
Biomechanics of Shoulder Injury in Athletes
Tirza Z. Tamin
Department of Physical Medicine and Rehabilitation, Dr. Cipto Mangunkusumo General Hospital,
Faculty of Medicine, University of Indonesia, Jakarta, Indonesia
tirzaediva.tamin@gmail.com
Keywords : Biomechanics of Shoulder, Shoulder Problems
Abstract : Balancing mobility and stability, the biomechanics of the shoulder provides optimal use of the thumb and
hand. More than a glenohumeral joint, the shoulder complex consists of four joints and numerous muscles
and ligaments. Injuries to the shoulder result from overuse, extremes of motion, and excessive forces.
This review describes basic shoulder biomechanics, their role in impingement and instability, and how
imaging can detail shoulder function and dysfunction.
1 INTRODUCTION
The shoulder is an engineering marvel, designed to
allow humans to maximize use of the opposable
thumb and hand in three-dimensional space. The
term shoulder is often used interchangeably with
glenohumeral joint, but the shoulder complex
actually consists of four joints and many ligaments
and muscles working synergistically. Limited bony
contact between the humeral head and glenoid fossa
allows extended range of motion at a cost of relative
instability. There must be a balance between
mobility and stability to maintain proper func- tion,
and it is this balance that embodies the biomechanics
of the shoulder complex.
Mechanical shoulder pathology typically results
when overuse, extremes of motion, or excessive
forces overwhelm intrinsic material properties and
disrupt the delicate balance of the shoulder complex
resulting in tears of the rotator cuff, capsule, and
labrum.
By reviewing basic biomechanical fundamentals
of the shoulder complex, we hope to further provide
the reader with a background to more fully
understand typical causes of more common shoulder
problems, such as impingement and instability, as
well as complex problems in the overhead athlete,
who often exhibits combined features of
impingement and instability.
2 DISCUSSION
2.1
Basic Biomechanics Of Shoulder
The glenohumeral joint is fundamentally the
central component of the shoulder complex, and yet,
like most successful groups and teams, it does not
work alone but rather depends on many individual
efforts. The other joints of the shoulder complex
include the sternoclavicular (SC), acromioclavicular
(AC), and scapulothoracic joints. The purpose of
these joints of the shoulder complex is to move and
stabilize the glenoid optimally during upper
extremity movement, similar to the coordinated
effort required to balance a spinning basketball on
your finger or a book on your head (Armfield et al,
2003).
2.2 Sternoclavicular Joint
The SC joint is a saddle joint that is a true synovial
joint. It is the only articulation of the shoulder with
the axial skeleton. Its saddle shape allows clavicular
elevation and depression (45 to –10 degrees),
anterior and posterior translation of about 15 degrees
(also called protraction and retraction, respectively),
and 50 degrees of posterior rotation along the long
axis of the clavicle. The bony articulation of the
joint consists of the primarily convex surface of
medial clavicle with the mostly concave surface of
the clavicular facet of the sternum. The SC joint
Tamin, T.
Biomechanics of Shoulder Injury in Athletes.
DOI: 10.5220/0009064200950104
In Proceedings of the 11th National Congress and the 18th Annual Scientific Meeting of Indonesian Physical Medicine and Rehabilitation Association (KONAS XI and PIT XVIII PERDOSRI
2019), pages 95-104
ISBN: 978-989-758-409-1
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
95

contains an intra-articular disc that helps with shock
absorption. The joint is strongly reinforced by the
anterior and posterior SC ligaments and capsule as
well as the interclavicular ligament and
costoclavicular ligaments (Armfield et al, 2003).
2.3 Acromioclavicular Joint
The AC joint is a plane joint. This type of joint
allows limited translation and rotation of two
relatively flat surfaces. The two surfaces of the
acromion and proximal clavicle are relatively
congruent but contain a variably sized intra-articular
disc that helps transmit forces evenly. The joint
provides a link between SC motion and scapular
positional changes via the strut configuration of the
clavicle. Because there is little motion at this joint,
movement initiated at the SC joint is transmitted into
scapular sliding and rotation along the
scapulothoracic plane. Joint stability results from the
AC joint capsule and its superior thickening called
the superior AC ligament. The connection between
the scapula and clavicle is further reinforced via the
coracoclavicular ligaments. In the past the joint
capsule was considered to be a relatively weak
structure, but cadaver studies have shown that
surgical transection of the capsule leads to increased
translation across the joint and these excess forces
may predispose the coracoclavicular ligaments to
failure (Debsi et al, 2001).
2.4 Scapulothoracic Joint
The scapulothoracic articulation is not a true
joint but rather the interface of the sliding scapula on
the thoracic cage. Scapular movement is essential
for upper extremity movement and it provides a
stable base for movement at the glenohumeral joint.
