
Immediate Effect of Quadriceps Elastic Taping Application as a
Supplementary Treatment on Gait Performance in Patients with
Knee Osteoarthritis: A Serial Case Report
Andwi Setiawan Kokok
1
, Fitri Anestherita
2
1
Resident of Department of Physical Medicine and Rehabilitation, University of Indonesia,
Dr, Cipto Mangunkunumo National Hospital, Jakarta, Indonesia
2
Staff of Department of Physical Medicine and Rehabilitation, University of Indonesia,
Dr, Cipto Mangunkunumo National Hospital, Jakarta, Indonesia
andwisetiawan@yahoo.com
Keywords: Elastic Taping, Gait Performance
Abstract: Quadriceps strength is an important determinant of walking in subjects with knee OA (KOA). Quadriceps
Elastic Taping (ET) application might immediately improve gait performance while other modalities may
need time to show improvement. Case Description: Seven patients with KOA (9 knees) presented with
pain during weight bearing. ET was prescribed as a supplementary treatment to improve gait performance.
Increased gait performance such as walking speed and reduced excessive knee flexion during loading
response was seen in 77% and 66% of subjects respectively. In order to evaluate changes in muscle
contraction immediately after ET application, surface EMG examination was done and we found only
55% of subjects have increased percentage of maximum voluntary contraction (MVC). Discussion:
Increased cutaneous input during ET application in the afferent nerves may activate a loop via afferent
and efferent nerve fibres which eventually increasing quadriceps muscle activation that may reduce joint
load during gait. Unexpectedly, increased quadriceps contraction after ET application was inconsistent,
therefore placebo effect may also play an important role in developing the findings in this study.
Conclusion: ET application have potential to improve gait performance in patients with KOA. Further
studies are needed to prove ET effect on gait performance.
1 INTRODUCTION
Many functional limitations are caused by muscle
impairments in knee osteoarthritis (KOA).
Understanding the extent of muscle impairments, its
relationship with physical function and disease
progression, and the evidence behind exercise
therapy that targets muscle impairments is crucial.
Muscle strength, especially quadriceps, is a
major determinant of both performance-based and
self-reported physical function. Quadriceps,
hamstrings, and hip muscles are significantly
impaired in subjects with KOA compared with age-
matched controls. (Alnahdi, Zeni, and Snyder-
Mackler, 2012) Quadriceps activation deficits in
KOA are largely predicted due to an alteration in
knee joint sensory receptors, which reduces the
excitability of the alpha motoneurons via spinal
and/or supraspinal mechanisms. (Rice, McNair, and
Lewis, 2011)
The quadriceps control the rate of descent of the
body’s center of mass. Eccentric activation of these
muscles also provides shock absorption to the knee.
At the initial contact phase of walking, the knee
flexes slightly in response to the ground reaction
force. Eccentrically active quadriceps control the
extent of the knee flexion. Acting as a spring, the
muscle helps dampen the impact of loading on the
joint. Strong muscles are less fatigable and exhibit
greater motor control, thus avoiding damaging
increases in shear forces and peak joint forces.
(Susko and Fitzgerald, 2013)
The quadriceps femoris is a large and powerful
extensor muscle, consisting of the rectus femoris
and three vasti muscles, with vastus lateralis as the
largest muscle with highest cross-sectional area.
The two main factors that determine the muscle’s
force production capabilities are the muscle cross-
Kokok, A. and Anestherita, F.
Immediate Effect of Quadriceps Elastic Taping Application as a Supplementary Treatment on Gait Performance in Patients with Knee Osteoarthritis: A Serial Case Report.
