F. Gustina Siregar
1
, Stefani Anastasia S.
1
, Fitriani
2
1
Faculty of Midwifery, Deli Husada Deli Tua Health Institute
2
Postgraduate of Public Health North Sumatra University
Keywords: Parity, Preeclampsia, Pregnant Woman.
Abstract: Preeclampsia and eclampsia are health problems that require special attention because they are as causes death
of pregnant women and high perinatal. This research type was analytical study with case control design. The
population of this research were all pregnant women who check their womb at Sembiring General Hospital.
The sampling technique used random sampling method. The research sample consisted of 62 pregnant women
consisting of 31 cases and 31 controls in which the case group were pregnant women diagnosed with
preeclampsia and the control group were pregnant women diagnosed with no preeclampsia. Primary data
collection methods obtained through direct interviews with research subjects. The research instruments were
standardized questionnaires. Data analysis used univariate analysis, bivariate with chi-square test and
multivariate analysis with multiple logistic regression tests. The research sample consisted from 31 cases and
31 controls. The results showed that respondents who experienced preeclampsia were 29 people with
abnormal weight gain and among respondents who did not experience preeclampsia there were 33 people with
normal weight gain. Chi square test results obtained p value <0.05, it shows that there was an influence of
weight gain on preeclampsia incidence in pregnant women. Obtained OR = 8.338 means that pregnant women
who have preeclampsia have 8.338 times chance of having abnormal weight gain compared to women who
don't have preeclampsia.
1 INTRODUCTION
Maternal Mortality Rate (MMR) is one indicator to
see the degree of women's health. United Nations
International Children's Emergency Founder
(UNICEF) (2015) states every year nearly 10,000
women die due to pregnancy and childbirth problems.
Preeclampsia is the second cause after bleeding
as specific immediate cause of maternal death, on the
other hand the incidence of eclampsia in developing
countries is around 1 case per 100 pregnancies to 1
case per 1700 pregnancies. In African countries, the
preeclampsia incidence is around 1.8% to 7.1%, in
Nigeria, the prevalence is around 2% to 16.7 and the
cause of preeclampsia is not only caused by one factor,
but many factors that cause preeclampsia and
eclampsia ( S. Shoda et al; Gerda G. Zeeman, ; Lars J.
Vatten & Rolv Skjærven ; M Knight,Osungbade,
2015).
Some experts conclude that women with better
socioeconomic conditions will suffer from
preeclampsia less often, without regard it,
preeclampsia suffered by women from capable family
can still be as severe and life-threatening as eclampsia
that affects women at slums (Carl A. Hubel et al.,
1989; Gordon CS Smith et al., 2002; Baha M Sibai,
2003; James M. Roberts & Hilary S. Gammill, 2005;
Richard J. Levine et al, ; Mary Beth Terry et al., 2016;
Labib Ghulmiyyah & Baha M Sibai, 2012;
Cunningham, 2016).
Risk factors of preeclampsia include age, parity,
weight gain during pregnancy, physical activity and
socioeconomic. Control of risk factors plays an
important role in connection with the preeclampsia
prevention. Early diagnosis of preeclampsia with
careful handling gives good prognosis. Preeclampsia
which is handled too late give the worst impact that is
death for mother and fetus (Chobanian, 2016).
The above data illustrates that the problem of
preeclampsia needs to get attention and good
handling, considering the high prevalence and quite
severe complications and knowledge in the
community that is still lacking in handling the
preeclampsia problem in pregnant women and can get
Hayati, E., Sari, H., Siregar, G., S., S. and Fitriani, .
Detection of Factors That Influence Preeclampsia in Pregnant Women.
DOI: 10.5220/0009472402550261
In Proceedings of the International Conference on Health Informatics and Medical Application Technology (ICHIMAT 2019), pages 255-261
ISBN: 978-989-758-460-2
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
255
a more precise picture then research is needed to know
the factors which influence occurence in pregnant
women.
2 METHODOLOGY
The research type was analytic study with case
control design. The study was conducted from
January to July 2018. The population of this study
were all pregnant women who examined the womb at
Sembiring General Hospital. The sample consisted of
62 pregnant women consisting of 31 cases and 31
controls in which the case group consisted of
pregnant women who were diagnosed with
preeclampsia and control group of pregnant women
who were diagnosed with no preeclampsia.