Scapular movement has been described in multiple
planes, including upward elevation and downward
depression, upward and downward rotation, anterior
and posterior movement along the thoracic cage
termed protraction and retraction as well small
adjustments along the AC joint plane. The major
muscles responsible for scapular movement include
the trapezius, levator scapulae, serratus anterior, and
rhomboids. Although often not considered a part of
the shoulder complex, spinal positioning is also
important for optimum scapular positioning.
2.5 Glenohumeral Joint
The fundamental central component of the shoulder
complex is the glenohumeral joint. It has a ball and
socket configuration with a surface area ratio of the
humeral head to glenoid fossa of about 3:1 with an
appearance similar to a golf ball on a tee. Overall,
there are minimal bony covering and limited contact
areas that allow for extensive translational and
rotational ability in all three planes via combinations
of several muscles.9 Stability is created through both
static (passive) and dynamic (active) mechanisms.
Static stabilizers include concavity of the glenoid
fossa, glenoid fossa retroversion and superior
angulation, glenoid labrum, which enhances glenoid
fossa depth by about 50%, the joint capsule and
glenohumeral ligaments, and a vacuum effect from
negative intra-articular pressure. It is estimated that
the labral structures represent 10 to 20% of
stabilization forces. Rotator cuff and deltoid muscle
mass also help compress the joint at rest. All of these
static restraints are important at rest, except for the
glenohumeral ligaments, which seem to be important
at extremes of motion.
During upper extremity movement the effects of
static stabilizers are minimized and dynamic or
active stabilizers become the dominant forces
responsible for glenohumeral stability. Dynamic
stabilization is merely the coordinated contraction of
the rotator cuff muscles that create forces that
compress the articular surfaces of the humeral head
into the concave surface of the glenoid fossa. This
phenomenon is known as concavity compression
and must occur during glenohumeral motion or
unwanted humeral head translation and instability
may occur, which can create forces that overload
native structures causing pathologic conditions.
Determining exact range of each movement is
difficult due to accompanying shoulder girdle
movement (Armfield, et al, 2003).
2.6 Arm Elevation
Although simply raising one’s arm is a complex task,
this motion occurs via the combination of
glenohumeral and scapulothoracic motion, together
known as scapulohumeral rhythm. This motion
usually takes place in the scapular plane, which is
about 40 degrees anterior to the coronal plane.
Overall, the ratio of glenohumeral to scapulothoracic
motion is 2:1. Initially, most motion in the first 25 to
30 degrees occurs at the glenohumeral joint. Beyond
this point, scapulothoracic motion begins and
movement at both joints occurs with a nearly 1:1
KONAS XI and PIT XVIII PERDOSRI 2019 - The 11th National Congress and The 18th Annual Scientific Meeting of Indonesian Physical
Medicine and Rehabilitation Association
96

ratio (Armfield et al, 2003). In addition, the humerus
must undergo external rotation to not only clear the
greater tuberosity posteriorly but also loosen the
inferior glenohumeral ligaments (IGHLs) to allow
maximum elevation. These osteokinematics require
appropriate coordinated contraction of the rotator
cuff muscles and the scapular stabilizers. The
anterior deltoid and supraspinatus muscles contract
in a coordinated fashion to initiate abduction. The
upper trapezius, lower trapezius, rhomboids, and
serratus anterior work together to create scapular
rotation.
The remainder of the rotator cuff muscles work
together to provide dynamic stability by ensuring
that the humeral head is compressed against the
glenoid fossa (concavity-compression principle).
This combined effect of rotator cuff muscular forces
results in net force effect (or summation vector)
known as a net joint reaction force. The joint
reaction forces must remain balanced during motion
via proprioreceptive feedback. If unbalanced
stability is compromised. The notion of a force
couple can be thought of in its simplest terms as a
tug of war contest between two teams. The sum
force (or vector) of the winning team causes the rope
to move in their direction. Imagine if there were
three teams; the rope would travel in a different
direction based on the strongest two teams. Now try
to imagine the complexity of the upper extremity
movement with over 20 different-sized muscles
contracting at slightly different times in all three
planes to create a desired motion.
2.7 Pitching Mechanics
Although there are many other sports that involve
overhead activity, baseball pitchers have been
studied as the prototypical overhead athlete. Most
information about the mechanics of throwing was
obtained with electromyographic analysis, high-
speed videography, and three dimensional motion
analysis in baseball pitchers. The motion of pitching
has been divided into different phases, including
wind up, early cocking, late cocking, acceleration,
deceleration, and follow-through (Armfield et al,
2003).
