
A Symptom Distribution Method in Global Knowledge to Medical
Expert System
Widyastuti Andriyani
1
, Samekto Wibowo
2
, Laurentinus Sandhi Prasetya
3
and Istianto Kuntjoro
4
1
Master of Information Technology, STMIK AKAKOM, Jl. Raya Majapahit No. 143 Karangjambe, Yogyakarta, Indonesia
2
Department of Neuroscience, Universitas Gadjah Mada, Yogyakarta, Indonesia
3
Department of Anesthesiology, Panti Rapih Hospital, Yogyakarta, Indonesia
4
Fakulty of Medicine, Universitas Kristen Duta Wacana, Yogyakarta, Indonesia
Keywords:
Emergency unit, medical records, knowledge base, global knowledge, specialist doctors.
Abstract:
Changes to services in the medical field will follow the changing of era, no longer relying on a single expert but
can adapt to multiple experts, by offering convenience to help emergency room doctors and specialist doctors.
The technology that will be discussed in this research is building a framework of knowledge of large-scale
medical experts. Knowledge is obtained by relying on medical record data as the results of that knowledge
that are used to distribute the symptoms according to specialist units in the hospital. Therefore, doctors who
are in the emergency unit can do first aid to patients as well as to get the appropriate specialist information
based on a knowledge-based system with the patient’s condition, so that the work of the emergency room
doctor and specialist doctors can utilize the knowledge-based system in conducting care in patients and can
save observation time in examining other patients.
1 INTRODUCTION
In today’s digital era, a lot of research has been done
to develop a system towards digitalization. One part
of computer science that can help make work eas-
ier is artificial intelligence (AI) (Dzierzanowski et al.,
1985). An expert system is a part of AI that is built
based on expert knowledge and information from
books (Gorzalczany and McLeish, 1992). In its ap-
plication, expert systems are often used to diagnose
problems that occur in the community. One of the
development of expert systems is to help in the med-
ical field (Dzierzanowski et al., 1985). During its
development, many systems were built using AI to
improve medical services (Krantz et al., 1988) and
(Cota et al., 2017), decision support (Razzouk et al.,
2006) – and (Navarra, 2016), to assist in diagnos-
ing diseases (Dzierzanowski et al., 1985), (Adlassnig
and Scheithauer, 1989), (Malmir et al., 2017). The
software that was successful in applying AI into the
medical field to diagnose diseases in the 20th cen-
tury included MYCIN, SPHINX, LOCALIZE (Brazis
et al., 2012), PUFF, INTERNIST, and GAITSPERT
(Dzierzanowski et al., 1985), (Chorbev et al., 2009).
AI which is a field of science has many branches that
can be applied in the medical field. This can be seen
in the success of various software that uses differ-
ent methods(Dzierzanowski et al., 1985). MYCIN
has succeeded in becoming a system based on ex-
pert systems that is able to help medical staff provide
clinical consultations (Van Remoortere, 1979), (Li,
2010), SPHINX uses inference and pattern recogni-
tion methods capable of providing consultations re-
lated to jaundice (Sampat et al., 2005), to the IN-
TERNIST which is able to provide diagnoses in vari-
ous diseases (Miller et al., 1982).
In developing AI for medical purepose it is insep-
arable from the role of medical personnel and doc-
tors directly. The combination of knowledge pos-
sessed by experts in the medical field with comput-
ing is an expert system. The expert system was de-
veloped from a simple display that was still in the
form of a command-line interface (CLI) (“Classifica-
tion and diagnosis of diabetes: Standards of medical
care in Diabetesd2018,” 2018) until finally a graphical
user interface (GUI) version was developed that made
it easy for users to interact with the system (Gianni
et al., 2019). Even Bao, et al. (Schiller and Mandvi-
walla, 2007) has been able to develop an expert sys-
tem that can be used in several hospitals in rural ar-
Andriyani, W., Wibowo, S., Prasetya, L. and Kuntjoro, I.
A Symptom Distribution Method in Global Knowledge to Medical Expert System.
DOI: 10.5220/0009431100490058
In Proceedings of the International Conferences on Information System and Technology (CONRIST 2019), pages 49-58
ISBN: 978-989-758-453-4
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
49

eas by using virtual machines that are connected to a
network. Further development of the expert system
that is connected to the network allows patients to do
longdistance consultations with several doctors or ex-
perts who are included in a system (Chambers and
Conway, 1992).
The use of expert systems in the medical field it-
self is divided into several types, namely expert sys-
tems based on rules or logic and expert systems based
on mathematical or statistical computations (Liao,
2005).
2 LITERATURE REVIEW
In improving the accuracy of expert system diagnos-
tics in the health sector, researchers conducted a com-
bination of rule-based and statistical-based. This sec-
tion will discuss previous studies related to the expert
system in its application in the health sector or medi-
cal expert system. The expert system was developed
using a rule-based method, based on statistics, or a
combination of both.
2.1 Rule-based (Logic- based) Expert
System
An expert system based on logic leads to a manipula-
tion of objects rather than mathematical computations
(Dzierzanowski et al., 1985), (“Foundations of neural
networks, fuzzy systems, and knowledge engineer-
ing,” 1997), (Herry and Frize, 2003). This is more
due to understanding between the problem domain
and the knowledge held by experts (Dzierzanowski
et al., 1985), (Li, 2010), (Albert et al., 2015). Fur-
thermore, the expert system that is built will greatly
affect the health of the lives of patients (Hyeon et al.,
2016). Knowledge from experts which is applied to
a rule-based expert system is capable of representing
the relationship between problems and consequences
that will occur (Adlassnig and Scheithauer, 1989) in
the form of IFTHEN (Gianni et al., 2019). The ability
to represent these relationships is obtained based on a
logical approach from real-world cases that are trans-
ferred from expert knowledge (Aronson et al., 2005).
The use of rule-based expert systems in the medical
field provides ease in enhancing system capabilities.
If one day the expert has a new experience or the ex-
pert’s knowledge increases in disease, then the rules
can be changed according to expert knowledge. For
example, there are rules which are deleted or added in
the diagnosis of disease to achieve better diagnostic
results, but the addition or deletion of rules cannot be
done instantly but requires verification and validation
so that the expert system that is built remains stable
(Schiller and Mandviwalla, 2007).