The sampling technique used random sampling.
Primary data collection methods obtained through the
distribution of questionnaires directly on the research
subjects. The research instruments were standardized
questionnaires. Data analysis used univariate
analysis, bivariate with chi-square test and
multivariate analysis with regression tests multiple
logistics.
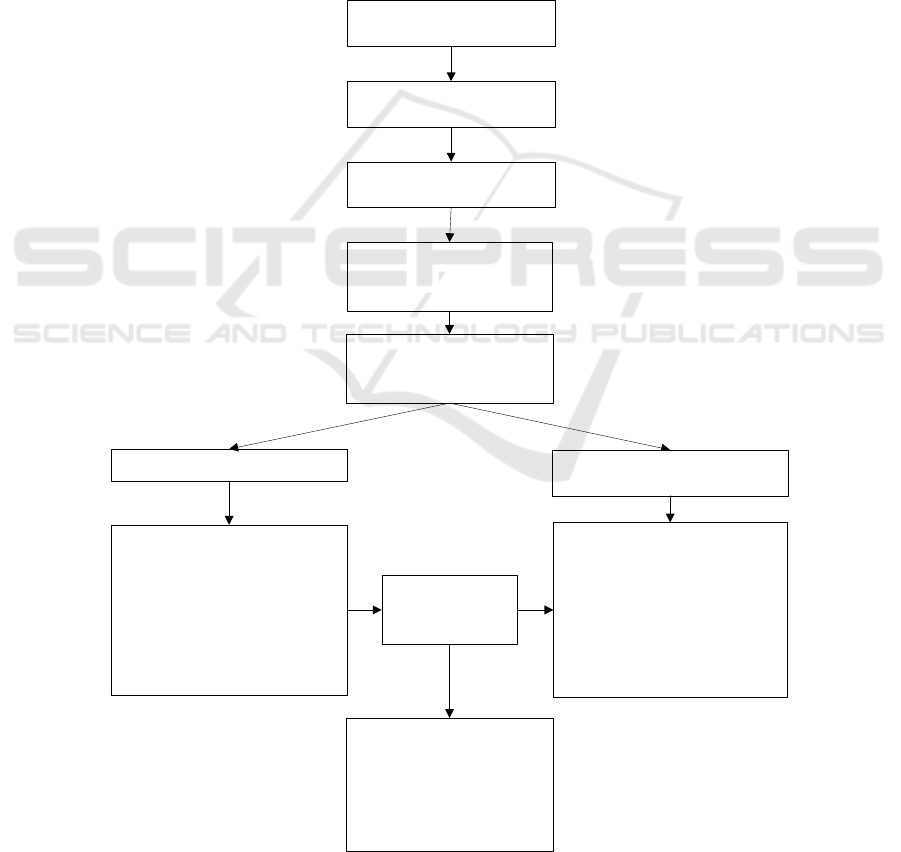
The research roadmap is as follows:
Preeclamsia Case
Case Control Design
Research period between
January-July 2018
Research respondent were
determined using Random
Sampling Method
Analitics Study
Inclusion criteria in the case
respondent are:
1 Pregnant woman suffer from
preeclamsia
2. Pregnant women with a
gestational age above 20 weeks
3. pregnant women live in Deli
Serdang district
Inclusion criteria in the control
Sample are :
1. Pregnant women who do not
experience preeclamsia
2. Pregnant women with a
gestational age above 20 weeks
3. Pregnant women live in Deli
Serdang district
Cases respondent : 31 persons
Data collection:
Interview and
Quetionnaire
Data analysis:
Univariate analysis,
bivariate analysis with chy-
square test, and multivariate
analysis with multiple
logistic regression test
Control respondent : 31 persons
Figure 1: Research Roadmap
ICHIMAT 2019 - International Conference on Health Informatics and Medical Application Technology
256
3 RESULTS AND DISCUSSION
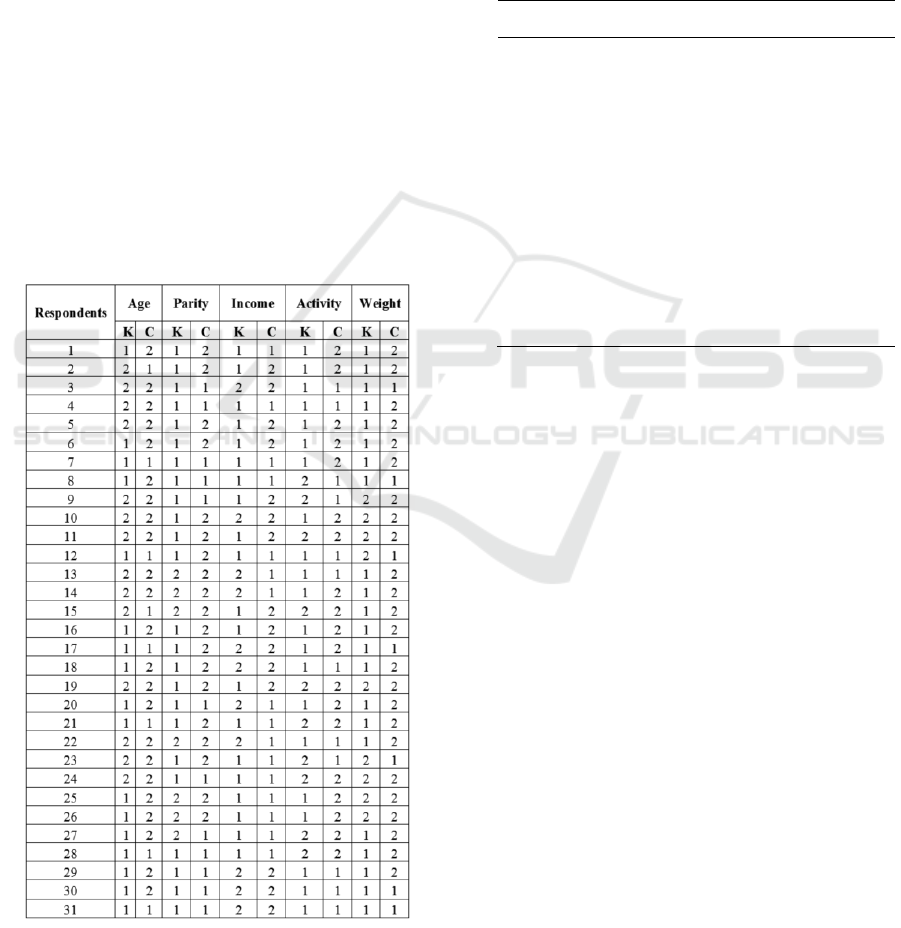
Table 1: Detection Respondents Data of Factors that
Influence the Preeclampsia Occurrences in Pregnant