The critical stages with respect to the shoulder
are late cocking, acceleration, and deceleration
phases. During these phases shoulder muscle activity
and load are maximized and the shoulder is most
vulnerable to injury. Coordination with the lower
legs and trunk is essential. During early arm cocking,
scapular stabilizers are active. Deltoid and
supraspinatus activity allows abduction with the
supraspinatus compressing the humeral head in the
glenoid fossa to prevent displacement. In the late
arm-cocking phase, increased activity in the
infraspinatus and teres minor creates extreme
external rotation and helps keep the humeral head
centered within the glenoid fossa, preventing
anterior displacement. This phase is also
characterized by activity in the subscapularis,
pectoralis major, and latissimus dorsi to help
stabilize and strengthen the anterior aspect of the
shoulder to prevent anterior translation of the
humeral head.
it also forces the head of the
humerus forward which places significant
stress on the ligaments in the front of the
shoulder. Over time, the ligaments loosen,
resulting in greater external rotation and
greater pitching speed, but less shoulder
stability
(Armfield et al, 2003)
.
During the acceleration phase there is high
activity of the internal rotators (latissimus dorsi,
pectoralis major, and subscapularis) with
complimentary activation of teres minor posteriorly
in an effort to center the humeral head. At the same
time scapular stabilizers are actively contracting to
create a stable base for humeral movement during
which time large angular and torsional forces are
created. During deceleration all posterior muscles
are active, especially teres minor, which
eccentrically contracts to limit internal rotation.
Once the ball is released, follow-through
begins and the ligaments and rotator cuff
tendons at the back of the shoulder must
handle significant stresses to decelerate the
arm and control the humeral head.
Figure 1: Pitching Mechanism.
2.8 Mechanical Abnormalities of the
Shoulder
Many people believe that many overhead athletes
experience subclincal instability (i.e., no subluxation
or dislocation on physical exam), which leads to
contact of the humeral head and labrum causing
pathology of the rotator cuff and surrounding labrum.
This subclinical instability is known as functional or
Biomechanics of Shoulder Injury in Athletes
97

microinstability and different theories regarding the
pathomechanics exits.
The two most commonly described mechanical
dysfunctional abnormalities of the shoulder are
rotator cuff impingement and glenohumeral
instability. Typical connotations of impingement
include individuals over 40 with pain during
movement. Instability stereotypically affects young
athletic males with gross instability resulting in
dislocation. For rotator cuff dysfunction that can be
intermingled, particularly in the overhead athlete
(Armfield et al, 2003).
2.9 Rotator Cuff Dysfunction
Most rotator cuff tears are due to end-tage
mechanical impingement of the cuff by the
coracoacromial arch during arm elevation has been
the cornerstone of diagnosis and treatment of rotator
cuff dysfunction. Bigliani correlated acromial
morphology, Aoki analyzed acromial slope, and
others have identified factors that cause narrowing
of the supraspinatus outlet that leads to impingement
and cuff tears. The coracoacromial ligament is
attached to the undersurface of the acromion and the
tip of the coracoid. It is often enlarged in patients
with rotator cuff pathology. It also serves as a
restraint to glenohumeral superior migration in end-
stage cuff tears. Traction forces at its acromial and
coracoid attachments may lead to spur formation,
resulting in subacromial and subcoracoid
impingement. Impingement involving narrowing of
the supraspinatus outlet is known as extrinsic or
outlet impingement.
6
Secondary extrinsic
impingement results from inferior narrowing of the
outlet from the rising humeral head in the setting of
instability or scapulothoracic dysfunction.
Regardless of primary or secondary types, both
forms repetitively damage the cuff tissue and
predispose it to eventual failure (Armfield et al,
2003).
This concept emphasizes the need for a
biomechanically stable rotator cuff. A person could
have a small cuff tear and be highly symptomatic
depending upon the location of the tear and its effect
on the balance of forces in the shoulder. Small
tendon tears can induce reflex inhibition of muscle
contractility, which can further lead to cuff
imbalance and symptoms, whereas a small
perforative full-thickness tear may be
biomechanically silent and clinically meaningless.
Consequently, it is important to describe not only the
type of tear but also its size, extent, and exact
location for the referring surgeon (Pandev and Jaap,
2015).
Muscles of the rotator cuff are active during
various phases of the throwing motion.
16
During the
late cocking and early acceleration phases, the arm is
maximally externally rotated, potentially placing the
rotator cuff in position to impinge between the
humeral head and the posterior-superior glenoid.
Known as “internal impingement” or “posterior
impingement,” this may place the rotator cuff at risk
for undersurface tearing (articular sided).
Conversely, in the deceleration phase of throwing,
the rotator cuff experiences extreme tensile loads
during its eccentric action, which may lead to injury
(Dugas and Andrew, 2003). Rotator cuff tears in the
overhead athlete may be of partial or full thickness.
