
Development of MENARI plus (Self Pulse Assessment and Clinical
Scoring) for Detecting Atrial Fibrillation in High-risk Population
Muhamad Rizki Fadlan
1,2
, Monika Sitio
1,2
, Diah Ivanasari
1,2
, Astrid Pramudya
1,2
,
Ardani Galih Prakosa
1,2
, Dea Arie Kurniawan
1,2
, Ardian Rizal
1,2
and Mohammad Saifur Rohman
1,2
1
Department of Cardiology and Vascular Medicine, Faculty of Medicine, Brawijaya University,
Dr. Saiful Anwar General Hospital, Malang, East Java, Indonesia
2
Brawijaya Cardiovascular Research Center, Brawijaya University, Malang, East Java, Indonesia
{deaariekurniawan, ardianrizal}@gmail.com, ippoenk@yahoo.com
Keywords: Atrial Fibrillation, Scoring System, Pulse Palpation.
Abstract: This study was intended to examine the accuracy of MENARI Plus in atrial fibrillation detection. We collected
data from a total of 476 subjects who were considered to be high-risk patients at Saiful Anwar General
Hospital, a member of Yayasan Jantung Indonesia in Banyuwangi and Batu, East Java, Indonesia. We
identified independent risk factors for detecting atrial fibrillation (AF) with multiple regressions. Every
participant underwent a self-pulse radial check and electrocardiography examination. AF was diagnosed by a
cardiologist. In this study, the mean age of these patients was 58,9, ± 10,9 years. We found 25% of patients
had AF, and 74,4% of our subjects were female. This tools had an area under the receiver operating curve
(AUC) of 0.83 (95% CI 0.84 to 0.92) with a sensitivity of 0.84 (95% CI 0.82 to 0.94) and a specificity of 0.80
(95% CI 0.79 to 0.84) at a cut-off score of 7 on the scale. In this study, the sensitivity of MENARI Plus was
high; however, it had low specificity for atrial fibrillation. Therefore, it is applicable for ruling out atrial
fibrillation, and it may also become an effective screening tool in earlier detection of atrial fibrillation. In
addition, MENARI Plus can be opportunistically used by the doctors to analyse patients with previously
undetected atrial fibrillation.
1 INTRODUCTION
The prevalence of AF was 1–2% in the general
Indonesian population; it is therefore important to
understand the risk factors associated with AF. Early
diagnoses are needed for stroke prevention in
40–60% of asymptomatic AF patients. Oral
anticoagulant is the most important medical measure
that can be taken to avoid unnecessary strokes in AF
patients (Rizal and Yuniadi, 2019). AF can be
identified by
pulse irregularity, which means that
pulse palpation is a prospective approach in
identifying undiagnosed AF patients.
The 2016 European Society of Cardiology
guidelines explained that opportunistic pulse
palpation and ECG record are applied when the
patients with a minimum age of 65 years experienced
pulse irregularity (Kirchhof et al., 2016). A
worldwide AF-awareness campaign is held annually.
The purpose is to increase public awareness of this
condition.
Indonesia started a national campaign to increase
awareness of atrial fibrillation in 2016 by celebrating
AF Campaign Day every September. Indonesia
promotes national screening program using the theme
of ‘AYO MENARI,’ which translates into English as,
‘Let’s Go Dancing’. MENARI stands for MEraba
NAdi sendiRI (translated into English as a self-pulse
check). Self-pulse checks are commonly used to
measure heart rate, and the measure is being
increasingly advocated as a means self-checking for
atrial fibrillation, of which an ‘irregularly irregular’
pulse is a characteristic feature. From a recent meta-
analysis, the self-pulse check has quite high
sensitivity and specificity compared to 12-lead ECG
recordings (0.98 and 0.92, respectively) (Taggar et
al., 2016).
In Indonesia, it is surprising that the effectiveness
of self-pulse checking for detecting atrial fibrillation
in the general population is unknown. This study was
intended to assess the effectiveness of our national
screening program ‘MENARI’ (self-pulse check) and
to try to increase the diagnosis yield by adding some
Fadlan, M., Sitio, M., Ivanasari, D., Pramudya, A., Prakosa, A., Kurniawan, D., Rizal, A. and Rohman, M.