DOI: 10.5220/0009090403370342
In Proceedings of the 11th National Congress and the 18th Annual Scientific Meeting of Indonesian Physical Medicine and Rehabilitation Association (KONAS XI and PIT XVIII PERDOSRI
2019), pages 337-342
ISBN: 978-989-758-409-1
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
337
sectional area and the ability of the nervous system
to fully activate the muscle. (Alnahdi, Zeni, and
Snyder-Mackler, 2012) Ikeda et al reported 12%
reduction in quadriceps cross sectional area in
women with radiographic evidence of knee OA,
compared to women without radiographic evidence
of knee OA. (Ikeda, Tsumura, and Torisu, 2005)
Several gait modification strategies were adopted
by KOA patients to alter knee joint load, such as
reduced gait speed, increased knee flexion, reduced
vertical acceleration at initial contact, reduced stride
length, and increased mediolateral trunk lean. (Simic,
et. al, 2011) These modifications might cause
increased quadriceps load and causing fatigue
consequently. Quadriceps weakness increased
accordingly as KOA progress.
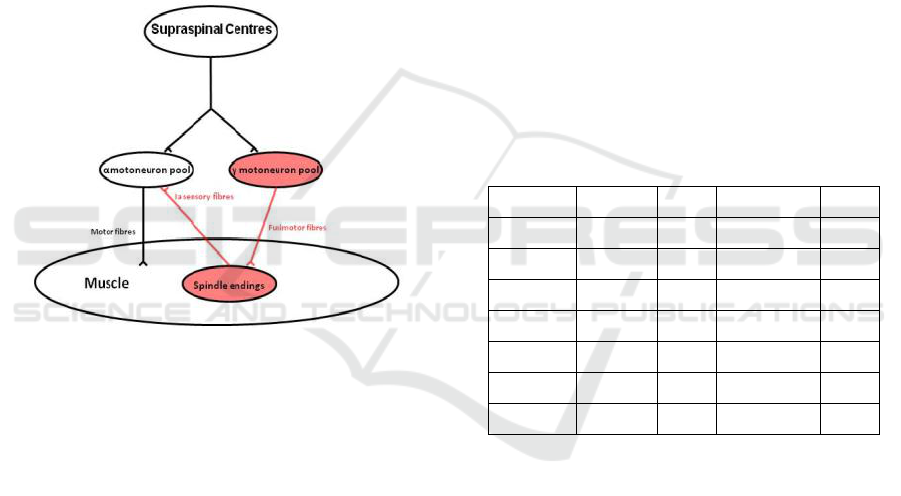
Figure 1: Muscle spindles provide a tonic excitatory input
to the homonymous a-motoneuron pool via Ia sensory
nerve fibres.
Taping is widely used in the field of
rehabilitation as both a means of treatment and
prevention of sports-related injuries. In recent years,
the use of Elastic Tape (ET) has become
increasingly popular. ET was designed to mimic the
qualities of human skin. It has roughly the same
thickness as the epidermis and can be stretched
between 30% and 40% of its resting length
longitudinally. (Thelen, Dauber, and Stoneman,
2008)
One of the proposed mechanisms how ET might
increase muscle activation is by increased cutaneous
input in the afferent nerves and therefore activating
feed forward loop via afferent and efferent nerve
fiber. (see Figure. 1) (Rice, McNair, and Lewis,
2011). When ET was applied on the quadriceps
muscles during gait, we presumed it would improve
gait alteration due to increased muscle contraction.
This case series is trying to see the effect of vastus
lateralis ET application on gait performance such as
gait speed and knee kinematic parameter and to
evaluate the muscle activation during gait in patients
with KOA.
2 CASE DESCRIPTION
Seven females with KOA (9 knees) presented
with pain during weight bearing activities. All
participants age range were 49 – 69 years old and
had a diagnosis of primary symptomatic knee OA
according to the criteria of the American College of
Rheumatology. Two patients had knee varus
deformity, and none has valgus deformity. All
patients did not have joint hyperlaxity. Knee pain
was scored between 3 – 6 on Numeric Rating Scale
(NRS). Several managements were prescribed to
these patients in accordance to their problems, such
as Low-Level Laser Therapy and Quadriceps
strengthening. ET was prescribed as a
supplementary treatment to improve gait
performance.