In addition to making the expert system that is
built remain stable, verification and validation are also
needed so that every rule and fact stored in the knowl-
edge base is still true and honestly made based on ex-
pert knowledge. Poor accuracy and incomplete rules
are of great concern in the validation of a rulebased
expert system (Lockwood and Chen, 1995), (Eya-
dat and Alsmadi, 2012). However, rule-based expert
systems have drawbacks, one of which is limitations
when the system is unable to explain or make a rule
against disease diagnosis so that it is combined with
several other methods in AI such as fuzzy logic (Sut-
ton et al., 2012) and (Das et al., 2013), data mining
(Mihaela-Adina and Gheorghis
˘
a, 2015) , (Fefilatyev
et al., 2007) and semantics (Sakorn, 2016).
CONRIST 2019 - International Conferences on Information System and Technology
50
space
Figure 1: Rule-Based Medical Expert System.
2.2 Quantity Measure based (Statistics
based) Expert System
Expert systems that are based on mathematical com-
putations arise because some researchers consider
that sometimes the systems are not able to make
or explain a rule to achieve the correct diagno-
sis. The development of expert systems of this type
uses mathematical methods such as Bayesian for-
mulas (Sapna and Tamilarasi, 2009), artificial neu-
ral networks (Yahia et al., 2000), data mining tech-
niques (Mihaela-Adina and Gheorghis
˘
a, 2015), and
optimization (Mihaela-Adina and Gheorghis
˘
a, 2015).
The use of expert systems based on mathematical
computations provides a jump in accuracy and a jump
in the speed of the diagnostic process. Mathematical
computations are not used to replace the rule-based
expert system, but rather to accomplish and improve
performance to cover the deficiencies that exist. Al-
though the system is capable of providing a good
spike in performance, but the use of expert systems
based on mathematical computations is limited to hu-
man ability to label (Valizadegan et al., 2013). This
can trigger debate from other medical personnel who
have different views based on knowledge and views
held (Sadideen et al., 2013). A simple example is a
usage of genes or offspring as a parameter or label in
making a diagnosis (Gay et al., 2013) and (Dharmar
et al., 2002).
Figure 2: Statistics-Based Medical Expert systems.
2.3 Medical Expert Systems Category
Technology development in the world of health is im-
portant. Starting from the examination process, di-
agnosis, to the patient care process must be done with
extreme care and precision. This becomes a challenge
for young doctors and paramedics who are just start-
ing a career in doing so, especially in dealing with
problems with a high degree of difficulty. Artificial
intelligence is a part of technologies that enables the
development of medical tools for junior paramedics
and doctors who are experienced in solving problems
they faced (Dharmar et al., 2002). One part of artifi-
cial intelligence that is often used in the development
of these tools is the expert system (Dzierzanowski
et al., 1985), (Dharmar et al., 2002), (Tan et al., 2016).
The development of expert systems themselves can
be divided into several categories including diagnosis,
repair, instruction, interpretation, prediction, forecast-
ing, design and planning, monitoring, control, classi-
fication/identification, discovery, debugging, and se-
lection (Tan et al., 2016).
2.3.1 Diagnosis
Diagnosis in the world of health requires compre-
hensive medical knowledge because sometimes the
causes of the disease (symptoms) can vary making it
difficult for patients to identify their health conditions
(Sakorn, 2016). An expert system that is capable of
making the right diagnosis is expected to be able to
help patients and medical staff in making a diagnosis.
A Symptom Distribution Method in Global Knowledge to Medical Expert System
51
2.3.2 Repair
Repair in the medical expert system is referred to as a
system that is capable of providing solutions in treat-
ment for patient recovery.
2.3.3 Instruction
Instruction in the expert system is capable of provid-
ing a sequence of handling of disease.
2.3.4 Interpretation
The interpretation referred to in this medical expert
system is a system capable of processing input from
users both experts, medical personnel, and patients to
be able to provide diagnosis results and good treat-
ment recommendations.
2.3.5 Prediction
The ability of the expert system developed is in mak-
ing predictions about what will happen. Prediction
generated by the system can be in the form of disease
progression towards positive or negative.
2.3.6 Design and Planning
The system is capable of providing a framework and
work plan for handling patients based on the results
of the system’s diagnosis of disease. Planning and
handling generated by the system can be knowledge
given by experts at the time of manufacture and the
results of learning the system (if the expert system
can learn).
2.3.7 Monitoring and Control
The capability of the expert system is in monitoring
patient conditions and comparing them with previous
conditions. Then the system is capable of providing
new treatment solutions to the development of the pa-
tient’s condition. Such monitoring and control capa-
bilities are very helpful for medical personnel in han-
dling patients who must be monitored closely and in
detail.
2.3.8 Classification and Identification
Classification is the ability of an expert system to
classify the type of disease to the patient’s condition.
While identification is the capability of an expert sys-
tem in recognizing patients from their symptoms.
2.3.9 Discovery
In the development, there is an expert system that is
capable of recognizing and/or discovering a new type
of disease based on symptoms and the development
of the patient’s condition.
2.3.10 Discovery
Expert systems with this category are expert systems
that are capable of fixing errors both independently
and with the help of experts.
Figure 3: The Use of Medical Expert System.
