
Validity and Reliability of 2 Minutes Walking Test in Frailty Elderly
Niken Pratiwi
1
, Rwahita Satyawati
1
, Damayanti Tinduh
1
, Soenarnatalina Melaniani
2
, Mahmuddah
Mahmuddah
2
1
Department of Physical Medicine and Rehabilitation, Dr. Soetomo General Hospital, Faculty of Medicine,
University of Airlangga, Surabaya, Indonesia
2
Department of Biostatistics and Population Study, Faculty of Public Health, University of Airlangga, Surabaya, Indonesia
nlk3np@gmail.com
Keywords: 2MWT, 6MWT, Frailty, Elderly, Validity, Reliability
Abstract: Frailty and age-related conditions are associated with morbidity and mortality. The 6-minute walk test
(6MWT) has been recommended by the American Thoracic Society to measure exercise capacity, but it is
time-consuming for the investigator and exhausting for frailty elderly. This study aims to investigate the
validity and reliability of 2 minutes walking test (2MWT) as measurements of physical performance. A
cross-sectional study was performed. Each subject performed 6MWT as a gold standard and two trials of
2MWT in two consecutive days at approximately the same time. The walking test was performed in the
same corridor with the same starting point. The subject was allowed to used ambulation aid. Frailty was
measured using the Cardiovascular Health Study score. The final subjects included sixty elderly (26 men, 34
women with mean age 73.40 years old). Pearson's r correlation of VO2max between 6MWT and 2MWT
was strong (r= 0.791, p=0.000). The 6MWT and 2MWT showed excellent reliability (ICC=0.926, p=0.000).
The 2MWT was shown to be a reliable and valid test for assessment of exercise capacity following
rehabilitation in frailty elderly. It is practical, simple, and well-tolerated by frailty Elderly.
1 INTRODUCTION
Frailty is a typical health condition associated with
the aging process that is when the body's system
gradually loses its ability to work. About 10% of
people over 65 years experience frailty, increasing to
between a quarter and half of those aged over 85
years (Clegg, 2013). Frailty can be a cause of
disability in some patients (BGS, 2014). Decreased
mobility, functional capacity and/or basic activities
of daily life (ADL) such as bathing, dressing, and
walking occur in 20-30% of the elderly population
over 70 years (Manton, 2000).
Mobilization ability is one of the most important
factors for assessing the level of health and well-
being in the elderly. Functional mobility and
independence are the main objectives of the
rehabilitation program. Functional capacity reflects a
person's cardiorespiratory capacity. Assessment of
cardiorespiratory ability was generally assessed by
measuring maximum oxygen uptake (maximal
oxygen uptake/VO2max) (Sykes, 2004), but the
measurement of VO2max directly requires complex
equipment and laboratories, specific and expensive
equipment, supervision of a professional medical
team, and also consideration of the motivation and
physical effort of the subject to carry out the training
test. Therefore an alternative test is needed to
estimate VO2max with the submaximal training test
(Katch, 2011).
The 6-minute walking test (6MWT) is a test
standard developed by the American Thoracic
Society in 2002 (ATS, 2002). However, this test has
limitations on the elderly, especially the elderly with
frailty. A 6-minute walking test (6MWT) is too
tiring, takes longer and increases the risk of falling
for elderly frailty, 2-minute walking test (2MWT)
can be an alternative. The 2-minute walking test is
considered to have the ability to assess exercise
tolerance (Hiengkaew, 2012).
At present, there are no research data on the
validity and reliability of 2MWT in elderly with
frailty, and 2MWT is an easy, inexpensive and safer
walking test for frailty elderly people. Researchers
242
Pratiwi, N., Satyawati, R., Tinduh, D., Melaniani, S. and Mahmuddah, M.
Validity and Reliability of 2 Minutes Walking Test in Frailty Elderly.
DOI: 10.5220/0009088802420247
In Proceedings of the 11th National Congress and the 18th Annual Scientific Meeting of Indonesian Physical Medicine and Rehabilitation Association (KONAS XI and PIT XVIII PERDOSRI
2019), pages 242-247
ISBN: 978-989-758-409-1
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

are interested in researching the validity and
reliability of 2MWT in the elderly with frailty.