Table 1: Subject characteristics
ET was attached using Y-strip method around vastus
lateralis muscle (VL) with anchor (5 cm) attached at
lateral side of patellar tendon and the tails (5 cm)
were attached at lateral thigh near greater trochanter.
ET was applied while patient’s knee is in full flexion
with 75% stretch. All participants were asked to rest
for 20 minutes after application. Surface EMG
electrodes were attached at VL muscle belly to
measure muscle activity.
Subject
Gender
Age
OA Site
VAS
1
F
69
Unilateral
5
2
F
59
Unilateral
4
3
F
55
Unilateral
3
4
F
49
Bilateral
5
5
F
52
Unilateral
4
6
F
57
Unilateral
3
7
F
50
Bilateral
6
KONAS XI and PIT XVIII PERDOSRI 2019 - The 11th National Congress and The 18th Annual Scientific Meeting of Indonesian Physical
Medicine and Rehabilitation Association
338
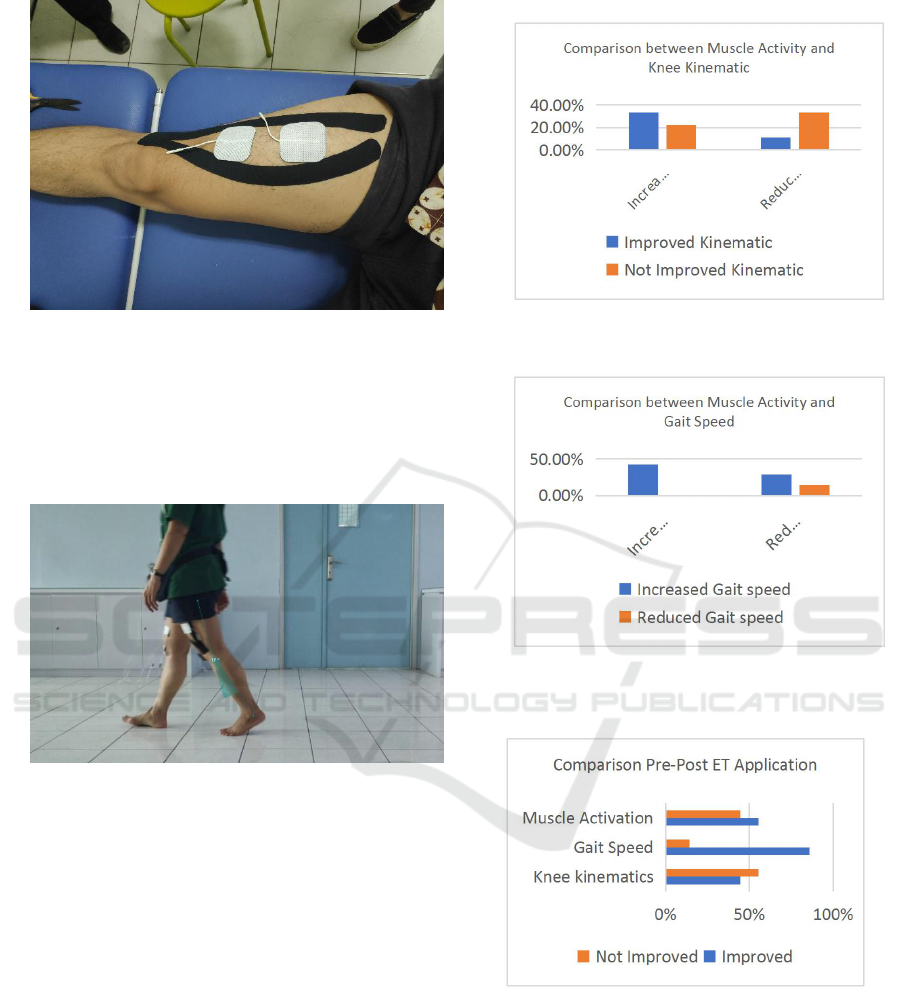
Figure 2: ET and sEMG Electrode Application.