Women
Note : Table :
K = Case
C = Control
Total of respondents = 62 Respondents
Based on above table, it can be explained that:
a. age: if 1 is <20 and 2 is> 35 years old 20-35
years old,
b. Parity is given by code 1 Primipara and code
2. Multipara,
c. Income is given code 1 <CMW and code 2
for ≥ CMW,
d. Activity is given code 1 Weight (PAL value
1.70-2.40) and given code 2 for the easy
category (PAL value 1.40-1.69),
e. Weight is given code 1 for not Normal (<7
and> 12kg) and code 2 for normal (7-12 kg).
Physical activity can be grouped into three
groups, namely:
a. Easy (activity types 25% of time is used for
sitting or standing, 75% for standing or
moving) or PAL value 1.40 - 1.69
b. Medium (activity types 40% of time is used
for sitting or standing, 60% for standing or
moving) or PAL value 1.70 - 1.99
c. Weight (activity types 75% time used for
sitting or standing, 25% to stand or move) or
PAL value 2.00 - 2.40
Respondents
PAL
Depends on chair or bed
1,2
Sitting job with little or no choice to
move and little or no reaction
activity
1,4 –
1,5
Sitting job with must move and little
or no reaction activity.
1,6 -
1,7
Standing work
1,8
Intensive reaction activities with a
significant amount (> 3 times a
week)
+ 0,3
Heavy manual work or very active
reaction activities.
2,0-2,4
Questions and data collected are taken based on
the results of data collection such as the respondents’
identities which there are questions namely income,
number of children and weight gain during pregnancy
and physical activity.
