
Principle of Orthosis Correction in Gait Problem
Tirza Z. Tamin
Department of Physical Medicine and Rehabilitation, Dr. Cipto Mangunkusumo General Hospital,
Faculty of Medicine, University of Indonesia, Jakarta, Indonesia
Keywords: Gait Problem, Orthosis Correction, Sport Injuries
Abstract: Abnormal gait or gait abnormality occurs when the body systems are unable to aid walking in the usual
way. Gait abnormality can be caused by musculoskeletal and neuromuscular problems. It can occur among
every population from pediatric, adult and geriatric cases. If this abnormal pattern persists, it can alter the
biomechanics of the body resulting in more complications such as pain, deformity, and balance problem.
One way to facilitate the gait pattern is by using lower extremity orthosis.
1 INTRODUCTION
Gait is the reflection of how a person walks. Many
factors contribute to constructing a normal gait
pattern, such as proper body alignment,
musculoskeletal system, neuromuscular system,
also balance and proprioceptive mechanism.
Disruption to one or more of these systems will alter
how the body responds to external force, resulting in
gait abnormalities. An orthosis is one of the
conservative techniques to correct misalignment of
lower extremities to facilitate normal gait patterns.
The application of orthosis also can prevent further
deformities. This article will explain about principles
of orthosis application to facilitate normal gait
pattern in several abnormalities.
2 DISCUSSION
Treatment and management of an underlying
condition causing abnormal gait may vary. Some
injuries causing abnormal gait may require surgery
or physical therapy to help return the gait to normal.
For long-term cases of abnormal gait, a person will
likely use assistive devices for treatment. These can
include orthosis, crutches, canes, and walkers. Some
treatments cannot always correct an abnormal gait
completely, but it can at least reduce the severity of
symptoms in most cases (Standford Medicine,
2019).
General principles of orthosis correction in gait
problems are required to be known to ensure proper
prescribing of an orthosis. In correcting gait
abnormalities, orthosis was used to provide support,
stability, and maintain proper alignment to the hip,
knee and ankle joints. Some injury may also cause
deformity or malalignment which will contribute to
the development of gait problems in the future, thus
orthosis were required to prevent the deformity. The
design of orthosis prescribed must allow safe and
effective ambulation by the patient to allow maximal
functional independence. The materials used should
be light, sturdy, and resistance to wear. Prescription
of orthosis should meet the functional requirement
of the client, correlate to the patient's personality and
impact of the device upon the patient, so each client
should be evaluated individually. It is also important
to remember that in some cases orthosis is only one
component of the treatment and is not the whole
treatment for the patient.
Types of Orthosis
Orthoses are braces or splints that serve to improve
the position of a joint (positioning type) and/or
function (functional type) of an injured extremity, it
used to modify the structural and functional
characteristics of the neuromuscular and skeletal
system. Lower limb orthoses are the most commonly
prescribed type of orthoses, with Foot Orthoses
(FO), Ankle-Foot Orthoses (AFOs), Knee Orthoses
(KO), Knee-Ankle-Foot Orthoses (KAFOs) and
knee braces (Fox et al, 2019).
Foot orthoses (FO) can be helpful to correct
problems in the foot, knee, hip, and spine.
62
Tamin, T.
Principle of Orthosis Correction in Gait Problem.
DOI: 10.5220/0009062400620066
In Proceedings of the 11th National Congress and the 18th Annual Scientific Meeting of Indonesian Physical Medicine and Rehabilitation Association (KONAS XI and PIT XVIII PERDOSRI
2019), pages 62-66
ISBN: 978-989-758-409-1
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

Prescription for foot orthoses are divided into two
categories as defined by the American Podiatric
Medical Association, there are (Fox et al, 2019).
1. Functional orthotics to control
abnormal motion may be used to treat foot
pain caused by abnormal motion; they can
also be used to treat injuries such as shin
splints or tendinitis. Functional orthotics
are usually crafted of a semirigid material
such as plastic or graphite.
2. Accommodative orthotics are
softer and provide additional cushioning
and support. They can be used to treat
diabetic foot ulcers, painful calluses on the
bottom of the foot, and other uncomfortable
conditions.
Two types are custom and non-custom orthoses.
Custom foot orthoses start with a thorough
examination of the foot-ankle complex to determine
limitations in range of motion in both the forefoot
and the rear foot, including calcaneal talus
alignment. Once this is done, a gait assessment is
performed without shoes and socks on. An
impression is taken using step-in foam, cast, or a
scan (with an optical digitizer) with the foot held in
subtalar neutral. Any other type of foot orthosis is
non-custom. This includes the type patients may
receive from various outlets claiming custom fit.