The history of shoulder pain either at the top of the
wind-up (acceleration) or during the deceleration
phase of throwing should alert the examiner to a
rotator cuff source of pain or loss of function. Any
history of trauma, changes in mechanics, loss of
playing time, previous treatments, voluntary time off
from throwing, and history of previous injury should
be noted. Rotator cuff tears may be caused by
primary tensile cuff disease (PTCD), primary
compressive cuff disease (PCCD), or internal
impingement. PTCD results from the large,
repetitive loads placed on the rotator cuff as it acts to
decelerate the shoulder during the deceleration phase
of throwing in the stable shoulder. The injury is seen
as a partial undersurface tear of the supraspinatus or
infraspinatus (Lynn and Lippert, 2003). PCCD is
found on the bursal surface of the rotator cuff in
throwers with stable shoulders. This process occurs
secondary to the inability of the rotator cuff to
produce sufficient adduction torque and inferior
force during the deceleration phase of throwing.
Processes that decrease the subacromial space
increase the risk for this type of pathology. Partial-
thickness rotator cuff tears can also occur from
internal impingement (Dugas and Andrew, 2003).
2.10 Clinical Significance
Rotator Cuff Injury
Rotator cuff tears are either partial thickness or
full-thickness tears. Partial thickness tears occur at
the articular (most commonly) or bursal side of the
rotator cuff tendons.
The patient's age, baseline shoulder
function,tear size, chronicity, and degree of tendon r
etraction are several critical elements to be
considered when deciding how to manage each
patient most appropriately. The supraspinatus tendon
KONAS XI and PIT XVIII PERDOSRI 2019 - The 11th National Congress and The 18th Annual Scientific Meeting of Indonesian Physical
Medicine and Rehabilitation Association
98

is the tendon most commonly injured of the rotator
cuff muscles, followed by infraspinatus,
subscapularis, and teres minor. The teres minor
tendon is only rarely involved in rotator cuff
injuries. The subscapularis tendon tear can be
associated with a biceps tendon dislocation from the
bicipital tendon groove moving into the
subscapularis tendon medially (Eovaldi et al, 2018).
Confirmation of intra-articular tendon tears is by
the absence of the biceps tendon in the empty
bicipital groove.18 Labral injuries and Dislocations
Multiple types of shoulder labral injuries can occur
in different patient populations. One particularly
common injury subgroup includes young athletes
afflicted with a traumatic shoulder dislocation. In
the setting of glenohumeral instability, clinicians
should recognize the importance of not only a
recurrent dislocation, but the risk of increased bone
loss and soft tissue compromise which may
ultimately affect the outcome following surgical
repair (Eovaldi et al, 2018).
Glenohumeral instability, especially in the
setting of trauma, is most commonly seen anteriorly.
Posterior shoulder instability can be seen in
weightlifter or football linemen. Rare dislocation
patterns include the superior and inferior
glenohumeral dislocation (luxatio erecta). It is
important to note that in the setting of
multidirectional instability (MDI), especially in the
case of bilateral ligamentous laxity or in a patient
with a personal or family history of a connective
tissue disorder, the probability of recurrent
instability is relatively common. The mainstay
treatment for these injuries centers on physical
therapy and shoulder strengthening programs
(Eovaldi et al, 2018).
Para-labral cysts are most often seen in
association with glenoid labral tears. Para-labral
cyst formation can cause subsequent nerve
compression and denervation of shoulder
muscles. The suprascapular nerve is susceptible to
compression from a para-labral cyst due to its
location as it passes through the suprascapular and
spinoglenoid notches adjacent to the anterior-inferior
labrum. The subscapular nerve is also susceptible to
compression from a para-labral cyst in the
subscapular recess. Isolated atrophy of the teres
minor implies injury to the axillary nerve (Cowan et
al, 2018).
2.11 Adhesive Capsulitis
The cause of frozen shoulder is deposition of
hydroxyapatite crystals into the muscle tendon.
The shoulder is the most common site of
hydroxyapatite calcification in the human body. The
supraspinatus tendon is the most common site of
hydroxyapatite crystal deposition. Frozen shoulder is
associated with diabetes mellitus but may also be
associated with coronary artery disease, cerebral
vascular disease,
rheumatoid arthritis, and thyroid disease (Friedman
et al, 2015).
There are numerous lesions that may occur in the
overhead athlete. Tendonitis, tendonosis, and
bursitis are 3 separate clinical entities for which the
names are often incorrectly used interchangeably.
Tendonitis is inflammation of the tendon. In many
cases, it is actually the tendon sheath that is inflamed
and not the tendon itself. Bursitis is inflammation of
the subacromial bursa. Tendonosis implies
intratendonous disease, such as intrasubstance
degeneration or tearing. The patient clinical
presentation of tendonitis or tendonosis of the rotator
cuff are pain with overhead activity and weakness
secondary to pain. The symptoms in the thrower are
pain during the late cocking phase of throwing,
when the arm is in maximal ER, or pain after ball
release, as the muscles of the rotator cuff slow the
arm during the deceleration phase (Wilk et al, 2009).
