
The Correlation between Physical Activity with Body Mass Index
in Obesity Patient with Knee Osteoarthritis
Ricky Fakhrazi
1
and Tirza Z. Tamin
2
1
Department of Physical Medicine and Rehabilitation Department, University of Indonesia, Jakarta, Indonesia.
2
Department of Physical Medicine and Rehabilitation Dr.Cipto Mangunkusumo National Hospital, Jakarta, Indonesia.
Keywords: Body Mass Index, Obesity, Osteoarthritis, Physical Activity.
Abstract: Obesity in Indonesia has significantly increased every year. Obesity occurs due to an imbalance of input and
output of energy, causing the accumulation of body fat. Weight gain causes stress to knee joints and prone
to osteoarthritis that will lead to pain during walking. Decreasing the level of physical activity (PAL) in
obese patients with osteoarthritis will risk them to deconditioning syndrome which will aggravate obesity.
The purpose of this study is to correlate the level of physical activity in obese patients with osteoarthritis of
the knee who was treated at the obesity clinic at Cipto Mangunkusumo Hospital. A cross-sectional method
with thirty-eight consecutive samples. Inclusion criteria are: early elderly patients, male and female, who
were diagnosed with obesity with knee osteoarthritis, can walk independently without assistance, can
communicate well. Anamnesis is conducted for one full day activity for three days a week, and the average
energy expenditure is calculated. The basal metabolic rate is calculated by the Harris-Benedict equation and
then the level of physical activity of the patient is determined. The results of this study are that there is a
weak positive correlation between PAL and body mass index (BMI) in obese patients with knee
osteoarthritis.
1 INTRODUCTION
Obesity is a disease caused by an imbalance of
energy produced due to excessive energy intake and
reduced-calorie use. However, the pathogenesis of
obesity is very complex and not yet fully understood
(Australian Government, 2013). Control of one's
appetite and sensitivity is regulated by neural and
neurohumoral mechanisms that are influenced by
genetic, nutritional, environmental, and
psychological. This mechanism is stimulated by a
metabolic response that is centered on the
hypothalamus. The neurohumoral mechanism is
divided into three components: regulation of
hormone secretion, the rate of energy expenditure,
and control of hunger and satiety.
Obesity is caused by many factors, 40-70% of
the most important factor is genetic in determining a
person's weight. Besides lifestyle, environment, and
socioeconomic status of a person can be a cause of
obesity. In general, obesity appears at age > 30 years
in men, whereas in women originating from
childhood (Sugondo, 2006).
In people with obesity, more calories are
consumed than is used and the appetite is not
reduced to compensate for the increase in body
energy stores. The amount of adipose tissue is
tightly regulated through the transmission of
humoral and neural signals to the brain. Failure of
fat cells to transmit adequate signals or errors from
the brain is responding to incoming signals that
cause obesity (Berthoud, 2002). An effective system
of regulation of energy balance, requiring sensors of
energy storage in adipose tissue, a mechanism for
delivering information to central control
(hypothalamus) for further integration, which in turn
will determine food intake and energy expenditure
(Berthoud and Morrison, 2008).
The brain gets a signal about the amount of fat
stored and secreted mainly by adipose, supplied by a
peptide hormone called Leptin. Leptin mRNA is
specifically expressed in fat cells. Leptin
concentrations in circulation, proportional to fat
reserves and BMI in normal subjects, and pulsatile
secretions are inversely related to hydrocortisone
levels. Glucocorticoids, estrogens and insulin and
are reduced by β-adrenergic agonists, triggering
316
Fakhrazi, R. and Tamin, T.
The Correlation between Physical Activity with Body Mass Index in Obesity Patient with Knee Osteoarthritis.