There are many minor foot problems for which non-
custom foot orthoses provide appropriate treatment
(Nolan et al, 2010).
Successful foot orthotic
treatment is dependent on the shoes that are used in
conjunction with the orthosis. If a person brings in a
shoe that barely accommodates his or her feet (too
tight or too worn), then placing a foot orthotic into it
will lead to failure. After fitting the patient using the
proper shoes, the orthotist reassesses the patient's
gait to determine whether goals for alignment,
posture, pain, and corrections to the foot-ankle
complex are being met. Education and follow up is
key to a successful outcome (Fox et al, 2019).
Ankle-Foot Orthoses (AFOs) are used for
problems dealing with foot and ankle issues. These
orthoses include any devices that pass across the
ankle joint but stay distal to the knee joint. This
orthosis is used for diagnoses that range from ankle
sprains to stroke management and potentially be
used for any neuromuscular condition requiring
support or assistance at the level of the foot and
ankle (Fox et al, 2019).
Figure 1. Ankle–Foot Orthosis (AFOs) (Fox et al, 2019).
A study conducted by Nolan KJ., Saalia KK. et
al (2010) in the evaluation of a dynamic ankle-foot
orthosis in hemiplegic gait showed that there was
increased hip flexion at foot strike and toe-off,
increased hip sagittal plane angular velocity during
the swing phase and decreased abduction. The
dynamic ankle-foot orthosis had a positive effect on
the participant's overall gait (Nolan et al, 2010). A
study conducted by Sankaranarayan H., Gupta A. et
al (2016) in Role of ankle-foot orthosis in improving
locomotion and functional recovery in patients with
stroke showed that ankle-foot orthosis (AFO)
improved locomotion and functional recovery after
stroke (Sankaranarayan et al, 2019).
A study
conducted by Ferreira LAB, Neto HP, et al (2013)
showed that all types of AFO (Ankle-foot Orthosis)
resulted in a significant improvement in gait velocity
compared to a control group without the use of an
AFO. There have been advances in understanding
how AFOs can enhance the patient's ability. This
includes functional electrical stimulation devices
that replace the traditional AFO with electrical
stimulation during various times in the gait cycle
(Ferreira et al, 2013).
Knee orthosis (KO) can provide stability, limits
motion, and controls the medial-lateral movement of
the knee joint. A KO is primarily used when the
ankle-foot complex is fully functional and thus a
knee–ankle– foot orthosis (KAFO) is unnecessary.
A study conducted by Jeffrey W, Sugar T. et al
(2011) showed that patients who got stroke and used
Principle of Orthosis Correction in Gait Problem
63
Powered Ankle Foot Orthosis (PAFO) showed
significant improvement in cadence, ankle range of
motion, and power generation capabilities. (sugar)
Indications for KO (Fox et al, 2019):
• Medial–lateral knee instability
• Post-surgery or injury
postoperative stabilization
• Support for medial collateral
ligament (MCL), anterior cruciate ligament
(ACL), and posterior cruciate ligament
(PCL) tears and stress to limit extension or
flexion
• Rotational control
• Osteoarthritis
Figure 2. Knee Orthosis tools (Fox et al, 2019).
Figure 3. Knee-Ankle-Foot Orthoses (KAFOs) (Fox et al,
2019).
Knee-Ankle-Foot Orthoses (KAFOs) provide
stability to the knee and foot when needed during the
stance phase of ambulation and knee hyperextension
control from midstance to the terminal stance phase
in the gait cycle. Clinical indications for a KAFO
include instability of the knee and ankle, quadriceps
weakness or absence, hyperextension of the knee,
varus or valgus deformity correction in children, and
paralysis of one or both legs.
Knee braces are designed to transfer load while
allowing for normal knee motion. This depends on
the amount of leverage the knee brace can provide.
Longer braces produce a greater amount of leverage;
therefore, athletes typically select the longest brace
that provides the best fit to the extremity. The
optimal position to apply the leverage depends on
the goal of the knee brace (An K et al).
Figure 4. Knee brace (An K et al)
Wedged insoles are one of the treatment options
frequently recommended for the management of
knee OA. There are two kinds of wedged insoles,
laterally wedged insole and medial wedged insole.