CONRIST 2019 - International Conferences on Information System and Technology
52
space space
A Symptom Distribution Method in Global Knowledge to Medical Expert System
53
space space
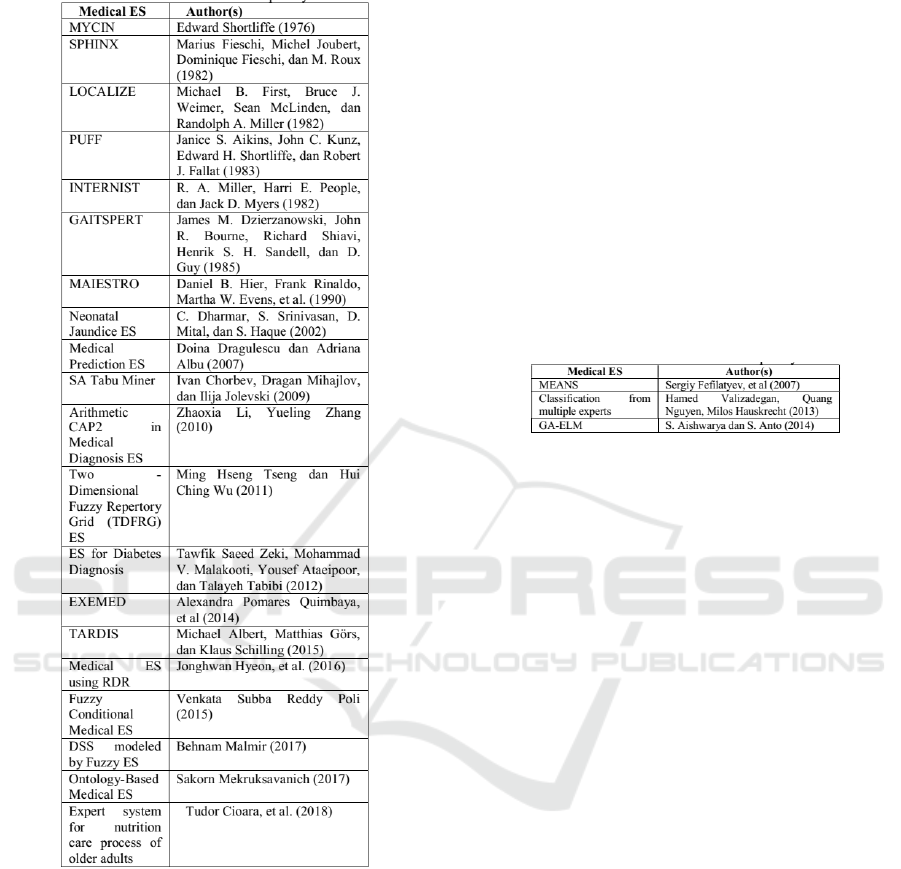
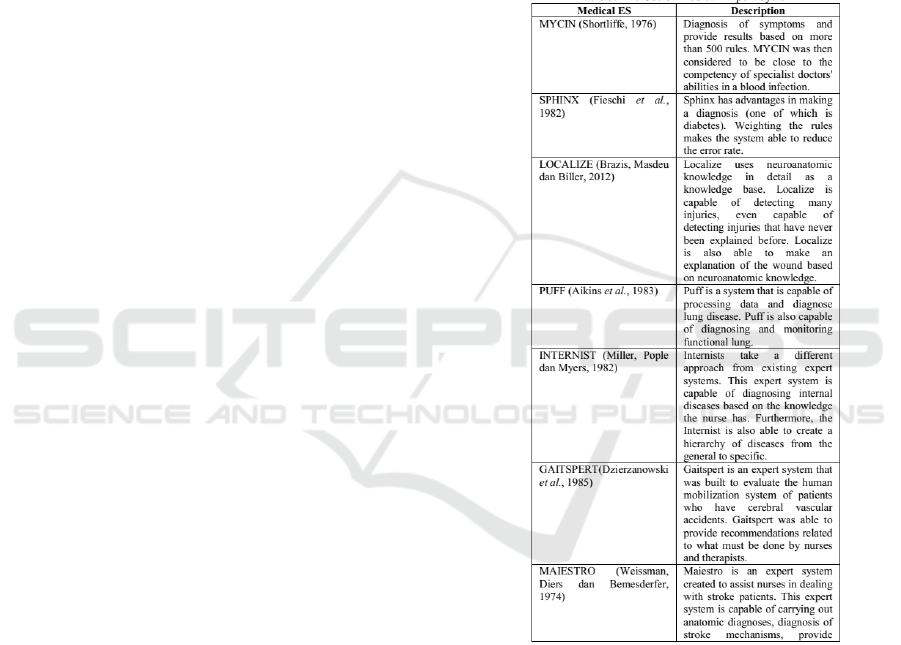
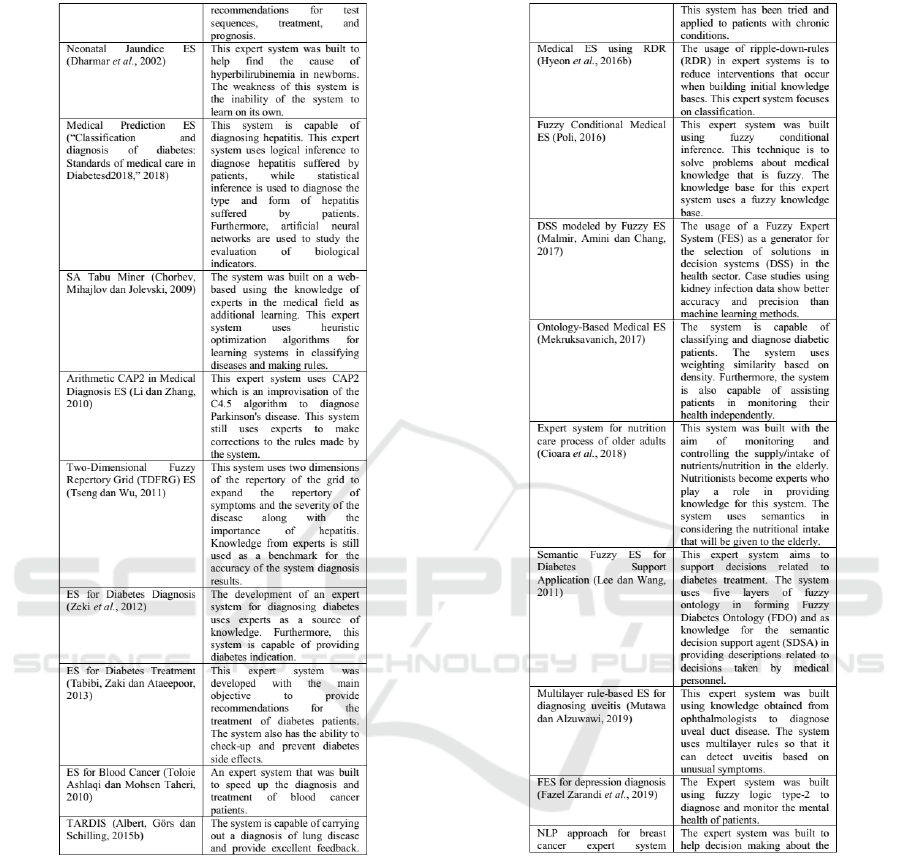
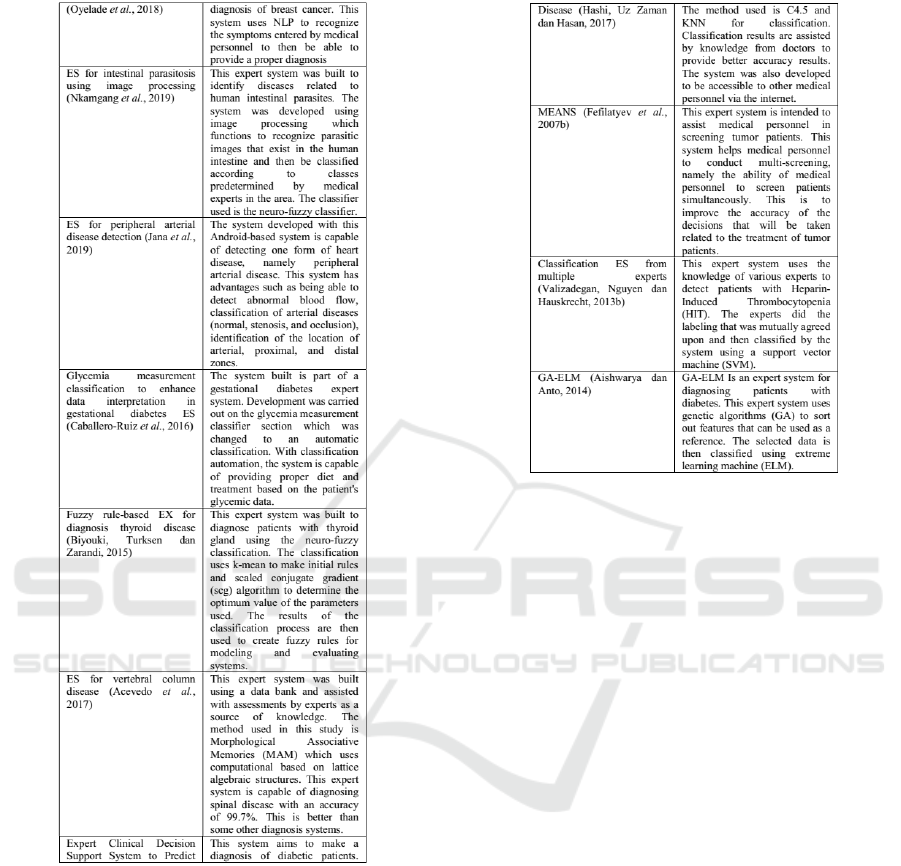
Source of Figure 3 : (Shortliffe, 2012), (Fieschi
et al., 1982), (Brazis et al., 2012), (Aikins et al.,
1983), (Miller et al., 1982), (Dzierzanowski et al.,
1985), (Weissman et al., 1974), (Dharmar et al.,
2002), (Chorbev et al., 2009), (Li, 2010), (Tseng and
Wu, 2011), (Zeki et al., 2012), (Tabibi et al., 2013),
(Toloie and Mohsen, 2010), (Albert et al., 2015),
(Hyeon et al., 2016), (Poli, 2015), (Malmir et al.,
2017), (Sakorn, 2016), (Cioara et al., 2018), (Lee and
Wang, 2010), (Mutawa, 2019), (Biyouki et al., 2015),
(Oyelade et al., 2018), (Nkamgang et al., 2019), (Jana
et al., 2019), (Estefania et al., 2016), (Biyouki et al.,
2015), (Elena et al., 2016), (Hashi et al., 2017), (Fefi-
latyev et al., 2007), (Valizadegan et al., 2013), (Aish-
warya and Anto, 2014).
3 GROUP EXPERT
This research will propose a group expert system
model (GDSS) that can be used in the Emergency
Unit (ER). The GDSS is capable of diagnosing patient
symptoms, physical examinations, and the anamne-
sis, and distribute the results of diagnoses to special-
ist doctors so that they can be followed up faster and
better.