Based on the study results note that the majority
of pregnant women who experience preeclampsia
under age 20 and above 35 years old are 29 people
from the study respondents, and those aged 20 to 35
years are 10 respondents. Respondents with income
above City Minimum Wage (CMW) are 20 people.
While the majority of pregnant women who do not
experience preeclampsia are age 20 to 35 years old,
as many as 24 people and with an income above the
CMW, as many as 16 people.
The results obtained data that the majority of
pregnant women who experience preeclampsia with
abnormal weight gain where pregnant women have
weight gain below 7 kg and above 12 kg are 38
people, while the majority of pregnant women who
do not experience preeclampsia with normal weight
gain where the mother pregnant who have weight
gain between 7 to 12 kg are 24 people.
It is also known from the study results that age
and income variables do not affect the preeclampsia
incidence. If we look at the age variable, it is known
that among respondents who experienced
Detection of Factors That Influence Preeclampsia in Pregnant Women
257

preeclampsia there were 17 mothers with age under
20 years or over 35 years and among respondents who
did not experience preeclampsia were 23 mothers
with ages 20-35 years.
The woman reproductive age is 20 to 35 years.
It is the safest period for pregnancy and childbirth
because at that age the risk of complications during
pregnancy is lower. Age less than 20 years and above
35 years are also referred as high-risk age to
experience complications during pregnancy. At the
age less than 20 years, the uterus size has not reached
the normal size for pregnancy, so the possibility of
disruption in pregnancy such as preeclampsia
becomes greater. At the age over 35 years, it occurs
degenerative processes that results structural and
functional changes in peripheral blood vessels that are
responsible for changes in blood pressure, so they are
more vulnerable to experiencing preeclampsia
(Gafur, 2011).
If we see income variable, based on the study
results there is no difference between mothers with
income ≥ CMW and mothers with income <CMW in
their influence toward preeclampsia incidence, it is
possible because high and low income does not
guarantee what kind of food will be consumed by
pregnant women and depends on the frequency of
eating and other factors.
Physical activity does not significantly
influence the preeclampsia incidence. The study
results indicate that among respondents who
experienced preeclampsia there are 21 mothers with
strenuous physical activity and among respondents
who do not experience preeclampsia there are19
mothers with easy physical activity.
Based on the study results, it can be assumed
that easy and heavy activities do not affect the
preeclampsia incidence for pregnant women. It may
be due to physical activity experienced by pregnant
women is difficult to measure by using questionnaire
and observation needs to be done so that in this study
found how physical activities carried out daily during
pregnancy.
Physical activity does not significantly
influence the preeclampsia incidence. The study
results indicate that among respondents who
experienced preeclampsia there are 21 mothers with
strenuous physical activity and among respondents
who do not experience preeclampsia there are19
mothers with easy physical activity.
From the research, it is known that weight
gain affects the preeclampsia incidence. The results
showed that among respondents who experienced
preeclampsia with abnormal weight gain there were
22 thousand cases and 7 mothers of controls and
among respondents who did not experience
preeclampsia with normal weight there were 9 people
from cases and 24 people from controls.
Table 2: Analysis Results of Multiple Logistic Regression
Test
Variable
B
Sig.
Exp (B)
95% CI
Age
0,72
0,273
2,060
0,566-
7,494
Parity
1,40
0,026
4,087
1,181-
14,139
Physical
Activity
0,22
0,746
1,252
0,322-
4,869
Weight
Gain
1,67
0,019
5,310
1,323-
21,306
Constant
1,98
0,001
0,137
Age
0,70
0,285
2,015
0,557-
7,287
Parity
1,43
0,022
4,200
1,225-
14,399
Weight
Gain
1,77
0,005
5,896
1,698-
20,479
Constant
1,92
0,001
0,146
Parity
1,46
0,019
4,328
1,271-
14,742
Weight
Gain
1,95
0,001
7,067
2,120-
23,557
Constant
1,76
0,002
0,171
After it is done multivariate analysis, it was
found that there were four research variables that
entered the candidates, namely age, parity, physical
activity and weight gain. The most dominant variable
influence the preeclampsia incidence in pregnant
women at Sembiring Hospital was weight gain, which
has Exp B value of 7.067 meaning that pregnant
women who experience preeclampsia had chance of
7.067 times having abnormal weight gain compared
to pregnant women who did not experience
preeclampsia.