2 METHODS
This study was an observational analytic study with
a cross-sectional study to determine the correlation
between the values of anthropometric parameters of
body weight, height, age, and gender from 2MWT
with VO2max from 6MWT. Besides, an assessment
of 2MWT reliability (test-retest) was also carried out
by measuring 2 times (1 consecutive day) by the
same examiner (interrater). We hypothesize that the
2-minute walking training test (2MWT) has validity
and reliability on the assessment of functional
training capacity compared to 6MWT in frailty
elderly.
The research will be conducted at Griya Wreda
Jambangan Surabaya and carried out in November
2018. The target population of this study was Frailty
Elderly with a sample size of 60 subjects taken
based on simple random sampling, which was,
calculated accordingly the following formula:
(1)
Description:
Alpha Error Rate (5%)
Beta Error Rate (10%)
In this study, inclusion and exclusion criteria
were applied. Inclusion Criteria are: 1) Age more
than or equal to 60 years. 2) Frailty criteria based on
the Cardiovascular Health Study. 3) Good hearing
function. Checked with a modified whisper test and
said to be normal if you could hear 80% of all the
items tested according to the procedure. 4) Good
vision function. Judged by a visual inspection using
Snellen u cards at a distance of 6 meters. 5) Can
understand and follow verbal instructions well. 6)
Independent ambulation with or without walking
aids. 7) Willing to participate in this study by
signing an informed consent sheet after obtaining an
explanation.
While the exclusion criteria used in this study
were 1) Being undergoing a routine physical
exercise program that aims to improve walking
speed and lower limb muscle mass in the past month.
2) Severe cognitive impairment was assessed using
the Mini-Mental State Examination questionnaire
(MMSE <23). 3) Having dementia. 4) Suffering
from severe cardiorespiratory disorder 5) Having
acute-severe knee OA according to clinical
appearance, 6) Chronic illness / that causes other
long-term disabilities (eg. ambulation disorders due
to stroke, uncontrolled diabetes, balance disorders
due to intracranial or extracranial processes, visual
disturbances, etc). 7) Falling risk is assessed by the
Timed Up and Go Test, for risk fell in the elderly
population ≥ 13.5 seconds.
Data from the results of the examination of
anthropometric response parameters are displayed
descriptively in table form. For correlation analysis
between the values of weight, height, age and
walking speed when 2MWT with VO 2max when
the 6MWT training test is used the Pearson
correlation test. If a good correlation is obtained,
then it will be followed by linear regression between
each parameter of 2MWT and multiple regression
with VO 2max when the training test runs for 6
minutes to obtain the prediction (formula) of VO
2max prediction. The interclass correlation
coefficient (ICC) test was used for reliability
analysis (test-retest reliability) of VO 2max 2MWT.
Data analysis was performed using SPSS 22 and
Lisrel.
3 RESULTS
This research was conducted by setting a place at the
Jambangan Surabaya nursing home. The number of
elderly who can be ambulated is 102 elderly.
Twenty-two elderly were included in the exclusion
criteria due to 8 dementia disorders, 5 elderly with
visual impairment and 8 elderly with hearing
impairment. Sixty elderly subjects who met the
inclusion and exclusion criteria completed the
2MWT I (first) and II (second) tests, as well as the
6MWT test. The characteristics of the research
subjects are shown in Table 1.