All participants were then asked to walk at their
own comfortable speed and were recorded using
video recorder from anterior and lateral view. The
video was then analysed using Kinovea® to measure
knee kinematic changes.
Figure 3.:Gait Recorded and Analysed using Kinovea®
3 RESULT
Increased gait speed was observed at this case series
with 6 out of 7 patients had increased speed.
Average gait speed pre ET application was 0,63 m/s
and average gait speed post ET application was 0,72
m/s. A systematic review was done to measure
MCID in comfortable gait speed of adults with
pathology and it reported gait speed MCID is 0,10 –
0,20 m/s. (Bohanon and Glenney, 2014) Reduced
knee flexion during loading response was recorded
in 4 out of 9 knees. The main outcome of this study
is to observe changes gait performance after
supplementary ET application, measured by muscle
activation, knee kinematic changes, and gait speed.
Figure 4: Comparison between Muscle Activity and Knee
Kinematic
Figure 5: Comparison between Muscle Activity and Gait
Speed
Figure 6: Comparison Pre-Post ET Application
Immediate Effect of Quadriceps Elastic Taping Application as a Supplementary Treatment on Gait Performance in Patients with Knee
Osteoarthritis: A Serial Case Report
339

Table 2. Knee flexion and gait speed changes
Su
bje
ct
Knee Flexion (during loading
response)
Gait Speed (m/s)
Muscle Activity (% MVIC)
Pre ET
Post ET
Delta
Pre ET
Post ET
Delta
Pre ET
Post ET
Delta
1
12,39
9,11
-3,29
0,67
0,68
0,01
25,70%
25,90%
0,20%
2
11,40
10,83
-0,57
0,79
0,8
0,01
14,70%
29,50%
14,80
%
3
20,09
21,91
1,82
0,53
0,52
-0,01
17%
11,70%
-
5,30%
4
9,63
8,44
-1,19
0,63
0,65
0,02
24,50%
23,20%
-
1,30%
5
3,99
2,70
-1,29
0,66
0,72
0,06
22,90%
13,40%
-
9,50%
6
0,45
1,98
1,53
0,66
0,72
0,06
13,90%
23,50%
9,60%
7
15,45
16,69
1,24
0,6
0,83
0,23
19,50%
14,70%
-
4,80%
8
15,51
15,87
0,36
0,6
0,83
0,23
11,40%
13,40%
2,00%
9
7,35
9,41
2,06
0,56
0,69
0,13
18,40%
21,80%
3,40%
Av
era
ge
10,70
10,77
0,07
0,63
0,72
0,09
18,67%
19,68%
1,01%
Increased gait performance such as walking
speed and reduced excessive knee flexion during
loading response was seen in 86% and 44% of
subjects respectively. In order to evaluate changes in
muscle activity immediately after ET application,
surface EMG electrodes was attached on VL muscle
belly and we found only 55% of subjects have
increased percentage of maximum voluntary
contraction (MVC) (see figure 6). No adverse effect
was observed during ET application.
4 DISCUSSION
Speed and other spatio-temporal parameters are
important outcomes used to characterize gait in a
wide range of pathologies. Numerous studies have
been reporting slower walking speed in KOA
patients compared with non-KOA individuals, and
slower walking speed in severe OA compared to
moderate OA patients. (Favre and Jolles, 2016). In
this study, 86% of patients had an increase in their
gait speed (see figure 6). This might be explained
because during ET application, patients might
experience decrease in knee pain, giving them the
ability to walk faster. Unfortunately, we didn't
record pain level pre-post ET application, since we
were focusing on objective clinical improvements in
gait performance. Decreased pain could be the result
of increased quadriceps activity. Therefore, reducing
the knee joint load.