Weakness of the supraspinatus and infraspinatus
are common findings in throwers with shoulder
pathology; but asymmetric muscle weakness in the
dominant shoulder is often seen in the healthy
thrower. Differential diagnosis of tendonitis versus
tendonosis is based on MRI and duration and
frequency of symptoms. On MRI, the patient with
tendonitis will exhibit inflammation of the tendon
sheath (the paratenon); conversely, when tendonosis
is present, there exists intrasubstance wear (signal)
of the tendon. Tendonitis/tendonosis is most
frequently an overuse injury in the overhead athlete
and does not usually represent an acute injury
process. The symptoms frequently occur early in the
season, when the athlete’s arm is not conditioned
properly. These injuries may also occur at the end of
the season, as the athlete begins to fatigue. If the
athlete does not participate in an in-season
strengthening program to continue proper muscular
conditioning, tendonitis/tendonosis may also
develop. Specific muscles (external rotator muscles
and scapular muscles) may become weak and
painful due to the stresses of throwing (Wilk et al,
2015).
Biomechanics of Shoulder Injury in Athletes
99

2.12 Internal Impingement
Internal impingement was first described in 1992 by
Walch and associates in tennis players. They
presented arthroscopic clinical evidence that partial,
articular-sided rotator cuff tears were a direct
consequence of what they termed “internal
impingement.” Internal impingement is
characterized by contact of the articular surface of
the rotator cuff and the greater tuberosity with the
posterior and superior glenoid rim and labrum in
extremes of combined shoulder abduction and ER.
In overhead throwing athletes, it appears that
excessive anterior translation of the humeral head,
coupled with excessive glenohumeral joint ER,
predisposes the rotator cuff to impingement against
the glenoid labrum. Repeated internal impingement
may be a cause of undersurface rotator cuff tearing
and posterior labral tears. It is important that the
underlying laxity of the glenohumeral joint be
addressed at the time of treatment for an internal
impingement lesion to prevent recurrence of the
lesion (Manske et al, 2013).
Burkhart et al have proposed that restricted
posterior capsular mobility may result in IR deficits
and may cause pathologic increases in internal
rotator cuff contact and injury. Patients with internal
impingement usually describe an insidious onset of
pain in the shoulder. Pain tends to increase as the
season progresses. Symptoms may have been
present over the past couple of seasons, worsening in
intensity with each successive year. Pain is usually
dull and aching, and is located over the posterior
aspect of the shoulder. Late cocking phase seems to
be most painful. Loss of control and velocity is often
present secondary to the inability to fully externally
rotate the arm without pain. On physical
examination, pain may be elicited over the
infraspinatus muscle and tendon with palpation. Pain
to palpation is more often posterior, in contrast to
rotator cuff tendonitis, which usually elicits pain to
palpation over the greater tuberosity. With internal
impingement, patients usually have full ROM. In
both the normal and pathologic thrower’s shoulder
the dominant arm tends to have 10° to 15° more ER
and 10° to 15° less IR with the arm abducted to 90°,
compared with the nondominant arm. The most
common presentation is for the overhead athlete to
have 1+ to 2+ anterior laxity and 2+ posterior laxity.
Inferior laxity is often present. Most provocative
tests are negative. The most frequent provocative
exam to elicit pain is the internal impingement sign,
described earlier (Rose et al, 2018).
2.13 Superior Labrum Anterior to
Posterior (SLAP) Lession
SLAP lesions are a complex of injuries to the
superior labrum and biceps anchor at the glenoid
attachment. Patients who have SLAP lesions fall
into 2 basic categories. The first consists of overhead
athletes, most commonly baseball players, with a
history of repetitive overhead activity and no history
of trauma. The second category involves patients
with a history of trauma. Burkhart et al have
described the peel-back lesion of the superior labrum,
which frequently occurs in the overhead athlete.
Peel-back lesions are considered a type II SLAP
lesion. The athlete often presents to the practitioner
with complaints of vague onset of shoulder pain and
possibly problems with velocity, control, or other
throwing complaints. The patient may complain of
mechanical symptoms or pain in the late cocking
phase, often poorly localized. This sign occurs when
the arm is placed in abduction and external rotation,
which causes the biceps anchor to twist posteriorly
because of its loose attachment. Typical symptoms
are a catching or locking sensation, and pain with
certain shoulder movements. Pain deep within the
shoulder or with certain arm positions is also
common. The diagnosis of SLAP lesions can be very
difficult, as symptoms can mimic rotator cuff
pathology and glenohumeral joint instability.
Definitive diagnosis can only be made by
arthroscopy (Wilk et al, 2013).