CONRIST 2019 - International Conferences on Information System and Technology
54
space
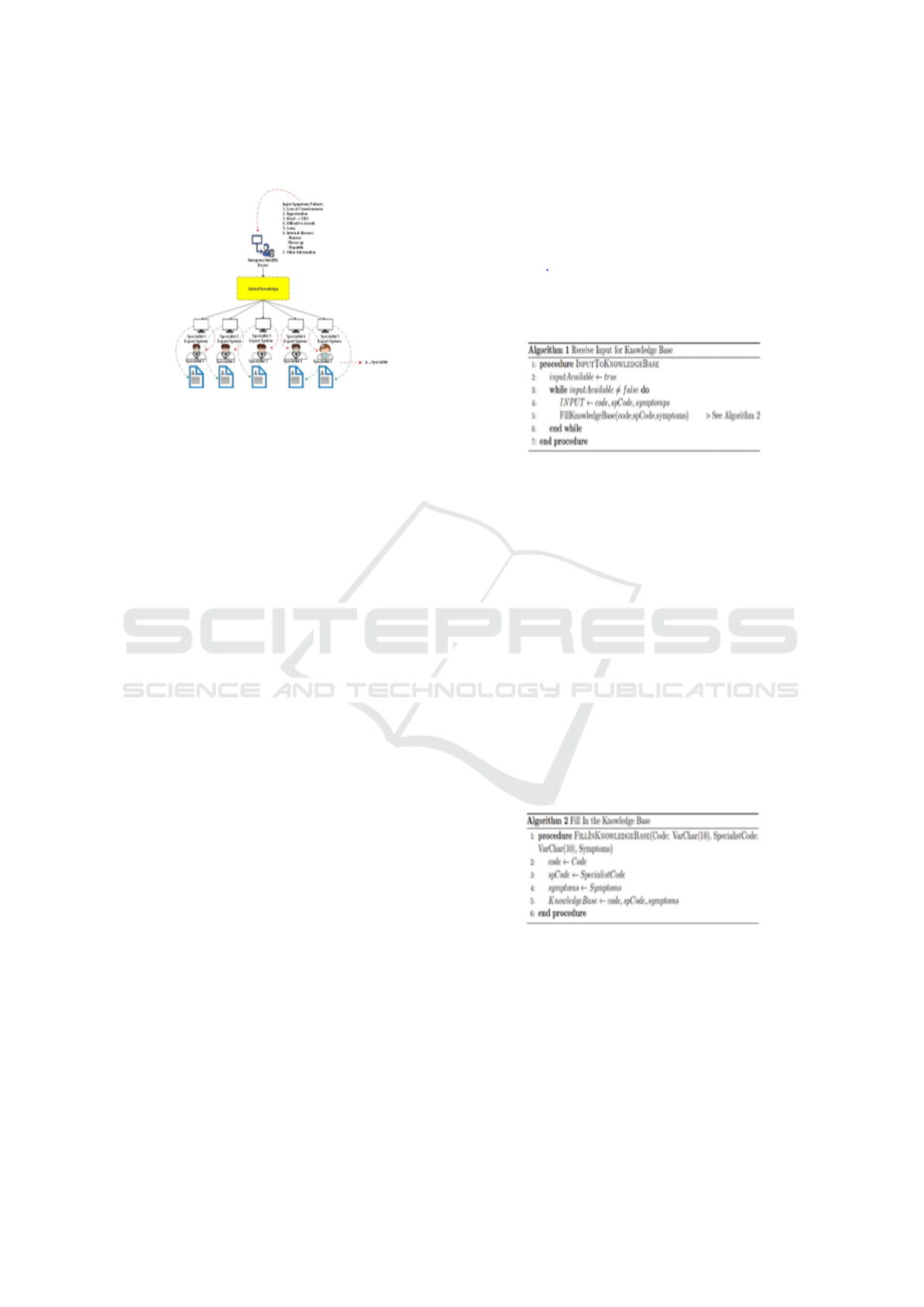
Figure 4: Group Expert System
Figure 4 is an illustration of the application of the
system carried out in the ER. The doctor on duty in
the ER is responsible for examining the patient’s con-
dition: physical examination, anamnesis and symp-
toms and laboratory results (if previously a labora-
tory examination has been conducted) that the pa-
tient has come to at the ER. Global Knowledge is a
gathering place for all knowledge obtained from the
patient’s medical record, input data: physical symp-
toms, anamnesis, and laboratory examination results
(if a laboratory examination is conducted). Data from
global knowledge is distributed to expert systems that
are owned by each specialist doctor. The final results
of the expert system of each specialist doctor will pro-
vide the results of the diagnosis and treatment care of
the patient in the ER.
3.1 Knowledge Representation
After the knowledge acquisition process has been
completed, the knowledge is transformed into a
knowledge base and a rule base which is then col-
lected, coded, organized and illustrated in another de-
sign form into a systematic form. The way to repre-
sent data into knowledge is in the form of attributes,
rules, semantic networks, frames, logic and produc-
tion rules (Leung and Wong, 1991), (“Proceedings of
the 1997 20th Annual International ACM SIGIR Con-
ference on Research and Development in Information
Retrieval,” 1997). It aims to simplify the data so that it
is easy to understand and make the program develop-
ment process effective. The expert system uses pro-
duction rules derived from decision trees and decision
tables.
3.2 Building a Knowledge Base
In building a knowledge base, two algorithms are
needed, namely an algorithm to receive knowledge
and an algorithm to fill knowledge.
Algorithm for receiving knowledge. The follow-
ing algorithm is the algorithm used in the system to
receive knowledge from experts. This algorithm is
used to fill all specialist medical doctors and symp-
toms data.
Figure 5: Algorithm 1 Receive Input for Knowledge Base
Row 1: Procedure definition, without parameter.
Row 2: Fill in the input Available variable with true
value. As long as input Available variable value is
true, the input is still available to be filled into the
knowledge.
Row 3-6: Looping for data input (code, specialist
medical doctor code, and symptoms). This part is
used to receive input and then fill those input into a
knowledge base (available in algorithm 2).
3.3 Algorithm for Filling Knowledge
There are three parameters to carry out this procedure,
namely code (code of symptoms), specialist code
(code for specialist doctors), and symptoms (knowl-
edge of symptoms).
Figure 6: Algorithm 2 Fill in the Knowledge Base
Row 1: Procedure definition. This procedure
needs 3 parameters: Code (for symptoms code), Spe-
cialist Code (for specialist medical doctor who has the
knowledge about this symptoms), and then Symptoms
(for symptoms knowledge).
Row 2-4: Fill all three parameters into local variabel
for later processing.
Row 5: Persistently write code, spCode, and symp-
toms into knowledge base.
A Symptom Distribution Method in Global Knowledge to Medical Expert System
55
3.4 Inference Algorithm
The inference algorithm of the system is divided
into two, namely the input distribution algorithm ac-
cording to the patient’s symptoms and the algorithm
to find the appropriate specialist to deal with these
symptoms.
