
Implementation of the ICF Concept in the Making of Problem
Framework based on Comprehensive Geriatric Assessment for
Physical Medicine and Rehabilitation Resident of Medical Faculty
University of Indonesia
Teffy Aulia Merry Dame
1
, Wanarani Alwin
1
,
Melinda Harini
1
1
Department of Physical Medicine and Rehabilitation, Dr. Cipto Mangunkusumo Hospital, University of Indonesia,
Jakarta, Indonesia
Keywords: International Classification of Functioning, Disability, and Health (ICF), Comprehensive Geriatric
Assessment (CGA)
Abstract: The Comprehensive Geriatric Assessment (CGA) is a multidisciplinary evaluation which the multiple
problems of elderly are uncovered, described, and explained, which the resources and strengths of the
person are cataloged, assessed and coordinated to make care plan which developed to focus interventions on
the person’s problems. In PMR, the International Classification of Functioning, Disability, and Health (ICF)
framework is fundamental for analysis and problem intervention. PMR residents expected to have a better
guidelines in establishing the CGA program. A Cross-sectional study with a quantitative approach carried at
the Medical Faculty University of Indonesia. The objective is to compare the process of making a problem
framework using the ICF concept based on a comprehensive geriatric examination with the problem-making
process without the use of the ICF concept and to evaluate the effectiveness of the ICF concept uses for
making problem framework based on CGA examination. All of the respondents agree that the ICF concept
makes an improvement in integrating, understanding, and analytical skills in the geriatric problem; defining
rehabilitation target, priority; and simplify communication with other colleagues and patients. On the other
hand, it takes more time (28,5%) and difficulty in writing of framework (35,7%). More respondents (85,7%)
agree that it facilitates in making functional diagnosis and prognosis. The ICF concept can help to make a
better comprehensive assessment of geriatric patients based on CGA.
1 INTRODUCTION
The percentage of the elderly population in
Indonesia continues to increase. In 2015 the number
of elderly people in Indonesia is 8.49% of the total
population of 21.70 million, in 2025 estimated that it
will be 11.83% and in 2035 will continue to increase
to 15.77% of total population (BPS, 2013). Elderly
patients have different characteristics with young
adult patients. Elderly patients often suffer from
various diseases, Mental function, impaired
mobility and independence, experience malnutrition,
and experience a decline in organ function. If in
these conditions elderly patients are stricken with an
illness, the patient may fall into a state of severe
illness. When the patient succeeds through the acute
phase, the recovery phase is still awaiting and will
take a long time. In the geriatric population, the
central point of attention to care is the patient as a
whole person, not just the illness he suffered. The
attention is not limited to individual patients but is
extended to include his family. For this reason, the
best approach is through an integrated approach
involving physical, mental, social, and spiritual
aspects. Geriatric patients who report greater
spirituality, are more likely to appraise their health
as good. Spirituality may be an important
explanatory factor of subjective health status in older
adults as physical, mental and social aspects
(DaelemanTP, 2004). Then a comprehensive
assessment is needed to set patient management
goals.
The CGA is “a multidisciplinary evaluation in
which the multiple problems of older persons are
uncovered, described, and explained, if possible, and
290
Dame, T., Alwin, W. and Harini, M.
Implementation of the ICF Concept in the Making of Problem Framework based on Comprehensive Geriatric Assessment for Physical Medicine and Rehabilitation Resident of Medical Faculty
University of Indonesia.
DOI: 10.5220/0009089602900295
In Proceedings of the 11th National Congress and the 18th Annual Scientific Meeting of Indonesian Physical Medicine and Rehabilitation Association (KONAS XI and PIT XVIII PERDOSRI
2019), pages 290-295
ISBN: 978-989-758-409-1
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
in which the resources and strengths of the person
are cataloged, need for services assessed, and a
coordinated care plan developed to focus
interventions on the person’s problems”. Physical
Medicine and Rehabilitation (PMR) Resident is
expected to be able to carry out a comprehensive
assessment of the elderly and can frame the problem
properly so that it can facilitate the problem
identification process for further intervention in the
elderly. The approach using the ICF framework
model when combined to identify problems found in
the elderly who have received a comprehensive
assessment through CGA is expected to facilitate the
process of identifying problems that occur to provide
optimal interventions for the elderly.