The data is presented in the table below:
Table 3: The Effect of Weight Gain on the Preeclampsia
Incidence
Weight
Gain
Preeclampsia Incidence
P
value
OR
(95
%
CI)
Cases
Control
N
%
N
%
Abnormal
Normal
22
9
71,0
29,0
4
22,6
77,4
<
0,001
8,6
32
Total
31
100
1
100
ICHIMAT 2019 - International Conference on Health Informatics and Medical Application Technology
258

The cross tabulation analysis results of weight
gain toward the preeclampsia incidence obtained that
among respondents who experienced preeclampsia
were 22 people (71.0%), mothers with abnormal
weight gain and among respondents who did not
experience preeclampsia were 24 people (77.4%)
mothers with normal weight gain. Chi square test
results obtained p value <0.05, it showed that there
was effect of weight gain on the preeclampsia
incidence in pregnant women at Sembiring General
Hospital. It is obtained OR = 8.338 means that
pregnant women who have preeclampsia have 8.3381
chance of having an abnormal weight gain compared
to women who don't have preeclampsia.
One of the abnormal weight gain risk for
pregnant women is preeclampsia (E. R. Hillesund et
al., 2018; Ernawati et al., 2018; Jovian M Wat et al.,
2018; Y Sherf et al., 2019).
Preeclampsia is estimated occur in five percent
pregnancies and it usually appears after 20 weeks'
gestation. It is more common in the first pregnancy.
If preeclampsia has occurred, prevention efforts are
made so that it doesn’t become more severe. Disease
recognition and antenatal testing play important role
in avoiding death and the possible risk factors.
(Octaviana Yoseffin, 2011; Jennifer A. Hutcheon et
al, 2018; Lisa M. Bodnar et al, 2018; Marianne
Lønnebotn et al, 2018; Argyro Syngelaki et al, 2019).
Multivariate analysis was performed to analyze
the effect of independent variables on the
characteristics of pregnant women (age, parity and
income), physical activity and weight gain with
dependent variables (preeclampsia events) at
Sembiring General Hospital. Multivariate analysis
used multiple logistic regression analysis. Before
conducting multivariate analysis, the selection of
variables which will become candidates for the
multivariate model is done first. Variables that
become multivariate candidates are independent
variables with p values <0.25 in bivariate analysis. It
is known that from five variables, three of them
should be included as model candidates, namely
parity, activity and weight gain toward the
preeclampsia incidence in pregnant women.
Table 4: Selections of Model Candidates for
Multivariate Modelling Phase
No
Variable
p value
1.
Age
0,038*
2.
Parity
0,005*
3.
Income
0,440
4.
Activity
0,042*
5.
Weight Gain
< 0,01*
After multivariate analysis, it was found that
there were four research variables that entered the
candidates, namely age, parity, physical activity and
weight gain. The most dominant variable influence
the preeclampsia incidence in pregnant women at
Sembiring General Hospital is weight gain, which has
an Exp B value of 7.067 meaning that pregnant
women who experience preeclampsia have chance of
7.067 times having abnormal weight gain compared
to pregnant women who did not experience
preeclampsia.
After multivariate analysis, it was found that
there were four research variables that entered the
candidates, namely age, parity, physical activity and
weight gain. The most dominant variable influence
the preeclampsia incidence in pregnant women at
Sembiring General Hospital is weight gain, The
percentage correct value obtained 74.2% means age,
parity, physical activity, and weight gain variables
explain the effect on the preeclampsia incidence in
pregnant women at Sembiring General Hospital as
much as74.2%, while the remaining 25.8% is
influenced by other factors which are not included in
this research variable.
Variables that are proven did not have effect on
the preeclampsia incidence namely age, income and
physical activity, it is recommended:
a. It is hoped that the government and relevant
agencies review existing programs by
emphasizing the importance of ANC (Ante Natal
Care) counseling to primigravida pregnant
women for early detection of the preeclampsia
risk and how to prevent it early
b. It is hoped that health workers will be more
active in providing health education to pregnant
women to increase understanding about
preeclampsia dangers, especially for
primigravida mothers and pregnant women with
abnormal weight gain to periodically carry out
pregnancy checks and conduct special
examinations (laboratory tests) routinely such as
blood and urine tests so that they can be detected
early. If abnormalities are found related to the
maternal pregnancy condition, especially to
monitor maternal blood pressure and other
examinations to monitor the preeclampsia
symptoms so that immediate action can be taken
if problems are found related to maternal
pregnancy, besides that it is needed to keep blood
pressure within normal limits during pregnancy
and how to prevent it from an early age by
regulating the weight of pregnant women to stay
in ideal conditions and still maintain adequate
and balanced nutrition.