Development of MENARI plus (Self Pulse Assessment and Clinical Scoring) for Detecting Atrial Fibrillation in High-risk Population.
DOI: 10.5220/0009427300570061
In Proceedings of the 4th Annual International Conference and Exhibition on Indonesian Medical Education and Research Institute (The 4th ICE on IMERI 2019), pages 57-61
ISBN: 978-989-758-433-6
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
57

clinical conditions to MENARI. We ultimately
attempted to build a simple scoring system that can be
used by the general population to detect AF.
2 MATERIAL AND METHODS
This was an observational analytic study with a cross-
sectional design. This research was conducted at the
Cardiology Outpatient Centre of Saiful Anwar
General Hospital Malang, with assistance from
Lavalette Hospital Malang, Indonesian Heart
Association and the geriatric association in Malang,
Indonesia. Our study samples included subjects
between the ages of 50–75 years old, since the
registry in Yayasan Jantung Indonesia, Malang Raya,
mostly found AF in patients within this age range.
After seeking and obtaining informed consent from
each participant, subjects of this study completed a
structured questionnaire and provided information on
gender, age, smoking status, medical history, physical
exercise, profession and level of education. We used
the patients’ medical records to collect medical
history, medication history and lifestyle factors. We
used standard methods for measuring blood pressure,
weight, height and waist circumference
Patients were able to assess their self-pulse. The
patients implemented the Mini-Mental State
Examination (MMSE). They receive an explanation
of the benefit of pulse palpation. The patients also
obtained knowledge of self-assessment of heart
regularity, especially the technique of radial artery
pulse palpation. Every participant performed self-
pulse palpation and electrocardiography.
2.1 Statistical Analyses
The mean with SD are presented for continuous
variables and several patients (%) for the categorical
variables. We used a multivariate regression to
develop clinical risk factors. The stepwise model
selection procedure was performed to develop clinical
scoring. The pool of variables was also confirmed by a
removal approach with a P-value threshold of 0.25.
Testing for interactions was applied for risk factors in
the final model; however, no potential advance
progression could be accomplished by involving these
interactions. The area under the curve (AUC) was used
to evaluate the performance of this score.
2.2 Ethics
This study received approval from the Medical Ethics