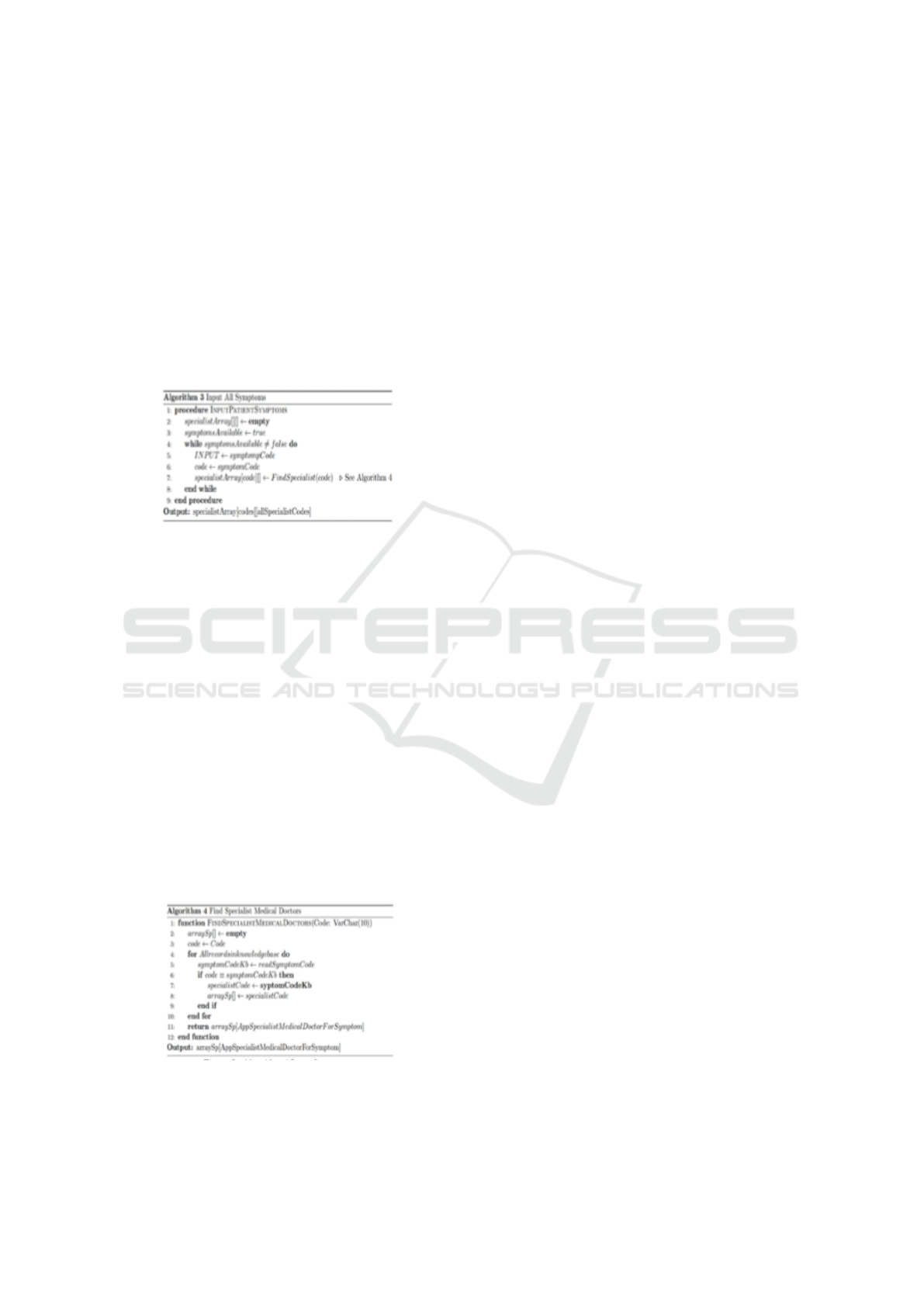
Input distribution algorithm for patient symptoms
Row 1: Procedure definition. It does not need any
parameter and is used for all patient symptoms’ input.
Output of this procedure is an array which consists of
all symptoms’ code for the patient and all specialist
codes who are able to handle the symptoms.
Figure 7: Algorithm 3 Input Symptoms
Row 2: specialist Array initialization. This array
is a 2 dimensions array which consists of [symptom
code] [list of specialist medical doctor]. At the of the
procedure, this array will be filled.
Row3: symptoms Available initialization. This vari-
able is used to mark the symptoms whether they are
still available or not.
Row 4-8: Looping as long as the data still available
for input. For every loop, symptom Code will become
the input and will be filled into local variable (code).
The code variable will become the parameter to find
the specialist in algorithm 4. Upon finishing, this pro-
cedure will return two dimensions array which con-
sists of all symptoms (codes) and all specialist codes
for every symptom (all Specialist Code).
Seeking algorithm for an appropriate specialist
This step, the step where the symptoms of the
patient will be related to the specialist’s knowledge
based on the knowledge of each specialist.
Figure 8: Algorithm 4 Input Symptoms
Row 1: Function definition. This function needs
one parameter: code (code of symptom for which the
specialist doctors are about to find. This function re-
turns array value which consists of all specialist med-
ical doctors for the symptom.
Row 2: array Sp initialization, begins with empty
value.
Row 3: Fill in Code into local variable code.
Row 4-10: Looping to read all records in knowledge
base. In every loop, symptom code in knowledge base
is read and become an input for symptom CodeKb
(row 5). If the code is the same as symptom CodeKb
then specialist medical doctor in knowledge base will
be put into arraySp (row 6-8).
Row 11: Return arraySp value which has already
filled with all specialist medical doctors for the symp-
toms.
4 CONCLUSIONS
The results of this study are an algorithm that will
be implemented in the next journal, which is an al-
gorithm that is implemented in real conditions in the
emergency unit and the distribution of symptoms to
patients received by each Specialist unit based on the
knowledge possessed by specialists in the unit emer-
gency. Knowledge data is extracted from medical
record data obtained at the hospital. The results of
this algorithm are a knowledge base that can produce
a conclusion of the type of disease so that it will help
the work of doctors in the ward of the emergency
unit and specialist units in making further observa-
tions and treatments on these patients.
REFERENCES
Adlassnig, K.-P. and Scheithauer, W. (1989). Performance
evaluation of medical expert systems using roc curves.
Computers and biomedical research, 22(4):297–313.
Aikins, J. S., Kunz, J. C., Shortliffe, E. H., and Fallat, R. J.
(1983). Puff: An expert system for interpretation of
pulmonary function data. Computers and biomedical
research, 16(3):199–208.
Aishwarya, S. and Anto, S. (2014). A medical expert sys-
tem based on genetic algorithm and extreme learning
machine for diabetes disease diagnosis. International
Journal of Science, Engineering and Technology Re-
search (IJSETR), 3(5):75–80.
Albert, M., Gors, M., and Schilling, K. (2015). Telemed-
ical applications with rulebased descision-and
information-systems (tardis). IFAC-PapersOnLine,
48(10):7–11.
Aronson, J. E., Liang, T.-P., and MacCarthy, R. V. (2005).
