
A Preliminary Study on the Effect of Low Energy Extracorporeal
Shock Wave Therapy as a Treatment for Shoulder Adhesive
Capsulitis in Hasan Sadikin Hospital Bandung, Indonesia
Megi Virgiabanon Otafirda, Tertianto Prabowo, Rachmat Zulkarnain Goesasi,
Irma Ruslina Defi and Novitri
Department of Physical Medicine and Rehabilitation, Dr. Hasan Sadikin General Hospital, University of Padjadjaran,
Bandung, Indonesia
Keywords: Adhesive Capsulitis, Frozen Shoulder, rESWT, Rehabilitation.
Abstract: Adhesive capsulitis or frozen shoulder describes the common shoulder condition characterized by painful
and limited active and passive range of motion. Extracorporeal shock wave therapy (ESWT) suggested as
alternative treatment for adhesive capsulitis. Aim of this study was to determine the effect of low energy
rESWT on adhesive capsulitis related to shoulder pain, shoulder range of motion, and function of the
shoulder joint. The study design was an interventional, experimental study. A series of single-case studies
was undertaken with patients shoulder adhesive capsulitis who came to the physical medicine and
rehabilitation department Hasan Sadikin Hospital. Each patient received four weeks applications of low
energy rESWT, 1 week apart. Outcome measure using NRS, ROM and DASH questionnaire. Result: Five
patient, 4 Female and 1 Male were included, with mean age of patient is 50,60 ± 2,97 years old, mean
length of symptoms 12 ± 6,96 month. Pain intensity, passive shoulder range of motions, and functional
outcome are improved after 4 weeks intervention rESWT(p<0,05). The low energy rESWT resulted in
significant clinical and statistical improvement pain, passive shoulder ROM and functional outcomes in
patients with shoulder adhesive capsulitis. Low energy rESWT as effective treatment alternative in
shoulder adhesive capsulitis.
1 INTRODUCTION
Adhesive capsulitis or frozen shoulder describes the
common shoulder condition characterized by painful
and limited active and passive range of motion. The
etiology of frozen shoulder remains unclear;
however, patients typically demonstrate a
characteristic history, clinical presentations, and
recovery.
Frozen shoulder is reported to affect 2% to
5% of the general population. Individuals with
primary frozen shoulder are commonly between 40
and 65 years old, and the incidence appears higher in
females than males (Kelley et al. 2009). More than
50% of frozen shoulder patients still have sequelae
of symptoms after years of undergoing therapy,
resulting in decreased quality of life of the patient
(Guiloff et al. 2015).
Extracorporeal Shock Wave Therapy (ESWT) is
defined as an acoustic wave characterized by high
pressure peaks (100 MPa), rapid pressure increase
with rise times of less than <10 nsec, shorter life
cycle less than 10 ms, and energy density range of
0.003 – 0.890 mJ/mm (Gerdesmeyer et al. 2003).
Radial ESWT is a pneumatic type shock wave,
producing low energy to medium compared with
traditional focused ESWT and lower penetration
depth than fESWT (3 cm vs 12 cm). This shock
wave will be focused at the tip of the applicator
without having to focus energy to the target point.
Systematic review studies and meta-analyses
reported rESWT has better result compared to
fESWT in patients with plantar fasciitis because the
result has a larger therapeutic area, so focusing
therapy becomes less important, does not require
local anesthesia and is more affordable (Chang et al.
2012).
Several studies have shown that ESWT is a
relatively non invasive therapeutic modality with
proven effectiveness, convenience and safety of the
therapy of musculoskeletal problems (Ioppolo et al.
Otafirda, M., Prabowo, T., Goesasi, R., Defi, I. and Novitri, .
A Preliminary Study on the Effect of Low Energy Extracorporeal Shock Wave Therapy as a Treatment for Shoulder Adhesive Capsulitis in Hasan Sadikin Hospital Bandung, Indonesia.