Committee at Saiful Anwar General Hospital Malang
(Ethical Clearance No. 400/122/K3/302/2019). All
subjects of this study signed and were given informed
consents.
3 RESULT
3.1 Clinical Characteristics
A total of 476 subjects participated in the study; 321
(65.6%) of the subjects were female. The mean age of
the population was 53,6, ±11,06 Years old. Mean
SBP and DBP were 125, ±17,5; and 79,7, ±11,5
mmHg; and the prevalence of subjects with atrial
fibrillation was found to be 23,5%. The baseline
characteristics of the subject are described in Table 1.
Table 1: Baseline Characteristic.
Characteristics Total n=476
Age 53,6 ± 11,06
Female 65,6%
SBP 125±17,5
DBP 79,7±11,5
AF 23,5%
Heart rate 83,5±12,5
Weight 61,57±9,7
BMI 26,27±6,6
MMSE score 28,6±0,5
Diabetes 9,8%
Hypertension 41%
History of TIA/Stroke 5,5%
3.2 Clinical Characteristics of
Participants by ECG
Derivation of patients’ characteristics are provided in
Table 2. A total of 461 subjects were analysed. As
many as 43 subjects with developed AF were
compared with other patients without AF. The
patients with developed AF were older (P < .03),
The 4th ICE on IMERI 2019 - The annual International Conference and Exhibition on Indonesian Medical Education and Research Institute
58
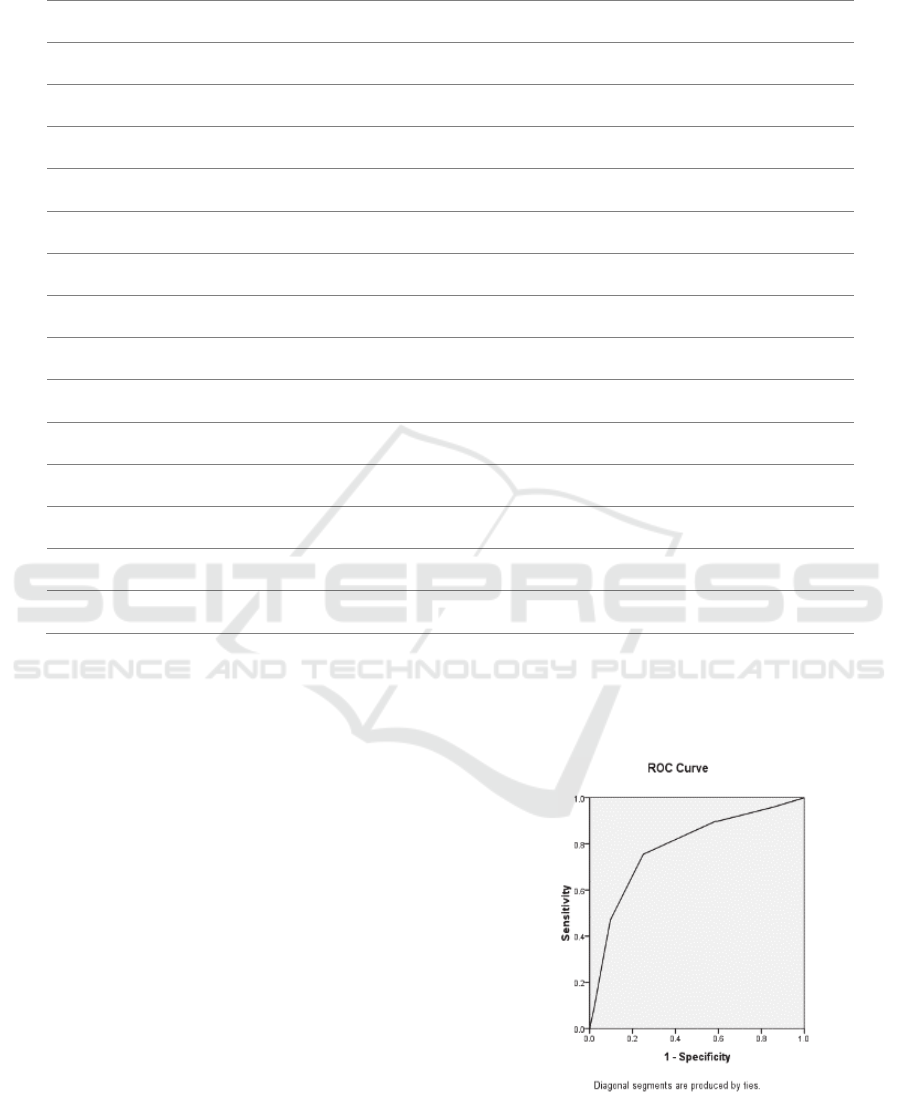
Table 2: Univariate Analysis.
Variables AF Non-AF P
Age >65 43.4% 26.8% 0.03
BMI > 26 9.3% 8.8% 0.45
MENARI (irregular) 66,6% 30,9% 0.000
Hypertension 66.1% 32.2% 0.000
Diabetes Mellitus 5.2% 9.8% 0.26
Stroke/TIA 11.1% 4.3% 0.138
Hyperthyroid 5.7% 0% 0.00
Dyspnoea 8.5% 6.5% 0.54
Palpitation 66% 32.5% 0.000
Chest pain 1.9% 5.3% 0.43
Syncope 2.2% 5.7 0.46
Dizziness 22.6% 11.4% 0.089
Fatigue 34% 17.9% 0.02
more frequently men (P < .001), and experienced
higher rates of hypertension (P < .000), hyperthyroid
(P < .000) and stroke (P < .138). Clinical
manifestation in AF patients were palpitations
(p < .000), fatigue (P < .02) dizziness (P< .089).
Risk Factors for incidences of AF and Score
Development Univariate Cox regression analysis is
shown in Table 3. On multivariable analyses, age was
>65 years, Irregular Self Pulse palpation (MENARI),
Hypertension, Palpitation, and fatigue were
independent risk factors for incident AF (Table 3).
Given the significant association with diagnosed AF,
a combination of independent risk factors was
identified as the new simple MENARI Plus score
(Table 3): Irregular self-pulse palpation (MENARI)
(4 point each); P: palpitation (2 points); L: oLd (age
> 65 years, 1 point); U: fatigUe (2 points); and H:
hypertenSion (2 points). The total score ranged from
0 to 11 points.