Detection of Factors That Influence Preeclampsia in Pregnant Women
259

c. For further researchers are expected to conduct
further research to find out other variables that
are thought as the influence of preeclampsia
occurrence.
4 CONCLUSIONS
It can be concluded that variable which is
proven to influence the preeclampsia incidence is
weight gain. Referring to the frequency distribution
of weight gain respondents, study results showed the
majority of pregnant women who experience
preeclampsia with abnormal weight gain.
a. Variables that are proven influence the
preeclampsia incidence are parity and weight
gain.
b. Variables that are proven do not have effect on
preeclampsia incidences are age, income and
physical activity.
c. Weight gain is proven become the most
influential factor on preeclampsia incidence in
pregnant women with Exp B value of 7.067 (95%
CI; 2.120-23.557) which means pregnant women
who have preeclampsia have 7.067 times chance
to experience excess weight gain compared to
pregnant women who do not experience
preeclampsia.
Chi square test results obtained p value
<0.05, it shows that there is an effect of weight gain
on the preeclampsia incidence in pregnant women at
Sembiring General Hospital. It is obtained OR =
8.338 means that pregnant women who have
preeclampsia have 8.3381 chance for having an
abnormal weight gain compared to women who don't
have preeclampsia.
ACKNOWLEDGEMENT
This research was supported by Health Institut of Deli
Husada Deli Tua, Health Institut of Medistra Lubuk
Pakam, Sembiring General Hospital Foundation, and
Grand Medistra Indonesia.
REFERENCES
Bodnar, L. M., Himes, K. P., Abrams, B., Parisi, S. M., &
Hutcheon, J. A. 2018. Early-pregnancy weight gain and
the risk of preeclampsia: A case-cohort study.
Pregnancy hypertension, 14, 205-212.
Cuningham, F. G. 2016. Obstetri william. Alih Bahasa:
Andry Hartono, Joko Suyono, Brahm U. Pendit.
Jakarta: ECG.
Denantika, O., Serudji, J., Revilla, G. 2015. Hubungan
Status Gravida dan Usia Ibu terhadap Kejadian
Preeklamsia di RSUP Dr.M. Djamil Padang. Jurnal
Kesehatan Andalas, diakses tanggal 10 Juni 2016
;http://jurnal.fk.unand.ac.id.
Dian, O., Serudji, J., Revilla, G. 2015. Hubungan Status
Gravida dan Usia Ibu terhadap Kejadian Preeklamsia di
RSUP Dr.M. Djamil Padang. Jurnal Kesehatan
Andalas, diakses tanggal 20 Juni 2017
;http://jurnal.fk.unand.ac.id.
Dennysantoso, 2016 Memilih Makanan Sehat Untuk
Masyarakat, 2011, Diakses tanggal 10 Februari 2016;
http//www.blogspotdennysantoso.com.
Departemen Kesehatan Republik Indonesia. Profil
Kesehatan Provinsi Sumatera Utara Tahun 2018.,
Medan.
Departemen Kesehatan Republik Indonesia. Profil
Kesehatan Provinsi Sumatera Utara Tahun 2019.,
Medan
Departemen Kesehatan Republik Indonesia. Profil
Kesehatan Provinsi Sumatera Utara Tahun 2019.,
Medan.
Depkes RI, 2018, Hipertensi Penyebab Kematian Nomor
Tiga. Kementerian Kesehatan.RI.Jakarta.-
http://www.depkes.go.id/index.php/-berita/press-
release/810-
Derek Lewellyn-jones, Dasar-dasar obstetric dan
ginekologi, Alih bahasa;Hadyanto, Ed.6 Jakarta,
Ernawati, E., Erliana, E., Sulistono, A., Joewono, H. T.,
Akbar, M. A., Wicaksono, B., ...& Etika, R. 2018. 53.