This orthosis is made from various materials. The
most common material is silicon rubber,
polypropylene, and ethylene-vinyl acetate. The usual
thickness of wedged insole is ¼ inch with the
density of a 40-70 durometer scale. The density of
insole is the most important consideration regarding
its effectiveness. Fisher et al (2007) suggest that the
most optimal insole density is within the range of
20% to 50%. Wedged insole application shows
reduced in external knee adduction moment.
Orthosis for Specific Gait Problem
Cerebral palsy
Cerebral palsy is one of the most common
movement abnormalities in children. In children,
gait is a prerequisite requirement for socializing and
playing. Gait abnormalities in cerebral palsy can be
caused by spasticity, abnormal motor tone, loss of
motoric control and balance disorder (Baxter et al).
KONAS XI and PIT XVIII PERDOSRI 2019 - The 11th National Congress and The 18th Annual Scientific Meeting of Indonesian Physical
Medicine and Rehabilitation Association
64

In general, spastic motor patterns are reasonably
consistent from stride to stride and from day to day.
However, as the age growing and there’s some
intervention over the longer term, the gait pattern
will change. The most common change with age is
from a pattern of `toe walking' (because the
gastrocnemius is dominant) to a pattern of increasing
hip and knee flexion and eventually, `crouch gait'
with hip and knee flexion and ankle dorsiflexion
(Concept for the Orthotic Treatment of Gait
Problems).
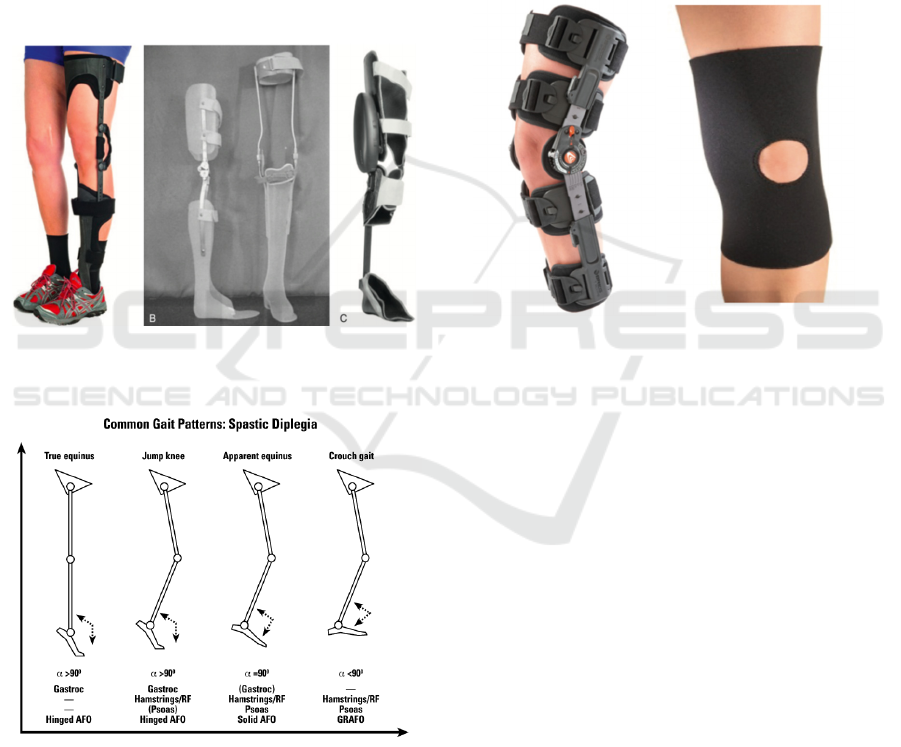
Figure 5. Common gait pattern in cerebral palsy diplegic
GRAFO and SAFO are the recommended type of
AFO to be used when the GRF directed to the
anterior knee. GRAFO is more recommended for a
patient with crouch gait to reduce ankle dorsiflexion
and increase knee extension moment. GRAFO can
control or reduce ankle and subtalar movement. By
controlling joint movement more distally, it will
change the GRF and also will affect the proximal
joint using PF-KE couple principal. A ventral shell
of GRAFO will reduce or limit anterior translation
of tibia thereby reducing ankle dorsiflexion.
(10,11)
Harrington et al and Gage reported that GRAFO will
limit ankle rocker and it will increase knee extension
(Rodda et al, 2001).
Obesity with knee osteoarthritis
Common malalignment regarding osteoarthritis is
varus and valgus alignment. Knee osteoarthritis
which affected the medial compartment will result in
a varus alignment, and which affected the lateral
compartment will result in valgus alignment.