Validity and Reliability of 2 Minutes Walking Test in Frailty Elderly
243
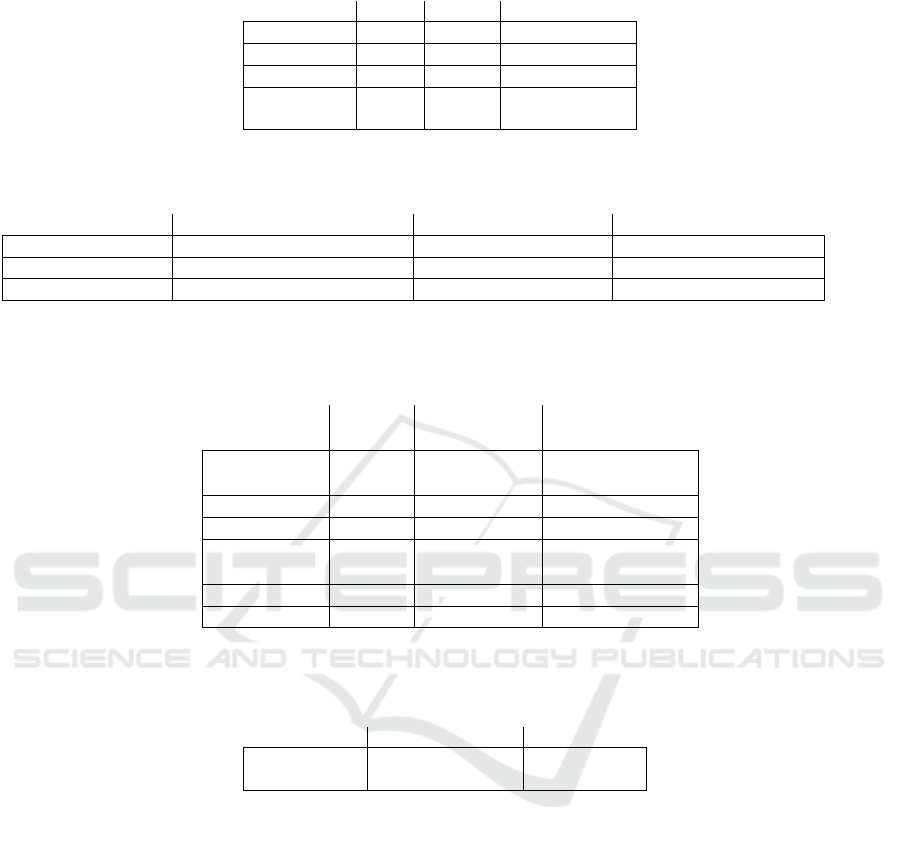
Table 1: Characteristics of Research Subjects.
Variable
Min
Maks
Mean ± SD
Age (years)
60
96
73.40 ± 8.928
Weight (Kg)
33
78
51.70 ± 10.617
Height (cm)
130
175
153 ± 0.103
BMI
(Kg/m2)
14.84
33.32
21.93 ± 3.918
Nb: SD = Standard Deviation, Min = Minimum Value, Max = Maximum Value.
Table 2: Percentage of Frailty.
Sex
Frailty
Pre frailty
Total
L
7 (26.9 %)
19 (73.1 %)
26 (100 %)
P
16 (47.1%)
18 (52.9 %)
34 (100 %)
Total
23 (38.3 %)
37 (61.7 %)
60 (100 %)
Nb: Sex = Gender, L = Male, P = Female.
Table 3: Correlation of VO
2max
2MWT and 6MWT
Parameter
VO
2max
6MWT
VO
2max
2MWT
VO
2max
6MWT
r
1
0.791**
p
0.000
N
60
60
VO
2max
2MWT
r
0.791**
1
p
0.000
N
60
60
Description: r = Pearson correlation coefficient, p = p value, N = number of subjects. Significant correlation at p <0.01 (2-
tailed)
Table 4: Test-retest reliability of Vo2Max 2MWT.
Parameter
ICC
CI 95%
VO
2max
0.925
0.874 –
0.955
Description: ICC = Interclass Correlation Coefficient, CI Confidence Interval, TDS = Systolic Blood Pressure, TDD =
Diastolic Blood Pressure
KONAS XI and PIT XVIII PERDOSRI 2019 - The 11th National Congress and The 18th Annual Scientific Meeting of Indonesian Physical
Medicine and Rehabilitation Association
244

Based on the Frailty score Cardiovascular Health
Study (CHS) Table 3.2 found 26 research subjects
male 7 (26.9%) including frailty and 19 (73.1%) pre-
frailty people. For female subjects, 16 (47.1%) were
frailty and 18 (52.9%) were pre-selected frailty.
To calculate the VO2max correlation from
2MWT and 6MWT, then carried out the 2MWT
validity assessment. The vo2max value obtained
from the equation calculated using Confirmatory
Factor Analysis. Table 3.3 illustrates the relationship
between the VO 2max value of the 2MWT and
6MWT submaximal load training tests. From the
calculation of the Pearson correlation coefficient the
strong correlation was found (r = 0.791; p = 0.000)
between the VO value of 2max. The training test
was two minutes and six minutes.
2MWT reliability (test-retest) assessment was
carried out by comparing VO2max values on two
measurements (between 2MWT I and 2MWT II)
within a span of 1 day carried out by the same
examiner (interrater), at the same hour and place.