DOI: 10.5220/0009088302150219
In Proceedings of the 11th National Congress and the 18th Annual Scientific Meeting of Indonesian Physical Medicine and Rehabilitation Association (KONAS XI and PIT XVIII PERDOSRI
2019), pages 215-219
ISBN: 978-989-758-409-1
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
215

2014). Extracorporeal shock wave therapy has been
suggested as an alternative treatment for refractory
shoulder pain due to calcific or noncalcific tendinitis
and may be an alternative to expensive and risky
surgical interventions (Bannuru et al. 2013). Recent
studies show the use of ESWT has been suggested
for the treatment of adhesive capsulitis (Vahdatpour
et al. 2018).
The main purpose of the adhesive capsulitis
treatment is to reduce pain, increase the range of
joint motion and improve the function of the
shoulder. Therapeutic effect of ESWT is to help
revascularization, stimulation, bone reactivation and
healing of connective tissues, which will lower the
pain and improve shoulder joint function.
Shockwave modality uses sound waves of high or
low energy that impart rapid fluctuations of pressure
to tissues. The degree of energy imparted to the
tissues is measured as energy flux density (EFD).
There are many manufacturers of ESWT devices.
Shockwave therapy is usually classified as high,
medium, or low energy, according to the EFD
administered. Although there is no consensus on the
threshold values, a commonly used grouping defines
EFD 0.08 to less than 0.27 mJ/ mm
2
as low energy,
0.28 to less than 0.59 mJ/mm
2
as medium energy, and
more than 0.60 mJ/mm
2
as high energy (Speed 2004).
Several studies have been conducted to observe
the effects of low dose and high dose rESWT in
patients with shoulder pathology. Low dose rESWT
does not reduce pain or improve function compared
with placebo treatment in patients with chronic
tendinitis of the rotator cuff (Kolk et al. 2013).
Systematic review show that high energy fESWT is
more effective than low energy fESWT for
improving pain and shoulder function in chronic
calcific shoulder tendinitis (no similar effects were
seen in noncalcific tendinitis) and can result in the
complete resolution of calcifications (Bannuru et al.
2013). Studies that conducted in adhesive capsulitis
patients reported more effective responses with
higher energy and proper session intervals in patients
with adhesive capsulitis, hematomas as adverse
event was reported in this study (Hussein et al.
2015).
Adverse effects of ESWT were dose dependent,
patients who received high or medium energy ESWT
reported more adverse events than those who
received low energy ESWT. The most commonly
reported adverse events related to ESWT were
temporary increase acute pain and local reactions,
such as swelling, local erythema, petechiae, small
bruises and hematomas. No serious side effects have
been reported (Bannuru et al. 2013).
The aim of this study was to determine the effect
of low energy rESWT in adhesive capsulitis patient
related to shoulder pain, shoulder range of motion,
and function of the shoulder joint.
2 METHODS
The study design was an interventional, experimental
study. A series of single case studies (n=5) was
undertaken with patients shoulder adhesive capsulitis
who visited the outpatient clinic of Physical
Medicine and Rehabilitation Department Hasan
Sadikin Hospital. The participants received oral and
written information about the study and were
informed of the potential risks of treatment. Written
informed consent was obtained from all subjects
before the baseline evaluation. Ethical clearence was
given by the Health Research Ethic Committee
Hasan Sadikin General Hospital.
The inclusion criteria were patients 40 - 65 years
with shoulder pain and restriction in ROM in at least
three directions, (i.e. flexion, abduction, external
rotation, and internal rotation) for a duration of at
least 6 months. Exclusion criteria were history of
shoulder fracture, shoulder dislocation or
subluxation, previous surgery on the shoulder, pre-
rupture tendon or tendon rupture in the shoulder
cancer, glenohumeral or acromioclavicular arthritis,
presence of severe osteoporosis, inflammatory
disorders, pulmonary diseases, bleeding disorders,
pregnancy, any neuromuscular disorders, implanted
pacemaker and unwillingness to participate in the
study.