Recent study highlighted an association between
mid-stance Knee flexion moment (KFM) and OA
progression, where patients walking with a larger
KFM peak at baseline lost more cartilage during
five-year follow-up. (Chebab, et. al, 2014). A critical
review of the literature suggests that in the KOA
patients the knee flexion angle (KFA) at heel strike
and during early stance are greater along with
reductions in the peak external knee extension
moment in late stance. (Heiden Lloyd, and Ackland,
2009) This parameter is seen larger in severe
compared with moderate OA patients. (Favre and
Jolles, 2016) KOA patients also showed a significant
smaller maximal knee extension angle in late stance.
Limitation in maximal knee extension angle in late
stance could be caused by contracture or pain during
end range extension. Previous studies also report a
lower peak knee flexion moment in early stance,
which has been associated with quadriceps weakness
or pain avoidance gait and could represent the
intention to minimize knee joint loading. (Baert, et.
al, 2013)
Reduced excessive knee flexion during loading
response was seen in 44% of subjects respectively
following ET application (see figure 6). We suspect
KONAS XI and PIT XVIII PERDOSRI 2019 - The 11th National Congress and The 18th Annual Scientific Meeting of Indonesian Physical
Medicine and Rehabilitation Association
340

that this change in knee kinematic parameter is
related to the increased activation of the vasti
muscles, especially the vastus lateralis. During gait,
activity of the vasti musc1es begins in terminal
swing (90% gait cycle (GC)). Musc1e intensity
rapidly increases to a peak of 25% MMT early in
loading response (5% GC). This level of effort is
maintained throughout the remainder of the loading
response period. They have functioned eccentrically
to restrain (decelerate) knee flexion. On the onset of
mid stance, the quadriceps rapidly reduces its effort
and ceases by the 15% GC point. With increased
quadriceps activity, we could expect reduced
excessive knee flexion during loading response.
In a tonus-increasing muscle application, the
elastic stretch tape exerts tension via the restoring
force in the direction of origin (punctum fixum) to
the fixed base, and thus displaces the skin in the
same direction. This brings about support of the
muscle contraction. (Kumbrink, 2014) Anatomically,
muscles are described by their proximal attachments
(origin), distal attachments (insertion), and actions in
producing specific joint motions. After all, knowing
where a muscle’s proximal and distal attachments
are and understanding the motion a muscle produces
is essential to appreciating more complicated muscle
functions. We can take this notion in another
direction to better understand muscle function in a
closed chain activity: If the distal segment of a
muscle’s attachment is stabilized, then the proximal
segment is the moving end of the muscle (Houglum
and Bertoti, 2012).
During loading response, quadriceps contracts
eccentrically to provides shock absorption. The
joint is protected from the deleterious force of full
floor impact. The quadriceps react to inhibit further
flexion by increased intensity of the vasti during
early midstance. Further demand on the quadriceps
is minimized by the tibial stability gained through
the action of the soleus. This allows the femur to
advance at a faster rate than the tibia (femoral on
tibial movement). Therefore, quadriceps contraction
during stance phase was considered as closed kinetic
chain. ET application on vastus lateralis in this case
series was done from lateral side of patellar tendon
to lateral thigh near greater trochanter and
considered as muscle facilitation, due to closed
kinetic chain quadriceps activation nature during
gait.
In this case series, Increased quadriceps muscle
activation (% MVC) was seen only in 55% of
subjects measured using sEMG. The increased
muscle activity doesn't seem to be consistent on
every patient experiencing improvement in gait
performance (see figure 4 and figure 5). The
discrepancies between increased muscle activation
and improved functional performance suggesting
other mechanism that might contributed to these
findings including the placebo effect.