DOI: 10.5220/0009090103160320
In Proceedings of the 11th National Congress and the 18th Annual Scientific Meeting of Indonesian Physical Medicine and Rehabilitation Association (KONAS XI and PIT XVIII PERDOSRI
2019), pages 316-320
ISBN: 978-989-758-409-1
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

leptin formation. Leptin reaches the brain and enters
saturated transportation in the hypothalamus from
fat storage (Diamond and Eichler, 2002). When
hungry adipose tissue secretes leptin, CNS
stimulation, cold exposure, and exercise. Obesity,
glucocorticoids, glucose, and insulin can inhibit the
secretion of leptin from adipose tissue. When leptin
reaches the hypothalamus, NPY secretion is
inhibited, which normally reduces energy
expenditure, stimulates synthesis, stores fat, and
increases appetite. Adiponectin sensitizes tissues for
the effects of insulin. Obesity and insulin resistance
negatively regulate adiponectin secretion from
adipose tissue, where weight loss increases secretion
(Diamond and Eichler, 2002).
Body mass index, formerly called the Quetelet
index, is a measure to indicate nutritional status in
adults. BMI measured by weight in kilograms (kg)
divided by height in meters squared (kg / m2) (CDC
USA, 2009). In Asians, the limit of overweight is
23.0 kg / m2 which is lower than WHO criteria. The
suggested classification for Asians while still needs
to be revised because of further validation and
clinical symptoms. Some research that supports this
limit comes from Chinese living in Hong Kong (ko
et al 1999) where the risk of morbidity increases
with a BMI> 23.0 kg / m2.
Osteoarthritis (OA) is a disease caused by
mechanical and biological disorders that damage the
stability of the normal series of degradation and
synthesis of joint cartilage chondrocytes,
extracellular matrix, and subchondral bone. This can
occur due to various factors including genetic,
developmental, metabolic and trauma factors. OA
involves various tissues in the arthritic joints. OA
manifestations include morphological, biochemical,
molecular and biochemical changes in both cellular
and bone matrix that cause softening, fibrillation,
ulceration, loss of joint cartilage, sclerosis and
subchondral bone eburnation, osteophytes and
subchondral cysts. Clinically the symptoms that
appear in patients with OA are joint pain and
stiffness, limited mobility, crepitation, effusion,
various signs of inflammation without accompanied
by systemic effects (Sharma L, 2007).
Obesity is a risk factor for the development of
osteoarthritis. The association of height weight with
the incidence of OA is still said to be uncertain but
may involve cartilage degeneration due to overload.
Another mechanical factor is knee alignment. In
patients with knee varus, BMI appears to be related
to the severity of OA, especially medial tibiofemoral
OA.
A very important factor in the pathomechanics of
OA genu is the high and repeated burden on the
knee joint during walking and activity. During
walking, the load that passes through the knee joint
is not transmitted equally between the medial and
lateral compartments. The load on the medial
compartment is about 2.5 times greater than the load
on the lateral compartment. This is the reason for the
high prevalence of OA genu media compartments
(75% of all cases) rather than lateral compartments
(Enohumah KO and Imarengiaye CO, 2008).
Also, there are changes in the synovial
membrane and synovial fluid. Mild to moderate
inflammatory reactions occur in the synovial
membrane that contains cartilage articular
fragments. Whereas in the synovial fluid there is a
decrease in the concentration of molecular weight
and abnormal production of hyaluronate. Impaired
hyaluronate production and increased hyaluronate
breakdown which causes a decrease in hyaluronate
concentration. Changes in the synovial fluid also
result from an increase in water content and an
increase in pathological concentrations (Enohumah
KO and Imarengiaye CO, 2008).
Physical activity is defined as body movements
produced by skeletal muscles that require energy
expenditure. The most commonly used way to be
always active is by walking, cycling, recreation, and
sports that can be done at any level of skill and
pleasure (“WHO | Physical Activity,” 2019). MET is
a unit used to estimate the energy expended from
each activity (Miles, 2007). Understanding the level
of physical activity is the total energy needed (TEE)
or used in 24 hours divided by the basal metabolic
rate (BMR) for 24 hours.
The total energy needed in 24 hours can be
calculated based on the activities carried out in one
day and calculated the amount of energy needed for
these activities, then added up. The amount of
energy used can be seen based on the compendium
of physical activity. The purpose of this study is to
find whether there is a relationship between the level
of physical activity and body mass index in obese
patients with knee osteoarthritis. We hypothesize
that a decrease in physical activity caused by an
increase in BMI in patients with obesity and
osteoarthritis of the knee who seek treatment at the
obesity clinic.