Decision support systems and intelligent systems, vol-
ume 4. Pearson Prentice-Hall Upper Saddle River, NJ,
USA:.
CONRIST 2019 - International Conferences on Information System and Technology
56

Biyouki, S. A., Turksen, I., and Zarandi, M. F. (2015).
Fuzzy rule-based expert system for diagnosis of thy-
roid disease. In 2015 IEEE Conference on Compu-
tational Intelligence in Bioinformatics and Computa-
tional Biology (CIBCB), pages 1–7. IEEE.
Brazis, P. W., Masdeu, J. C., and Biller, J. (2012). Local-
ization in clinical neurology. Lippincott Williams &
Wilkins.
Chambers, R. and Conway, G. (1992). Sustainable rural
livelihoods: practical concepts for the 21st century.
Institute of Development Studies (UK).
Chorbev, I., Mihajlov, D., and Jolevski, I. (2009). Web
based medical expert system with a self training
heuristic rule induction algorithm. In 2009 First
International Confernce on Advances in Databases,
Knowledge, and Data Applications, pages 143–148.
IEEE.
Cioara, T., Anghel, I., Salomie, I., Barakat, L., Miles, S.,
Reidlinger, D., Taweel, A., Dobre, C., and Pop, F.
(2018). Expert system for nutrition care process of
older adults. Future Generation Computer Systems,
80:368–383.
Cota,
´
E., Ribeiro, L., Bezerra, J. S., Costa, A., da Silva,
R. E., and Cota, G. (2017). Using formal methods for
content validation of medical procedure documents.
International journal of medical informatics, 104:10–
25.
Das, S., Ghosh, P. K., and Kar, S. (2013). Hypertension di-
agnosis: a comparative study using fuzzy expert sys-
tem and neuro fuzzy system. In 2013 IEEE Inter-
national Conference on Fuzzy Systems (FUZZ-IEEE),
pages 1–7. IEEE.
Dharmar, C., Srinivasan, S., Mital, D., and Haque, S.
(2002). Expert system for the diagnosis of neona-
tal jaundice for use by medical field personnel. In
7th International Conference on Control, Automation,
Robotics and Vision, 2002. ICARCV 2002., volume 2,
pages 1002–1006. IEEE.
Dzierzanowski, J. M., Bourne, J. R., Shiavi, R., Sandell,
H. S., and Guy, D. (1985). Gaitspert: An expert sys-
tem for the evaluation of abnormal human locomotion
arising from stroke. IEEE transactions on biomedical
engineering, (11):935–942.
Elena, A., Acevedo, A., Felipe, F., and Avil
´
es, P. (2016).
Expert system for the diagnosis of vertebral column
diseases. In 2016 IEEE 36th Central American and
Panama Convention (CONCAPAN XXXVI), pages 1–
4. IEEE.
Estefania, C.-R., Garc
´
ıa-S
´
aez, G., Rigla, M., Villaplana, M.,
Pons, B., and Hernando, M. E. (2016). Automatic
classification of glycaemia measurements to enhance
data interpretation in an expert system for gestational
diabetes. Expert Systems with Applications, 63:386–
396.
Eyadat, A. and Alsmadi, I. (2012). Automatic coverage
evaluation for a medical expert system. In 2012 Ninth
International Conference on Information Technology-
New Generations, pages 867–872. IEEE.
Fefilatyev, S., Ivanovskiy, T. V., Hall, L. O., Goldgof, D. B.,
Pobi, S., Greenstien, H., Pathak, A. P., and Garrett,
C. R. (2007). Clinical deployment of a medical ex-
pert system to increase accruals for clinical trials:
Challenges. In 2007 IEEE International Conference
on Systems, Man and Cybernetics, pages 1482–1487.
IEEE.
Fieschi, M., Joubert, M., Fieschi, D., and Roux, M.
(1982). Sphinx—a system for computer-aided diagno-
sis. Methods of information in medicine, 21(03):143–
148.
Gay, P., L
´
opez, B., Pl
`
a, A., Saperas, J., and Pous, C. (2013).
Enabling the use of hereditary information from pedi-
gree tools in medical knowledge-based systems. Jour-
nal of biomedical informatics, 46(4):710–720.
Gianni, F., Mora, S., and Divitini, M. (2019). Rapiot toolkit:
Rapid prototyping of collaborative internet of things
applications. Future Generation Computer Systems,
95:867–879.
Gorzalczany, M. B. and McLeish, M. (1992). Combina-
tion of neural networks and fuzzy sets as a basis for
medical expert systems. In [1992] Proceedings Fifth
Annual IEEE Symposium on Computer-Based Medi-
cal Systems, pages 412–420. IEEE.
Hashi, E. K., Zaman, M. S. U., and Hasan, M. R. (2017).
An expert clinical decision support system to predict
disease using classification techniques. In 2017 In-
ternational Conference on Electrical, Computer and
Communication Engineering (ECCE), pages 396–
400. IEEE.
Herry, C. and Frize, M. (2003). Design considerations for
a medical thermographic expert system. In Proceed-
ings of the 25th Annual International Conference of
the IEEE Engineering in Medicine and Biology So-
ciety (IEEE Cat. No. 03CH37439), volume 2, pages
1252–1255. IEEE.
Hyeon, J., Oh, K.-J., Kim, Y. J., Chung, H., Kang, B. H.,
and Choi, H.-J. (2016). Constructing an initial knowl-
edge base for medical domain expert system using in-
duct rdr. In 2016 International Conference on Big
Data and Smart Computing (BigComp), pages 408–
410. IEEE.
Jana, B., Oswal, K., Mitra, S., Saha, G., and Banerjee, S.
(2019). Detection of peripheral arterial disease using
doppler spectrogram based expert system for point-of-
care applications. Biomedical Signal Processing and
Control, 54:101599.
Krantz, K., Youssef, H., and Newcomb, R. (1988). Medical
usage of an expert system for recognizing chaos. In
Proceedings of the Annual International Conference
of the IEEE Engineering in Medicine and Biology So-
ciety, pages 1303–1304. IEEE.