4 DISCUSSION
In this study, 60 elderly subjects met the inclusion
criteria and were not included in the exclusion
criteria and were willing to take part in the study
after signing informed consent. The age of the
subjects in this study was 60-96 years (mean 73.40
years). The body mass index of the subjects in this
study ranged from underweight to obese, namely
14.84 - 33.32 Kg/m
2
. The normal value of the
Indonesian body mass index is 18.5 - 25 Kg/m
2
(Harahap, 2005). All research subjects completed
the 2MWT I (first) training test and 6MWT training
test at the first meeting, as well as the 2MWT II
(second) training test 1 day after the first. Before
carrying out the training test the subject's
cardiorespiratory parameters were measured. The
mean resting heart rate at the first meeting (before
2MWT I) was 77.20 beats/minute. The average
resting heart rate is not much different when
compared to the average resting heart rate during the
second meeting (before 2MWT II), with an average
of 77.30 beats/minute. From the paired t-test there
was no significant difference between
cardiorespiratory parameters (heart rate, systolic
blood pressure, diastolic blood pressure, and pulse
blood pressure) pre-2MWT I and pre-2MWT II with
p values for all parameters >0.05. With this, it can be
said that the conditions or cardiorespiratory
parameters break the subjects between the first and
second meetings in this study are the same. In this
study, the VO2max equation is calculated using
Confirmatory Factor Analysis.
Prediction of VO2max values can be done using
anthropometric parameters. This, of course, can be
done if the anthropometric parameters have a good
correlation with the VO2max value when the
submaximal stress test measured using 6MWT. The
statistical analysis used for this purpose is linear
regression. From the linear regression analysis, a
regression equation will be obtained which states the
relationship of the variable you want to predict with
the measured variable (Tumbelaka, 2014). In this
study, the predicted variable is the value of VO2max
and the measured variable is the anthropometric
parameter namely age, weight, height, and walking
speed (m / min). The regression equation for
VO2max prediction is shown in Table 4.
Table 4: Regression equation for prediction of VO
2max.
Equation
VO
2max
I
(R
2
= 71.4 %)
- 116.244 + (1.17 x umur)
II
(R
2
= 66.6%)
18.164 – ( 0.918 x BB)
III (R
2
= 62.4%)
105.432 – ( 0.878 x TB)
IV (R
2
= 93.6%)
- 0.854 x
Running speed
Description: BB = Body Weight, TB = Height, R =
Coefficient of determination
From the regression equation above we can see
that the highest r-value (r = 1.00) is obtained if all
four parameters (weight, height, age, sex, and
walking speed) during the 2MWT training test are
included in the calculation. The higher the R-value
of a regression equation, the higher the accuracy of
the equation (the prediction results are getting closer
to the actual value with a smaller error rate). Thus,
the best equation from the 2MWT training test for
the prediction of VO2max:
The submaximal training test developed in this
study is a 2-minute walking training test (2MWT).
VO
2Max
(mL/KgBB/minute) =
2.809 + (0.868xU) – (0.0412 x BB) –
(0.382 x TB) – (0.474 x Walking speed) (2)
Nb:
- U = Age (Years)
- BB = Weight (Kg)
- TB = Height (Cm)
- Running Speed (m/minutes)
- Estimation of Error Standart = 0.119
Validity and Reliability of 2 Minutes Walking Test in Frailty Elderly
245

These submaximal training test subjects were asked
to walk for 2 minutes in a 30m corridor. Unlike the
6MWT submaximal test as the gold standard, 2
minutes test in this study was chosen to minimize
muscle fatigue, especially in untrained subjects.
Besides, the cardiorespiratory physiological
condition remained (steady-state) when the exercise
test was reached after 2-3 minutes (Prentice, 2011).
So that 2 minutes was sufficient to obtain the
cardiorespiratory parameters of the condition during
the training test. Maximum oxygen consumption
(VO2max) is the largest amount of oxygen that can
be inhaled during a training test, which involves a
large part of the total muscle mass. This is
considered the best measure of cardiovascular
fitness and aerobic capacity.