The rESWT was administered by the same
experienced trained doctor with the EMS Swiss
Dolorclast Smart20
®
(EMS Electro Medical Systems
Corporation, Dallas, TX, USA).
Each patient received four applications of
rESWT, 1 week apart, with 2000 impulses per
session. The air pressure of the device was set to 2.5
bars, frequency of 8 Hz, energy flux density (EFD)
0.11 mJ/mm
2
, and the impulses were applied with a
15 mm applicator.
The shock waves were delivered to two separate
locations per session with the coupling gel. The first
location was applied 1000 impulses in a posterior-to-
anterior direction on the posterior side of the
shoulder joint located beneath the lateral border of
the scapular spine. The second location was applied
remaining 1000 impulses of the total 2000 impulses
per session in an anterior-to-posterior direction of the
anterior shoulder joint, was about one finger breadth
lateral to the coracoid process (Hussein et al. 2015)
(Vahdatpour et al. 2018).
KONAS XI and PIT XVIII PERDOSRI 2019 - The 11th National Congress and The 18th Annual Scientific Meeting of Indonesian Physical
Medicine and Rehabilitation Association
216
The outcome measure consists of pain intensity
during rest and activity over the past 24 hr was
assessed on Numeric rating Scale (NRS), the
involved shoulder passive flexion abduction and
passive external internal rotation were measured by a
goniometer, function that measured by the
Disabilities of the Arm, Shoulder and Hand (DASH)
questionnaire which has been validated in
Indonesian language (Magetsari 2010). Home-based
exercise that performed by patients, incidence of
painful activity or other adverse events are
documented. All outcome measures were taken at
baseline before the treatment, after 4 weeks (at the
end of treatment) by experienced trained doctor.
The obtained data were analyses were performed
using The Statistical Package for Social Sciences
(SPSS) software ver.18.0 (SPSS Inc., Chicago, IL,
USA). A paired t-test was conducted to determine
statistical differences in the variables between the
pre and post treatment. Values are presented as mean
± standard deviation for data with a normal
distribution, and p<0.05 was considered statistically
significant.
3 RESULTS
Five patients with shoulder adhesive capsulitis who
met the selection criteria were recruited. Subject
more likely to be female, with mean age of patients
is 50,6 years old and mean length of symptoms 12
month (Table 1). All the subjects complete the
intervention phase.
Table 1: Subject demographic characteristics.
No Variable n = 5
1.
2.
3.
Gender, Female ; Male
Age (years), Mean ± SD
Length of symptom (month),
Mean ±SD
4 ; 1
50,6 ± 2,97
12 ± 6,96
Shoulder pain is statistically significantly
decreased for all the subjects. Mean pain NRS was
decreased from 6 point at the baseline to 1 point after
4 weeks treatment. (Table 2)
Table 2: Numeric rating scale at initial and after 4 weeks
intervention of Reswt.