2.14 Thrower’s Exostosis
Thrower’s exostosis is an extracapsular ossification
of the posteroinferior glenoid rarely seen except in
older longtime throwers. This condition is a result of
secondary ossification involving the posterior
capsule, probably due to repetitive trauma. The
osteophyte is thought to originate in the glenoid
attachment of the posterior band of the inferior
glenohumeral ligament, possibly from traction
during deceleration. Patients often have a tight
posterior capsule, with capsular contracture and
asymmetric shoulder motion with an IR deficit. This
lesion can often mimic internal impingement. Pain is
often found in the posterior part of the shoulder and
is worse in late cocking. Patients often describe a
pinching sensation during throwing. Pain usually is
relieved by rest. Plain radiographs will assist in
differentiating this lesion from internal impingement
(Wilk et al, 2009).
KONAS XI and PIT XVIII PERDOSRI 2019 - The 11th National Congress and The 18th Annual Scientific Meeting of Indonesian Physical
Medicine and Rehabilitation Association
100
2.15 Acromioclavicular Joint Injury
Acute acromioclavicular joint (ACJ) injuries can
occur due to a direct force to the acromion typically
with the shoulder adducted, or from an indirect force
elsewhere in the body, for example, a fall onto an
outstretched arm. Patients present with acute
localised pain, swelling and sometimes redness.
Injuries can range from a simple acromioclavicular
ligament sprain that can be managed conservatively,
to ligament tears with ACJ displacement that often
require surgery. Chronic ACJ pain can occur
following acute ACJ injuries or from repeated
irritation to the joint that can develop into osteolysis
or osteoarthritis. These chronic changes can be
caused by sports that involve throwing or lifting
weights. The symptoms will be similar to acute ACJ,
but the pain develops insidiously (Leung, 2016).
2.16 Clavicle Fracture
Clavicle fractures, particularly the mid-third of the
clavicle, are the most common acute shoulder
injuries and account for one in twenty adult fractures.
Fractures located more laterally can disrupt the
acromioclavicular joint. Over 80% of clavicle
fractures can be managed conservatively These
injuries usually occur from a fall onto the clavicle or,
less frequently, a direct blow to the clavicle. Patients
may be involved with contact sports or other at- risk
sports such as horse-riding and cycling. They
present with acute localised pain with swelling and
sometimes visible deformity. Acute injuries are
more likely to present to the hospital Accident &
Emergency Department than primary care (Leung,
2016).
2.17 Glenohumeral Internal Rotation
Deficit (GIRD)
GIRD is defined as a loss of internal rotation in
excess of the adaptive gain in external rotation in the
throwing shoulder (Lin et al, 2018). Clinically
relevant GIRD has been defined as a loss of greater
than 25° of internal rotation in the throwing shoulder
relative to the nonthrowing side (Bukhart, 2003).
The biomechanical model of GIRD is based on the
contractures of the posterior capsule and posterior
band of the inferior glenohumeral ligament
discussed previously. On magnetic resonance (MR)
images, thickening of the posteroinferior capsule is
present, which can be an important clue to look for
concurrent findings in the labrum and rotator cuff.
The proposed pathologic cascade due to GIRD starts
with posterior soft tissue contractures causing
posterosuperior shift of the humeral head, resulting
in excessive external rotation.
This “peels back” the biceps anchor under
extreme tension, subjecting the posterosuperior
structures, including the labrum, to injury. The
extreme external rotation also submits the rotator
cuff to torsional or twisting injury, leading to
eccentric fiber failure and undersurface tearing,
which is distinct from the compressive injury in the
internal impingement model. While prior data
suggested an association between GIRD and an
increased risk for shoulder injuries, specifically
superior labrum anteroposterior (SLAP) tears, a
more recent study proposes that external rotation
insufficiency 5° difference in external rotation
between throwing and nonthrowing arms) rather
than GIRD is associated with shoulder injury.
Nevertheless it is still current practice to manage the
majority of athletes with GIRD via a stretching
regimen, with the 10% who fail conservative
treatment pursuing posterior capsulotomy and SLAP
tear repair (Lin et al, 2018).