Several studies have shown mixed findings about
the effect of ET application to increased muscle
activation. One of the possible mechanisms of ET is
placebo effect. The role of expectation in the
placebo effect was demonstrated in a series of
clinical trials investigating the treatment of
postpartum pain. While the majority of the literature
on the biological approach relates the placebo effect
to the release of endogenous opioids and dopamine
as an explanatory mechanism. Dopamine may also
play a significant role in controlling opioid release
and could therefore play a role in the transmission
and perception of pain. (Thelen, Dauber, and
Stoneman, 2008)
5 LIMITATION
This case series is a retrospective study with limited
number of cases. Bigger study with randomized
prospective design and several ET application
methods (including different direction and stretch) is
needed to evaluate the effect of ET on increased
muscle activation and strength, as well as
improvement on gait performance.
6 CONCLUSION
Quadriceps ET application have the potential to
improve gait performance immediately in patients
with KOA. Better studies are needed in order to
evaluate whether these changes were associated to
ET application
.
REFERENCES
Alnahdi AH, Zeni JA, Snyder-Mackler L. 2012. “Muscle
Impairments in Patients with Knee Osteoarthritis”,
Sports Health, 4(4):284-92
Baert IAC, et al. 2013. “Gait characteristics and lower
limb muscle strength in women with early and
established knee osteoarthritis”. Clinical Biomechanic.
28(1):40-7.
Bohanon RW, Glenney SS.2014. “Minimal clinically
important difference for change in comfortable gait
speed of adults with pathology: A systematic review”.
Immediate Effect of Quadriceps Elastic Taping Application as a Supplementary Treatment on Gait Performance in Patients with Knee
Osteoarthritis: A Serial Case Report
341

Journal of Evaluation in Clinical Practice. 20(4):295-
300.
Chehab EF, et al. 2014. “Baseline knee adduction and
flexion moments during walking are both associated
with 5 year cartilage changes in patients with medial
knee osteoarthritis”. Osteoarthritis and Cartilage.
22(11):1833-9.
Favre J, Jolles BM. 2016. “Gait analysis of patients with
knee osteoarthritis highlights a pathological
mechanical pathway and provides a basis for
therapeutic interventions”. EFORT Open Reviews.
13;1(10):368-374.
Heiden TL, Lloyd DG, Ackland TR. 2009. “Knee joint
kinematics, kinetics and muscle co-contraction in knee
osteoarthritis patient gait”. Clinical Biomechanic.
24(10):833-41.
Houglum PA, Bertoti DB. 2012. “Brunnstorm’s clinical
kinesiology”. 6
th
Ed. Philladelphia: F.A. Davis
IRA. 2014. “Rekomendasi IRA untuk diagnosis dan
penatalaksanaan osteoartritis. dalam: Diagnosis dan
Penatalaksanaan Osteoarthritis”.
Kumbrink. 2014. “K-Taping”. 2
nd
Ed. Dortmund: Springer.
Rice DA, McNair PJ, Lewis GN. 2011. “Mechanisms of
quadriceps muscle weakness in knee joint
osteoarthritis: the effects of prolonged vibration on
torque and muscle activation in osteoarthritic and
healthy control subjects”. Arthritis Research &
Therapy. 13(5):R151.
Susko AM, Fitzgerald GK. 2013. “The pain-relieving
qualities of exercise in knee osteoarthritis”. Open
Access Rheumatology: Research and Reviews. 5: 81–
91.
Simic M. et al. 2011. “Gait Modification Strategies for
Altering Medial Knee Joint Load: A Systematic
Review”. Arthritis Care and Research. 63(3):405-26.
Thelen MD, Dauber JA, Stoneman PD. 2008. “The
clinical efficacy of kinesio tape for shoulder pain: a
randomized, double-blinded, clinical trial”. Journal of
Orthopaedic & Sports Physical Therapy. 38(7):389-95.
KONAS XI and PIT XVIII PERDOSRI 2019 - The 11th National Congress and The 18th Annual Scientific Meeting of Indonesian Physical
Medicine and Rehabilitation Association
342