2 METHODS
This study protocol was approved by the University
of Indonesia Ethics Committee and written consent
The Correlation between Physical Activity with Body Mass Index in Obesity Patient with Knee Osteoarthritis
317
was obtained from all the participants of the study.
The design of this study was cross-sectional with
consecutive sampling. The study was conducted on
obese patients with knee OA at the Obesity
Polyclinic of the Department of Medical
Rehabilitation at the National Center General
Hospital (Cipto Mangunkusumo Hospital/
University of Indonesia). The sample obtained was
37 women and 1 man based on the criteria for
sample acceptance with a diagnosis of Overweight
/obese (table 1) and OA of the knee, age > 50 years,
never had knee surgery before, can walk
independently without assistance, can communicate
well, and are willing to fill out informed consent.
The criteria for rejection in this study were patients
with a history of knee surgery, using walking aids,
having cardiorespiratory system disorders, having
knee deformity > 15
0
, experiencing cognitive
impairment or mental health disorders, impaired
balance, and were unwilling to participate in the
study.
Table 1: Asia Pasific BMI Classification.
Classification BMI (kg/m
2
) Risk of co-morbidities
Waist circumference
Men
Women
< 90 cm
<80 cm
90 cm
80 cm
Underweight < 18,5 Low Average
Normal range 18,5 – 22,9 Average Increased
Overweight
23
At risk 23 – 24,9 Increased Moderate
Obese I 25 – 29,9 Moderate Severe
Obese II
30
Severe Very severe
Samples that meet the inclusion criteria and do
not meet the exclusion criteria are given background
information on the research, objectives, and benefits
of the study. They were asked to sign the informed
consent provided if they agree to participate in this
study. Then the researchers conducted anamnesis,
height, and weight measurements, followed by
interviews. Interview of physical activities carried
out in one full day, starting from waking up, to
going back to sleep. Retrieval of data at 3 days a
week. 2 days between Monday to Friday, and 1 day
between Saturday and Sunday.
Table 2: PAL Classification.
Category PAL value
Sedentary or light activity lifestyle 1,40-1,69
Active or moderately active lifestyle 1,70-1,99
Vigorous or vigorously active lifestyle 2,00-2,40
All data in the 3 days were carried out with the
Compendium physical activity, then totaled and
divided by 3, then obtained the energy expended in
one day. Furthermore, energy expenditure is
calculated in one day by multiplication between the
energy expended by weight. Each sample is
calculated BMR with the Harris-Benedict formula.
Then calculate the level of physical activity (table 2)
with the division between energy expenditure (EE) /
BMR.
3 RESULT
In this study, a total sample of 38 people was
obtained. The largest sample in this study were
women. Education levels in both bachelor and non-
bachelor are in somewhat balanced proportion. This
study reveals that most of the subjects received a
rehabilitation program for more than one year.
Table 3: Subjects Characteristic.