This study found that there was a significant
increase in walking distance in the 2MWT repeat
trial in frailty elderly. According to a study
conducted by Brooks in 2007 found an increase in
walking distance in amputee patients and heart
surgery patients who did not experience
improvement after three trials. Repeated trials in
pediatric patients with cystic fibrosis revealed no
significant difference in walking distance. In
contrast, repeated trials in pediatric patients with
cystic fibrosis revealed no significant difference in
walking distance (Upton, 2015). Guyatt et al.
Showed that, in repeated trials of patients with
limited chronic airflow and/or chronic heart failure,
there was a stable training effect after two trials. An
interesting finding from this study is that walking
distance in 2 minutes increased during the two trials.
VO2max value generally decreased according to
age. Decreasing VO2max 8-10% per decade in both
mobile and inactive populations (Pin, 2012). In VO
2max women are lower because muscle mass is
smaller than men. Because both of these affect VO
2max (Tumbelaka, 2014), anthropometric
parameters are used to find out VO2max. In this
study, 2MWT validity was assessed by analyzing
anthropometric parameter correlations (age, weight,
height, sex, and walking speed) at 2MWT against
VO2max values measured using equations
calculated using Confirmatory Factor Analysis.
From the calculation of the Pearson correlation
coefficient, we found a significant correlation (r =
0.791) between the VO2max value at 2MWT and
6MWT.
Based on the interpretation of the Pearson (r)
correlation coefficient by Tumbelaka et al, the
correlation is stated to be good if the value of r =
>0.8; medium if the value of r = 0.6 - 0.79; weak if
the value of r = 0.4 - 0.59; and very weak if the
value of r = <0.4. Correlation values obtained in this
study indicate that the 2MWT submaximal training
test has quite good validity in the assessment of
cardiorespiratory capacity in frailty elderly.
The VO2max correlation value in this study is
not much different when compared with the VO
2max correlation value in a study conducted by
Bohannon et a1 and Bernstein et a1 both evaluated
concurrent validity in individuals with respiratory
disease and reported that the running distance at
2MWT was highly correlated with walking distance
in 6 and 12 minutes running test (r = 0.892–0.995).
Bernstein examined the validity of individuals with
COPD and reported that walking distance in 2
minutes was moderate to maximal correlated and
strongly correlated with submaximal oxygen
consumption (r = 0.45; r = 0.55; respectively).
Furthermore, Upton et al. Concluded that, in
children with cystic fibrosis who have a near-normal
respiratory function, 2MWT is a measure that is
more discriminatory than the peak expiratory flow
rate. In individuals with lower limb amputations, a
distance of 2MWT correlates with measures of
physical function and prosthetic use.
Reliability Test is a fundamental measurement
property that is relatively easy to determine and
quantified in terms of the level of consistency and
repetition when managed properly in similar
circumstances for certain populations. Assessment
of reliability (test-retest reliability) of 2MWT in this
study was conducted by comparing the parameter
values of age, weight, height, gender and walking
speed with VO 2max using the prediction formula
on two measurements (between 2MWT-I and
2MWT-II) in the 1 consecutive day by the same
examiner (interrater).
The 2MWT reliability for age parameters is quite
good with a value of R 2 = 71.4% (SE = 0.151).
2MWT reliability for weight parameters is quite
good with a value of R 2 = 66.6% (SE = 0.135).
Reliability for the Height parameters is quite good
with an ICC value of 62.4% (SE = 0.145).
Reliability for the sex parameter is quite good with
an ICC value of 58.1% (SE = 3.132). If the four
parameters (weight, height, age, gender, and walking
speed) during the 2MWT training test are included
in the calculation, the ICC score is very good at
92.5%. The higher the ICC value of an equation, the
higher the reliability. This shows that the 2MWT
submaximal training test has good reliability in the
assessment of cardiorespiratory capacity.
KONAS XI and PIT XVIII PERDOSRI 2019 - The 11th National Congress and The 18th Annual Scientific Meeting of Indonesian Physical
Medicine and Rehabilitation Association
246

5 CONCLUSIONS
The 2-minute walking exercise test (2MWT) has
good validity where anthropometric parameters of
weight, height, age, sex and walking speed when
2MWT have a significant correlation with VO 2max
values during the 6MWT submaximal training test.
The 2-minute walking test (2MWT) has very good
reliability (test-retest reliability).