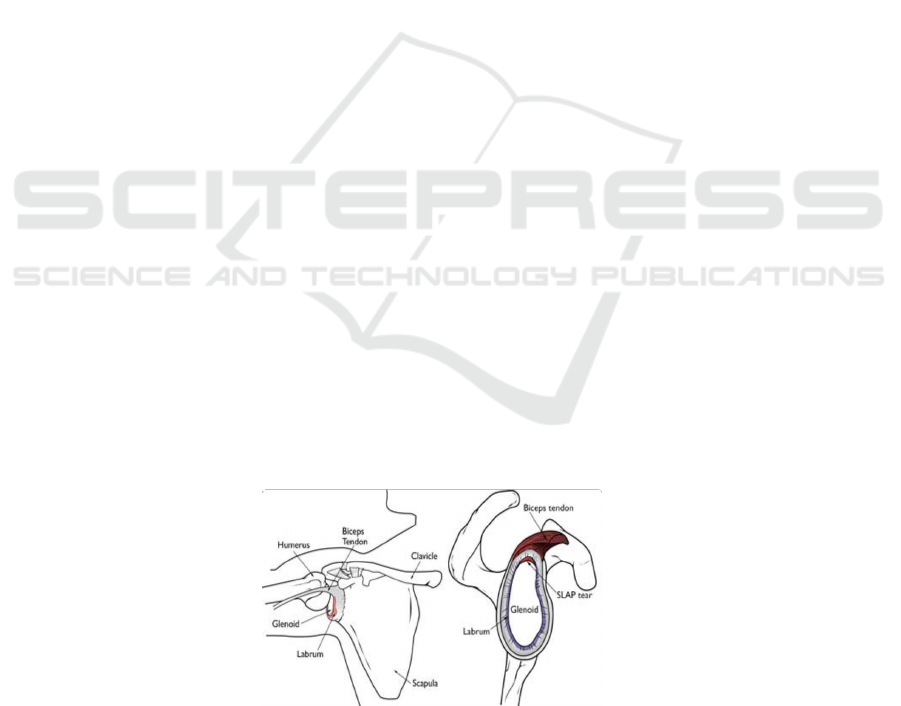
Figure 2: The Labrum and SLAP Tear (Left: Labrum helps to deepen the shoulder socket; Right: cross section view of
shoulder socket shows tipical SLAP tear)
Biomechanics of Shoulder Injury in Athletes
101
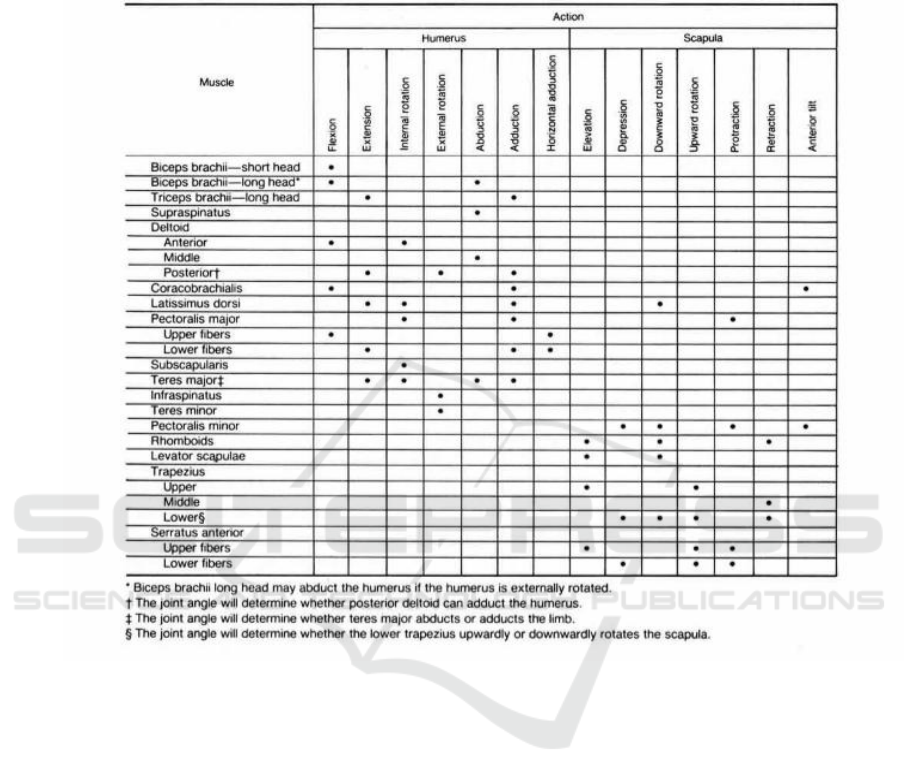
Table 1: Muscle Actions at the Shoulder
KONAS XI and PIT XVIII PERDOSRI 2019 - The 11th National Congress and The 18th Annual Scientific Meeting of Indonesian Physical
Medicine and Rehabilitation Association
102
Table 2: Sports-related shoulder conditions and their possible clinical signs.