Age
64.13 5.34
Sex
Male
Female
1 (2.6%)
37 (97.4%)
Height (cm)
152.55 6.68
Weight (kg) 64.00 (63.78-69.53)
BMI
28.61 3.05
Formal Education
Bachelor
Non-bachelor
17 (44.7%)
21 (55.3%)
Information, Education, and
Communication (IEC)
< 6 Months
6 Mo – 1 Yr
> 1 Yr
6 (15.8%)
3 (7.9%)
29 (76.3%)
PAL 1.52 (1.52-1.62)
KONAS XI and PIT XVIII PERDOSRI 2019 - The 11th National Congress and The 18th Annual Scientific Meeting of Indonesian Physical
Medicine and Rehabilitation Association
318
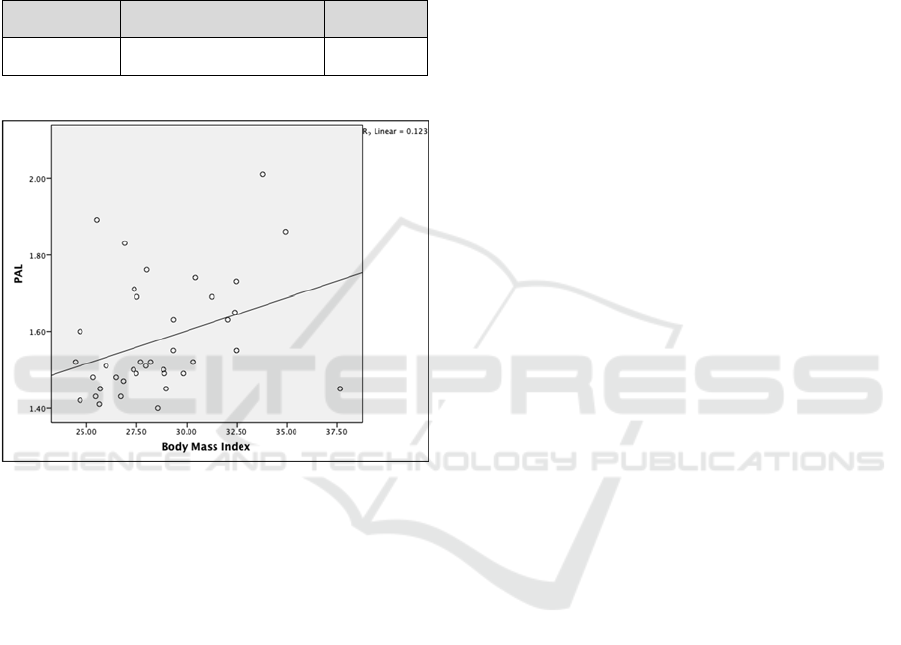
In this study, we want to find the correlation
between PAL and BMI. On the normality test we
found that the PAL variable is not normally
distributed (Table 3), a non-parametric correlation
test (spearman's) was used. In the Spearman test,
there was a significant relationship (p = 0.016)
between the PAL group and the BMI with a positive
weak correlation (r = 0.390)(Figure 1).
Table 4: Correlation test.
PAL (r)
BMI 0.390 0.016
S
S
Spearman’s
Figure 1: Scatterplots of the correlations BMI and PAL.
4 DISCUSSION
The largest sample in this study was women with the
length of therapy in rehabilitation clinics for more
than one year. 44.7%(17) of grade 1 obese samples
had undergone rehabilitation for more than one year.
It is a positive value of a patient's compliance with
treatment.
Rehabilitation treatment is most important for
the return of function in obese patients with OA
(Lau et al., 2011), is to provide education and
emotional approaches, so that patients have high
motivation to carry out rehabilitation not only during
treatment but also during daily activities. Some
patients with obesity have active physical activity
even very active, this proves that education to
always do activities, applied by patients in daily life.
In one study, an extra minute in the encounter
discussing these issues was associated with a 2.5-
fold increase inpatient recall. (Carroll et al., 2008)
With comprehensive education, patient compliance
will also increase In addition to increasing daily
activities, food intake and calories must also be
closely monitored.
Diet is an important factor if there are limitations
in daily activities (Oenema and Brug, 2003). the
sample we examined had an average age of 64 years,
most of them only spending time at home and
hospital. The differences in the associations between
BMI and PA in obese vs non-obese people indicate
that obesity may act as a barrier to PA (Hemmingsson
and Ekelund, 2007). A recent longitudinal cohort
study indeed suggested that obesity preceded low
levels of PA, but not the commonly held notion that
low levels of PA predicted the development of obesity
(Petersen et al., 2004).
In this study, a significant relationship was seen
between PAL and BMI. Our results show that one of
the grade 2 obese patients with osteoarthritis of the
knee has PAL which is very active. This shows that
people with high BMI do not necessarily have low
activity. This can be because the sample is an obese
patient with knee OA who is undergoing treatment
in an obesity clinic and get a lot of education. This
result shows that people with higher BMI who have
been visiting Obese Clinic routinely can have a high
activity level. Highlighting the importance and
effectiveness of proper rehabilitation treatment for
obese patients.
More than 75% of patients have undergone
rehabilitation for more than 1 year, where the
duration of this treatment has an impact on
increasing physical activity from the sample, making
it difficult to get a strong correlation value. Our
study has the advantage of researching health
facilities which are referral centers from various
regions. The rehabilitation program that is
implemented already has measurable targets for
patient achievement.