REFERENCES
American Thoracic Society (ATS)., 2002. ATS Statement:
Guidelines for the Six-Minute Walk Test. American
Journal of Respiratory Critical Care
Medicine,166(111117).DOI:10.1164/rccm.166/1/111
Bernstein, ML., Despars, JA., Singh, NP., Avalos, K.,
Stansbury, DW., Light RW., 1994, Reanalysis of the
12 minute walk-in patients with chronic obstructive
pulmonary disease, Chest, 105:163–7.
Bohannon, RW., Bubela, D., Magasi, S., McCreath, H.,
Wang, YC., Reuben, D., Gershon, R., 2014,
Comparison of walking performance over the first 2
minutes and the full 6 minutes of the Six-Minute Walk
Test. BMC Research Notes, 7, 269.
http://doi.org/10.1186/1756-0500-7-269
British Geriatric Society (BGS)., 2014. Fit For Frailty,
Consensus Best Practice Guidance for the Care of
Older People Living with Frailty in Community and
Outpatient Setting, Majory Warren House, London.
Brooks, Dina., 2002, Reliability of the two-minute walk
test in individuals with transtibial amputation,
Archives of Physical Medicine and Rehabilitation,
83(11), 1562–1565.
Brooks, D., Parsons, J., Hunter, JP., Devlin, M., Walker, J.,
2001, The 2-minute walk test as a measure of
functional improvement in persons with lower limb
amputation, Arch Phys Med Rehabil, 82:1478–83.
Clegg, A., Young, J., Iliffe, S., Rikkert, MO., Rockwood,
K., 2013, Frailty in elderly people, Lancet,
381(868):752-762.
Guyatt, GH., Sullivan, MJ., Thompson, PJ., Fallen, EL.,
Pugsley, SO., Taylor, DW., 1985, The 6-minute walk:
a new measure of exercise capacity in patients with
chronic heart failure. Can Med Assoc J, 132(8):919-23.
Harahap, H., Widodo, Y., Mulyati Sri., 2005, Penggunaan
berbagai cut-off indeks massa tubuh sebagai indikator
obesitas terkait penyakit degeneratif di Indonesia. Gizi
Indon, 31, pp. 1-12.
Hiengkaew, V., Jitaree, K., Chaiyawat, P., 2012, Minimal
detectable changes of the Berg balance scale, Fugl–
Meyer Assessment Scale, Timed "Up & Go" Test, gait
speeds, and 2-minute walk test in individuals with
chronic stroke with different degrees of ankle plantar
flexor tone, Archive of Physical Medicine
Rehabilitation, 93:1201–1208.
Katch, VL., McArdle, WD., Katch, F. I., 2011, Measuring
and Evaluating Human Energy-Expenditure Capacities
During Exercise, In: Essential of Exercise Physiology,
5th edition, Philadelphia: Lippincott William &
Wilkins, pp. 203-233.
Manton, KG., Land, KC., 2000, Multidimensional
Disability/Mortality Trajectories at Ages 65 and Over:
The Impact of State Dependence, Social Indicators
Research, 51: 193.
Pin, TW., Lewis, J., 2012, Pilot normative study on 2- and
6-minute walk tests on typically developing children
in Australia, Australasian Academy of Cerebral Palsy
and Developmental Medicine Conference.
Developmental Medicine Children Neurology, 54:85.
Prentice, W., 2011, Maintaining Aerobic Capacity and
Endurance during Rehabilitation. In W. Prentice,
Rehabilitation Techniques for Sports Medicine and
Athletic Training, New York: McGraw-Hill, pp. 214-
25.
Sykes, K., Roberts, A., 2004, The Chester Step Test - a
Simple yet Effective Tool for The Prediction of
Aerobic Capacity, Physiotherapy, 90, pp. 183- 188.
Tumbelaka, A. R., Riono, P., Sastroasmoro, S.,
Wirjodiarjo, M., Pudjiastuti, P., Firman, K., 2014,
Pemilihan Uji Hipotesis. In: S. Sastroasmoro & S.
Ismael, eds. Dasar-dasar Metodologi Penelitian Klinis.
Jakarta : CV. Sagung Seto, pp. 328-350.
Upton CJ, Tyrrell JC, Hiller EJ., 2015. Two-minute
walking distance in cystic fibrosis. Arch Dis Child;
63:1444–1448
.
Validity and Reliability of 2 Minutes Walking Test in Frailty Elderly
247