Malalignment will cause GRF response to muscle
activation and the moment. These changes will alter
the normal gait pattern.
Patients with medial knee osteoarthritis and
varus malalignment of the knee are subject to high
overload and high angles of dynamic varus in the
knee. In these individuals, there is a pattern of gait in
external rotation with a reduction of velocity as
adaptive factors, yet insufficient to reduce weight-
bearing to normal values.
The highest flexor moment presented
demonstrates another adaptive mechanism which is
to transfer weight bearing from the frontal plane to
the sagittal plane. Individuals with medial knee
osteoarthritis have less flexion-extension variation,
which characterizes with a predominance of flexion.
Patients with knee OA demonstrate changes in gait
patterns such as increased toeing-out, reduction in
gait speed, and lateral sway of the trunk in the stance
leg.
In mild to moderate knee osteoarthritis, lateral
wedged insole (LWI) is one of the nonoperative
realignment strategies for medial compartment knee
OA. Several studies reported that LWI will displace
vector of GRF from the center of plantar pedis more
laterally to reduce medial compartment knee
loading. The force that applied on the knee started
from the center of pressure on plantar pedis. This
force will be transferred superiorly towards the knee.
A recent study shows that LWI will reduce external
knee adduction moments.
Knee unloader braces with valgus adjustment are
a mechanical intervention designed to reduce pain,
improve physical function, and possibly slow
disease progression. Pain relief is thought to be
mediated by distracting the involved compartment
via external valgus forces applied to the knee. In so
doing, tibiofemoral alignment is improved, and load
is shifted off the degenerative compartment, where
exposure to potentially damaging and provocative
mechanical stresses are reduced.
Figure 6. Knee unloader braces with valgus adjustment
Principle of Orthosis Correction in Gait Problem
65

Knee unloader braces with valgus adjustment are
effective in mediating pain relief caused by knee
osteoarthritis and malalignment, bracing should be
fully used before joint realignment or replacement
surgery is considered. Knee unloader braces with
valgus adjustment are reported to be a safe and
inexpensive treatment that mediates pain relief and
ameliorates function for patients with knee OA.
3 CONCLUSIONS
The orthosis is an externally applied device used to
modify the structural and functional characteristics
of the neuromuscular and skeletal system. The
orthosis can improve the quality of life of patients, it
showed that they can do activity daily living
properly especially in gait problems.
REFERENCES
Standford Medicine. Gait Abnormalities [Internet]. 2019
[cited 2019 Aug 27]. Available from:
https://stanfordmedicine25.stanford.edu/the25/gait.htm
l
Fox J, Lovegreen W. Lower Limb Orthoses : Atlas of
Orthoses and Assistive Devices. 5th ed. Philadelphia:
Elsevier; 2019. 239-246 p.
Nolan KJ, Savalia KK, Yarossi M, Elovic EP. Evaluation
of a dynamic ankle foot orthosis in hemiplegic gait : A
case report. 2010;27:343–50.
Sankaranarayan H, Gupta A, Khanna M, Taly AB,
Thennarasu K. Role of ankle foot orthosis in
improving locomotion and functional recovery in
patients with stroke : A prospective rehabilitation
study. 2019;
Ferreira LAB, Neto HP, Grecco LA, Et.al. Effect of
Ankle-foot Orthosis on Gait Velocity and Cadence of
Stroke Patients : A Systematic Review. 2013;1503–8.
Street JC. Practice Analysis of Certified Technicians in the
Disciplines of Orthotics and Prosthetics.
An K, Bowker JH, Andrews S, Bunch WH, Calhoun CL.
Atlas of Orthoses and Assistive Devices. Fourth.
Baxter P, Morris C, Rosenbaum P, Paneth N, Leviton A,
Goldstein M, et al. The Definition and Classification
of Cerebral Palsy Contents Foreword Historical
Perspective Definition and Classification Document.
:1–44.
Treatment O, Problems G, Palsy C. A Concept for the
Orthotic Treatment of Gait Problems.
Rodda J, Graham HK. Classi ® cation of gait patterns in
spastic hemiplegia and spastic diplegia : a basis for a
management algorithm. 2001;8(03):98–108.
Harrington ED, Lin RS, Gage JR. Use of the Anterior
Floor Reaction Orthosis in Patients with Cerebral
Palsy.
KONAS XI and PIT XVIII PERDOSRI 2019 - The 11th National Congress and The 18th Annual Scientific Meeting of Indonesian Physical
Medicine and Rehabilitation Association
66