Rotator cuff
tendinopathy
Asymmetry and muscle wasting
Palpation tenderness at the
greater tubercle (insertion sites of
three rotator cuff muscles)
Reduced active ROM
Passive ROM intact
Reduced power on resisted movements
Impingement signs
Rotator cuff tears
Shoulder shrug appearance
Partial or no active ROM
Passive ROM often intact
Reduced power on resisted movements
Drop-arm sign in complete tears if
arm cannot be
actively maintained
at 90
○
abduction
Impingement signs
Glenoid
labral injury
Palpation tenderness in the
anterior shoulder structures
Swelling if acute
Reducedexternalrotationandor abduction ROM
Reduced poweron resisted
movements
Biceps load 2 test positiveif
superior labrum
anterior posterior (SLAP) tear
Speed’s test positive if SLAP
Yergason’s test positiveif SLAP
Jerk’s test positive if postero-inferior labral injury
Shoulder
instability
and
dislocation
Prominent humeral head if anter
ior dislocation
Swelling ifacute
Reduced active and passive ROM
if dislocated
Increased active or passive ROM
if instability with
laxity
Apprehension test positive if anterior dislocation
Jerk’s test positive if postero-
inferior dislocation
Upper arm axillary nerve sensation can be reduced
in anterior dislocations
Clavicle Fracture
Localised swelling with deformity
Clavicle shortened or angulated
Localised bony tenderness
ACJ Injury
Step deformity and swelling if
acute
Localised ACJ tenderness
Scarf test positive
Impingement signs if chronic
Biceps
tendinopathy
Bicipital groove tenderness
Speed’s test positive
Yergason’s test positive
REFERENCES
Rockwood CA, Matsen FA, Wirth MA, Lippitt SB. 2009.
The Shoulder. Fourth Edition. Volume One. Saunders
Elsevier: Philadelpia
Lin DJ, Wong TT, Kazam JK. 2018. Shoulder Injuries in
the Throwing Athlete.Radiology. 286(2): 370-87
Eovaldi BJ. Varacallo M. 2018. Anatomy, shoulder and
upper limb, shoulder muscle. NCBI Bookshelf.
[accessed online at:
https://www.ncbi.nlm.nih.gov/books/NBK534836/]
Lynn s. Lippert. Clinical Kinesiology and Anatomy of the
Upper Extremities. 4ed.
Armfield DR, Stickle RL, Robertson DD, Towers JD,
Debski RE. 2003. Biomechanical Basis of Common
Shoulder Problems. Seminars in Musculoskeletal
Radiology.7(1): 5-20.
Biomechanics of Shoulder Injury in Athletes
103

Pandev V. Jaap WW. 2015. Rotator cuff tear: A detailed
update. Asia Pac J Sports Med Arthrosc Rehabil
Technol. 2(1):1-14
Dugas JR, Andrews JR. 2003. Throwing injuries in the
adult. In: DeLee JC, Drez D, Miller MD, eds. DeLee
and Drez’s Orhopaedic Sports Medicine. Philadelphia,
PA: Elsevier Science.
Carroll KW, Helms CA, Otte MT, Moellken SM, Fritz R.
2003. Enlarged spinoglenoid notch veins causing
suprascapular nerve compression. Skeletal Radiol.
Feb;32(2):72-7.
Cowan PT, Varacallo M. StatPearls
[Internet].2018. StatPearls Publishing; Treasure Island
(FL). Anatomy, Back, Scapula.
Friedman JL, FitzPatrick JL, Rylander LS, Bennett C,
Vidal AF, McCarty EC. 2015. Biceps Tenotomy
Versus Tenodesis in Active Patients Younger Than 55
Years: Is There a Difference in Strength and
Outcomes? Orthop J Sports Med.
Wilk KE, Obma P, Simpson CD, Cain EL, Dugas J,
Andrews JR. 2009. Shoulder Injuries in the Overhead
Athlete. Journal of Orthopaedic & Sports Physical
Therapy.39(2):38-54
Manske RC. Grant NM. Lucas B. 2013. Shoulder posterior
internal impingement in the overhead athlete. Int J
Sports Phys Ther.8(2):194-204.
Rose MB, Noonan T. 2018. Glenohumeral internal
rotation deficit in throwing athletes: current
perspectives. Open Access J Sports Med. 9:69-78.
Wilk KE, Macrina LC, Cain EL, Dugas JR, Andrews JR.
2013. The recognition and treatment of superior labral
(SLAP) lesions in the overhead athlete. Int J Sports
Phys Ther.8(5):579-600
Leung R. 2016. Common sports-related shoulder injuries.
Macquarie university Library. [accessed online at:
https://journals.sagepub.com/doi/pdf/10.1177/1755738
016678436]
Burkhart SS, Morgan CD, Kibler WB. 2003. The disabled
throwing shoulder: spectrum of pathology Part I:
pathoanatomy and biomechanics.
Arthroscopy.19(4):404–420.
KONAS XI and PIT XVIII PERDOSRI 2019 - The 11th National Congress and The 18th Annual Scientific Meeting of Indonesian Physical
Medicine and Rehabilitation Association
104