Lee, C.-S. and Wang, M.-H. (2010). A fuzzy expert sys-
tem for diabetes decision support application. IEEE
Transactions on Systems, Man, and Cybernetics, Part
B (Cybernetics), 41(1):139–153.
Leung, K. and Wong, M. (1991). Inducing and refining rule-
based knowledge from inexact examples. Knowledge
Acquisition, 3(3):291–315.
Li, L.-b. (2010). Study on experts scheduling strategy of
collective consultation in long-distance medical sys-
tem. In 2010 International Conference on Manage-
ment and Service Science, pages 1–4. IEEE.
A Symptom Distribution Method in Global Knowledge to Medical Expert System
57

Liao, S.-H. (2005). Expert system methodologies and appli-
cations—a decade review from 1995 to 2004. Expert
systems with applications, 28(1):93–103.
Lockwood, S. and Chen, Z. (1995). Knowledge validation
of engineering expert systems. Advances in Engineer-
ing Software, 23(2):97–104.
Malmir, B., Amini, M., and Chang, S. I. (2017). A medical
decision support system for disease diagnosis under
uncertainty. Expert Systems with Applications, 88:95–
108.
Mihaela-Adina, M. and Gheorghis
˘
a, P. (2015). An ex-
pert system architecture for managing the biomateri-
als used in medical devices. In 2015 7th International
Conference on Electronics, Computers and Artificial
Intelligence (ECAI), pages P–67. IEEE.
Miller, R. A., Pople Jr, H. E., and Myers, J. D. (1982).
Internist-i, an experimental computer-based diagnos-
tic consultant for general internal medicine. New Eng-
land Journal of Medicine, 307(8):468–476.
Mutawa, AM, A. M. A. (2019). Multilayered rule-based
expert system for diagnosing uveitis. Artificial intelli-
gence in medicine, 99:101691.
Navarra, S. e. a. (2016). Decision table editor: A web appli-
cation for the management of the international tables
for mortality coding.
Nkamgang, O. T., Tchiotsop, D., Fotsin, H. B., Talla, P. K.,
Dorr, V. L., and Wolf, D. (2019). Automating the clin-
ical stools exam using image processing integrated in
an expert system. Informatics in Medicine Unlocked,
15:100165.
Oyelade, O., Obiniyi, A., Junaidu, S., and Adewuyi, S.
(2018). Patient symptoms elicitation process for
breast cancer medical expert systems: A semantic web
and natural language parsing approach. Future Com-
puting and Informatics Journal, 3(1):72–81.
Poli, V. S. R. (2015). Method of fuzzy conditional inference
and application to fuzzy medical expert systems. In
2015 International Conference on Fuzzy Theory and
Its Applications (iFUZZY), pages 115–120. IEEE.
Razzouk, D., Mari, J. d. J., Shirakawa, I., Wainer, J., and
Sigulem, D. (2006). Decision support system for the
diagnosis of schizophrenia disorders. Brazilian jour-
nal of medical and biological research, 39(1):119–
128.
Sadideen, H., Alvand, A., Saadeddin, M., and Kneebone, R.
(2013). Surgical experts: born or made? International
Journal of Surgery, 11(9):773–778.
Sakorn, M. (2016). Medical expert system based ontology
for diabetes disease diagnosis. In 2016 7th IEEE In-
ternational Conference on Software Engineering and
Service Science (ICSESS), pages 383–389. IEEE.
Sampat, M. P., Markey, M. K., Bovik, A. C., et al. (2005).
Computer-aided detection and diagnosis in mammog-
raphy. Handbook of image and video processing,
2(1):1195–1217.
Sapna, S. and Tamilarasi, A. (2009). Fuzzy relational equa-
tion in preventing diabetic heart attack. In 2009 Inter-
national Conference on Advances in Recent Technolo-
gies in Communication and Computing, pages 635–
637. IEEE.
Schiller, S. Z. and Mandviwalla, M. (2007). Virtual team re-
search: An analysis of theory use and a framework for
theory appropriation. Small group research, 38(1):12–
59.
Shortliffe, E. (2012). Computer-based medical consulta-
tions: MYCIN, volume 2. Elsevier.
Sutton, C., McCallum, A., et al. (2012). An introduction to
conditional random fields. Foundations and Trends
R
in Machine Learning, 4(4):267–373.
Tabibi, S. T., Zaki, T. S., and Ataeepoor, Y. (2013). De-
veloping an expert system for diabetics treatment ad-
vices. International Journal of Hospital Research,
2(3):155–162.
Tan, C., Wahidin, L., Khalil, S., Tamaldin, N., Hu, J.,
and Rauterberg, G. (2016). The application of ex-
pert system: A review of research and applications.
ARPN Journal of Engineering and Applied Sciences,
11(4):2448–2453.
Toloie, A. and Mohsen, S. (2010). Designing an expert sys-
tem for suggesting the blood cancer treatment. Jour-
nal of Health Administration, 13(40):41–50.
Tseng, M.-H. and Wu, H.-C. (2011). A two-dimensional
fuzzy repertory grid approach for building medical ex-
pert systems. In 2011 International Conference on
Machine Learning and Cybernetics, volume 1, pages
183–188. IEEE.
Valizadegan, H., Nguyen, Q., and Hauskrecht, M. (2013).
Learning classification models from multiple experts.
Journal of biomedical informatics, 46(6):1125–1135.
Van Remoortere, P. (1979). Computer-based medical con-
sultations: Mycin: Eh shortliffe: Published by north-
holland, amsterdam and ny, 1976, 264 pages, us
$19.95, isbn 0-444-00179-4.
Weissman, S., Diers, A., and Bemesderfer, S. (1974). Psy-
chiatric services in a youth corrections unit. Psychi-
atric Services, 25(9):602–605.
Yahia, M., Mahmod, R., Sulaiman, N., and Ahmad, F.
(2000). Rough neural expert systems. Expert Systems
with Applications, 18(2):87–99.
Zeki, T. S., Malakooti, M. V., Ataeipoor, Y., and Tabibi,
S. T. (2012). An expert system for diabetes diagno-
sis. American Academic & Scholarly Research Jour-
nal, 4(5):1.
CONRIST 2019 - International Conferences on Information System and Technology
58