Pain
NRS initial
(Mean ± SD)
NRS 4 weeks
(Mean ± SD)
p
NRS 6 ± 0.71 1.20 ± 0.44 0.000
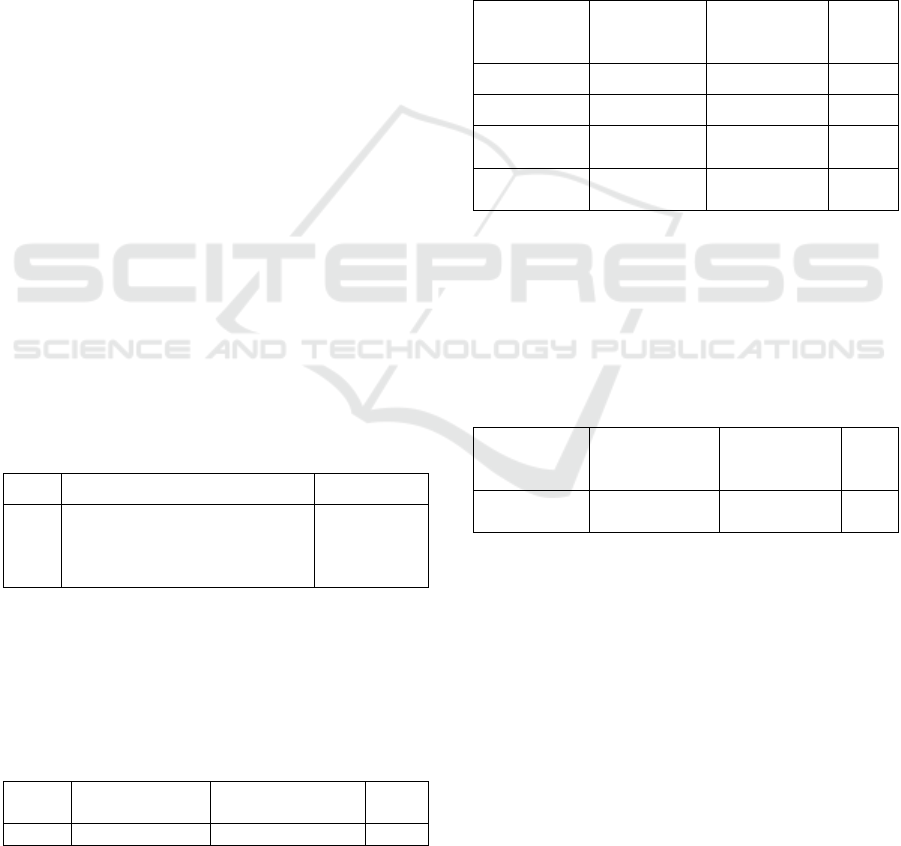
Mean passive shoulder range of motions are
statistically significantly increased in all planes after
4 weeks after radial rESWT (Table 3). Shoulder
flexion range of motion was increased from 126
degrees at baseline to 156 degrees after the
treatment. Shoulder abduction range of motion was
increased from 76 degrees at baseline to 111 degrees
after the treatment. Shoulder external rotation range
of motion was increased from 23 degress at baseline
to 48 degrees after the treatment. Shoulder internal
rotation range of motion was increased from 43
degrees at baseline to 63 degrees after the treatment.
Table 3: Shoulder range of motion at initial and after 4
weeks intervention of rESWT.
Passive
Shoulder ROM
ROM initial
(Mean ± SD)
ROM
4 weeks
(Mean ± SD)
p
Flexion 126 ± 21.91 156 ± 20.73 0.003
Abduction 76 ± 17.82 111 ± 27.48 0.011
Eksternal
Rotation
23 ± 14.83 48 ± 11.51 0.001
Internal
Rotation
43 ± 12.04 63 ± 13.04 0.003
Function that measured by the DASH
questionnaire improved after 4 weeks after radial
rESWT (Table 4). There was a statistically
significant decreased in mean DASH scores from
53 at baseline to 16 after the treatment.
Table 4: Functional (DASH score) at initial and after 4
weeks intervention of rESWT.
Functional
DASH Score
initial
(Mean ± SD)
DASH Score
4 weeks
(Mean ± SD)
p
DASH
questionnaire
53 ± 10.64 16,98 ± 11.47 0.01
Three subjects were reported discomfort or pain
when rESWT is applied at the first week of
treatment, because of that the rESWT application
was interrupted, but all of the patients were able to
completed therapy. There are no adverse events that
reported in this study.