The score presented a good discrimination with an
area under the receiver operating curve (AUC) of 0.83
(95% CI 0.84 to 0.92) with a sensitivity of 0.84 (95%
CI 0.82 to 0.94) and a specificity of 0.80 (95% CI 0.79
to 0.84). A bootstrap sampling procedure was used
internally to validate the score results, which gave an
AUC of the validation (AUC 0.87 [95% CI 0.80 to
0.95).
Figure 1: AUC of Derivation Set.
Development of MENARI plus (Self Pulse Assessment and Clinical Scoring) for Detecting Atrial Fibrillation in High-risk Population
59
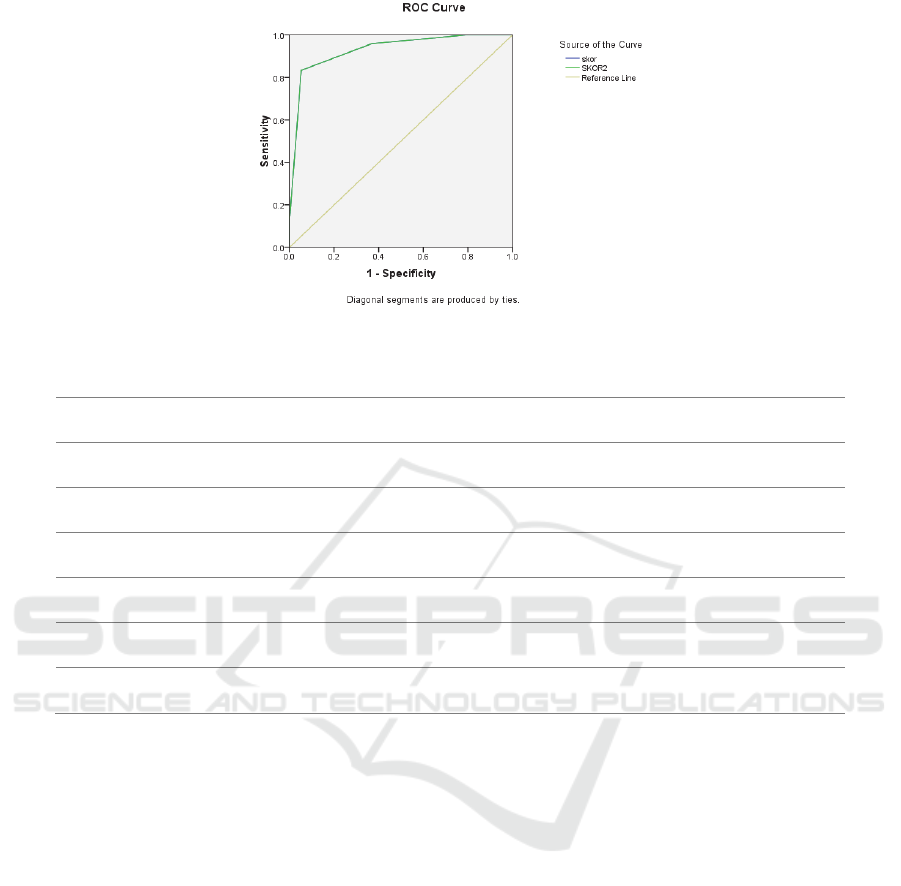
Figure 2: AUC of Validation Set.
Table 3: MENARI Plus Score.
Predictors Multiplying Factor Value
Irregular MENARI +4 0.000
Palpitation +2 0.000
Age >65 +1 0.046
Hypertension +2 0.006
Fatigue +2 0.02
TOTAL POSSIBLE SCORE 11
4 DISCUSSION
4.1 Baseline Data
The prevalence of AF in our sample was high (23.5%
of the sample), compared to another study that ranged
between 6–9% of the population. This is likely due to
the fact that the sample was taken from a high-risk
population group. This study was performed with
patients between the ages 50–75 years old because
according to the registry from Yayasan Jantung
Indonesia, Malang Raya, incidences of atrial
fibrillation were mostly found in their age. It is often
associated with a higher prevalence of another
cardiovascular comorbidity, such as hypertension
(41%), the history of stroke or TIA (5.5%) and/or
diabetes mellitus (9.8%). Therefore, this number
cannot be generalised to the overall prevalence of AF
in Indonesia. AF is found more frequently in older
patients (43.4% vs. 26.8%, p = 0.03) and hypertensive
patients (66.1% vs. 32.2%, p = 0.00), compared to
younger and non-hypertensive patients. European
data revealed that incidences of AF are discovered in
3.7–4.2% of those aged 60–70 years of age; these
numbers increase to 10–17% in older ages.