Expectant management of severe preeclampsia in a
developing country: Maternal outcomes and perinatal
survival. Pregnancy Hypertension, 13, S19.
Erliana, E., Sulistono, A., Joewono, H. T., Akbar, M. A.,
Wicaksono, B., ...& Etika, R. 2018. 53. Expectant
management of severe preeclampsia in a developing
country: Maternal outcomes and perinatal survival.
Pregnancy Hypertension, 13, S19
Fajarwati Paramitasari. 2017. Hubungan antara gaya hidup
selama masa kehamilan dan kejadian preeklamsia di
Puskesmas Waru Sidoarjo, The Indonesian Journal Of
public Health Universitas Airlangga Surabaya.Vol.8 :
122-125
Gafur, A., Nurdin, A., Ramadhany, S., & Rahim, M. R.
2017. Hubungan antara primigravida dengan
preeklampsia. Makassar: Universitas Hasanuddin.
Ghulmiyyah, L., & Sibai, B. 2016, February. Maternal
mortality from preeclampsia/eclampsia.In Seminars in
perinatology (Vol. 36, No. 1, pp. 56-59). WB Saunders.
Gonçalo Miguel Peres, Melissa Mariana and Elisa Cairrão,
Januari 2018. Pre-Eclampsia and Eclampsia: An Update on
the Pharmacological Treatment Applied in Portugal
Hillesund, E. R., Seland, S., Bere, E., Sagedal, L. R.,
Torstveit, M. K., Lohne-Seiler, H., ...& Øverby, N. C.
2018. Preeclampsia and gestational weight gain in the
Norwegian Fit for Delivery trial. BMC research notes,
11(1), 282.
ICHIMAT 2019 - International Conference on Health Informatics and Medical Application Technology
260

Hubel, C. A., Roberts, J. M., Taylor, R. N., Musci, T. J.,
Rogers, G. M., & McLaughlin, M. K. Lipid
peroxidation in pregnancy: new perspectives on
preeclampsia. American journal of obstetrics and
gynecology, 161(4), 1025-1034.
Hutcheon, J. A., Stephansson, O., Cnattingius, S., Bodnar,
L. M., Wikström, A. K., & Johansson, K. 2018.
Pregnancy weight gain before diagnosis and risk of
preeclampsia: a population-based cohort study in
nulliparous women. Hypertension, 72(2), 433-441.
Knight, M. Eclampsia in the united kingdom 2016. BJOG:
An International Journal of Obstetrics & Gynaecology,
114(9), 1072-1078.
Levine, R. J., Lam, C., Qian, C., Yu, K. F., Maynard, S. E.,
Sachs, B. P., ... & Karumanchi, S. A. 2006. Soluble
endoglin and other circulating antiangiogenic factors in
preeclampsia.New England Journal of Medicine,
355(10), 992-1005.
Lønnebotn, M., Natvig, G. K., Benediktsdóttir, B., Burgess,
J. A., Holm, M., Jógi, R., ...& Franklin, K. A. 2018.
Polycystic ovary syndrome, body mass index and
hypertensive disorders in pregnancy.Pregnancy
hypertension, 11, 32-37.
Osungbade, K. O., & Ige, O. K. 2016. Public health
perspectives of preeclampsia in developing countries:
implication for health system strengthening. Journal of
pregnancy, 2016.
Rachael Fox , Jamie Kitt, Paul Leeson, oktober 2019.
Preeclampsia: Risk Factors, Diagnosis, Management,
and the Cardiovascular Impact on the Offspring.
Risthiana, D. 2016. Hubungan Antara PreeklampsiaBerat
dengan Asfiksia Neonatorum di RSUD Ponogoro per 1
Januari 2017-31 Desember 2017
Roberts, J. M., & Gammill, H. S. 2016. Preeclampsia:
recent insights. Hypertension, 46(6), 1243-1249.
Sherf, Y., Sheiner, E., Shoham Vardi, I., Sergienko, R.,
Klein, J., & Bilenko, N. 2019. Like mother like
daughter: low birth weight and preeclampsia tend to
reoccur at the next generation. The Journal of Maternal-
Fetal & Neonatal Medicine, 32(9), 1478-1484.
Sibai, B. M. 2017. Diagnosis and management of
gestational hypertension and preeclampsia.Obstetrics
& Gynecology, 102(1), 181-192.