In PMR, the International Classification of
Functioning, Disability, and Health (ICF) framework
is fundamental for analysis and problem
intervention.ICF is a framework for describing and
regulating information about functions and
disabilities that can provide standard and conceptual
basic language for definitions and measurements of
health and disability. ICF offers an international
scientific tool for studying disability, in all its
dimensions especially in the geriatric population
which requires comprehensive assessment for
further therapy (World Health Organization, 2001).
The ICF was developed by the World Health
Organization to provide a framework to describe
health and health-related states and to suggest
standardized language to describe these states. (BPS,
2013). Based on the work of Nagi, the ICF model
shifts the focus of disablement from cause to impact,
from disability to health and function, and from a
static process to a dynamic process. As stated
previously, the ICF defines 3 domains of human
function (Figure): body function and structure,
activity, and participation. Body function and
structure refers to the anatomical and physiological
function of the body systems, and these body
functions and body structures are categorized into
the subdomains listed in Figure 2. Deficits in this
domain are called “impairments” (eg, muscle
weakness, restricted joint motion, poor
cardiorespiratory fitness) and often are identified,
measured, and treated. The activity domain
describes the ability of an individual to perform
specific tasks such as sweeping the floor, raking the
yard, or putting away groceries (Nagi, 1965 ).
Decrements in the activity domain are called
“limitations” and describe the difficulty an
individual has performing a particular task.
Rehabilitation goals often are aimed at reversing or
normalizing such activity limitations. The
participation domain describes the ability of a person
to be involved in life situations ( Jette AM, 2006 ).
Participation restrictions describe the reduced ability
of a person to maintain normal role functions and
interact with society. Rehabilitation interventions are
designed, directly or indirectly, to enhance
participation levels for every client at home, school,
or work; on the athletic field; or in any community
setting. In the ICF model, health conditions,
personal factors, and the environment interact
dynamically across the 3 domains of a body function
to help determine whether disordered function
results in disability. For example, if a geriatric
patient had a cancer treatment (eg, chemotherapy)
that causes a patient to develop unresolved
peripheral neuropathy and ankle weakness, this
patient may have a limited ability to walk
(limitation) and may require long-term use of an
ankle brace. Limited ability to walk could result in
an employment restriction for an active elderly.
Participation restrictions occur when activity
limitations cannot be sufficiently overcome to
maintain role functions in a person's normal
environment.
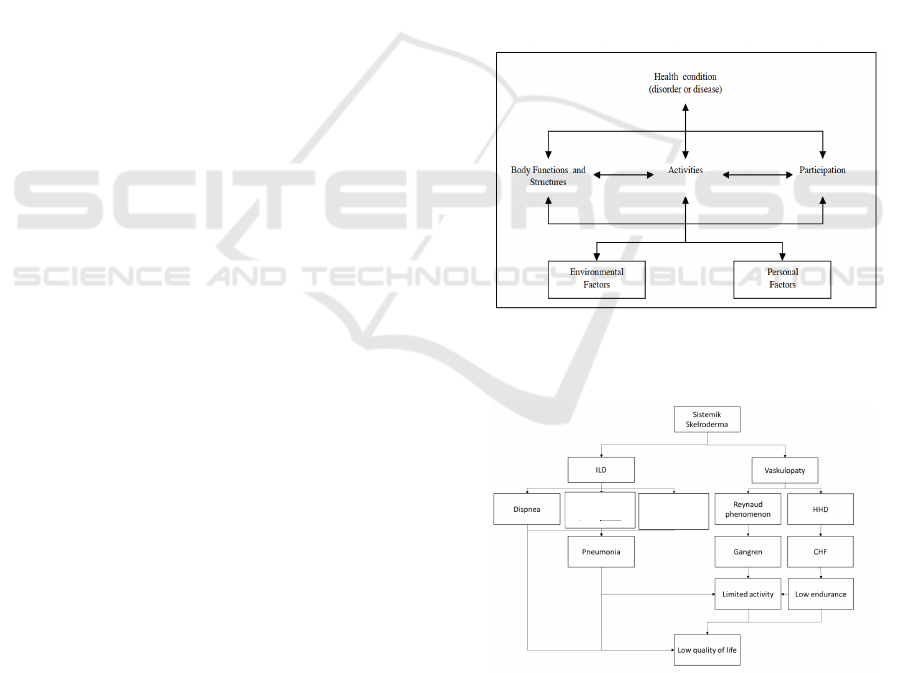
Figure 1: Interactions between the component of ICF
(World Health Organization. 2001).