4 DISCUSSIONS
In the present preliminary study, five patients with
adhesive capsulitis assigned to receive rESWT
treatment. This study has reported the successful
positive change use of rESWT in treating patients
A Preliminary Study on the Effect of Low Energy Extracorporeal Shock Wave Therapy as a Treatment for Shoulder Adhesive Capsulitis in
Hasan Sadikin Hospital Bandung, Indonesia
217

with shoulder adhesive capsulitis. Clinically and
statistically significant differences were shown in
pain, passive shoulder ROM and functional
outcomes that measure in rESWT treated patients.
The characteristics of the all subjects in the
present study consist of age, onset, symptoms, were
truly representative of the reported shoulder adhesive
capsulitis patient population.
The shock waves were delivered to two separate
locations at posterior-to-anterior direction and
anterior-to-posterior direction. In the present study,
we did not deliver rESWT in a third oblique
direction into the glenohumeral joint at about one
finger breadth beyond the anterior border of the
acromion tip (Chen et al. 2014) because the
arthroscopic findings showed that adhesions occur
more in the descendants fold and surrounding
synovium (Vahdatpour et al. 2018). Therefore,
stimulation from anterior and posterior directions is
more effective than of the lateral direction
(Vahdatpour et al. 2018).
The present study results in pain, passive
shoulder ROM and functional outcomes are similar
to those reported by Hussein et al., who performed a
double-blind RCT to evaluate the effectiveness of
rESWT that applied 2000 impulses each session,
with an air pressure of 3.5 bars, an EFD of 0.16
mJ/mm
2
and a frequency of 8 Hz and proper session
intervals. Adverse events that reported in those
studies is hematomas, which lasted from 2 to 4 days,
were that observed in 5.6% patients; no associated
discomfort or pain was reported and the rESWT
application was not interrupted (Hussein et al. 2015).
This present study using rESWT with air pressure of
2.5 bar, with the same frequency and interval as the
previous study, and EFD of 0.11 mJ/mm
2
that
considered to be a low energy dose (Speed 2004),
resulting significant changes in all outcome
measures; no adverse events (hematomas, etc) as
found in previous studies.
Studies that conducted rESWT in adhesive
capsulitis patients using several intervals. Previous
study that applied rESWT with an intervals 10 to 14
days show that low dose rESWT does not reduce
pain or improve function in chronic rotator cuff
tendinitis patient (Kolk et al. 2013). This present
study show more effective responses rESWT with
proper session intervals that similar with previous
study that applied rESWT in adhesive capsulitis
patient using 1 weeks intervals (Hussein et al. 2015)
(Vahdatpour et al. 2018).
Shock wave therapy stimulates soft-tissue
healing, increases blood flow to the treated site and
induces an inflammatory-mediated healing process,
and has been used in treating soft-tissue disorders
(Chen et al. 2014). Shock wave therapy using
fESWT was reported successful treating pathological
shoulder conditions, previous use of in primary
shoulder adhesive capsulitis and frozen shoulder,
(Chen et al. 2014)(Vahdatpour et al. 2018) while the
reported use of rESWT also successful treating
frozen shoulder (Hussein et al. 2015).r
The present study shows that
effect of rESWT
for hyperstimulation analgesia and
neovascularization could be attributed to the pain
relief (Yuan et al. 2018). Effect ESWT for anti-
inflammatory, antifibrotic effects, tissue healing, and
increased flexibility of the collagen fibers and
tendons, could be attributed to increase of the range
of motion (Vahdatpour et al. 2018). Consequent
functional improvement of shoulder joint would
result from the decrease in pain and the increase in
mobility.
The present study has several limitations. This
study had a small sample size and there is no control
group. The follow up time was too short to
determine the longterm effects of treatment. We
suggest to do a further investigation with larger
sample size, with short and long term evaluation for
effect of low dose rESWT on adhesive capsulitis
patient with comparison to conventional therapy.
5 CONCLUSIONS
The low energy rESWT resulted in significant
clinical and statistical improvement pain, passive
shoulder ROM and functional outcomes in patients
with shoulder adhesive capsulitis. It could be
considered low energy rESWT as an effective
optimal treatment alternative in shoulder adhesive
capsulitis, and safe without serious adverse event.