5 CONCLUSIONS
There is a significant relationship between physical
activity level and body mass index of someone
suffering from obesity with knee osteoarthritis with
a weak correlation.
REFERENCES
Australian Government, A. G., 2013. Clinical practice
guidelines for the management of overweight and
The Correlation between Physical Activity with Body Mass Index in Obesity Patient with Knee Osteoarthritis
319

obesity in adults, adolescents, and children in
Australia.
Berthoud, H.-R., 2002. Multiple neural systems
controlling food intake and body weight. Neurosci.
Biobehav. Rev. 26, 393–428. https://doi.org/10.
1016/S0149-7634(02)00014-3
Berthoud, H.-R., Morrison, C., 2008. The Brain, Appetite,
and Obesity. Annu. Rev. Psychol. 59, 55–92.
https://doi.org/10.1146/annurev.psych.59.103006.093551
Carroll, J. K., Fiscella, K., Meldrum, S. C., Williams,
G.C., Sciamanna, C. N., Jean-Pierre, P., Morrow, G.
R., Epstein, R. M., 2008. Clinician-Patient
Communication About Physical Activity in an
Underserved Population. J. Am. Board Fam. Med. 21,
118–127. https://doi.org/10.3122/jabfm.02.070117
CDC USA, 2009. Body Mass Index: Considerations for
Practitioners 4.
Diamond, F. B., Eichler, D. C., 2002. Leptin and the
Adipocyte Endocrine System. Crit. Rev. Clin. Lab.
Sci. 39, 499–525. https://doi.org/10.1080/
10408360290795565
Enohumah KO, Imarengiaye CO, 2008. Pain in
Osteoarthritis. Afr. J. Biomed. Res. 11, 119–128.
Hemmingsson, E., Ekelund, U., 2007. Is the association
between physical activity and body mass index obesity
dependent? Int. J. Obes. 31, 663–668.
https://doi.org/10.1038/sj.ijo.0803458
Lau, P. W., Lau, E. Y., Wong, D. P., Ransdell, L., 2011. A
Systematic Review of Information and
Communication Technology-Based Interventions for
Promoting Physical Activity Behavior Change in
Children and Adolescents. J. Med. Internet Res. 13,
e48. https://doi.org/10.2196/jmir.1533
Oenema, A., Brug, J., 2003. Feedback strategies to raise
awareness of personal dietary intake: results of a
randomized controlled trial. Prev. Med. 36, 429–439.
https://doi.org/10.1016/S0091-7435(02)00043-9
Petersen, L., Schnohr, P., Sørensen, T. I. A., 2004. A
longitudinal study of the long-term relation between
physical activity and obesity in adults. Int. J. Obes. 28,
105–112. https://doi.org/10.1038/sj.ijo.0802548
Rimmer, J., Schiller, W., Chen, M.-D., 2012. Effects of
Disability-Associated Low Energy Expenditure
Deconditioning Syndrome. Exerc. Sport Sci. Rev. 40,
22–29. https://doi.org/10.1097/JES.0b013e31823b8b82
Sharma L, K. D., 2007. Epidemiology of Osteoarthritis,
4th ed, Osteoarthritis Diagnosis, and Medical/Surgical
Management. Lippincott Williams & Wilkins,
Philadelphia.
Sugondo, S., 2006. Buku Ajar IPD, in: Buku Ajar IPD,
Perhimpunan Dokter Spesialis Penyakit Dalam
Indonesia. Jakarta, p. 439.
WHO | Obesity [WWW Document], n.d. . WHO. URL
https://www.who.int/topics/obesity/en/ (accessed
7.11.19).
WHO | Physical Activity [WWW Document], 2019.
WHO. URL http://www.who.int/dietphysicalactivity/
pa/en/ (accessed 7.4.19).
KONAS XI and PIT XVIII PERDOSRI 2019 - The 11th National Congress and The 18th Annual Scientific Meeting of Indonesian Physical
Medicine and Rehabilitation Association
320