Figure 2: Problem framework without using ICF concept
in Geriatric patient with Digital Ulcer in Scleroderma,
Community-Acquired Pneumonia, Chronic Heart Failure
Functional Class II, Hypertension, Chest expansion
problem, Low Endurance Cardiorespiration, Visual and
hearing Problems, Frailty, Risk of falls and decrease of
Quality of life.
Decreased
Chest
Expansion
Decreased
Cough Activity
Implementation of the ICF Concept in the Making of Problem Framework based on Comprehensive Geriatric Assessment for Physical
Medicine and Rehabilitation Resident of Medical Faculty University of Indonesia
291
In the PMR learning process, the most important
things are to recognize disability, premorbid factors
and the reciprocal relationship between. PMR
residents expected to make a rehabilitation program
with considering environmental and personal factors
that can be a facilitator or barrier to our programs.
All this time, PMR resident asked to make a
problem framework that including all those factors
without a certain format. Start from 2019, an ICF
concept was proposed to be used to make a problem
framework by problems found from CGA.
As an example of Using an ICF concept in
geriatric patient based on CGA in patient with
Digital Ulcer in Scleroderma, Community-Acquired
Pneumonia, Chronic Heart Failure Functional Class
II, Hypertension, Chest expansion problem, Low
Endurance Cardiorespiration, visual and hearing
Problems , Frailty, Risk of falls and decrease of
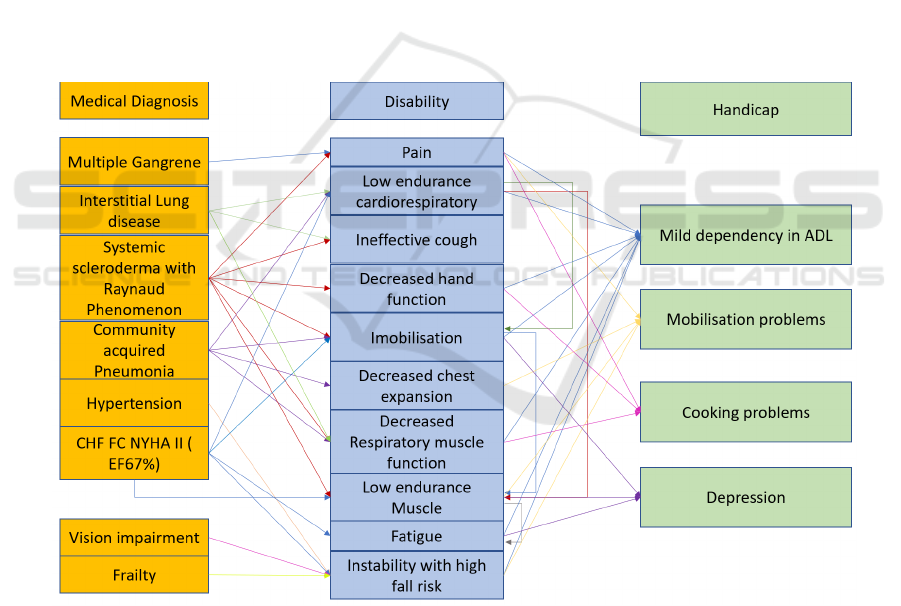
Quality of life can be seen in figure 3 and 4. From
the figure below, see that using an ICF concept
makes a more clear vision of what kind of
impairment, disability, and handicap happens in the
geriatric patient. We can classify at what stage
patients meet the disability, impairment and
handicap criteria So that we can take immediate
action to prevent deterioration of function in the
patient.
The purpose and benefit of this research are to
measure and compare the process of making a
problem framework using the ICF concept based on
comprehensive geriatric examination with the
problem-making process without the use of the ICF
concept and to evaluate the effectiveness of ICF
concept uses for making problem framework based
on CGA examination.
Figure 3: Problem framework using ICF concept in Geriatric patient with Digital Ulcer in Scleroderma, Community-
Acquired Pneumonia, Chronic Heart Failure Functional Class II, Hypertension, Chest expansion problem,
Low Endurance Cardiorespiration, Visual and hearing Problems, Frailty, Risk of falls and decrease of Quality of life.