Sutrimah, Mikbakhuddin, Wahyuni. D, 2014 .Faktor-
Faktor yang Berhubungan dengan Kejadian
Preeklamsia pada Ibu Hamil di Rumah Sakit Roemani
Muhammadiyah Semarang.
Syngelaki, A., Sequeira Campos, M., Roberge, S., Andrade,
W., & Nicolaides, K. H. 2019. Diet and exercise for
preeclampsia prevention in overweight and obese
pregnant women: systematic review and meta-analysis.
The Journal of Maternal-Fetal & Neonatal Medicine,
32(20), 3495-3501.
Smith, G. C., Stenhouse, E. J., Crossley, J. A., Aitken, D.
A., Cameron, A. D., & Connor, J. M. 2016. Early
pregnancy levels of pregnancy-associated plasma
protein a and the risk of intrauterine growth restriction,
premature birth, preeclampsia, and stillbirth. The
Journal of Clinical Endocrinology & Metabolism,
87(4), 1762-1767.
Sohda, S., Arinami, T., Hamada, H., Yamada, N.,
Hamaguchi, H., & Kubo, T.
1997.Methylenetetrahydrofolate reductase
polymorphism and pre-eclampsia.Journal of medical
genetics, 34(6), 525-526.
Sutrimah, Mikbakhuddin, Wahyuni. D, 2014 .Faktor-
Faktor yang Berhubungan dengan Kejadian
Preeklamsia pada Ibu Hamil di Rumah Sakit Roemani
Muhammadiyah Semarang.
Syngelaki, A., Sequeira Campos, M., Roberge, S., Andrade,
W., & Nicolaides, K. H. 2019. Diet and exercise for
preeclampsia prevention in overweight and obese
pregnant women: systematic review and meta-analysis.
The Journal of Maternal-Fetal & Neonatal Medicine,
32(20), 3495-3501.
Tamher S, 2017 Kesehatan Usia Lanjut dengan Pendekatan
Asuhan Keperawatan, Salemba Medika, Jakarta.
Terry, M. B., Perrin, M., Salafia, C. M., Zhang, F. F.,
Neugut, A. I., Teitelbaum, S. L., ...& Gammon, M. D.
2017. Preeclampsia, pregnancy-related hypertension
and breast cancer risk. American journal of
epidemiology, 165(9), 1007-1014.
Tina Fajarwati Paramitasari. 2017. Hubungan antara gaya
hidup selama masa kehamilan dan kejadian
preeklamsia di Puskesmas Waru Sidoarjo, The
Indonesian Journal Of public Health Universitas
Airlangga Surabaya.Vol.8 : 122-125
Trijatmo Rachimhadbi .2016. Preeklamsia dan
Eklaamsia Jakarta:Yayasan Bina Pustaka Sarwono
Prawiroharjo.
Vatten, L. J., & Skjærven, R. 2016. Is pre‐ eclampsia more
than one disease?.BJOG: An International Journal of
Obstetrics & Gynaecology, 111(4), 298-302.
Wat, J. M., Hawrylyshyn, K., Baczyk, D., Greig, I. R., &
Kingdom, J. C. 2018. Effects of glycol-split low
molecular weight heparin on placental, endothelial, and
anti-inflammatory pathways relevant to
preeclampsia.Biology of reproduction, 99(5), 1082-
1090.
Wati, Risthiana, D. 2016. Hubungan Antara
PreeklampsiaBerat dengan Asfiksia Neonatorum di
RSUD Ponogoro per 1 Januari 2017-31 Desember 2017
Yoseffin, O. 2017.Correlations of Chronic Periodontitis
with Preeclampsia and Fetal Birth Weight.Indonesian
Journal of Obstetrics and Gynecology.
Zeeman, G. G., Fleckenstein, J. L., Twickler, D. M., &
Cunningham, F. G. 2015. Cerebral infarction in
eclampsia.American journal of obstetrics and
gynecology, 190(3), 714-720.
zoseffin, O. 2017.Correlations of Chronic Periodontitis
with Preeclampsia and Fetal Birth Weight.Indonesian
Journal of Obstetrics and Gynecology.
Detection of Factors That Influence Preeclampsia in Pregnant Women
261