REFERENCES
Bannuru R, Flavin N, Vaysbrot E, Harvey W. 2013. High-
energy extracorporeal shock-wave therapy for treating
chronic calcific tendinitis of the shoulder. Annals of
internal medicine. vol. 160.
Chang K, Chen S, Chen W, Tu Y, Chien K. 2012.
Comparative effectiveness of focused shock wave
therapy of different intensity levels and radial shock
wave therapy for treating plantar fasciitis: a systematic
review and network meta-analysis. Arch Phys Med
Rehabil. vol. 93.
Chen C, Hu C, Weng P, Huang Y, Chiang C, Chen C,
Tsuang Y. 2014. Extracorporeal shockwave therapy
improves short-term functional outcomes of shoulder
KONAS XI and PIT XVIII PERDOSRI 2019 - The 11th National Congress and The 18th Annual Scientific Meeting of Indonesian Physical
Medicine and Rehabilitation Association
218

adhesive capsulitis. Journal of Shoulder and Elbow
Surgery. vol. 23, no. 12, pp.1843–1851.
Gerdesmeyer L, Wagenpfeil S, Haake M et al. 2003.
Extracorporeal shock wave therapy for the treatment of
chronic calcifying tendonitis of the rotator cuff: a
randomized controlled trial. JAMA, vol. 290, no. 19,
pp.2573–80.
Guiloff L, Gerdesmeyer L, Moya D, Ram S. 2015. Current
knowledge on evidence-based shockwave treatments
for shoulder pathology. International journal of
surgery. vol. 24. pp.171-178
Hussein AZ, Donatelli RA. 2015. The efficacy of radial
extracorporeal shockwave therapy in shoulder
adhesive capsulitis : a controlled, clinical study.
European journal of physiotherapy. vol. 9169
Ioppolo F, Rompe JD, Furia JP, Cacchio A. 2014. Clinical
application of shockwave therapy (SWT) in
musculoskeletal disorders. European journal of
physical and rehabilitation medicine. vol. 50. no. 2.
pp. 217–230.
Kelley MJ, McClure PW, Leggin BG. 2009. Frozen
shoulder: evidence and a proposed model guiding
rehabilitation. Journal of orthopaedic and sport
physical therapy, vol. 39, no. 2, pp.135–148.
Kolk A, Yang K, Tamminga R. 2013. Radial
extracorporeal shock-wave therapy in patients with
chronic rotator cuff tendinitis. The british editorial
society of bone & joint surgery. vol. 95. no. 11. pp.
1521–1526.
Magetsari R. 2010. Sensitiveness of the constant-murley’s
shoulder and quick dash as an outcome measure for
midshaft clavicle. Malaysian orthopaedic journal. vol.
4. no. 1. pp. 4–7.
Speed CA. 2004. Extracorporeal shock-wave therapy in
the management of chronic soft-tissue conditions. The
british editorial society of bone & joint surgery. vol.
86. no. 2. pp. 165–171.
Vahdatpour B, Taheri P, Zade AZ, Moradian S. 2018.
Efficacy of extracorporeal shockwave therapy in
frozen shoulder efficacy of extracorporeal shockwave
therapy in frozen shoulder. International Journal of
Preventive Medicine. vol. 5. no.7. pp. 875 - 881.
Yuan X, Zhou F, Zhang L, Zhang Z, Li J. 2018. Analgesic
effect of extracorporeal shock wave treatment
combined with fascial manipulation theory for
adhesive capsulitis of the shoulder : a retrospective
study. Biomed research international. vol. 2018.
A Preliminary Study on the Effect of Low Energy Extracorporeal Shock Wave Therapy as a Treatment for Shoulder Adhesive Capsulitis in
Hasan Sadikin Hospital Bandung, Indonesia
219