2 METHODS
This is a cross-sectional study and a quantitative
approach. The study was conducted in a PMR
department - Rumah Sakit Cipto Mangunkusumo,
Medical Faculty University of Indonesia located in
Jakarta, Indonesia, between the months of April and
September 2019. PMR resident, Faculty of
Medicine, University of Indonesia who had gone
KONAS XI and PIT XVIII PERDOSRI 2019 - The 11th National Congress and The 18th Annual Scientific Meeting of Indonesian Physical
Medicine and Rehabilitation Association
292
through the Geriatric Division and had made a
problem framework based on CGA using the ICF
concept were included. The studied population
comprised of 14 PMR residents.
Data collection was supported by a structured
script to obtain personal and social information. The
data collection instrument was validated by experts
on the subject, concluding that the language and the
presentation of the items were pertinent to the
objective of the study.
Subjects will be asked to fill out a short closed
questionnaire about the method of making a problem
without and using the ICF concept ( Lichstenstein G,
2011). The questionnaire including 3 fields;
framework making process, problem management
and other clinical skills contains questions about the
comparison of time needed to make a framework,
writing process, differences of integrating,
understanding, and analytical skills in geriatric
problems, defining rehabilitation target, priority; and
simplify communication with other colleagues and
patients, facilitates in making functional diagnosis
and prognosis using ICF models in geriatric patients
as seen in table 1.
Table 1: Questionnaire list.
No Questionnaire Yes No
Framework Making
1 Using of ICF concept in
making problem
framework based on CGA
give a faster time than the
usual approach
2 Using of ICF concept can
simplify the writing
process of problem
framework based on CGA
Problem Management
3 Using of ICF concept help
me to integrate problems
found from CGA
4 Using of ICF concept help
me understanding
problems found from
CGA
5 Using of ICF concept
increase my analytical
skill to recognize social
and environmental factors
affect patient problems
6 Using of ICF concept
increase my analytical
skill to recognize
disability problem in the
patient
7 Using of ICF concept
increase my analytical
skill from problems found
from CGA
8 Using of ICF concept can
simplify the
communication of
problems found to another
division
9 Using of ICF concept help
me in presenting a list of
problems found to the
patient and their family
Other Clinical Skills
10 Using of ICF concept
facilitate to make a
functional diagnosis
11 Using of ICF concept
facilitate to make a patient
functional prognosis
12 Using of ICF concept
facilitate to decide
programs needed by the
geriatrician
13 Using of ICF concept
facilitate to set up
rehabilitation target in the
geriatric patient
14 Using of ICF concept help
me to determine problems
priority
3 RESULTS
Among the 14 resident included in the sample
with a mean age of 32,14 (± 3.8) years, a large
majority agree that ICF concept make an
improvement in integrating, understanding, and
analytical skills in geriatric problem; defining
rehabilitation target, priority; and simplify
communication with other colleagues and patients
(100 %). On the other hand, it takes more time
(28,5%) and difficulty in writing of framework
(35,7%). More respondents (85,7%) agree that it
facilitates in making functional diagnosis and
prognosis
Implementation of the ICF Concept in the Making of Problem Framework based on Comprehensive Geriatric Assessment for Physical
Medicine and Rehabilitation Resident of Medical Faculty University of Indonesia
293

Figure 4: Percentage of questionnaire agreement.
4 DISCUSSIONS
A questionnaire including 14 questions revealed the
first use of the ICF concept for making a problem
framework in a geriatric patient by PMR resident.
All of the respondents (100%) agree that the ICF
concept improves integrating, understanding, and
analytical skills in a geriatric problem. Respondent
agrees that using a framework based on the ICF
concept makes them more understanding of how to
analyze the problem found from CGA, so its easier
to defining rehabilitation targets and priority
problems in geriatric patients. The using of ICF
concept in a process to make a problem framework
in geriatric patient simplify communication with
other colleagues and patients, to communicate what
is need to support rehabilitation process to solve a
problem found in a geriatric patient. On the other
hand, 4 respondents (28,5%) reveal the using of the
ICF concept takes more time in the process to make
the framework compare to their usual approach.
However this is their first time implementing an ICF
concept to make a geriatric problem framework, so it
needs habituation in applying the ICF concept to
make a problem framework. We also revealed that 5
respondent showed that using an ICF concept make
a difficulty in writing of framework (35,7%). They
find a difficulty to recognize what problems should
be placed first of the many problems found from
CGA, but due to time, they admit that using the ICF
concept getting easier for them because of the
habituation process.