Hypertension and diabetes mellitus were already
known to be risk factors for AF.
Although Self-Pulse Check / MENARI has been
widely used for screening purposes, its effectiveness
in Indonesia had never been evaluated. According to
a systematic review by Harris et al. conducted in
2012, the self-pulse check showed a high rate of
accuracy for detecting AF. The sensitivity and
specificity range were 87–97% and 70–81%,
respectively. This rate is high, but there still room for
improvement. A European Heart Rhythm Association
(EHRA) Consensus document from 2017 started to
divine another screening tool and technique with
higher diagnosis yield, such as a handled device and
smartphone.
The 4th ICE on IMERI 2019 - The annual International Conference and Exhibition on Indonesian Medical Education and Research Institute
60

Adding some clinical characteristics to increase
the accuracy of diagnosis has been widely used in
another diagnostic method, such as well-known
SYNTAX and Clinical Syntax for predicting clinical
outcome in patients who underwent percutaneous
coronary intervention. By adding these clinical
predictors, it can increase its accuracy; borrowing the
idea of adding simple clinical characteristics,
MENARI PLUS was built.
Several clinical conditions that were previously
known as symptoms and risk factors were analysed.
Statistically, some characteristics have proven to be
correlated to AF. MENARI Plus consists of self-pulse
check (MENARI / MEraba Nadi sendiRI in
Indonesian words); palpitation is the most common
symptom found in AF patients. More than half of all
patients with AF had an episode of palpitation as the
primary symptom; another symptom that has proven
to be significant is fatigue; and loss of atrial kick
during diastole, short diastolic filling time (in AF with
rapid ventricular response) and increased mitral and
tricuspid regurgitation are believed to be responsible
for the decrease in cardiac output.
The number of the patients admitted to the
hospital due to heart failure related to AF has
increased in the last decade. Current guidelines also
showed a strong correlation between heart failure and
atrial fibrillation. Catheter ablation of AF was shown
to reduce the morbidity and morbidity patient with
heart failure. Thus, indicated that fatigue and another
sign of heart failure are correlated with AF. As
previously mentioned, hypertension and older age are
strongly correlated with AF.
Table 4: Predictor for Atrial Fibrillation.
MENARI
Self-pulse check (MEraba NAdi
sendiRI in Indonesian word)
P
Palpitation
L
OLder Age (> 65 years old)
U
FatigUe
S
HypertenSion
5 CONCLUSION
We found that the specificity of MENARI Plus is low,
while its sensitivity is high for atrial fibrillation
identification in high-risk patients. This scoring
system can also rule out undetected atrial fibrillation.
REFERENCES
Kirchhof, P., Benussi, S., Kotecha, D., Ahlsson, A., Atar,
D., Casadei, B., … Vardas, P. (2016). 2016 ESC
Guidelines for the management of atrial fibrillation
developed in collaboration with EACTS. European
Heart Journal, 37(38), 2893–2962. http://doi.org/
10.1093/eurheartj/ehw210
Rizal, A., & Yuniadi, Y. (2019). Epigenetic implication in
atrial fibrillation: A potential biomarker? Journal of
Laboratory and Precision Medicine (JLPM), 4, 1–8.
http://doi.org/10.21037/jlpm.2019.09.02
Taggar, J. S., Coleman, T., Lewis, S., Heneghan, C., &
Jones, M. (2016). Accuracy of methods for detecting an
irregular pulse and suspected atrial fibrillation: A
systematic review and meta-analysis. European
Journal of Preventive Cardiology, 23(12), 1330–1338.
http://doi.org/10.1177/2047487315611347.
Development of MENARI plus (Self Pulse Assessment and Clinical Scoring) for Detecting Atrial Fibrillation in High-risk Population
61