There is 12 respondent from 14 respondent
(85,7%) agree that it facilitates in making functional
diagnosis and prognosis, only 2 of 14 respondents
said an ICF concept did not support and make no
differences in deciding for diagnosis and prognosis
in geriatric patients compared to their usual
methods. Considering to make a functional diagnosis
and prognosis is important learning material for
PMR residents, this shows that along with the higher
frequency of contact with patients, PMR residents
will be more capable to make a functional diagnosis
and patient prognosis. Unlike the rehabilitation
programs, target and priority, which can find from
more sources, skills to set up prognosis and
functional diagnosis develop as the time they spend
with patient and habituation using the ICF concept.
Studies show that diagnosis alone does not
predict service needs, length of hospitalization, level
of care or functional outcomes. Nor is the presence
of a disease or disorder an accurate predictor of
receipt of disability benefits, work performance,
return to work potential or likelihood of social
integration. This means that if we use a medical
classification of diagnoses alone we will not have
the information we need for health planning and
management purposes. ICF makes it possible to
collect those vital data in a consistent and
internationally comparable manner. For basic public
health purposes, including determining the overall
health of populations, the prevalence, and incidence
of non-fatal health outcomes, and to measure health
care needs and the performance and effectiveness of
health care systems, we need reliable and
comparable data on the health of individuals and
populations. ICF provides the framework and
classification system for these purposes. With using
an ICF concept there is an increased recognition
among social planners and service agencies that
reductions in the incidence and severity of disability
in a population can be brought about both by
enhancing the functional capacity of the person and
by improving performance by modifying features of
the social and physical environment. ICF allows
analyzing the impact of these different interventions,
classifying domains of areas of life as well as the
environmental factors that improve performance
especially in the geriatric population ( WHO, 2002).
ICF is an essential basis for the standardization
of data concerning all aspects of human functioning
and disability around the world to evaluate health
care settings that deal with chronic illness and
disability, such as rehabilitation centers, nursing
homes, psychiatric institutions, and community
services. ICF is useful for persons with all forms of
disabilities, not only for identifying their health care
and rehabilitative needs but also in identifying and
measuring the effect of the physical and social
environment on the disadvantages that they
experience in their lives. From the viewpoint of
health economics, ICF will help monitor and explain
health care and other disability costs. Measuring
functioning and disabilities will make it possible to
KONAS XI and PIT XVIII PERDOSRI 2019 - The 11th National Congress and The 18th Annual Scientific Meeting of Indonesian Physical
Medicine and Rehabilitation Association
294

quantify the productivity loss and its impact on the
lives of the people in each society. The classification
will also be of great use in the evaluation of
intervention programs (WHO, 2002)
By using an ICF concept in geriatric patients
based on the problem found from CGA, we can
recognize impairment and disability problem, thus
we can prevent more deterioration which can lead to
a handicap. Health Education can be applied earlier
to prevent deterioration of function as a secondary
prevention, aims to reduce the impact of the disease
by detecting and treating disease or injury as soon as
possible to halt or slow its progress, encouraging
personal strategies to prevent re-injury or recurrence,
and implementing programs to return people to their
original health and function to prevent long-term
problems.
5 CONCLUSIONS
ICF concept can help to make a better
comprehensive assessment of geriatric patients
based on CGA and effective ways to improve
problem management and other clinical skills of
PMR residents.
REFERENCES
Badan Pusat Statistik. 2013. Data untuk perencanaan
pembangunan dalam era desentralisasi [internet].
Jakarta: BPS;[cited 18th July 2019]. Available from:
http://www.datastatistikindonesia.com
Daeleman TP, et al. 2004. Religion, Spirituality, and
Health Status in Geriatric Outpatients. Ann Fam
Med.2:49-53.
JetteAM. 2006. Toward a common language for function,
disability, and health. Phys Ther. 86:726–734
Lichtenstein G, Thorne T, Cutforth N, Tombari ML. 2011.
Development of a National Survey to Assess Student
Learning Outcomes of Community-Based Research.
Journal of Higher Education Outreach and
Engagement; 15: 2-7
World Health Organization. 2001 International
Classification of Functioning, Disability, and Health
(ICF). Geneva: World Health Organization.
World Health Organization. 2002. Towards a common
language for functioning, disability, and Health (ICF).
Geneva. World Health Organization
Implementation of the ICF Concept in the Making of Problem Framework based on Comprehensive Geriatric Assessment for Physical
Medicine and Rehabilitation Resident of Medical Faculty University of Indonesia
295
